
Feasibility and Acceptability of an Overdose Prevention Intervention Delivered by Community Pharmacists for Patients Prescribed Opioids for Chronic Non-Cancer Pain

 ,
,  ,
,  , ,
, ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
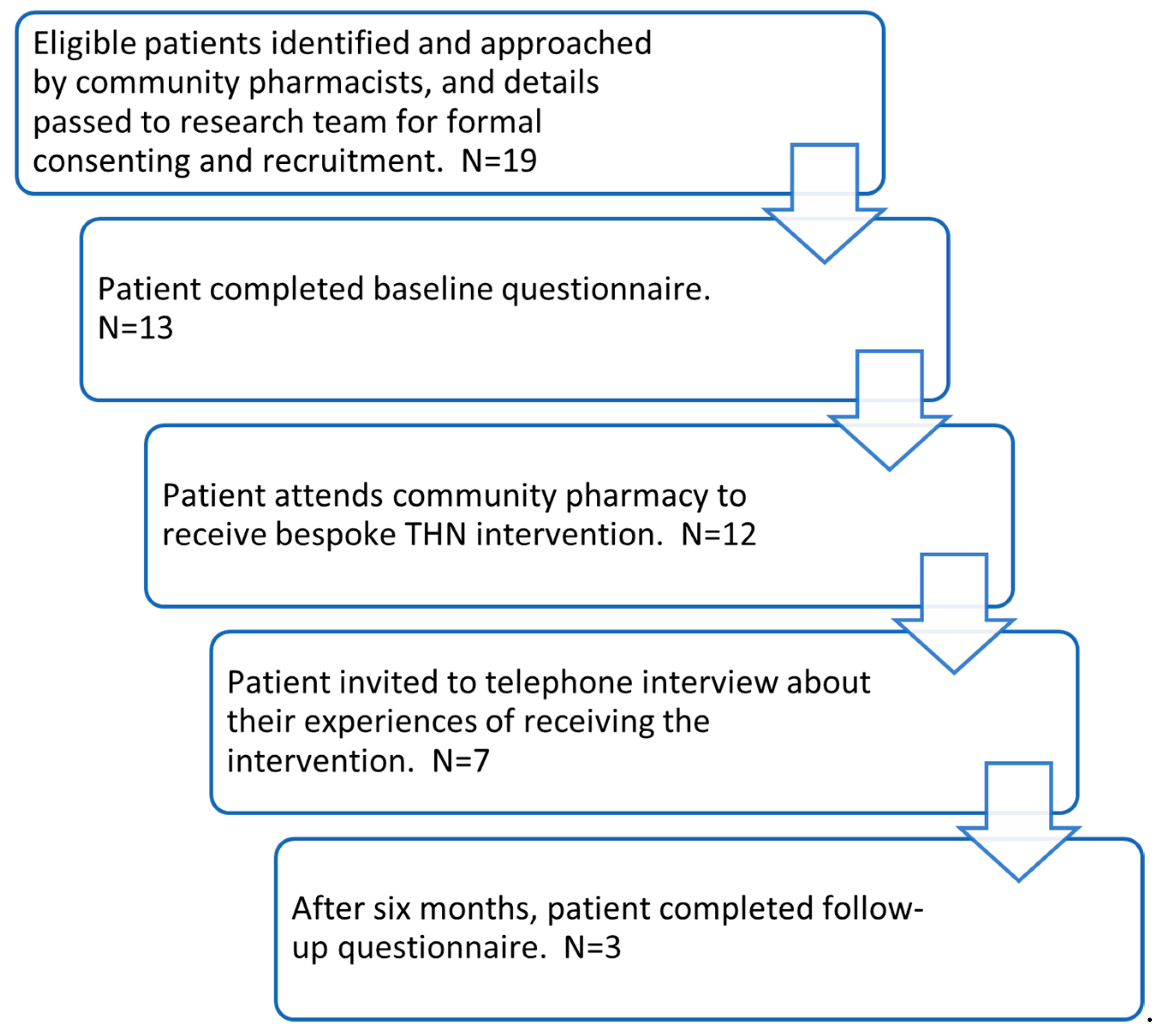
3. Results
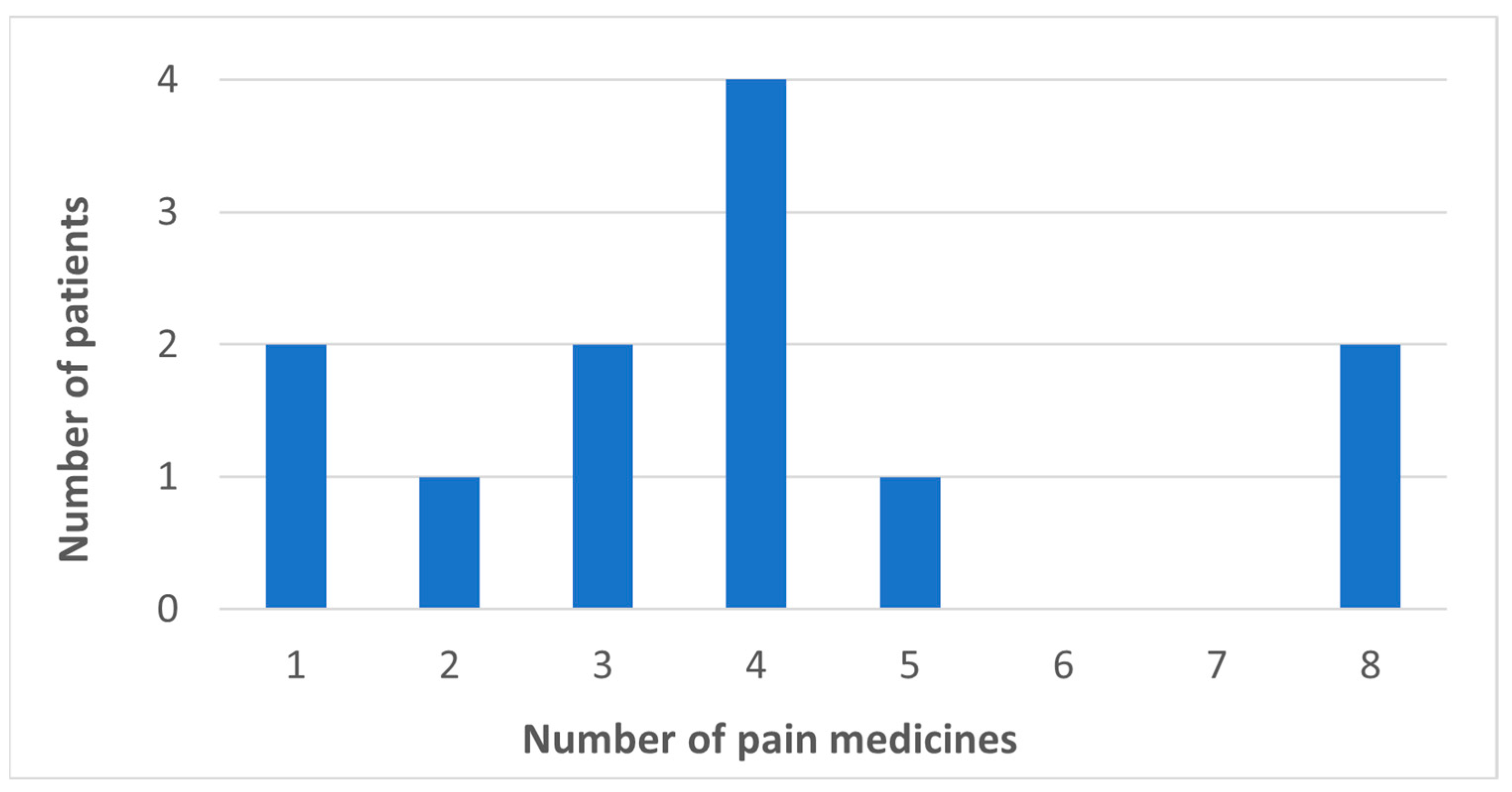
3.1. Patient Characteristics
3.2. Patient Interview Findings
3.2.1. Theme One: Relationship with Health, Medication, and Overdose
I didnae [didn’t] really know the signs and didnae think I needed to know.(W, 67)
It was a big shock because I didn’t really know about anything until the chemist was speaking to me about it […] I didn’t have a clue.(M, 65)
I really don’t feel that I need this […] I personally don’t think that I would even accidentally overdose.(W, 67)
When he said it was to do with drug overuse or drug abuse, naturally you think about drug addicts. […] I thought, well I’m not a drug addict, I don’t inject myself, I don’t abuse my medication.(M, 51)
I wouldn’t have thought that I was at risk of having an overdose, but I am. And I now accept that to a degree.(M, 74)
3.2.2. Theme Two: Experiences and Perceptions of Support
He [the community pharmacist] was very, very good. I mean sometimes I’m hard of hearing and he took his time to explain things because sometimes I’ve to watch people’s lips. He was very informative and straightforward with it. It was very, very relaxed, it really was. And I was under no pressure whatsoever.(M, 51)
I find that the relationship with the pharmacy is much more important to a degree than it is with the GP surgery, particularly so since COVID-19 because of the lockdown procedures.(M, 74)
Can I just say something? I’ve got [redacted to retain anonymity] disorder and my wife is here with me. I’ve got a memory like a sieve and a lot of the time it’s my wife that knows the answer.(M, 47)
It doesn’t just give me peace of mind, it gives my family peace of mind as well.(M, 51)
3.2.3. Theme Three: Perceptions of Intervention and Participation
I would give it ten [out of ten] because he genuinely took his time to sit and explain things to me. And it was such a relaxed atmosphere.(M, 51)
