
Knowledge and Attitudes of Cannabidiol in Croatia among Students, Physicians, and Pharmacists

 , , , ,
, , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Surveys Design
2.2. Statistical Analysis
3. Results
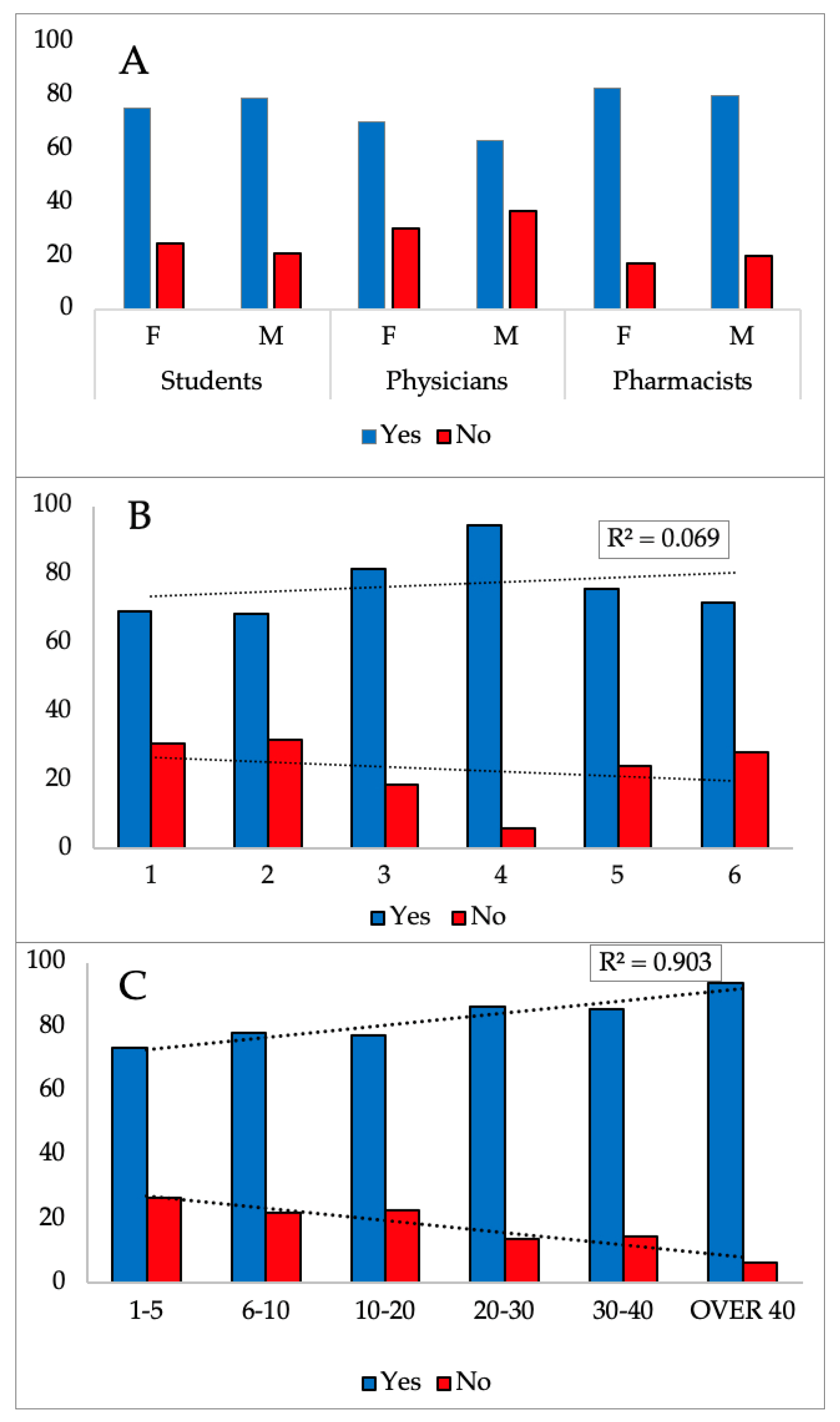
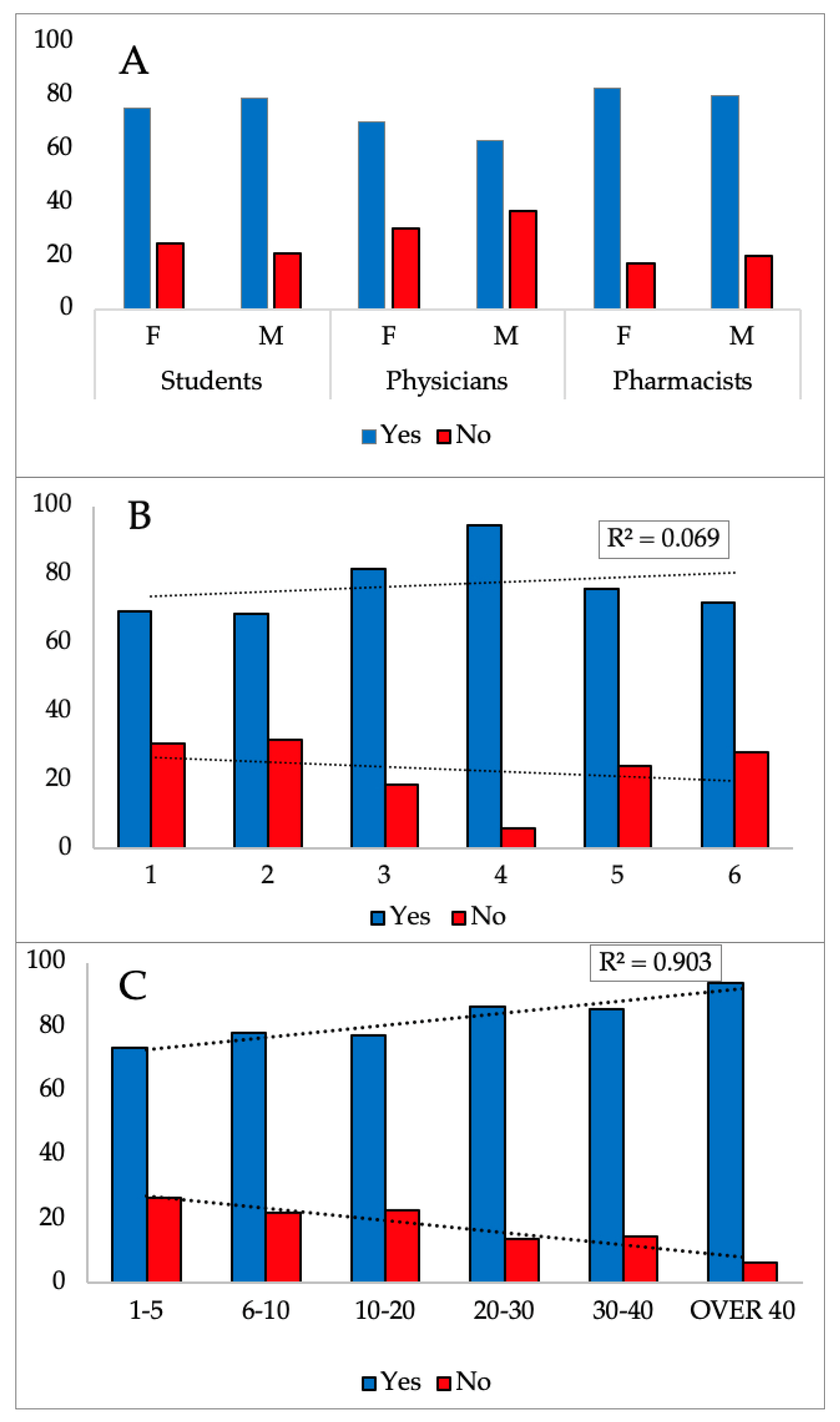
3.1. Demographic Data
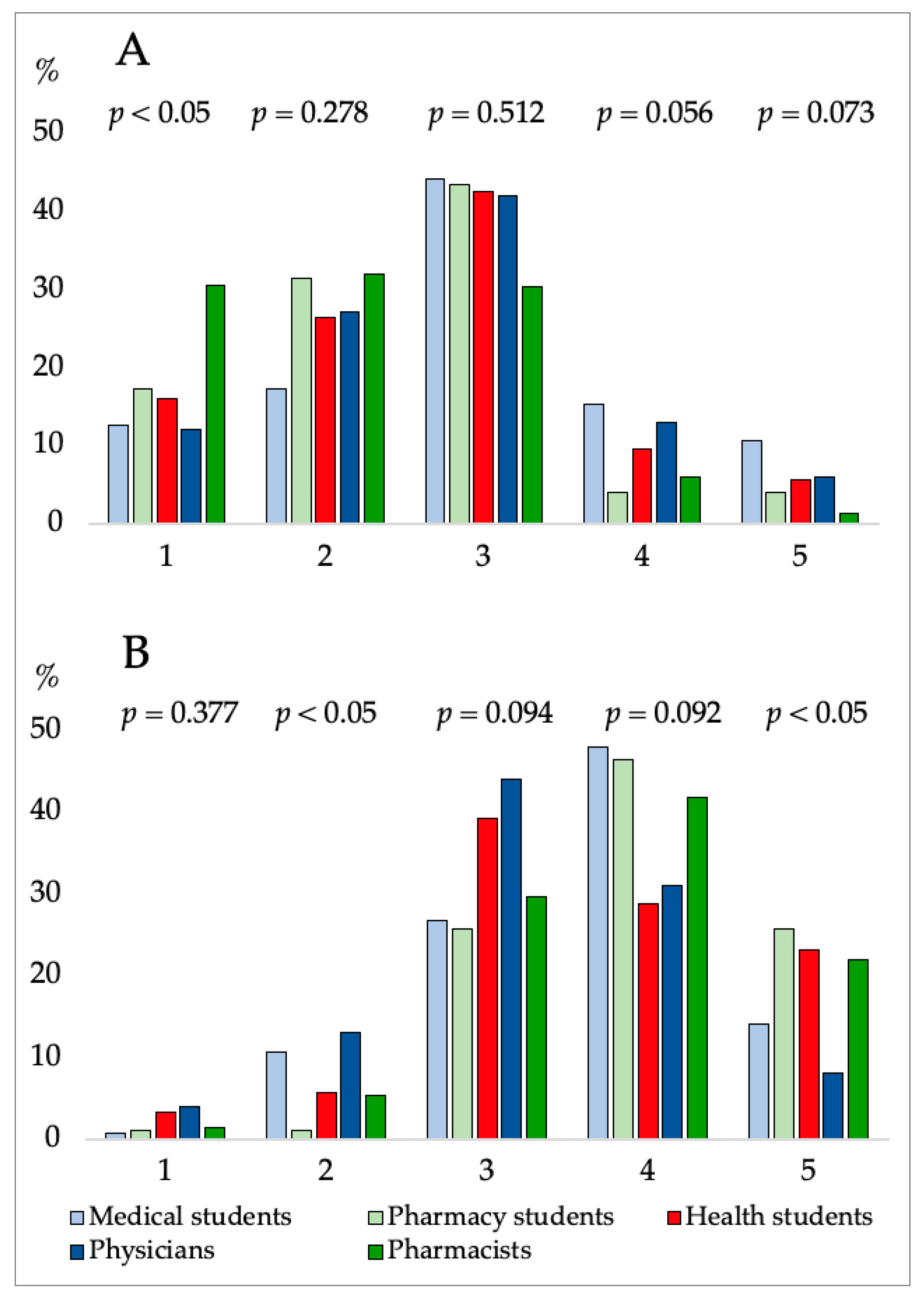
3.2. Results of Respondent’s Knowledge about CBD
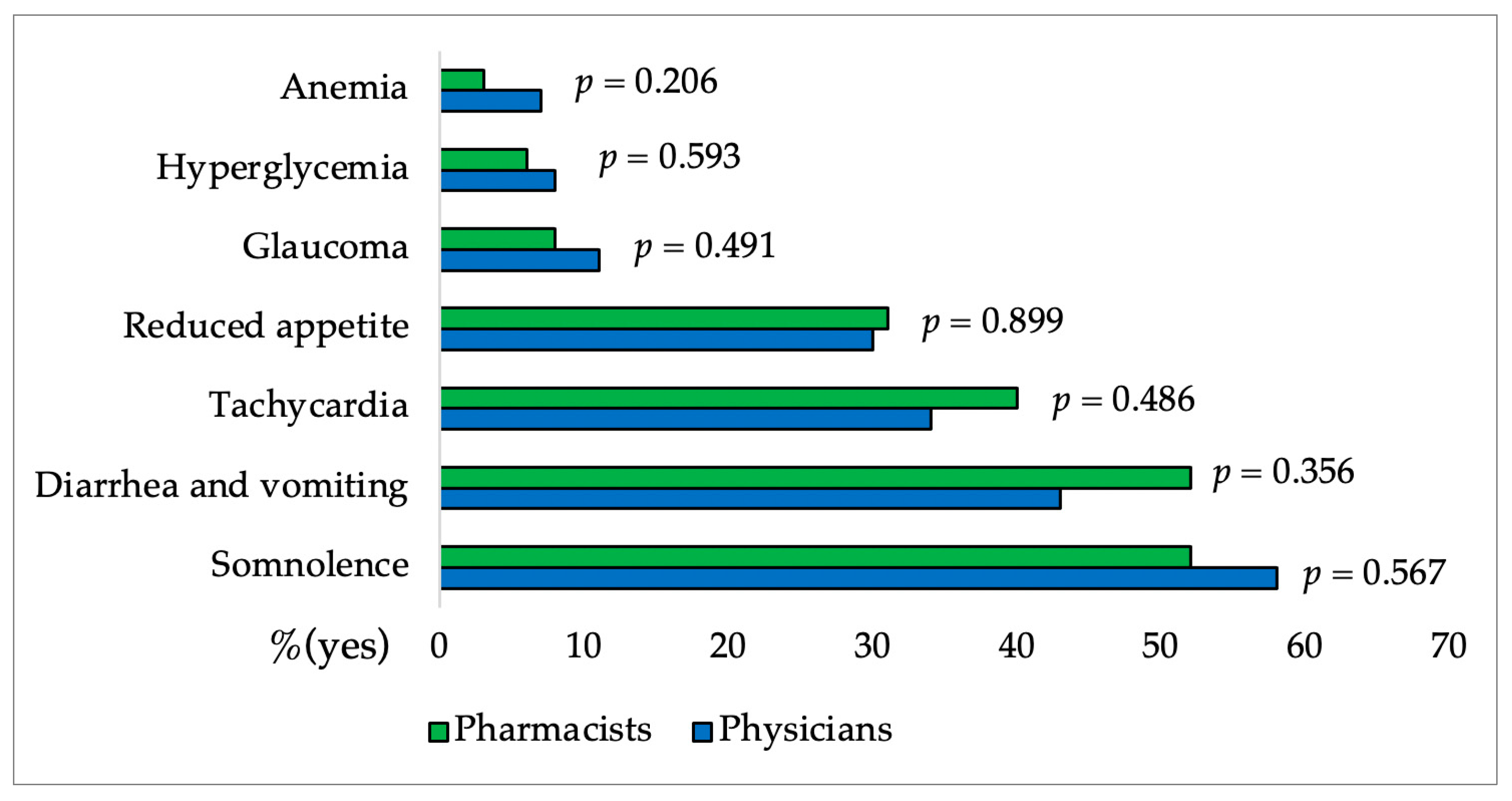
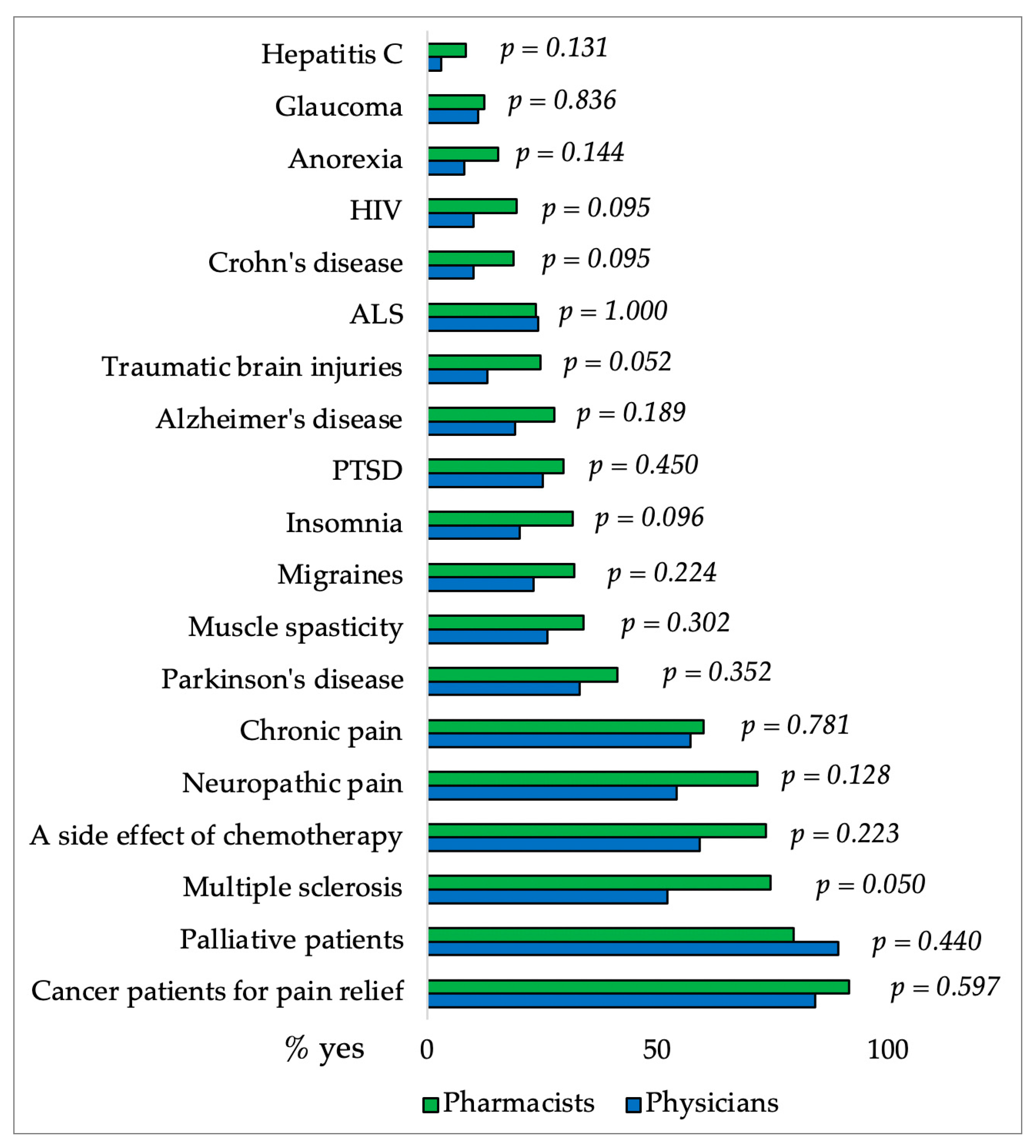
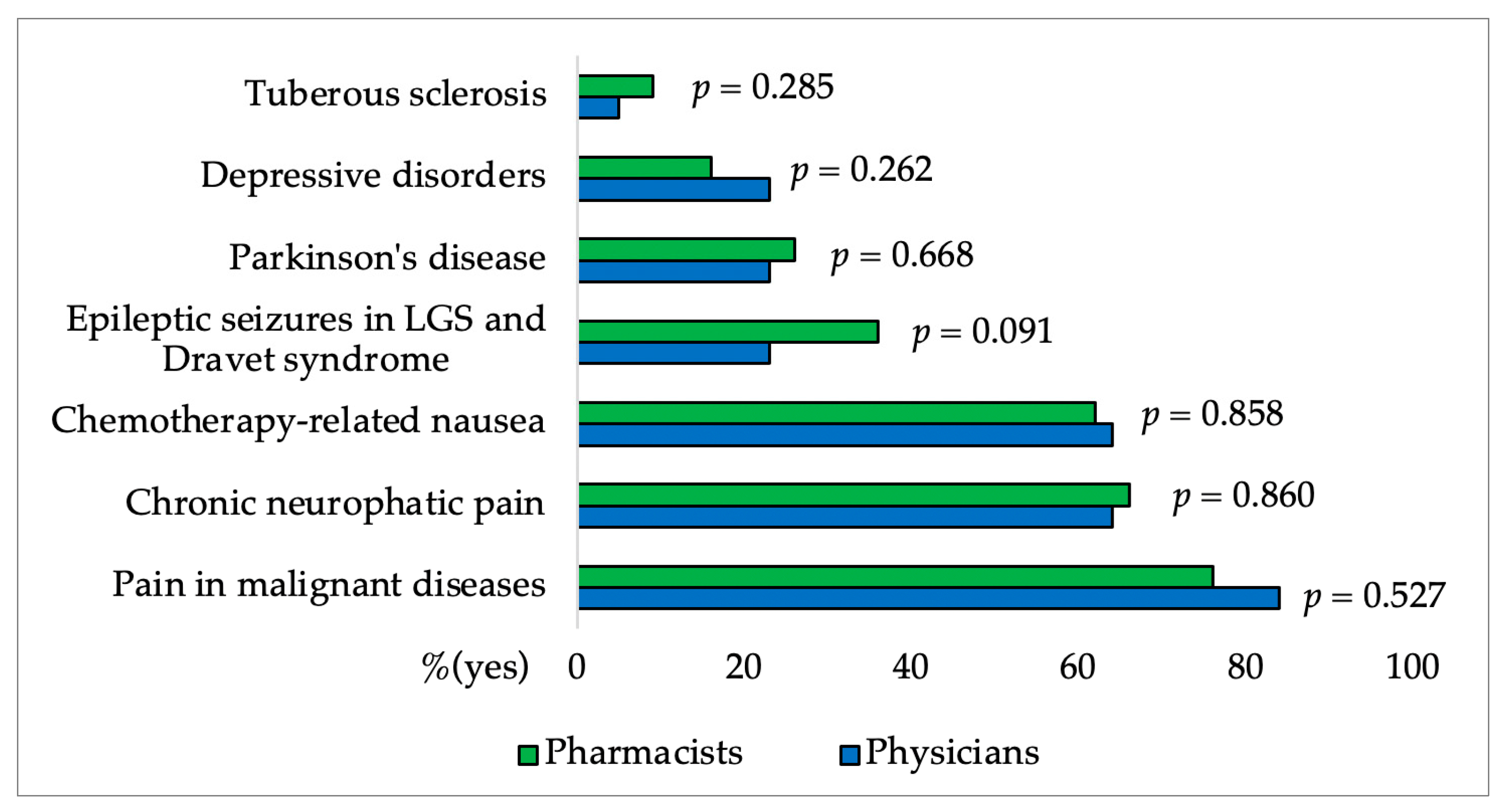
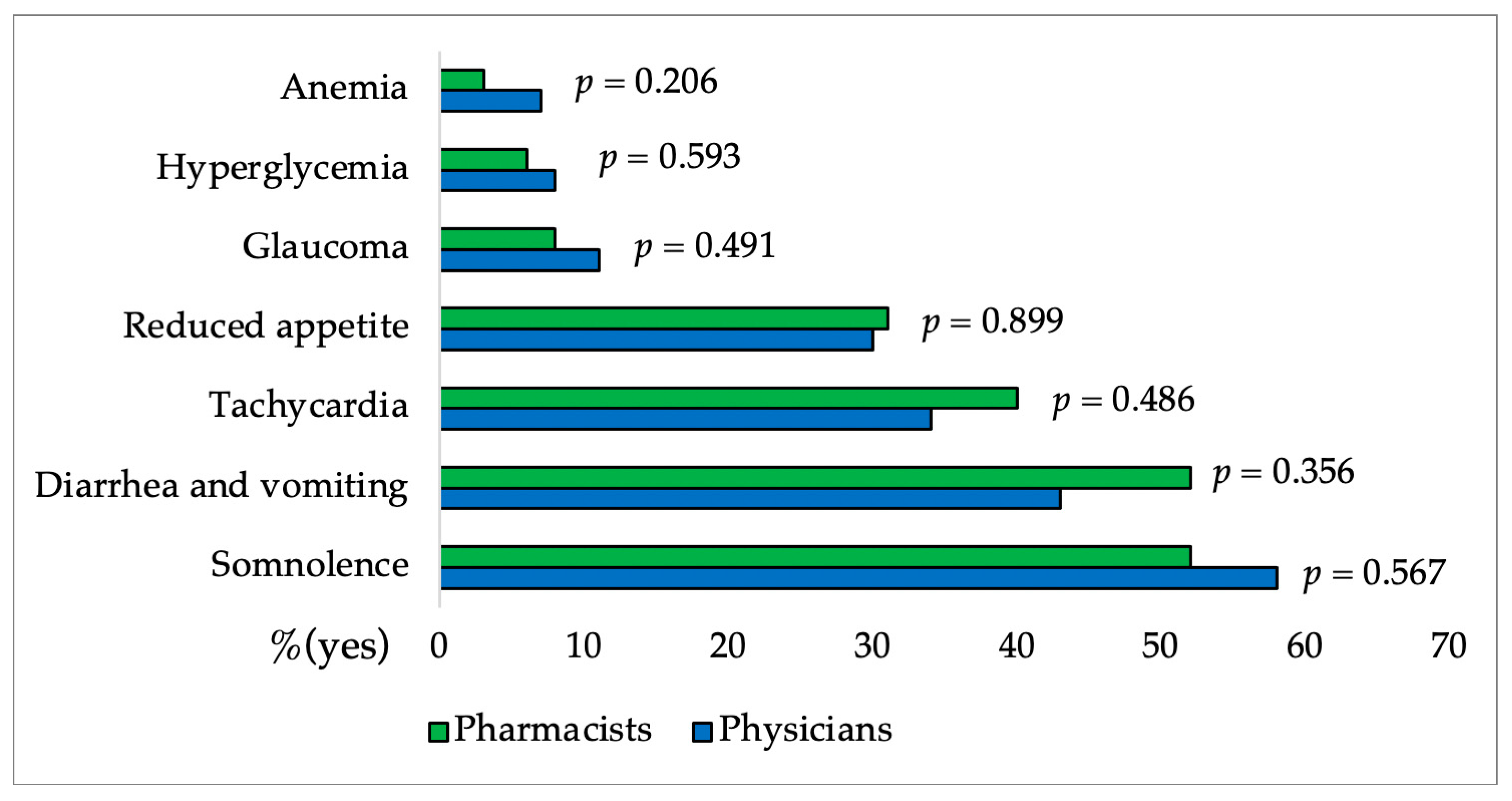
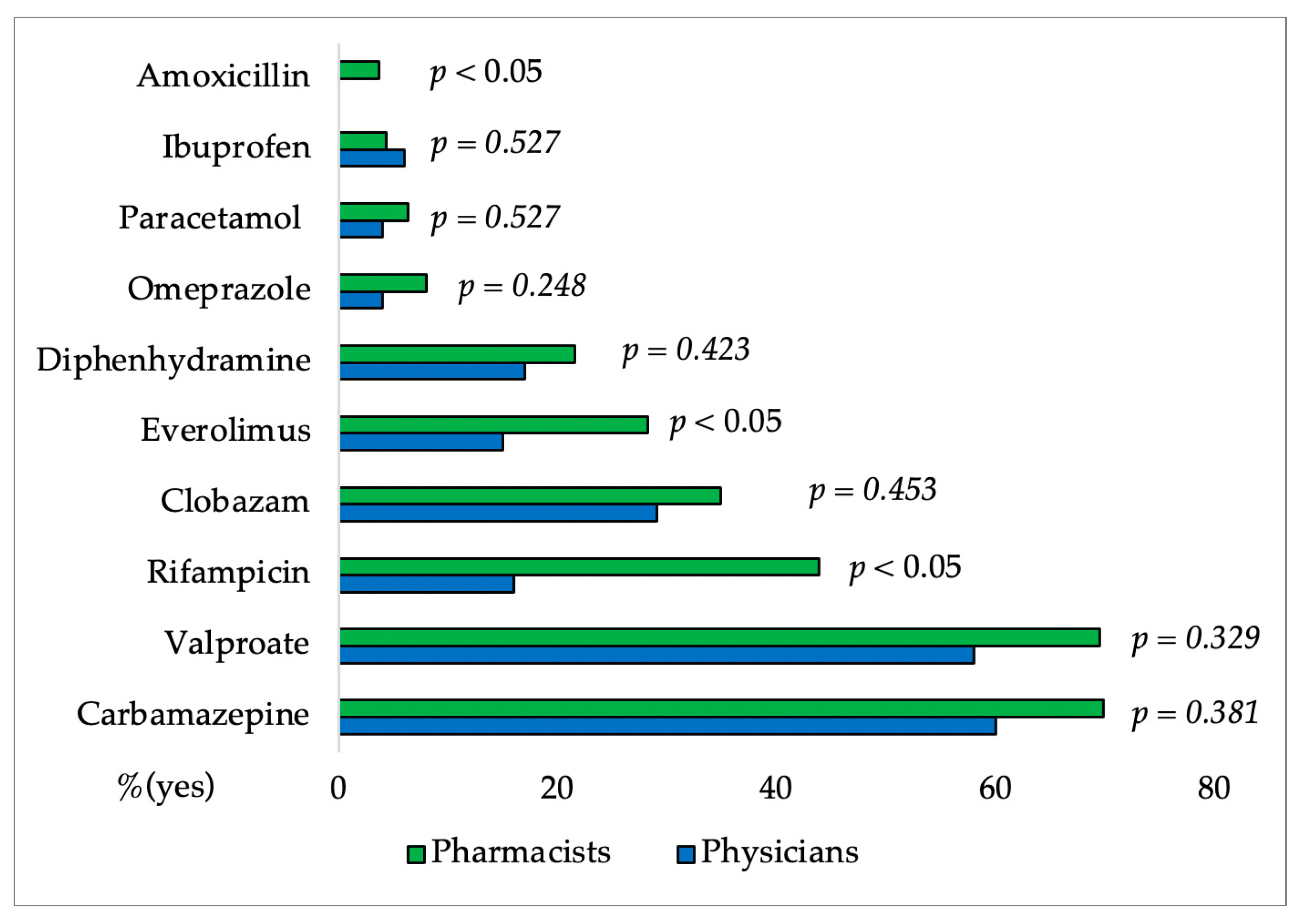
3.3. Results of the Questionnaire Presented Only for Physicians’ and Pharmacists’
4. Discussion
4.1. Questions Presented in Both Questionnaires
4.2. Specific Knowledge of CBD among Physicians and Pharmacists
