
Assessment of Physicians’ Practice in Implementing Antibiotic Stewardship Program in Najran City, Saudi Arabia: A Cross-Sectional Study

 ,
,
Abstract
1. Introduction
2. Methodology
2.1. Study Design and Population
2.2. Sample Size, Sampling Method, and Data Collection
2.3. Construction, Validation, and Reliability of Study Tool
2.4. Ethical Clearance
2.5. Questionnaire Criteria
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Haseeb, A.; Faidah, H.S.; Al-Gethamy, M.; Iqbal, M.S.; Alhifany, A.A.; Ali, M.; Abuhussain, S.S.A.; Elrggal, M.E.; Almalki, W.H.; Alghamdi, S.; et al. Evaluation of Antimicrobial Stewardship Programs (ASPs) and their perceived level of success at Makkah region hospitals, Kingdom of Saudi Arabia. Saudi Pharm. J. 2020, 28, 1166–1171. [Google Scholar] [CrossRef] [PubMed]
- Klein, E.Y.; Van Boeckel, T.P.; Martinez, E.M.; Pant, S.; Gandra, S.; Levin, S.A.; Goossens, H.; Laxminarayan, R. Global Increase and Geographic Convergence in Antibiotic Consumption between 2000 and 2015. Proc. Natl. Acad. Sci. USA 2018, 115, E3463–E3470. [Google Scholar] [CrossRef] [PubMed]
- Atif, M.; Ihsan, B.; Malik, I.; Ahmad, N.; Saleem, Z.; Sehar, A.; Babar, Z.-u.-D. Antibiotic stewardship program in Pakistan: A multicenter qualitative study exploring medical doctors’ knowledge, perception and practices. BMC Infect. Dis. 2021, 21, 374. [Google Scholar] [CrossRef] [PubMed]
- Atif, M.; Asghar, S.; Mushtaq, I.; Malik, I. Community pharmacists as antibiotic st ewards: A qualitative study exploring the current status of Antibiotic Stewardship Program in Bahawalpur, Pakistan. J. Infect. Public Health 2020, 13, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Ha, D.R.; Haste, N.M.; Gluckstein, D.P. The Role of Antibiotic Stewardship in Promoting Appropriate Antibiotic Use. Am. J. Lifestyle Med. 2017, 13, 376–383. [Google Scholar] [CrossRef] [PubMed]
- Howard, P.; Pulcini, C.; Hara, G.L.; West, R.M.; Gould, I.M.; Harbarth, S.; Nathwani, D. An international cross-sectional survey of antimicrobial stewardship programmes in hospitals. J. Antimicrob. Chemother. 2015, 70, 1245–1255. [Google Scholar] [CrossRef] [PubMed]
- Salem, M.R.; Youssef, M.R.L.; Shalaby, S.F.; Mahmoud, A.T.; Ismail, M.; Ibrahim, S.K. Perspectives on Antibiotic Stewardship Programs among Health Care Providers at Two University Hospitals in Egypt. Int. J. Environ. Res. Public Health 2023, 20, 3777. [Google Scholar] [CrossRef]