She [community pharmacist] never really told us much about it […] Just spray it up your nose and that was it.(W, 67)
3.3. Pharmacist Interview Findings
3.3.1. Theme One: Healthcare System and Naloxone Perspectives
They [doctors] should be telling their patients about the risks and the side effects, instead of just prescribing them [opioids]. Because I feel that’s what they do a lot of the time. And then they [patients] will come in here and I’ll explain the risks, and they will be like, “Oh the doctor never said.” And some of them are actually a bit wary about going onto the opioids once they hear the risks because you know it’s, it can’t, well, obviously it’s quite dangerous and it causes a lot of death.(Pharmacist one)
There is not much communication between the GPs and pharmacies regarding increasing or decreasing dose. It’s just maybe by chance if you are looking at their file and you see that, “oh you know, that’s different to what they used to be on.” Yeah, it’s not, it’s not quite as obvious as you might hope.(Pharmacist four)
I would say that it was one of the more trickier subjects. It’s not really something we would discuss with people that were on opioids that weren’t like substance misuse. So, like we do that for substance misuse, but not for people who take prescribed opioid drugs.(Pharmacist two)
3.3.2. Theme Two: Patients’ Risk Awareness and Suitability for the Intervention
So, the patients that we did contact, they received the information very well. They weren’t that knowledgeable, in fact, [that they were] at a higher risk, compared to others, of opioid overdose.(Pharmacist two)
A lot of the recruits that I managed to get were on tramadol. And at least two if not three of those recruits were very surprised to learn that tramadol was morphine-based. So that was a bit of a shock to those recruits.(Pharmacist three)
Quite a large number of patients who I identified as being eligible for the study, were, in fact, delivery patients, and so we didn’t really have a lot of face-to-face contact with them. And I think that I probably swayed towards excluding those from the study because I didn’t feel like talking to them over the phone would have allowed proper engagement and proper understanding to be achieved.(Pharmacist three)