4.3. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Helmer, S.M.; Mikolajczyk, R.T.; McAlaney, J.; Vriesacker, B.; Van Hal, G.; Akvardar, Y.; Guillen-Grima, F.; Salonna, F.; Stock, C.; Dempsey, R.C.; et al. Illicit substance use among university students from seven European countries: A comparison of personal and perceived peer use and attitudes towards illicit substance use. Prev. Med. 2014, 67, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Moeller, K.E.; McGuire, J.M.; Melton, B.L. A nationwide survey of pharmacy students’ knowledge and perceptions regarding medical cannabis. J. Am. Pharm. Assoc. 2020, 60, 218–224.e213. [Google Scholar] [CrossRef] [PubMed]
- Radwan, M.M.; ElSohly, M.A.; El-Alfy, A.T.; Ahmed, S.A.; Slade, D.; Husni, A.S.; Manly, S.P.; Wilson, L.; Seale, S.; Cutler, S.J.; et al. Isolation and Pharmacological Evaluation of Minor Cannabinoids from High-Potency Cannabis sativa. J. Nat. Prod. 2015, 78, 1271–1276. [Google Scholar] [CrossRef] [PubMed]
- Bhamra, S.K.; Desai, A.; Imani-Berendjestanki, P.; Horgan, M. The emerging role of cannabidiol (CBD) products; a survey exploring the public’s use and perceptions of CBD. Phytother. Res. 2021, 35, 5734–5740. [Google Scholar] [CrossRef] [PubMed]
- Calabrese, E.J.; Rubio-Casillas, A. Biphasic effects of THC in memory and cognition. Eur. J. Clin. Investig. 2018, 48, e12920. [Google Scholar] [CrossRef] [PubMed]
- Chesney, E.; Oliver, D.; Green, A.; Sovi, S.; Wilson, J.; Englund, A.; Freeman, T.P.; McGuire, P. Adverse effects of cannabidiol: A systematic review and meta-analysis of randomized clinical trials. Neuropsychopharmacology 2020, 45, 1799–1806. [Google Scholar] [CrossRef] [PubMed]
- Taylor, L.; Gidal, B.; Blakey, G.; Tayo, B.; Morrison, G. A Phase I, Randomized, Double-Blind, Placebo-Controlled, Single Ascending Dose, Multiple Dose, and Food Effect Trial of the Safety, Tolerability and Pharmacokinetics of Highly Purified Cannabidiol in Healthy Subjects. CNS Drugs 2018, 32, 1053–1067. [Google Scholar] [CrossRef]
- Goodman, S.; Wadsworth, E.; Schauer, G.; Hammond, D. Use and Perceptions of Cannabidiol Products in Canada and in the United States. Cannabis Cannabinoid Res. 2022, 7, 355–364. [Google Scholar] [CrossRef]
- Levinsohn, E.A.; Hill, K.P. Clinical uses of cannabis and cannabinoids in the United States. J. Neurol. Sci. 2020, 411, 116717. [Google Scholar] [CrossRef]
- Casanova, C.; Ramier, C.; Fortin, D.; Carrieri, P.; Mancini, J.; Barre, T. Cannabidiol use and perceptions in France: A national survey. BMC Public Health 2022, 22, 1628. [Google Scholar] [CrossRef]
- FDA and Cannabis: Research and Drug Approval Process. Available online: https://www.fda.gov/news-events/public-health-focus/fda-and-cannabis-research-and-drug-approval-process (accessed on 22 July 2023).