- Harun, M.G.D.; Anwar, M.M.U.; Sumon, S.A.; Hassan, M.Z.; Mohona, T.M.; Rahman, A.; Abdullah, S.A.H.M.; Islam, M.S.; Kaydos-Daniels, S.C.; Styczynski, A.R. Rationale and guidance for strengthening infection prevention and control measures and antimicrobial stewardship programs in Bangladesh: A study protocol. BMC Health Serv. Res. 2022, 22, 1239. [Google Scholar] [CrossRef]
- Setiawan, E.; Cotta, M.O.; Abdul-Aziz, M.H.; Sosilya, H.; Widjanarko, D.; Wardhani, D.K.; Roberts, J.A. Indonesian healthcare providers’ perceptions and attitude on antimicrobial resistance, prescription and stewardship programs. Future Microbiol. 2022, 17, 351–362. [Google Scholar] [CrossRef]
- Thabit, A.K.; Alabbasi, A.Y.; Alnezary, F.S.; Almasoudi, I.A. An Overview of Antimicrobial Resistance in Saudi Arabia (2013–2023) and the Need for National Surveillance. Microorganisms 2023, 11, 2086. [Google Scholar] [CrossRef]
- Cunha, C.B.; Varughese, C.A.; Mylonakis, E. Antimicrobial Stewardship Programs (ASPs): The Devil Is in the Details. Virulence 2013, 4, 147–149. [Google Scholar] [CrossRef]
- Baraka, M.A.; Alsultan, H.; Alsalman, T.; Alaithan, H.; Islam, M.A.; Alasseri, A.A. Health care providers’ perceptions regarding antimicrobial stewardship programs (AMS) implementation-facilitators and challenges: A cross-sectional study in the Eastern province of Saudi Arabia. Ann. Clin. Microbiol. Antimicrob. 2019, 18, 26. [Google Scholar] [CrossRef]
- Alghamdi, S.; Atef-Shebl, N.; Aslanpour, Z.; Berrou, I. Barriers to implementing antimicrobial stewardship programmes in three Saudi hospitals: Evidence from a qualitative study. J. Glob. Antimicrob. Resist. 2019, 18, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Core Elements of Antibiotic Stewardship. Global Alliance for Infections in Surgery. (8 November 2019). Available online: https://infectionsinsurgery.org/core-elements-of-antibiotic-stewardship/ (accessed on 1 December 2023).
- Jinks, T.; Lee, N.; Sharland, M.; Rex, J.; Gertler, N.; Diver, M.; Jones, I.; Jones, K.; Mathewson, S.; Chiara, F. A time for action: Antimicrobial resistance needs global response. Bull. World Health Organ. 2016, 94, 558. [Google Scholar] [CrossRef]