3.3.3. Theme Three: Perceptions of Intervention Content and Delivering the Intervention
It was, all in all, a very positive experience. And just feeling that I was helping them as well for something potentially if it was to go wrong in the future. I had given them that little bit of help.(Pharmacist four)
The EHC—[the emergency hormonal contraception provision] contract—does attract a fee I think of £25 or £30, or whatever it is per consultation. So, probably given the time it takes to have a conversation about their prescription opioids, that would probably be a fair remuneration for a patient.(Pharmacist three)
The intervention went perfectly well, and they were able to understand, but I think having them hold it [the demonstration intranasal spray] in their hands and being able to practice what it feels like […] I think that might have been beneficial.(Pharmacist four)
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Institute for Health and Care Excellence. Chronic Pain (Primary and Secondary) in over 16s: Assessment of All Chronic Pain and Management of Chronic Primary Pain; NICE: London, UK, 2021. [Google Scholar]
- Cohen, S.P.; Vase, L.; Hooten, W.M. Chronic pain: An update on burden, best practices, and new advances. Lancet 2021, 397, 2082–2097. [Google Scholar] [CrossRef] [PubMed]
- Davey, A.; Chilcot, J.; Driscoll, E.; McCracken, L.M. Psychological flexibility, self-compassion and daily functioning in chronic pain. J. Context. Behav. Sci. 2020, 17, 79–85. [Google Scholar] [CrossRef]
- Bannon, S.; Greenberg, J.; Mace, R.A.; Locascio, J.J.; Vranceanu, A.M. The role of social isolation in physical and emotional outcomes among patients with chronic pain. Gen. Hosp. Psychiatry 2021, 69, 50–54. [Google Scholar] [CrossRef] [PubMed]
- Boscarino, J.A.; Kirchner, H.L.; Pitcavage, J.M.; Nadipelli, V.R.; Ronquest, N.A.; Fitzpatrick, M.H.; Han, J.J. Factors associated with opioid overdose: A 10-year retrospective study of patients in a large integrated health care system. Subst. Abus. Rehabil. 2016, 7, 131–141. [Google Scholar] [CrossRef]
