
Application of Exploratory Factor Analysis and Item Response Theory to Validate NHANES ADL Scale in Patients Reporting Rheumatoid Arthritis

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. ADL Assessment
2.3. Statistical Analysis
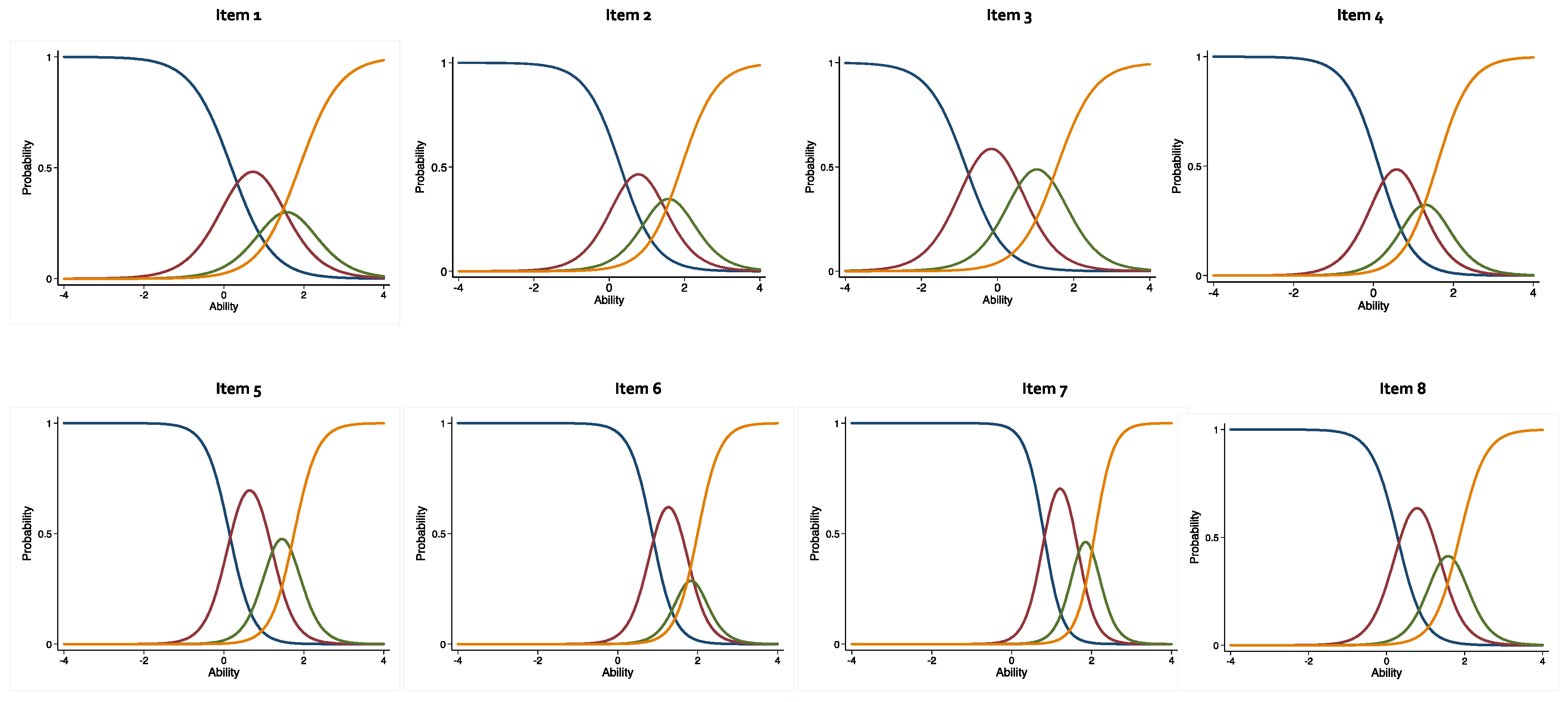
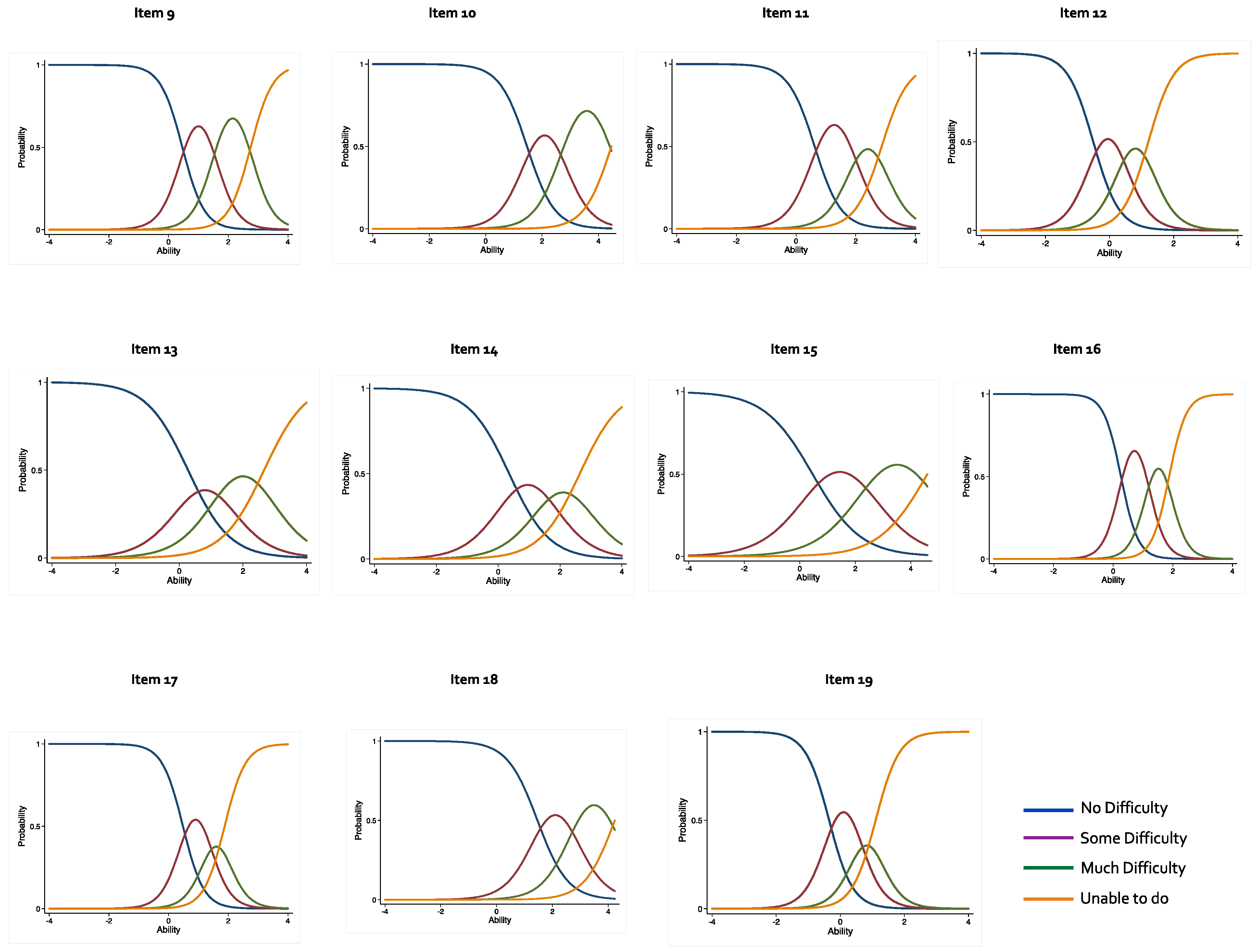
2.4. Item Characteristics Curves (ICC)
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. The NHANES-ADL Questionnaire
| Item | No Difficulty | Some Difficulty | Much Difficulty | Unable to Do |
| 1. Walking for a quarter of a mile; that is about 2 or 3 blocks? | 1 | 2 | 3 | 4 |
| 2. Walking up 10 steps without resting? | 1 | 2 | 3 | 4 |
| 3. Stooping, crouching, kneeling? | 1 | 2 | 3 | 4 |
| 4. Lifting or carrying something as heavy as 10 pounds; like a sack of potatoes or rice? | 1 | 2 | 3 | 4 |
| 5. Doing chores around the house like vacuuming, sweeping, dusting or straightening up? | 1 | 2 | 3 | 4 |
| 6. Preparing your own meals? | 1 | 2 | 3 | 4 |
| 7. Walking from one room to another on the same level? | 1 | 2 | 3 | 4 |
| 8. Standing up from an armless straight chair? | 1 | 2 | 3 | 4 |
| 9. Getting in and out of bed? | 1 | 2 | 3 | 4 |
| 10. Eating, like holding a fork, cutting food or drinking from a glass? | 1 | 2 | 3 | 4 |
| 11. Dressing yourself, including tying shoes, working zippers, and doing buttons? | 1 | 2 | 3 | 4 |
| 12. Standing or being on your feet for about 2 h? | 1 | 2 | 3 | 4 |
| 13. Sitting for about 2 h? | 1 | 2 | 3 | 4 |
| 14. Reaching up over your head? | 1 | 2 | 3 | 4 |
| 15. Using fingers to grasp or handle small objects? | 1 | 2 | 3 | 4 |
| 16. Going out to things like shopping, movies, or sporting events? | 1 | 2 | 3 | 4 |
| 17. Participating in social activities such as visiting friends, attending clubs or meetings, or going to parties? | 1 | 2 | 3 | 4 |
| 18. Doing things to relax at home or for leisure such as reading, watching TV, sewing, or listening to music? | 1 | 2 | 3 | 4 |
| 19. Pushing or pulling large objects like a living room chair? | 1 | 2 | 3 | 4 |
References