- Global Action Plan on Antimicrobial Resistance. Available online: http://www.who.int/antimicrobial-resistance/global-action-plan/en (accessed on 22 January 2024).
- Boucher, H.W.; Bakken, J.S.; Murray, B.E. The United Nations and the urgent need for coordinated global action in the fight against antimicrobial ResistanceCoordinated global action to fight against antimicrobial resistance. Ann. Intern. Med. 2016, 165, 812–813. [Google Scholar] [CrossRef]
- Vernooy, C.P.; Ang, A.; Émond, Y.; Leduc, J.M.; Morency-Potvin, P. Assessment of antimicrobial prescribing practice, knowledge, and culture in three teaching hospitals. Off. J. Assoc. Med. Microbiol. Infect. Dis. Can. 2022, 7, 317–322. [Google Scholar] [CrossRef]
- Sayegh, N.; Hallit, S.; Hallit, R.; Saleh, N.; Zeidan, R.K. Physicians’ attitudes on the implementation of an antimicrobial stewardship program in Lebanese hospitals. Pharm. Pract. 2021, 19, 2192. [Google Scholar] [CrossRef]
- Babatola, A.O.; Fadare, J.O.; Olatunya, O.S.; Obiako, R.; Enwere, O.; Kalungia, A.; Ojo, T.O.; Sunmonu, T.A.; Desalu, O.; Godman, B. Addressing antimicrobial resistance in Nigerian hospitals: Exploring physicians prescribing behavior, knowledge, and perception of antimicrobial resistance and stewardship programs. Expert. Rev. Anti-Infect. Ther. 2021, 19, 537–546. [Google Scholar] [CrossRef]
- Yau, J.W.; Thor, S.M.; Tsai, D.; Speare, T.; Rissel, C. Antimicrobial stewardship in rural and remote primary health care: A narrative review. Antimicrob. Resist. Infect. Control 2021, 10, 105. [Google Scholar] [CrossRef]
- Zhuo, C.; Wei, X.; Zhang, Z.; Hicks, J.P.; Zheng, J.; Chen, Z.; Haldane, V.; Walley, J.; Guan, Y.; Xu, H.; et al. An antibiotic stewardship programme to reduce inappropriate antibiotic prescribing for acute respiratory infections in rural Chinese primary care facilities: Study protocol for a clustered randomised controlled trial. Trials 2020, 21, 394. [Google Scholar] [CrossRef]
- Kim, B.; Lee, M.J.; Moon, S.M.; Park, S.Y.; Song, K.H.; Lee, H.; Park, J.S.; Lee, M.S.; Choi, S.M.; Yeom, J.S.; et al. Current status of antimicrobial stewardship programmes in Korean hospitals: Results of a 2018 nationwide survey. J. Hosp. Infect. 2020, 104, 172–180. [Google Scholar] [CrossRef] [PubMed]