- Schofield, J.; Steven, D.; Foster, R.; Matheson, C.; Baldacchino, A.; McAuley, A.; Parkes, T. Quantifying prescribed high dose opioids in the community and risk of overdose. BMC Public Health 2021, 21, 1174. [Google Scholar] [CrossRef]
- Wu, L.T.; Ghitza, U.E.; Burns, A.L.; Mannelli, P. The opioid overdose epidemic: Opportunities for pharmacists. Subst. Abus. Rehabil. 2017, 8, 53–55. [Google Scholar] [CrossRef]
- Busse, J.W.; Wang, L.; Kamaleldin, M.; Craigie, S.; Riva, J.J.; Montoya, L.; Mulla, S.M.; Lopes, L.C.; Vogel, N.; Chen, E.; et al. Opioids for Chronic Noncancer Pain: A Systematic Review and Meta-analysis. JAMA 2018, 320, 2448–2460. [Google Scholar] [CrossRef]
- Bialas, P.; Maier, C.; Klose, P.; Hauser, W. Efficacy and harms of long-term opioid therapy in chronic non-cancer pain: Systematic review and meta-analysis of open-label extension trials with a study duration >/=26 weeks. Eur. J. Pain 2020, 24, 265–278. [Google Scholar] [CrossRef]
- Kurdi, A. Opioids and Gabapentinoids Utilisation and Their Related-Mortality Trends in the United Kingdom Primary Care Setting, 2010-2019: A Cross-National, Population-Based Comparison Study. Front. Pharmacol. 2021, 12, 732345. [Google Scholar] [CrossRef]
- Nury, E.; Schmucker, C.; Nagavci, B.; Motschall, E.; Nitschke, K.; Schulte, E.; Wegwarth, O.; Meerpohl, J.J. Efficacy and safety of strong opioids for chronic noncancer pain and chronic low back pain: A systematic review and meta-analyses. Pain 2022, 163, 610–636. [Google Scholar] [CrossRef]
- Els, C.; Jackson, T.D.; Hagtvedt, R.; Kunyk, D.; Sonnenberg, B.; Lappi, V.G.; Straube, S. High-dose opioids for chronic non-cancer pain: An overview of Cochrane Reviews. Cochrane Database Syst. Rev. 2017, 10, CD012299. [Google Scholar] [CrossRef]
- MHRA. Opioids: Risk of Dependence and Addiction; Medicines and Healthcare Products Regulatory Agency: London, UK, 2020. [Google Scholar]
- Campbell, G.; Nielsen, S.; Bruno, R.; Lintzeris, N.; Cohen, M.; Hall, W.; Larance, B.; Mattick, R.P.; Degenhardt, L. The Pain and Opioids IN Treatment study: Characteristics of a cohort using opioids to manage chronic non-cancer pain. Pain 2015, 156, 231–242. [Google Scholar] [CrossRef]