- Bazzari, F.H.; Bazzari, A.H. Attitudes and Knowledge Regarding the Therapeutic Use of Cannabinoids among Community Pharmacists: A Pilot Cross-Sectional Study in Amman, Jordan. Healthcare 2023, 11, 694. [Google Scholar] [CrossRef] [PubMed]
- Abu-Sawwa, R.; Chase, A.; Fowowe, O.; Park, Y. Effects of Epidiolex (Cannabidiol) on seizure-related emergency department visits and hospital admissions: A retrospective cohort study. Epilepsy Behav. 2022, 127, 108538. [Google Scholar] [CrossRef] [PubMed]
- Cooper, Z.D.; Comer, S.D.; Haney, M. Comparison of the analgesic effects of dronabinol and smoked marijuana in daily marijuana smokers. Neuropsychopharmacology 2013, 38, 1984–1992. [Google Scholar] [CrossRef] [PubMed]
- Epidyolex. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/epidyolex (accessed on 22 July 2023).
- Sativex. Available online: https://www.ema.europa.eu/en/medicines/human/paediatric-investigation-plans/emea-000181-pip02-13-m01 (accessed on 23 July 2023).
- Khalsa, J.H.; Bunt, G.; Blum, K.; Maggirwar, S.B.; Galanter, M.; Potenza, M.N. Review: Cannabinoids as Medicinals. Curr. Addict. Rep. 2022, 9, 630–646. [Google Scholar] [CrossRef] [PubMed]
- Zeraatkar, D.; Cooper, M.A.; Agarwal, A.; Vernooij, R.W.M.; Leung, G.; Loniewski, K.; Dookie, J.E.; Ahmed, M.M.; Hong, B.Y.; Hong, C.; et al. Long-term and serious harms of medical cannabis and cannabinoids for chronic pain: A systematic review of non-randomised studies. BMJ Open 2022, 12, e054282. [Google Scholar] [CrossRef] [PubMed]
- Batinic, A.; Sutlović, D.; Kuret, S.; Matana, A.; Kumric, M.; Bozic, J.; Dujic, Z. Trial of a Novel Oral Cannabinoid Formulation in Patients with Hypertension: A Double-Blind, Placebo-Controlled Pharmacogenetic Study. Pharmaceuticals 2023, 16, 645. [Google Scholar] [CrossRef] [PubMed]
- Batinic, A.; Sutlovic, D.; Kuret, S.; Burcul, F.; Kalajzic, N.; Matana, A.; Dujic, G.; Vrdoljak, J.; Kumric, M.; Bozic, J.; et al. Differences in Plasma Cannabidiol Concentrations in Women and Men: A Randomized, Placebo-Controlled, Crossover Study. Int. J. Mol. Sci. 2023, 24, 10273. [Google Scholar] [CrossRef]
- Patrician, A.; Versic-Bratincevic, M.; Mijacika, T.; Banic, I.; Marendic, M.; Sutlovic, D.; Dujic, Z.; Ainslie, P.N. Examination of a New Delivery Approach for Oral Cannabidiol in Healthy Subjects: A Randomized, Double-Blinded, Placebo-Controlled Pharmacokinetics Study. Adv. Ther. 2019, 36, 3196–3210. [Google Scholar] [CrossRef]
- Dujic, G.; Kumric, M.; Vrdoljak, J.; Dujic, Z.; Bozic, J. Chronic Effects of Oral Cannabidiol Delivery on 24-h Ambulatory Blood Pressure in Patients with Hypertension (HYPER-H21-4): A Randomized, Placebo-Controlled, and Crossover Study. Cannabis Cannabinoid Res. 2023. Epub ahead of print. [Google Scholar] [CrossRef]
- Dragun, T.; Brown, C.V.; Tulppo, M.P.; Obad, A.; Dujić, Ž. The Influence of Oral Cannabidiol on 24-h Ambulatory Blood Pressure and Arterial Stiffness in Untreated Hypertension: A Double-Blind, Placebo-Controlled, Cross-Over Pilot Study. Adv. Ther. 2023, 40, 3495–3511. [Google Scholar] [CrossRef]
- HALMED: Baza Lijekova: Epidyolex. Available online: https://www.halmed.hr/Lijekovi/Baza-lijekova/Epidyolex/15646/ (accessed on 23 July 2023).
- Miller, O.S.; Elder, E.J., Jr.; Jones, K.J.; Gidal, B.E. Analysis of cannabidiol (CBD) and THC in nonprescription consumer products: Implications for patients and practitioners. Epilepsy Behav. 2022, 127, 108514. [Google Scholar] [CrossRef] [PubMed]
- Wysota, C.N.; Le, D.; Clausen, M.E.; Ciceron, A.C.; Fuss, C.; Bennett, B.; Romm, K.F.; Duan, Z.; Berg, C.J. Young adults’ knowledge, perceptions and use of cannabidiol products: A mixed-methods study. Health Educ. Res. 2022, 37, 379–392. [Google Scholar] [CrossRef] [PubMed]
- Schilling, J.M.; Hughes, C.G.; Wallace, M.S.; Sexton, M.; Backonja, M.; Moeller-Bertram, T. Cannabidiol as a Treatment for Chronic Pain: A Survey of Patients’ Perspectives and Attitudes. J. Pain Res. 2021, 14, 1241–1250. [Google Scholar] [CrossRef] [PubMed]
- Felnhofer, A.; Kothgassner, O.D.; Stoll, A.; Klier, C. Knowledge about and attitudes towards medical cannabis among Austrian university students. Complement. Ther. Med. 2021, 58, 102700. [Google Scholar] [CrossRef] [PubMed]
- Spinella, T.C.; Bartholomeusz, J.; Stewart, S.H.; Barrett, S.P. Perceptions about THC and CBD effects among adults with and without prior cannabis experience. Addict. Behav. 2023, 137, 107508. [Google Scholar] [CrossRef]
- Stayduhar, J.M.; Covvey, J.R.; Schreiber, J.B.; Witt-Enderby, P.A. Pharmacist and Student Knowledge and Perceptions of Herbal Supplements and Natural Products. Pharmacy 2023, 11, 96. [Google Scholar] [CrossRef]
- Jacobs, R.J.; Colon, J.; Kane, M.N. Medical Students’ Attitudes, Knowledge, and Beliefs about Medical Cannabis: A Qualitative Descriptive Study. Cureus 2022, 14, e28336. [Google Scholar] [CrossRef]