- Mistry, R.D.; Newland, J.G.; Gerber, J.S.; Hersh, A.L.; May, L.; Perman, S.M.; Kuppermann, N.; Dayan, P.S. Current State of Antimicrobial Stewardship in Children’s Hospital Emergency Departments. Infect. Control Hosp. Epidemiol. 2017, 38, 469–475. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study Variables | n (%) |
|---|---|
| Age group | |
| 24–35 years | 50 (39.1%) |
| 36–45 years | 56 (43.8%) |
| >45 years | 22 (17.2%) |
| Gender | |
| Male | 77 (60.2%) |
| Female | 51 (39.8%) |
| Marital status | |
| Single | 35 (27.3%) |
| Married | 93 (72.7%) |
| Nationality † | |
| Saudi | 38 (31.1%) |
| Non-Saudi | 84 (68.9%) |
| Position † | |
| Supervisor | 13 (12%) |
| Practitioner | 75 (69.4%) |
| Both | 20 (18.5%) |
| Qualifications | |
| Diploma | 43 (33.6%) |
| Bachelor | 5 (3.9%) |
| Master | 21 (16.4%) |
| PhD | 8 (6.3%) |
| Board | 42 (32.8%) |
| Others | 9 (7%) |
| Healthcare facility † | |
| PHC Center | 16 (13.1%) |
| Hospital-Outpatient Clinic | 54 (44.3%) |
| Hospital-Emergency Department | 47 (38.5%) |
| Polyclinic | 5 (4.1%) |
| Workplace † | |
| MOH | 67 (54%) |
| University Health Services | 16 (12.9%) |
| Military Health Services | 17 (13.7%) |
| National Guard Health Services | 5 (4%) |
| Interior Ministry Health Services | 1 (0.8%) |
| Private Sector | 18 (14.5%) |
| Years of experience | |
| 1–5 years | 40 (31.3%) |
| 6–10 years | 32 (25%) |
| 11–15 years | 31 (24.2%) |
| >15 years | 25 (19.5%) |
| Statement | Mean ± SD | Never n (%) | Rarely n (%) | Sometimes n (%) | Often n (%) | Always n (%) |
|---|---|---|---|---|---|---|
| Enhancing infection prevention and control score | 4.75 ± 0.51 | -- | -- | -- | -- | -- |
| 4.75 ± 0.61 | 1 (0.80%) | 0 | 6 (4.7%) | 16 (12.5%) | 105 (82.0%) |
| 4.74 ± 0.55 | 0 | 0 | 7 (5.5%) | 19 (14.8%) | 102 (79.7%) |
| Controlling source control score | 4.83 ± 0.39 | -- | -- | -- | -- | -- |
| 4.86 ± 0.39 | 0 | 0 | 2 (1.6%) | 14 (10.9%) | 112 (87.5%) |
| 4.8 ± 0.49 | 0 | 1 (0.80%) | 2 (1.6%) | 18 (14.1%) | 107 (83.6%) |
| Prescribing antibiotics when they are truly needed score | 4.45 ± 0.59 | -- | -- | -- | -- | -- |
| 4.5 ± 0.95 | 2 (1.6%) | 7 (5.5%) | 4 (3.1%) | 26 (20.3%) | 89 (69.5%) |
| 4.59 ± 0.66 | 0 | 1 (0.80%) | 9 (7.0%) | 32 (25.0%) | 86 (67.2%) |
| 4.37 ± 0.95 | 3 (2.3%) | 0 | 17 (13.3%) | 33 (25.8%) | 75 (58.6%) |
| 4.36 ± 0.99 | 4 (3.1%) | 6 (4.7%) | 6 (4.7%) | 36 (28.1%) | 76 (59.4%) |
| Prescribing appropriate antibiotics with adequate dosages score | 4.43 ± 0.79 | -- | -- | -- | -- | -- |