- Compton, W.M.; Jones, C.M.; Baldwin, G.T. Relationship between Nonmedical Prescription-Opioid Use and Heroin Use. N. Engl. J. Med. 2016, 374, 154–163. [Google Scholar] [CrossRef]
- Wilton, J.; Abdia, Y.; Chong, M.; Karim, M.E.; Wong, S.; MacInnes, A.; Balshaw, R.; Zhao, B.; Gomes, T.; Yu, A.; et al. Prescription opioid treatment for non-cancer pain and initiation of injection drug use: Large retrospective cohort study. BMJ 2021, 375, e066965. [Google Scholar] [CrossRef]
- Coffin, P.O.; Rowe, C.; Oman, N.; Sinchek, K.; Santos, G.M.; Faul, M.; Bagnulo, R.; Mohamed, D.; Vittinghoff, E. Illicit opioid use following changes in opioids prescribed for chronic non-cancer pain. PLoS ONE 2020, 15, e0232538. [Google Scholar] [CrossRef]
- Campbell, G.; Noghrehchi, F.; Nielsen, S.; Clare, P.; Bruno, R.; Lintzeris, N.; Cohen, M.; Blyth, F.; Hall, W.; Larance, B.; et al. Risk factors for indicators of opioid-related harms amongst people living with chronic non-cancer pain: Findings from a 5-year prospective cohort study. EClinicalMedicine 2020, 28, 100592. [Google Scholar] [CrossRef]
- John, W.S.; Wu, L.T. Chronic non-cancer pain among adults with substance use disorders: Prevalence, characteristics, and association with opioid overdose and healthcare utilization. Drug Alcohol Depend. 2020, 209, 107902. [Google Scholar] [CrossRef]
- Witkiewitz, K.; Vowles, K.E. Alcohol and Opioid Use, Co-Use, and Chronic Pain in the Context of the Opioid Epidemic: A Critical Review. Alcohol Clin. Exp. Res. 2018, 42, 478–488. [Google Scholar] [CrossRef]
- Scottish Drugs Forum. Older People with Drug Problems in Scotland: Addressing the Needs of an Ageing Population; Scottish Drugs Forum: Glasgow, UK, 2017. [Google Scholar]
- Jones, W.; Kaoser, R.; Fischer, B. Patterns, trends and determinants of medical opioid utilization in Canada 2005-2020: Characterizing an era of intensive rise and fall. Subst. Abus. Treat. Prev. Policy 2021, 16, 65. [Google Scholar] [CrossRef]
- National Records of Scotland. Drug-Related Deaths in Scotland in 2020; National Records of Scotland: Edinburgh, UK, 2021. Available online: https://www.nrscotland.gov.uk/files//statistics/drug-related-deaths/20/drug-related-deaths-20-pub.pdf (accessed on 18 December 2022).