- Hunter, T.M.; Boytsov, N.N.; Zhang, X.; Schroeder, K.; Michaud, K.; Araujo, A.B. Prevalence of rheumatoid arthritis in the United States adult population in healthcare claims databases, 2004–2014. Rheumatol Int. 2017, 37, 1551–1557. [Google Scholar] [CrossRef] [PubMed]
- Theis, K.A.; Steinweg, A.; Helmick, C.G.; Courtney-Long, E.; Bolen, J.A.; Lee, R. Which one? what kind? how many? types, causes, and prevalence of disability among U.S. adults. Disabil. Health J. 2019, 12, 411–421. [Google Scholar] [CrossRef] [PubMed]
- Hootman, J.M.; Helmick, C.G.; Barbour, K.E.; Theis, K.A.; Boring, M.A. Updated projected prevalence of self-reported doctor-diagnosed arthritis and arthritis-attributable activity limitation among U.S. adults, 2015–2040. Arthritis. Rheumatol. 2016, 68, 1582–1587. [Google Scholar] [CrossRef] [PubMed]
- Bullock, J.; Rizvi, S.A.A.; Saleh, A.M.; Ahmed, S.S.; Do, D.P.; Ansari, R.A.; Ahmed, J. Rheumatoid Arthritis: A Brief Overview of the Treatment. Med. Princ. Pract. 2018, 27, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Caroline, A. Flurey, Marianne Morris, Pam Richards, Rodney Hughes, Sarah Hewlett, It’s like a juggling act: Rheumatoid arthritis patient perspectives on daily life and flare while on current treatment regimes. Rheumatology 2014, 53, 696–703. [Google Scholar] [CrossRef]
- Malm, K.; Bergman, S.; Andersson, M.L.; Bremander, A.; Larsson, I. Quality of life in patients with established rheumatoid arthritis: A phenomenographic study. SAGE Open Med. 2017, 7, 2050312117713647. [Google Scholar] [CrossRef]
- Martinec, R.; Pinjatela, R.; Balen, D. Quality of life in patients with rheumatoid arthritis—A preliminary study. Acta Clin Croat. 2019, 58, 157–166. [Google Scholar] [CrossRef]
- Barbour, K.E.; Helmick, C.G.; Boring, M.; Brady, T.J. Vital signs: Prevalence of doctor-diagnosed arthritis and arthritis-attributable activity limitation—United States, 2013–2015. Morb. Mortal. Wkly. Rep. 2017, 66, 246–253. [Google Scholar] [CrossRef]