| 4.52 ± 1.05 | 5 (3.9%) | 0 | 8 (6.3%) | 22 (17.2%) | 93 (72.7%) |
| 4.16 ± 1.17 | 4 (3.1%) | 8 (6.3%) | 18 (14.1%) | 28 (21.9%) | 70 (54.7%) |
| 4.45 ± 0.91 | 2 (1.6%) | 3 (2.3%) | 8 (6.3%) | 35 (27.3%) | 80 (62.5%) |
| 4.42 ± 1.05 | 4 (3.1%) | 3 (2.3%) | 10 (7.8%) | 26 (20.3%) | 85 (66.4%) |
| 4.39 ± 0.98 | 3 (2.3%) | 1 (0.80%) | 13 (10.2%) | 34 (6.6%) | 77 (60.2%) |
| 4.57 ± 0.94 | 3 (2.3%) | 0 | 10 (7.8%) | 20 (7.8%) | 95 (74.2%) |
| 4.51 ± 0.99 | 4 (3.1%) | 0 | 6 (4.7%) | 31 (24.2%) | 87 (68.0%) |
| Reassessing antimicrobial treatment when culture results are available score | 4.33 ± 0.87 | -- | -- | -- | -- | -- |
| 4.69 ± 0.78 | 2 (1.6%) | 0 | 5 (3.9%) | 20 (15.6%) | 101 (78.9%) |
| 4.16 ± 1.08 | 3 (2.3%) | 5 (3.9%) | 21 (16.4%) | 35 (27.3%) | 64 (50.0%) |
| 4.13 ± 1.24 | 6 (4.7%) | 5 (3.9%) | 15 (11.7%) | 36 (28.1%) | 66 (51.6%) |
| Using the shortest duration of antibiotics based on evidence score | 4.42 ± 0.85 | -- | -- | -- | -- | -- |
| 4.49 ± 0.88 | 2 (1.6%) | 1 (0.80%) | 10 (7.8%) | 32 (25.0%) | 83 (64.8%) |
| 4.40 ± 0.99 | 3 (2.3%) | 2 (1.6%) | 15 (11.7%) | 27 (21.1%) | 81 (63.3%) |
| 4.23 ± 0.99 | 2 (1.6%) | 6 (4.7%) | 13 (10.2%) | 44 (34.4%) | 63 (49.2%) |
| 4.55 ± 1.11 | 6 (4.7%) | 0 | 3 (2.3%) | 22 (17.2%) | 97 (75.8%) |
| Educating staff score | 3.67 ± 1.27 | -- | -- | -- | -- | -- |
| 3.54 ± 1.48 | 16 (12.5%) | 15 (11.7%) | 25 (19.5%) | 24 (18.8%) | 48 (37.5%) |
| 3.66 ± 1.39 | 10 (7.8%) | 10 (7.8%) | 35 (19.5%) | 25 (19.5%) | 48 (37.5%) |
| 3.81 ± 1.35 | 9 (7.0%) | 8 (6.3%) | 28 (21.9%) | 30 (23.4%) | 53 (41.4%) |
| Supporting surveillance of AMR and HAIs and monitoring of antibiotic consumption score | 3.56 ± 1.34 | -- | -- | -- | -- | -- |
| 3.74 ± 1.38 | 13 (10.2%) | 7 (5.5%) | 26 (20.3%) | 32 (25.0%) | 50 (39.1%) |
| 3.48 ± 1.49 | 18 (14.1%) | 11 (8.6%) | 28 (21.9%) | 28 (21.9%) | 43 (33.6%) |
| 3.47 ± 1.56 | 18 (14.1%) | 18 (14.1%) | 16 (12.5%) | 31 (24.2%) | 45 (35.2%) |
| 3.56 ± 1.52 | 20 (15.6%) | 10 (7.8%) | 21 (16.4%) | 28 (21.9%) | 49 (38.3%) |
| Supporting an interdisciplinary approach score | 3.88 ± 1.09 | -- | -- | -- | -- | -- |
| 3.95 ± 1.28 | 8 (6.3%) | 6 (4.7%) | 22 (17.2%) | 35 (27.3%) | 57 (44.5%) |
| 3.96 ± 1.27 | 7 (5.5%) | 7 (5.5%) | 22 (17.2%) | 35 (27.3%) | 57 (44.5%) |
| 4.27 ± 1.02 | 3 (2.3%) | 3 (2.3%) | 15 (11.7%) | 40 (31.3%) | 67 (52.3%) |