- McAuley, A.; Best, D.; Taylor, A.; Hunter, C.; Robertson, R. From evidence to policy: The Scottish national naloxone programme. Drugs Educ. Prev. Policy 2012, 19, 309–319. [Google Scholar] [CrossRef]
- NHS Scotland. Quality Prescribing for Chronic Pain 2018–2021; Scottish Government: Edinburgh, UK, 2018.
- Matheson, C.; Thiruvothiyur, M.; Robertson, H.; Bond, C. Community pharmacy services for people with drug problems over two decades in Scotland: Implications for future development. Int. J. Drug Policy 2016, 27, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Moustaqim-Barrette, A.; Papamihali, K.; Mamdani, Z.; Williams, S.; Buxton, J.A. Accessing Take-Home Naloxone in British Columbia and the role of community pharmacies: Results from the analysis of administrative data. PLoS ONE 2020, 15, e0238618. [Google Scholar] [CrossRef] [PubMed]
- Royal Pharmaceutical Society. Pharmacy’s Role in Reducing Harms and Preventing Drug Deaths (Scotland); Royal Pharmaceutical Society: Edinburgh, UK, 2021. [Google Scholar]
- Parkes, T.; Foster, R.; McAuley, A.; Steven, D.; Matheson, C.; Baldacchino, A. Chronic pain, prescribed opioids and overdose risk: A qualitative exploration of the views of affected individuals and family members. Drugs Educ. Prev. Policy 2022, 30, 229–240. [Google Scholar] [CrossRef]
- Volpe, I.; Nielsen, S.; Manning, V.; Savic, M.; McMaugh, J. Overdose Prevention Information for People Prescribed Opioids for Chronic Pain: Enhancing Community Pharmacists’ Capacity to Respond; Monash University: Clayton, Australia, 2020. [Google Scholar]
- NHS Scotland. Information about Near Me for Professionals. Available online: https://www.nearme.scot/information-about-near-me-for-professionals (accessed on 18 December 2022).
- Mercer, F.; Parkes, T.; Foster, R.; Steven, D.; McAuley, A.; Baldacchino, A.; Steele, W.; Schofield, J.; Matheson, C. Patient, family members and community pharmacists’ views of a proposed overdose prevention intervention delivered in community pharmacies for patients prescribed high-strength opioids for chronic non-cancer pain: An explorative intervention development study. Drug Alcohol Rev. 2023, 42, 517–526. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. British National Formulary. Available online: https://bnf.nice.org.uk (accessed on 21 February 2022).
- Knisely, J.S.; Wunsch, M.J.; Cropsey, K.L.; Campbell, E.D. Prescription Opioid Misuse Index: A brief questionnaire to assess misuse. J. Subst. Abus. Treat. 2008, 35, 380–386. [Google Scholar] [CrossRef]
- Nielsen, S. Maximising Opioid Safety. Available online: https://www.monash.edu/__data/assets/pdf_file/0008/2315159/June2020-Naloxone-Patient-Leaflet.pdf (accessed on 13 February 2022).
- Skivington, K.; Matthews, L.; Simpson, S.A.; Craig, P.; Baird, J.; Blazeby, J.M.; Boyd, K.A.; Craig, N.; French, D.P.; McIntosh, E.; et al. A new framework for developing and evaluating complex interventions: Update of Medical Research Council guidance. BMJ 2021, 374, n2061. [Google Scholar] [CrossRef]
- Cochran, G.; Bacci, J.L.; Ylioja, T.; Hruschak, V.; Miller, S.; Seybert, A.L.; Tarter, R. Prescription opioid use: Patient characteristics and misuse in community pharmacy. J. Am. Pharm. Assoc. 2016, 56, 248–256.e246. [Google Scholar] [CrossRef]
- Nielsen, S.; Peacock, A.; Lintzeris, N.; Bruno, R.; Larance, B.; Degenhardt, L. Knowledge of Opioid Overdose and Attitudes to Supply of Take-Home Naloxone Among People with Chronic Noncancer Pain Prescribed Opioids. Pain Med. 2018, 19, 533–540. [Google Scholar] [CrossRef]
- National Records of Scotland. Drug-Related Deaths in Scotland in 2021: Data; National Records of Scotland: Edinburgh, UK, 2022. Available online: https://www.nrscotland.gov.uk/files//statistics/drug-related-deaths/21/drug-related-deaths-21-tabs-figs.xlsx (accessed on 21 February 2022).