- Maska, L.; Anderson, J.; Michaud, K. Measures of functional status and quality of life in rheumatoid arthritis: Health Assessment Questionnaire Disability Index (HAQ), Modified Health Assessment Questionnaire (MHAQ), Multidimensional Health Assessment Questionnaire (MDHAQ), Health Assessment Questionnaire II (HAQ-II), Improved Health Assessment Questionnaire (Improved HAQ), and Rheumatoid Arthritis Quality of Life (RAQoL). Arthritis. Care Res. 2011, 63, S4–S13. [Google Scholar] [CrossRef]
- Katz, P. Measures of adult general functional status: The Barthel Index, Katz Index of Activities of Daily Living, Health Assessment Questionnaire (HAQ), MACTAR Patient Preference Disability Questionnaire, and Modified Health Assessment Questionnaire (MHAQ). Arthritis Rheumatism 2003, 49, S15–S27. [Google Scholar] [CrossRef]
- Uhlig, T.; Haavardsholm, E.A.; Kvien, T.K. Comparison of the Health Assessment Questionnaire (HAQ) and the modified HAQ (MHAQ) in patients with rheumatoid arthritis. Rheumatology 2006, 45, 454–458. [Google Scholar] [CrossRef] [PubMed]
- Ren, X.S.; Kazis, L.; Meenan, R.F. Short-form Arthritis Impact Measurement Scales 2: Tests of reliability and validity among patients with osteoarthritis. Arthritis. Care Res. 1999, 12, 163–171. [Google Scholar] [CrossRef]
- Suurmeijer, T.P.; Doeglas, D.M.; Moum, T.; Briançon, S.; Krol, B.; Sanderman, R.; Guillemin, F.; Bjelle, A.; van den Heuvel, W.J. The Groningen Activity Restriction Scale for measuring disability: Its utility in international comparisons. Am. J. Public Health 1994, 84, 1270–1273. [Google Scholar] [CrossRef] [PubMed]
- Giambelluca, E.; Panigazzi, M.; Saade, A.; Imbriani, M. Assessment of functional status and rehabilitative strategies in occupational therapy: Role of the Groningen Activity Restriction Questionnaire. Giornale Ital. Med. Lav. Ergon. 2019, 41, 52–57. [Google Scholar]
- Kempen, G.I.; Miedema, I.; Ormel, J.; Molenaar, W. The assessment of disability with the Groningen Activity Restriction Scale. Conceptual framework and psychometric properties. Soc. Sci. Med. 1996, 43, 1601–1610. [Google Scholar] [CrossRef]