| 4.02 ± 1.33 | 11 (8.6%) | 2 (1.6%) | 16 (12.5%) | 38 (29.7%) | 61 (47.7%) |
| 3.83 ± 1.32 | 10 (7.8%) | 7 (5.5%) | 22 (17.2%) | 40 (31.3%) | 49 (38.3%) |
| 3.58 ± 1.43 | 17 (13.3%) | 4 (3.1%) | 30 (23.4%) | 36 (28.1%) | 41 (32.0%) |
| 3.71 ± 1.33 | 12 (9.4%) | 4 (3.1%) | 36 (28.1%) | 29 (22.7%) | 47 (36.7%) |
| 3.72 ± 1.38 | 11 (8.6%) | 12 (9.4%) | 26 (20.3%) | 28 (21.9%) | 51 (39.8%) |
| Total practice score | 154.9 ± 25.5 | -- | -- | -- | -- | -- |
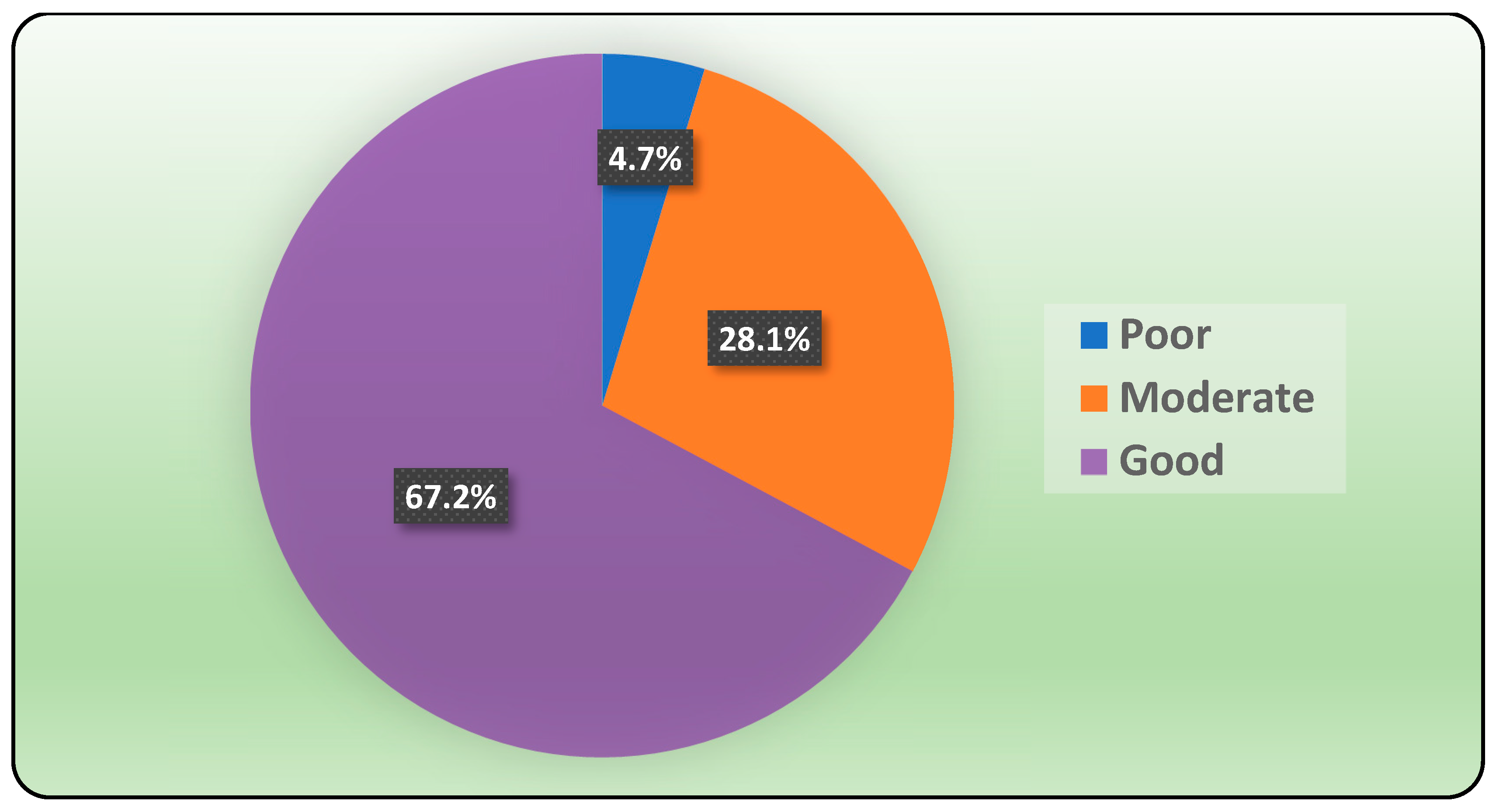
| Level of practice in the efficacy of ASP | ||||||
| • Poor | 06 (04.7%) | -- | -- | -- | -- | -- |
| • Moderate | 36 (28.1%) | -- | -- | -- | -- | -- |
| • Good | 86 (67.2%) | -- | -- | -- | -- | -- |
| Variables | n (%) |
|---|---|
| Average number of infection cases you manage daily (mean ± SD) | 13.5 ± 14.1 |
| ≤5 | 52 (40.6%) |
| 6–10 | 17 (13.3%) |
| 11–20 | 36 (28.1%) |
| >20 | 23 (18.0%) |
| Average number of infection cases you manage daily with symptomatic treatment (no antibiotic) (mean ± SD) | 5.98 ± 8.11 |
| ≤5 | 82 (64.1%) |
| 6–10 | 28 (21.9%) |
| 11–20 | 16 (12.5%) |
| >20 | 2 (1.6%) |
| Average number of infection cases you manage daily with delayed antibiotic prescribing treatment (mean ± SD) | 3.58 ± 4.29 |
| ≤5 | 103 (80.5%) |
| 6–10 | 23 (18.0%) |
| 11–20 | 2 (1.6%) |
| >20 | 0 |
| Average number of infection cases you manage daily with initiated antibiotic prescribing treatment (mean ± SD) | 6.43 ± 6.65 |
| ≤5 | 80 (62.5%) |
| 6–10 | 26 (20.3%) |
| 11–20 | 18 (14.1%) |
| >20 | 4 (3.1%) |
| Factor | Practice Score (185) Mean ± SD | Z-Test | p-Value § |
|---|---|---|---|
| Age group | |||
| <40 years | 150 ± 28.6 | 3.004 | 0.003 ** |
| ≥40 years | 164 ± 14.9 | ||
| Gender | |||
| Male | 159.8 ± 18.9 | 2.124 | 0.034 ** |
| Female | 147.9 ± 31.8 | ||
| Marital status | |||
| Single | 157.9 ± 20.2 | 0.3 | 0.764 |
| Married | 153.8 ± 27.3 | ||
| Nationality † | |||
| Saudi | 163 ± 15.9 | 2.279 | 0.023 ** |
| Non-Saudi | 150.9 ± 28.3 | ||
| Position † | |||
| Supervisor | 157.8 ± 19.2 | 3.34 | 0.188 ‡ |
| Practitioner | 150.5 ± 28.6 | ||
| Both | 162.1 ± 6.4 | ||
| Qualifications | |||
| Bachelor or diploma | 156.9 ± 25.9 | 0.81 | 0.418 |
| Master or higher | 153.7 ± 25.3 | ||
| Healthcare facility † | |||
| PHC Center/Polyclinic | 161.9 ± 17.7 | 0.657 | 0.72 |