- National Records of Scotland. Drug-Related Deaths in Scotland in 2021: Additional Analyses; National Records of Scotland: Edinburgh, UK, 2022. [Google Scholar]
- Dassieu, L.; Paul-Savoie, E.; Develay, E.; Villela Guilhon, A.C.; Lacasse, A.; Guenette, L.; Perreault, K.; Beaudry, H.; Dupuis, L.; Quebec Consortium on Adverse Effects of Pain, M. Swallowing the pill of adverse effects: A qualitative study of patients’ and pharmacists’ experiences and decision-making regarding the adverse effects of chronic pain medications. Health Expect. 2022, 25, 394–407. [Google Scholar] [CrossRef]
- Mueller, S.R.; Koester, S.; Glanz, J.M.; Gardner, E.M.; Binswanger, I.A. Attitudes Toward Naloxone Prescribing in Clinical Settings: A Qualitative Study of Patients Prescribed High Dose Opioids for Chronic Non-Cancer Pain. J. Gen. Intern. Med. 2017, 32, 277–283. [Google Scholar] [CrossRef]
- Nichols, M.A.; Kepley, K.L.; Rosko, K.S.; Hudmon, K.S.; Curran, G.M.; Ott, C.A.; Snyder, M.E.; Miller, M.L. Community pharmacist-provided opioid intervention frequencies and barriers. J. Am. Pharm. Assoc. 2023, 63, 336–342. [Google Scholar] [CrossRef]
- Tabeefar, H.; Chang, F.; Cooke, M.; Patel, T. Community pharmacists and chronic pain: A qualitative study of experience, perception, and challenges. Can. J. Pain 2020, 4, 29–39. [Google Scholar] [CrossRef]
- MacLure, K.; Stewart, D. A qualitative case study of ehealth and digital literacy experiences of pharmacy staff. Res. Soc. Adm. Pharm. 2018, 14, 555–563. [Google Scholar] [CrossRef]
- Eldridge, S.M.; Lancaster, G.A.; Campbell, M.J.; Thabane, L.; Hopewell, S.; Coleman, C.L.; Bond, C.M. Defining Feasibility and Pilot Studies in Preparation for Randomised Controlled Trials: Development of a Conceptual Framework. PLoS ONE 2016, 11, e0150205. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Drug | Number | Proportion |
|---|---|---|
| Opioid | 12 | 100% |
| Analgesic (paracetamol/ibuprofen) | 7 | 58% |
| Gabapentin/pregabalin | 5 | 42% |
| Antidepressant (e.g., amitriptyline) | 5 | 42% |
| Antihistamine (e.g., promethazine) | 2 | 17% |
| Non-steroidal anti-inflammatory (e.g., diclofenac) | 2 | 17% |
| Antacid/proton pump inhibitor (e.g., omeprazole) | 2 | 17% |
| POMI Risk Factors | Number | Proportion |
|---|---|---|
| Use pain medication more often than is prescribed. | 3 | 25% |
| Need early refills for pain medication. | 3 | 25% |
| Gone to a different doctor or an A&E unit to try to get more pain medication. | 1 | 8% |
| Take a higher dose than prescribed | 0 | 0% |
| Feel high or get a buzz after using pain medication | 0 | 0% |
| Take pain medication because upset, or to relieve or cope with problems other than pain. | 0 | 0% |
| Condition | Diagnosed But Not Being Treated | Diagnosed and Being Treated | ||
|---|---|---|---|---|
| Cardiovascular | 1 | 8% | 4 | 33% |
| Respiratory | 2 | 17% | 6 | 50% |
| Renal | 1 | 8% | 0 | 0% |
| Sleep apnoea | 0 | 0% | 2 | 17% |
| Liver | 2 | 17% | 0 | 0% |
| Alcohol/drug problem | 0 | 0% | 0 | 0% |
| Patient Identifier (Gender and Age) | |||
|---|---|---|---|
| M 74 | M 51 | M 72 | |
| Please tell us what you thought about the information you received | |||