- Barber, C.E.H.; Zell, J.; Yazdany, J.; Davis, A.M.; Cappelli, L.; Ehrlich-Jones, L.; Everix, D.; Thorne, J.C.; Bohm, V.; Suter, L.; et al. 2019 American College of Rheumatology Recommended Patient-Reported Functional Status Assessment Measures in Rheumatoid Arthritis. Arthritis Care Res. 2019, 71, 1531–1539. [Google Scholar] [CrossRef]
- Oude Voshaar, M.A.; ten Klooster, P.M.; Taal, E.; van de Laar, M.A. Measurement properties of physical function scales validated for use in patients with rheumatoid arthritis: A systematic review of the literature. Health Qual. Life Outcomes 2011, 9, 99. [Google Scholar] [CrossRef]
- Küçükdeveci, A.A.; Elhan, A.H.; Erdoğan, B.D.; Kutlay, Ş.; Gökmen, D.; Ateş, C.; Yüksel, S.; Lundgren-Nilsson, A.; Escorpizo, R.; Stucki, G.; et al. Use and detailed metric properties of patient-reported outcome measures for rheumatoid arthritis: A systematic review covering two decades. RMD Open. 2021, 7, e001707. [Google Scholar] [CrossRef]
- Lee, J.; Kim, S.H.; Moon, S.H.; Lee, E.H. Measurement properties of rheumatoid arthritis-specific quality-of-life questionnaires: Systematic review of the literature. Qual. Life Res. 2014, 23, 2779–2791. [Google Scholar] [CrossRef]
- Cook, C.E.; Richardson, J.K.; Pietrobon, R.; Braga, L.; Silva, H.M.; Turner, D. Validation of the NHANES ADL scale in a sample of patients with report of cervical pain: Factor analysis, item response theory analysis, and line-item validity. Disabil. Rehabil. 2006, 28, 929–935. [Google Scholar] [CrossRef]
- Cook, C.E.; Richardson, J.K.; Pietrobon, R. Dimensionality, internal consistency, and item analysis of the National Health and Nutrition Examination Surveys activities of daily living instrument among patients with report of low back pain. J. Manip. Physiol. Ther. 2006, 29, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Cook, C.; Pietrobon, R. Item analysis of the NHANES ADL instrument in a sample of patients reporting frequent severe headaches. Physiother. Res. Int. 2006, 11, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Cook, C.E.; Goode, A.; Erb, D.; Richardson, J.K.; Pietrobon, R. Validation