- Kruger, D.J.; Mokbel, M.A.; Clauw, D.J.; Boehnke, K.F. Assessing Health Care Providers’ Knowledge of Medical Cannabis. Cannabis Cannabinoid Res. 2022, 7, 501–507. [Google Scholar] [CrossRef]
- Bawa, Z.; Saini, B.; McCartney, D.; Bedoya-Perez, M.; McLachlan, A.J.; McGregor, I.S. A cross-sectional survey exploring the knowledge, experiences and attitudes of Australian pharmacists toward medicinal cannabis. Int. J. Clin. Pharm. 2023, 45, 375–386. [Google Scholar] [CrossRef]
- Philpot, L.M.; Ebbert, J.O.; Hurt, R.T. A survey of the attitudes, beliefs and knowledge about medical cannabis among primary care providers. BMC Fam. Pract. 2019, 20, 17. [Google Scholar] [CrossRef]
- Emmerling, S.; Martin, B.; Schmitz, N. A survey of Wisconsin pharmacists about cannabinoid products: Are we ready to recommend? J. Am. Pharm. Assoc. 2021, 61, e71–e75. [Google Scholar] [CrossRef] [PubMed]
- Chung, A.K.; Tse, C.Y.; Law, J.K. Attitudes and beliefs of medical students on cannabis in Hong Kong. Complement. Ther. Med. 2022, 70, 102870. [Google Scholar] [CrossRef] [PubMed]
- Szaflarski, M.; McGoldrick, P.; Currens, L.; Blodgett, D.; Land, H.; Szaflarski, J.P.; Segal, E. Attitudes and knowledge about cannabis and cannabis-based therapies among US neurologists, nurses, and pharmacists. Epilepsy Behav. 2020, 109, 107102. [Google Scholar] [CrossRef] [PubMed]
- King, D.D.; DeCarlo, M.; Mylott, L.; Yarossi, M. Cannabis knowledge gaps in nursing education: Pilot testing cannabis curriculum. Teach. Learn. Nurs. 2023, 18, 474–479. [Google Scholar] [CrossRef]
- Patel, S.; Doroudgar, S.; Ip, E.J. Community pharmacists’ lack of knowledge and confidence in non-prescription cannabidiol products. Res. Soc. Adm. Pharm. RSAP 2021, 17, 1356–1360. [Google Scholar] [CrossRef] [PubMed]
- Gardiner, K.M.; Singleton, J.A.; Sheridan, J.; Kyle, G.J.; Nissen, L.M. Health professional beliefs, knowledge, and concerns surrounding medicinal cannabis—A systematic review. PLoS ONE 2019, 14, e0216556. [Google Scholar] [CrossRef]
- Karanges, E.A.; Suraev, A.; Elias, N.; Manocha, R.; McGregor, I.S. Knowledge and attitudes of Australian general practitioners towards medicinal cannabis: A cross-sectional survey. BMJ Open 2018, 8, e022101. [Google Scholar] [CrossRef]
- Nichols, M.A.; Arnett, S.J.; Fa, B.; Marchionda, R.A.; Cutting, M.C.; McDonald, M.R.; Miller, M.L. National survey identifying community pharmacist preceptors’ experience, knowledge, attitudes, and behaviors influencing intent to recommend cannabidiol products. J. Am. Pharm. Assoc. 2021, 61, S91–S104. [Google Scholar] [CrossRef]
- Kruger, D.J.; Gerlach, J.; Kruger, J.S.; Mokbel, M.A.; Clauw, D.J.; Boehnke, K.F. Physicians’ Attitudes and Practices Regarding Cannabis and Recommending Medical Cannabis Use. Cannabis Cannabinoid Res. 2023. Epub ahead of print. [Google Scholar] [CrossRef]
- Sharma, P.; Holland, A.; Sheikh, T.; Novy, B.; Oesterle, T.; Platt, R.; Hammond, C.J. Primary care provider attitudes, experiences and practices about cannabidiol (CBD) and barriers to patient-provider communication about CBD use: A qualitative study. PEC Innov. 2022, 1, 100044. [Google Scholar] [CrossRef]
- Caligiuri, F.J.; Ulrich, E.E.; Welter, K.J. Pharmacy Student Knowledge, Confidence and Attitudes Toward Medical Cannabis and Curricular Coverage. Am. J. Pharm. Educ. 2018, 82, 6296. [Google Scholar] [CrossRef] [PubMed]
- Eysenbach, G. Improving the quality of Web surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J. Med. Internet Res. 2004, 6, e34. [Google Scholar] [CrossRef] [PubMed]
- SurveyMonkey Inc. Available online: https://www.surveymonkey.com/mp/sample-size-calculator/ (accessed on 11 June 2023).
- Croatian Bureau of Statistics. Students Enrolled on Professional and University Study in Winter Semester, According to Place of Permanent Residence, Academic Year; Croatian Bureau of Statistics: Zagreb, Croatia, 2023; Available online: https://podaci.dzs.hr/hr/statistika-u-nizu/ (accessed on 17 September 2023).
- Croatian Chamber of Pharmacists. Register of Pharmacists. Zagreb, Croatia. Available online: https://www.hljk.hr/registar-ljekarnika-s36 (accessed on 18 September 2023).
- Croatian Medical Chamber. Digital Atlas of Croatian Medicine. Zagreb, Croatia. Available online: https://www.hlk.hr/digitalni-atlas-hrvatskog-lijecnistva.aspx (accessed on 18 September 2023.).
- Fedorova, E.V.; Wong, C.F.; Ataiants, J.; Iverson, E.; Conn, B.M.; Lankenau, S.E. Cannabidiol (CBD) and other drug use among young adults who use cannabis in Los Angeles. Drug Alcohol. Depend. 2021, 221, 108648. [Google Scholar] [CrossRef] [PubMed]
- Sultan, S.R.; O’Sullivan, S.E.; England, T.J. The effects of acute and sustained cannabidiol dosing for seven days on the haemodynamics in healthy men: A randomised controlled trial. Br. J. Clin. Pharmacol. 2020, 86, 1125–1138. [Google Scholar] [CrossRef]
- McNabb, M.; Durante, K.A.; Trocchio, S.; Ritter, D.J.; MacCaffrie, R.; Brum, A.; Mandile, S.; White, S. Self-reported Medicinal Cannabis Use as an Alternative to Prescription and Over-the-counter Medication Use Among US Military Veterans. Clin. Ther. 2023, 45, 562–577. [Google Scholar] [CrossRef]