| Hospital-Outpatient Clinic | 152.5 ± 30.3 | ||
| Hospital-Emergency Department | 153.9 ± 23.7 | ||
| Workplace † | |||
| MOH | 151.9 ± 26.7 | 0.903 | 0.366 |
| Non-MOH | 157.8 ± 19.9 | ||
| Years of experience | |||
| ≤10 years | 156.6 ± 24.4 | 0.606 | 0.545 |
| >10 years | 152.8 ± 26.9 |
| Factor | Practice Score (185) Mean ± SD | Z-Test | p-Value § |
|---|---|---|---|
| Average number of infections cases you manage daily | |||
| ≤5 | 161.8 ± 19.4 | 2.53 | 0.011 ** |
| >5 | 150.2 ± 28.2 | ||
| Average number of infection cases you manage daily with symptomatic treatment (no antibiotic) | |||
| ≤5 | 155.5 ± 25.4 | 0.318 | 0.75 |
| >5 | 153.9 ± 25.9 | ||
| Average number of infection cases you manage daily with delayed antibiotic prescribing treatment | |||
| ≤5 | 154.5 ± 24.2 | 1.23 | 0.219 |
| >5 | 156.8 ± 30.9 | ||
| Average number of infection cases you manage daily with initiated antibiotic prescribing treatment | |||
| ≤5 | 158.4 ± 23.9 | 2.288 | 0.022 ** |
| >5 | 149.2 ± 27.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alqahtani, N.S.; Bilal, M.M.; Al Margan, A.M.; Albaghrah, F.A.; Al Sharyan, A.M.; Alyami, A.S.M. Assessment of Physicians’ Practice in Implementing Antibiotic Stewardship Program in Najran City, Saudi Arabia: A Cross-Sectional Study. Pharmacy 2024, 12, 24. https://doi.org/10.3390/pharmacy12010024
Alqahtani NS, Bilal MM, Al Margan AM, Albaghrah FA, Al Sharyan AM, Alyami ASM. Assessment of Physicians’ Practice in Implementing Antibiotic Stewardship Program in Najran City, Saudi Arabia: A Cross-Sectional Study. Pharmacy. 2024; 12(1):24. https://doi.org/10.3390/pharmacy12010024
Chicago/Turabian StyleAlqahtani, Nasser Saeed, Maha Mohammed Bilal, Albatoul M. Al Margan, Fatimah Ahmad Albaghrah, Anwar Mana Al Sharyan, and Aljawharh Salem M. Alyami. 2024. "Assessment of Physicians’ Practice in Implementing Antibiotic Stewardship Program in Najran City, Saudi Arabia: A Cross-Sectional Study" Pharmacy 12, no. 1: 24. https://doi.org/10.3390/pharmacy12010024
APA StyleAlqahtani, N. S., Bilal, M. M., Al Margan, A. M., Albaghrah, F. A., Al Sharyan, A. M., & Alyami, A. S. M. (2024). Assessment of Physicians’ Practice in Implementing Antibiotic Stewardship Program in Najran City, Saudi Arabia: A Cross-Sectional Study. Pharmacy, 12(1), 24. https://doi.org/10.3390/pharmacy12010024