of an Item Bank in a Sample of Community-Dwelling Survivors of a Stroke. J. Geriatr. Phys. Therapy 2006, 29, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Terman, S.W.; Burke, J.F. Use of item response theory to investigate disability-related questions in the National Health and Nutrition Examination Survey. SAGE Open Med. 2021, 9, 20503121211012253. [Google Scholar] [CrossRef] [PubMed]
- NHANES—About the National Health and Nutrition Examination Survey. Centers for Disease Control and Prevention. 2017. Available online: https://www.cdc.gov/nchs/nhanes/about_nhanes.htm (accessed on 15 May 2021).
- Centers for Disease Control and Prevention: National health and Nutritional Examination Survey, Interviewer Procedures Manual, March 2017. 2017; Volume 1, p. 568. Available online: https://wwwn.cdc.gov/nchs/data/nhanes/2017-2018/manuals/2017_Interviewer_Procedures_Manual.pdf (accessed on 20 July 2021).
- Centers for Disease Control and Prevention: National health and Nutritional Examination Survey, MEC Interviewers Procedures Manual, January 2017, 1, 515. Available online: https://wwwn.cdc.gov/nchs/data/nhanes/2017-2018/manuals/2017_MEC_Interviewers_Procedures.pdf. (accessed on 22 July 2021).
- National Health and Nutrition Examination Survey: Analytic Guidelines, 2011–2014 and 2015–2016. 14 December 2018. Available online: https://wwwn.cdc.gov/nchs/data/nhanes/analyticguidelines/11-16-analytic-guidelines.pdf (accessed on 18 October 2021).
- Morizot, J.; Ainsworth, A.T.; Reise, S.P. Toward modern psychometrics: Application of item response theory models in personality research. In Handbook of Research Methods in Personality Psychology; Robins, R.W., Fraley, R.C., Krueger, R.F., Eds.; Guilford Press: New York, NY, USA, 2007; pp. 407–423. [Google Scholar]
- Centers for Disease Control and Prevention: National health and Nutritional Examination Survey, Physical Functionality—PFQ. 2012; pp. 1–12. Available online: https://wwwn.cdc.gov/nchs/data/nhanes/2015-2016/questionnaires/PAQ_I.pdf (accessed on 21 October 2021).