| How helpful did you find the information overall? | Very | Very | Extremely |
| How easy to understand was the printed/online information? | Extremely | Very | Extremely |
| How easy to understand was the information provided by the community pharmacist? | Very | Extremely | Extremely |
| The information was relevant to me | Extremely | Moderately | A little |
| The information will be relevant to other people who are prescribed opioids. | Extremely | Extremely | Very |
| To what extent do you agree or disagree with the following statements? | |||
| I learned new things about the risk of prescription opioid overdose. | Agree | Agree | Neither agree nor disagree |
| I learned how to reduce my risk of having an overdose. | Neither agree nor disagree | Strongly agree | Neither agree nor disagree |
| I learned what steps someone around me should take if they think I am having an overdose. | Strongly agree | Strongly agree | Strongly agree |
| I am confident talking to people I live with about what they should do if they think I am having an overdose. | Strongly agree | Strongly agree | Does not apply to me |
| The information and naloxone training caused me to feel upset. | Strongly disagree | Strongly disagree | Strongly disagree |
| The information and naloxone training caused someone I live with to feel upset. | Disagree | Strongly disagree | Does not apply to me |
| I would recommend the information and naloxone training to other people who are prescribed opioids. | Strongly agree | Strongly agree | Agree |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schofield, J.; Parkes, T.; Mercer, F.; Foster, R.; Hnízdilová, K.; Matheson, C.; Steele, W.; McAuley, A.; Raeburn, F.; Skea, L.; et al. Feasibility and Acceptability of an Overdose Prevention Intervention Delivered by Community Pharmacists for Patients Prescribed Opioids for Chronic Non-Cancer Pain. Pharmacy 2023, 11, 88. https://doi.org/10.3390/pharmacy11030088
Schofield J, Parkes T, Mercer F, Foster R, Hnízdilová K, Matheson C, Steele W, McAuley A, Raeburn F, Skea L, et al. Feasibility and Acceptability of an Overdose Prevention Intervention Delivered by Community Pharmacists for Patients Prescribed Opioids for Chronic Non-Cancer Pain. Pharmacy. 2023; 11(3):88. https://doi.org/10.3390/pharmacy11030088
Chicago/Turabian StyleSchofield, Joe, Tessa Parkes, Fiona Mercer, Rebecca Foster, Kristina Hnízdilová, Catriona Matheson, Wez Steele, Andrew McAuley, Fiona Raeburn, Lucy Skea, and et al. 2023. "Feasibility and Acceptability of an Overdose Prevention Intervention Delivered by Community Pharmacists for Patients Prescribed Opioids for Chronic Non-Cancer Pain" Pharmacy 11, no. 3: 88. https://doi.org/10.3390/pharmacy11030088
APA StyleSchofield, J., Parkes, T., Mercer, F., Foster, R., Hnízdilová, K., Matheson, C., Steele, W., McAuley, A., Raeburn, F., Skea, L., & Baldacchino, A. (2023). Feasibility and Acceptability of an Overdose Prevention Intervention Delivered by Community Pharmacists for Patients Prescribed Opioids for Chronic Non-Cancer Pain. Pharmacy, 11(3), 88. https://doi.org/10.3390/pharmacy11030088