- Weisman, J.M.; Rodriguez, M. A systematic review of medical students’ and professionals’ attitudes and knowledge regarding medical cannabis. J. Cannabis Res. 2021, 3, 47. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Question Category | Physicians’ and Pharmacist’ Questionnaire | Students’ Questionnaire |
|---|---|---|
| General | Gender, profession, specialization, years of work in practice, county of residence | Gender, study program, year of study |
| Questions represented in both questionnaires | ||
| Knowledge self-assessment | Do you have knowledge about CBD? Through my formal education, I had an education about CBD. I think that I need more education about CBD. I am aware of CBD use risks. I am aware of CBD use benefits. | |
| Researcher-assessed knowledge | CBD is bad for health. CBD treatment is efficacious. CBD has positive effects on physical health. CBD has positive effects on mental health. CBD helps patients with chronically debilitating conditions. CBD is physically addictive. CBD is psychologically addictive. Using CBD can lead to addiction to other opioids and drugs. CBD causes a feeling of euphoria. Have you ever read a scientific paper about CBD? | |
| CBD experience | Have you ever consumed CBD? | |
| Attitudes about CBD use | The educational curricula of Physicians, health professionals, and pharmacists should include subjects on the use of CBD for medical purposes. | |
| Questions presented in physicians’ and pharmacists’ questionnaire only | ||
| Knowledge self-assessment | I believe that I have enough knowledge about the use of CBD for medical purposes and that I can recommend it to patients. | |
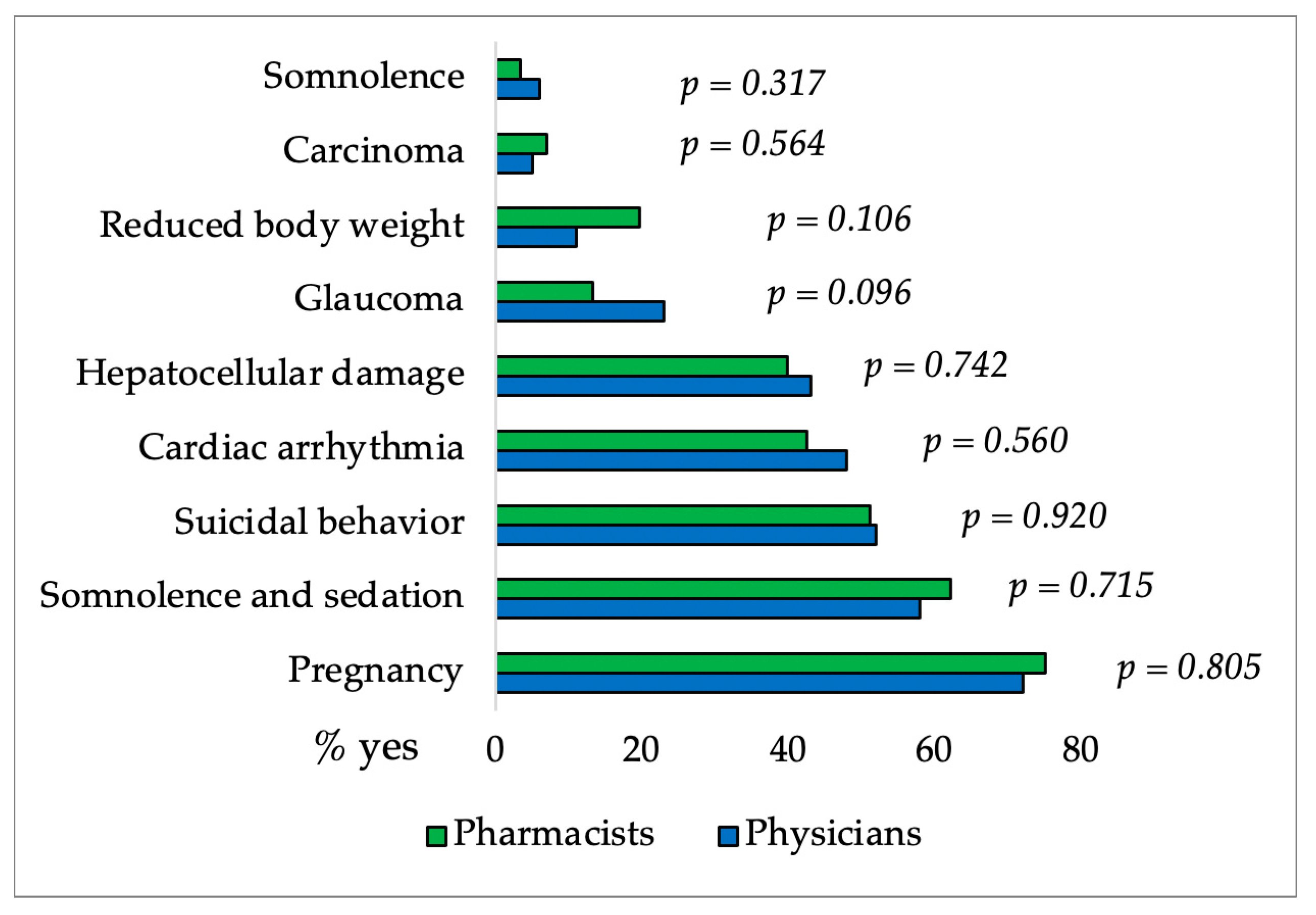
| Researcher-assessed knowledge | FDA has approved CBD drugs for nausea associated with chemotherapy, chronic neuropathic pain, EPI attacks in Lennox-Gastaut and Dravet syndrome, depressive disorders, Parkinson’s disease, tuberous sclerosis, and pain in malignant diseases. ** Side effects of CBD are anemia, tachycardia, diarrhea and vomiting, glaucoma, decreased appetite, hyperglycemia, and somnolence. ** Medications that have moderate or severe interactions with CBD include: paracetamol, valproat, omeprazole, karbamazepin, ibuprofen, rifampicin, amoksicilin, everolimus, klobazam, fehidramin. ** Conditions that require caution when using CBD are cardiac arrhythmia, hepatocellular damage, glaucoma, somnolence, cancer, reduced body weight, pregnancy, suicidal behaviour, somnolence, and sedation. ** | |
| CBD experience | Have you ever recommended/prescribed CBD to your patients? | |
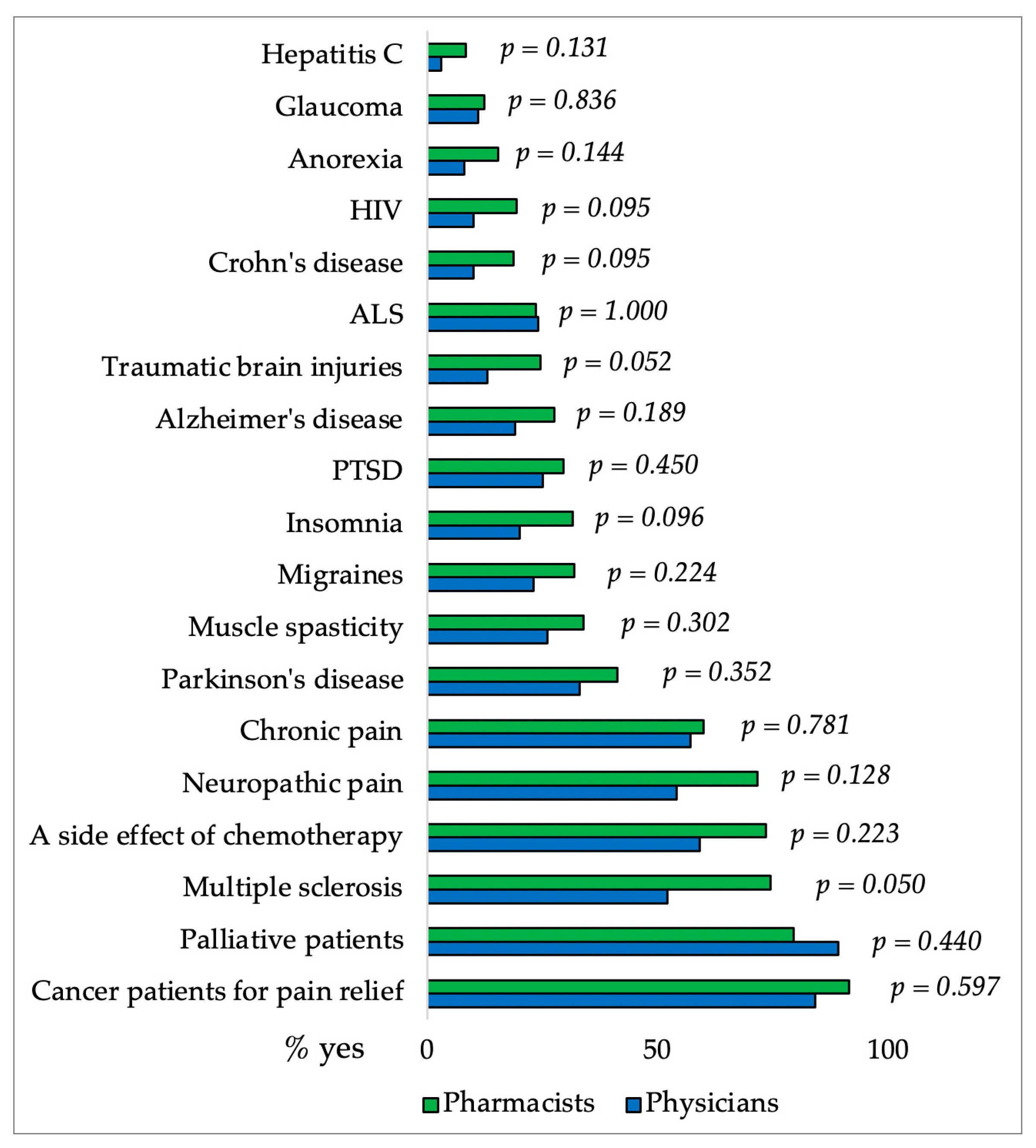
| Attitudes about CBD use | I support the use of CBD in palliative patients, cancer pain relief, side effects of chemotherapy, multiple sclerosis, neuropathic pain, chronic pain, PTSD, insomnia, Crohn’s disease, glaucoma, hepatitis C, muscle spasticity, HIV, traumatic brain injury, ALS, Alzheimer’s disease, anorexia, Parkinson’s disease, migraine. ** I believe that recommending/prescribing CBD could reduce the use of opioids in chronic pain. I believe that health insurance should cover the cost of CBD if a doctor prescribes it as therapy. | |
| Variable | Students N (%) | Physicians’ and Pharmacists’ N (%) | Difference between Groups χ2 Test | |
|---|---|---|---|---|
| Gender | F | 372 (78.6) | 326 (81.3) | p = 0.330 |
| M | 101 (21.4) | 75 (18.7) | ||
| Study program | Medical | 150 (31.7) | - | |
| Pharmacy | 198 (41.9) | - | ||
| Health | 125 (26.4) | - | ||
| Year of study program Medical 1–6; Pharmacy 1–5 | 1 | 111 (23.5) | - | |
| 2 | 92 (19.5) | - | ||
| 3 | 92 (19.5) | - | ||
| 4 | 71 (15.0) | - | ||
| 5 | 50 (10.6) | - | ||
| 6 | 57 (12.1) | - | ||
| Years of work in practice physicians’/pharmacists’ (N = 401) | 1–5 | - | 135 (33.7) | |
| 6–10 | - | 50 (12.5) | ||
| 11–20 | - | 101 (25.2) | ||
| 21–30 | - | 65 (16.2) | ||
| 31–40 | - | 34 (8.5) | ||
| >40 | - | 16 (4.0) | ||
| Do you have knowledge about CBD? | Yes | 361 (76.3) | 316 (78.8) | p = 0.382 |
| No | 112 (23.7) | 85 (21.2) | ||
| Through my formal education, I had an education about CBD. | Yes | 127 (26.8) | 90 (22.4) | p = 0.136 |
| No | 346 (73.2) | 311 (77.6) | ||
| Have you ever read a scientific paper about CBD? | Yes | 83 (17.5) | 187 (46.6) | p < 0.05 |
| No | 390 (82.5) | 214 (53.4) | ||
| Have you ever consumed CBD? | Yes | 120 (25.4) | 65 (16.2) | p < 0.05 |
| No | 353 (74.6) | 336 (83.8) | ||
| The educational curricula of Physicians, health professionals, and pharmacists should include subjects on The use of CBD for medical purposes. | 1 | 11 (2.3) | 14 (3.5) | p < 0.05 |
| 2 | 15 (3.2) | 9 (2.2) | ||
| 3 | 67 (14.2) | 39 (9.7) | ||
| 4 | 143 (30.2) | 85 (21.2) | ||
| 5 | 237 (50.1) | 254 (63.3) | ||
| I think that I need more education about CBD. | 1 | 17 (3.6) | 10 (2.5) | p < 0.05 |