- Cortina, J.M. What is coefficient alpha? An examination of theory and applications. J. Appl. Psychol. 1993, 78, 98. [Google Scholar] [CrossRef]
- Kawata, A.K.; Coeytaux, R.R.; Devellis, R.F.; Finkel, A.G.; Mann, J.D.; Kahn, K. Psychometric properties of the HIT-6 among patients in a headache specific practice. Headache 2005, 45, 638–643. [Google Scholar] [CrossRef]
- Yang, F.M.; Kao, S.T. Item response theory for measurement validity. Shanghai Arch. Psychiatry 2014, 26, 171–177. [Google Scholar] [CrossRef]
- Cho, G.; Hwang, H.; Sarstedt, M.; Ringle, C. Cutoff criteria for overall model fit indexes in generalized structured component analysis. J. Market. Anal. 2020, 8, 189–202. [Google Scholar] [CrossRef]
- Adedoyin, O.; Nenty, H.; Chilisa, B. Investigating the invariance of item difficulty parameter estimates based on CTT and IRT. Educ. Res. Rev. 2008, 3, 083–093. [Google Scholar]
- Freedman, V.A.; Kasper, J.D.; Cornman, J.C.; Agree, E.M.; Bandeen-Roche, K.; Mor, V.; Spillman, B.C.; Wallace, R.; Wolf, D.A. Validation of new measures of disability and functioning in the National Health and Aging Trends Study. J. Gerontol. A Biol. Sci. Med. Sci. 2011, 66, 1013–1021. [Google Scholar] [CrossRef]
- McHorney, C.A. Use of item response theory to link 3 modules of functional status items from the asset and health dynamics among the oldest old study. Arch. Phys. Med. Rehabil. 2002, 83, 383–394. [Google Scholar] [CrossRef] [PubMed]
- Kasper, J.D.; Chan, K.S.; Freedman, V.A. Measuring physical capacity: An assessment of a composite measure using self-report and performance-based items. J. Aging Health 2017, 29, 289–309. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | N (%) |
|---|---|
| Age (years) Mean SD | 58.2 ± 0.6 |
| Gender | |
| Male | 468 (41.3%) |
| Female | 664 (58.7%) |
| Race/Ethnicity | |
| Mexican American | 155 (13.7%) |
| Other Hispanic | 126 (11.1%) |
| Non-Hispanic White | 397 (35.1%) |
| Non-Hispanic Black | 346 (30.6%) |
| Other Race-Multiracial | 108 (9.5%) |
| Marital Status | |
| Married | 532 (47.0%) |
| Unmarried | 496 (43.8%) |
| Other | 102 (9.0%) |
| Education Level | |
| <12th Grade | 353 (31.2%) |
| High School Graduate/GED | 273 (24.1%) |
| Some College/AA Degree | 354 (31.3%) |
| College Graduate | 149 (13.2%) |
| Annual Household Income | |
| <$25,000 | 500 (44.2%) |
| $25,000–$49,999 | 289 (25.5%) |
| $50,000–$74,999 | 91 (8.0%) |
| $75,000–$99,000 | 62.0 (5.5%) |
| ≥$100,000 | 104 (9.2%) |
| Health Insurance Coverage | |
| Yes | 1011 (89.3%) |
| No | 118 (10.4%) |
| Item | Factor Loadings |
|---|---|
| Difficulty walking for a quarter mile | 0.536 |
| Difficulty walking up ten stairs | 0.524 |
| Difficulty stooping, crouching, kneeling | 0.592 |
| Difficulty lifting or carrying | 0.616 |
| Difficulty doing house chores | 0.646 |
| Difficulty preparing meals | 0.501 |
| Difficulty walking between rooms | 0.407 |
| Difficulty standing up from armless chair | 0.600 |
| Difficulty getting in and out of bed | 0.635 |
| Difficulty using fork, knife, cup | 0.337 |
| Difficulty dressing yourself | 0.510 |
| Difficulty standing for long periods | 0.661 |
| Difficulty sitting for long periods | 0.634 |
| Difficulty reaching up | 0.491 |
| Difficulty grasp/holding small objects | 0.411 |
| Difficulty going out to movies/events | 0.697 |
| Difficulty attending social event | 0.626 |
| Difficulty with home leisure activities | 0.387 |
| Difficulty moving large objects | 0.726 |
| Item | Discrimination | Difficulty | p-Value | ||
|---|---|---|---|---|---|
| α (SE) | β 1 (SE) | β 2 (SE) | β 3 (SE) | ||
| Difficulty walking for a quarter mile | 1.97 (0.20) | 0.19 (0.09) | 1.26 (0.14) | 1.89 (0.22) | 0.000 |
| Difficulty walking up ten stairs | 2.14 (0.23) | 0.30 (0.10) | 1.24 (0.15) | 1.92 (0.32) | 0.000 |
| Difficulty stooping, crouching, kneeling | 2.02 (0.12) | −0.83 (0.09) | 0.51 (0.06) | 1.56 (0.11) | 0.000 |
| Difficulty lifting or carrying | 2.39 (0.21) | 0.13 (0.08) | 1.02 (0.08) | 1.58 (0.10) | 0.000 |
| Difficulty doing house chores | 3.41 (0.24) | 0.14 (0.08) | 1.15 (0.08) | 1.76 (0.11) | 0.000 |
| Difficulty preparing meals | 3.59 (0.34) | 0.86 (0.08) | 1.67 (0.10) | 2.00 (0.12) | 0.000 |
| Difficulty walking between rooms | 4.31 (0.51) | 0.81 (0.06) | 1.62 (0.09) | 2.08 (0.14) | 0.000 |
| Difficulty standing up from armless chair | 3.00 (0.23) | 0.28 (0.05) | 1.28 (0.08) | 1.87 (0.12) | 0.000 |
| Difficulty getting in and out of bed | 2.72 (0.28) | 0.46 (0.06) | 1.55 (0.09) | 2.75 (0.23) | 0.000 |
| Difficulty using fork, knife, cup | 2.06 (0.24) | 1.47 (0.15) | 2.71 (0.25) | 4.46 (0.62) | 0.000 |
| Difficulty dressing yourself | 2.26 (0.24) | 0.62 (0.06) | 1.94 (0.18) | 2.87 (0.22) | 0.000 |
| Difficulty standing for long periods | 2.49 (0.21) | −0.51 (0.08) | 0.41 (0.06) | 1.21 (0.09) | 0.000 |
| Difficulty sitting for long periods | 1.52 (0.20) | 0.27 (0.08) | 1.34 (0.16) | 2.66 (0.34) | 0.000 |
| Difficulty reaching up | 1.53 (0.16) | 0.35 (0.10) | 1.57 (0.16) | 2.64 (0.23) | 0.000 |
| Difficulty grasp/holding small objects | 1.15 (0.14) | 0.46 (0.12) | 2.42 (0.29) | 4.60 (0.62) | 0.000 |
| Difficulty going out to movies/events | 3.47 (0.27) | 0.26 (0.07) | 1.17 (0.08) | 1.88 (0.11) | 0.000 |
| Difficulty attending social event | 2.86 (0.30) | 0.48 (0.06) | 1.33 (0.08) | 1.88 (0.12) | 0.000 |
| Difficulty with home leisure activities | 1.85 (0.23) | 1.46 (0.14) | 2.75 (0.27) | 4.24 (0.61) | 0.000 |
| Difficulty moving large objects | 2.71 (0.25) | −0.35 (0.08) | 0.55 (0.07) | 1.10 (0.09) | 0.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sakharkar, P.; Ansari, N. Application of Exploratory Factor Analysis and Item Response Theory to Validate NHANES ADL Scale in Patients Reporting Rheumatoid Arthritis. Pharmacy 2022, 10, 138. https://doi.org/10.3390/pharmacy10060138
Sakharkar P, Ansari N. Application of Exploratory Factor Analysis and Item Response Theory to Validate NHANES ADL Scale in Patients Reporting Rheumatoid Arthritis. Pharmacy. 2022; 10(6):138. https://doi.org/10.3390/pharmacy10060138
Chicago/Turabian StyleSakharkar, Prashant, and Najma Ansari. 2022. "Application of Exploratory Factor Analysis and Item Response Theory to Validate NHANES ADL Scale in Patients Reporting Rheumatoid Arthritis" Pharmacy 10, no. 6: 138. https://doi.org/10.3390/pharmacy10060138
APA StyleSakharkar, P., & Ansari, N. (2022). Application of Exploratory Factor Analysis and Item Response Theory to Validate NHANES ADL Scale in Patients Reporting Rheumatoid Arthritis. Pharmacy, 10(6), 138. https://doi.org/10.3390/pharmacy10060138