| 2 | 11 (2.3) | 15 (3.7) | ||
| 3 | 44 (9.3) | 18 (4.5) | ||
| 4 | 108 (22.8) | 61 (15.2) | ||
| 5 | 293 (61.9) | 297 (74.1) | ||
| I am aware of CBD use risks. | 1 | 88 (18.6) | 61 (15.2) | p < 0.05 |
| 2 | 96 (20.3) | 78 (19.5) | ||
| 3 | 140 (29.6) | 157 (39.2) | ||
| 4 | 91 (19.2) | 70 (17.5) | ||
| 5 | 58 (12.3) | 35 (8.7) | ||
| I am aware of CBD use benefits. | 1 | 50 (10.6) | 33 (8.2) | p < 0.05 |
| 2 | 75 (15.9) | 36 (9.0) | ||
| 3 | 144 (30.4) | 162 (40.4) | ||
| 4 | 155 (32.8) | 136 (33.9) | ||
| 5 | 49 (10.4) | 34 (8.5) | ||
| Variable | * Participants Agreement Level | Students N (%) | Physicians’ and Pharmacists’ N (%) | Difference between Groups χ2 Test |
|---|---|---|---|---|
| CBD is bad for health. | 1 | 73 (15.4) | 104 (25.9) | p < 0.05 |
| 2 | 121 (25.6) | 123 (30.7) | ||
| 3 | 205 (43.3) | 133 (33.2) | ||
| 4 | 43 (9.1) | 31 (7.7) | ||
| 5 | 31 (6.6) | 10 (2.5) | ||
| CBD treatment is efficacious. | 1 | 7 (1.5) | 8 (2.0) | p = 0.408 |
| 2 | 25 (5.3) | 29 (7.2) | ||
| 3 | 140 (29.6) | 133 (33.2) | ||
| 4 | 200 (42.3) | 157 (39.2) | ||
| 5 | 101 (21.4) | 74 (18.5) | ||
| CBD has positive effects on physical health. | 1 | 21 (4.4) | 11 (2.7) | p = 0.158 |
| 2 | 37 (7.8) | 29 (7.2) | ||
| 3 | 225 (47.6) | 168 (41.9) | ||
| 4 | 140 (29.6) | 145 (36.2) | ||
| 5 | 50 (10.6) | 48 (12.0) | ||
| CBD has positive effects on mental health. | 1 | 41 (8.7) | 21 (5.2) | p = 0.092 |
| 2 | 75 (15.9) | 49 (12.2) | ||
| 3 | 181 (38.3) | 164 (40.9) | ||
| 4 | 126 (26.6) | 127 (31.7) | ||
| 5 | 50 (10.6) | 40 (10.0) | ||
| CBD helps patients with chronically debilitating conditions. | 1 | 5 (1.1) | 5 (1.2) | p = 0.546 |
| 2 | 18 (3.8) | 12 (3.0) | ||
| 3 | 120 (25.4) | 112 (27.9) | ||
| 4 | 194 (41.0) | 175 (43.6) | ||
| 5 | 136 (28.8) | 97 (24.2) | ||
| CBD is physically addictive. | 1 | 74 (15.6) | 92 (22.9) | p < 0.05 |
| 2 | 98 (20.7) | 89 (22.2) | ||
| 3 | 168 (35.5) | 143 (35.7) | ||
| 4 | 88 (18.6) | 46 (11.5) | ||
| 5 | 45 (9.5) | 31 (7.7) | ||
| CBD is psychologically addictive. | 1 | 40 (8.5) | 71 (17.7) | p < 0.05 |
| 2 | 58 (12.3) | 70 (17.5) | ||
| 3 | 164 (34.7) | 136 (33.9) | ||
| 4 | 125 (26.4) | 77 (19.2) | ||
| 5 | 86 (18.2) | 47 (11.7) | ||
| Using CBD can lead to addiction to other opioids and drugs. | 1 | 87 (18.4) | 126 (31.4) | p < 0.05 |
| 2 | 88 (18.6) | 91 (22.7) | ||
| 3 | 155 (32.8) | 115 (28.7) | ||
| 4 | 87 (18.4) | 38 (9.5) | ||
| 5 | 56 (11.8) | 31 (7.7) | ||
| CBD causes a feeling of euphoria. | 1 | 81 (17.1) | 118 (29.4) | p < 0.05 |
| 2 | 86 (18.2) | 100 (24.9) | ||
| 3 | 177 (37.4) | 126 (31.4) | ||
| 4 | 77 (16.3) | 38 (9.5) | ||
| 5 | 52 (11.0) | 19 (4.7) |
| Variable | Physicians n (%) | Pharmacists n (%) | Differences between Groups (χ2 Test) | |
|---|---|---|---|---|
| Question 25 I believe that recommending/prescribing CBD could reduce the use of opioids in chronic pain. | Yes | 6 (6) | 251 (83.4) | p < 0.05 |
| No | 94 (94) | 50 (16.6) | ||
| Question 26 I believe that I have enough knowledge about the use of CBD for medical purposes and that I can recommend it to patients. | Yes | 6 (6) | 34 (11.3) | p = 0.126 |
| No | 94 (94) | 267 (88.7) | ||
| Question 27 Have you ever recommended/prescribed the use of CBD to patients in your practice so far? | Yes, just once | 5 (5) | 25 (8.3) | p = 0.108 |
| Yes, more than once | 1 (1) | 19 (6.3) | ||
| Yes, often to patients with specific diagnoses | 2 (2) | 7 (2.3) | ||
| No | 92 (92) | 250 (83.1) | ||
| Question 28 I believe that healthcare insurance should cover the cost of CBD if a doctor prescribes it as therapy. | Yes | 83 (83) | 256 (85.0) | p = 0.623 |
| No | 17 (17) | 45 (15.0) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Batinic, A.; Curkovic, A.; Bukic, J.; Žuntar, I.; Kuret, S.; Mimica, B.; Kalajzic, N.; Dujic, G.; Glavaš-Obrovac, L.; Soldo, A.; et al. Knowledge and Attitudes of Cannabidiol in Croatia among Students, Physicians, and Pharmacists. Pharmacy 2024, 12, 2. https://doi.org/10.3390/pharmacy12010002
Batinic A, Curkovic A, Bukic J, Žuntar I, Kuret S, Mimica B, Kalajzic N, Dujic G, Glavaš-Obrovac L, Soldo A, et al. Knowledge and Attitudes of Cannabidiol in Croatia among Students, Physicians, and Pharmacists. Pharmacy. 2024; 12(1):2. https://doi.org/10.3390/pharmacy12010002
Chicago/Turabian StyleBatinic, Ana, Ana Curkovic, Josipa Bukic, Irena Žuntar, Sendi Kuret, Bianka Mimica, Nina Kalajzic, Goran Dujic, Ljubica Glavaš-Obrovac, Ana Soldo, and et al. 2024. "Knowledge and Attitudes of Cannabidiol in Croatia among Students, Physicians, and Pharmacists" Pharmacy 12, no. 1: 2. https://doi.org/10.3390/pharmacy12010002
APA StyleBatinic, A., Curkovic, A., Bukic, J., Žuntar, I., Kuret, S., Mimica, B., Kalajzic, N., Dujic, G., Glavaš-Obrovac, L., Soldo, A., Včeva, A., Dujic, Z., & Sutlovic, D. (2024). Knowledge and Attitudes of Cannabidiol in Croatia among Students, Physicians, and Pharmacists. Pharmacy, 12(1), 2. https://doi.org/10.3390/pharmacy12010002