1. Introduction
Today, many interacting global changes are taking place at an unprecedented rate, often interrelated with human activities. These changes impact our ecological as well as societal systems. Climate change is one of the significant examples of these types of predominantly human-induced global changes, with already noticeable and anticipated consequences [
1,
2,
3].
In Europe, climate change will become an increasing burden, socio-economically and in terms of health. Climate change directly and/or indirectly affects health. Specifically, there is growing scientific evidence of its effects on infectious disease risk in Europe [
4,
5,
6,
7]. Climate change can bring about changes in the distribution and transmission of communicable diseases, and relating to this, the number of disease cases by influencing e.g., the disease pathogen directly, the suitability of environments, or human behaviors leading to exposure [
5,
6,
7,
8].
Many population health problems are embedded in a global context [
9,
10]. When trying to understand the infectious disease reality that Europe is facing today and in the future due to climate change, other relevant non-climatic mediating developments at the global but also local level need to be taken into account, such as urbanization, the movement of people (travel and migration), land use, and socio-economic inequalities [
5,
6,
11,
12]. Climatic and non-climatic developments and their infectious disease risk outcomes will play out differently across countries and regions. This is true on a global scale, but also within Europe. Moreover, adaptive capacities differ amongst European countries, and varying climate change impacts can in turn influence the ability to adapt to and control infectious disease risk [
5,
13,
14,
15]. The relevance of the global context for health outcomes encompassing multiple drivers contributes to complexities and uncertainties with regard to the relationship between climate change and infectious disease risk.
It is integral for healthy and sustainable development that a priority is placed on understanding and tackling climate change and its health impacts [
16,
17,
18]. Many studies have been done to find evidence for the effects of climate change on infectious disease risk, taking into consideration other non-climatic drivers (see e.g., [
6,
7,
19,
20,
21]). However, the relationship between climate change and infectious disease risk in a European context requires further research [
6,
7]. Besides the necessity to gain more understanding and knowledge of this complex relationship, it is also important to recognize that there will most likely always be uncertainty and therefore imperfect predictions of how climate change together with other factors will result in infectious disease risk [
13,
22]. Stakeholder involvement using participatory research methods can be a way to address complexities and uncertainties, common to environmental and specifically climate change problems [
23,
24].
In this study, the perspectives of experts on the relationship between climate change and infectious disease risk in Western Europe are investigated with a survey. Potentially relevant non-climatic drivers of infectious disease risk in Western Europe are also addressed in this survey, and compared in terms of importance with climatic drivers by the experts. The analysis integrates multiple drivers and takes on an overall holistic view on the causation of infectious disease risk.
2. Methodology and Research Design
This study has been conducted to shed more light on the views Dutch experts have on the causation of infectious disease risk in Western Europe, integrating climatic and non-climatic drivers. Surveying expert stakeholders is a way to uncover existing perspectives (and the possible diversity amongst these) in the Netherlands, concerning the relationship between climate change and infectious disease outcomes in Western Europe. For this purpose, a qualitative survey was executed. In preparation of this, a stakeholder analysis has been performed for the identification of experts and selection of an expert sample for the survey.
2.1. Stakeholder Analysis and Sampling
A stakeholder analysis was conducted to identify stakeholders for the selection of potential respondents for the expert survey used in this study [
25,
26]. A broad definition of stakeholders was assumed for this analysis: individuals and organizations that are likely to be affected by or can influence climate change and related health impacts; the latter e.g., through the implementation of adaptation measures [
26,
27,
28,
29]. The analysis was performed in the Netherlands, being a priority research focus of the ERA-ENVHEALTH ENHanCE research project. The stakeholder approach aimed to map out Dutch stakeholders in relation to the topic of climate change and infectious disease risk in Western Europe; to create a useful inventory for potential participants for the participatory elements in the broader research setup of the project; and to facilitate the collection of expert knowledge and perspectives on climate change and health impacts. This approach can be characterized as descriptive and instrumental [
26].
The stakeholder analysis yielded a stakeholder matrix where detailed information was stored for each stakeholder, such as the stakeholder’s expertise and professional background. The stakeholder matrix could then be used for the selection of an expert sample of respondents for the survey. The guiding criterion for selecting a sample of experts from the stakeholder matrix was that the individuals possess expertise relevant for the survey’s topic and scope;
i.e., expertise on climate change/environment, and health/infectious diseases. Information on the expertise of each stakeholder was documented in the stakeholder matrix and could therefore be retrieved for the purpose of sampling. Since a guiding criterion was used as a base for sample selection, this sampling method can be called judgment sampling, a non-probabilistic sampling method [
30,
31]. From the stakeholder matrix a sample of 56 experts on climate change/environment, and health/infectious diseases could be drawn. Based on the information collected about each stakeholder’s professional background, the expert sample included mostly scientists and policy advisors. The survey was conducted in 2012 and yielded a useful response of 29 (out of the 56 experts that were approached as respondents for the survey).
The survey included a section where respondents could indicate their professional background, using predefined categories with the possibility of adding additional categories in an open section. This data was used to divide the sample into groups. This was done to explore potential differences and similarities in opinions of experts with different professional backgrounds in the analysis. The sample groups were formed in the following manner: first, all respondents who indicated a professional background in policy were placed in one sample group labeled “Policy” and thereafter removed from the full list of respondents. After that, the respondents who indicated a professional background in science were included in another sample group labeled “Science”; finally, the remaining three respondents were added to the group “Policy” as the indicated professional backgrounds seemed to allow for such a compilation. This process resulted in two sample subgroups: “Policy” consisting of 12 experts, and “Science” consisting of 17 experts. As explained earlier, based on information collected in the stakeholder matrix on professional backgrounds of the selected sample, the sample could be characterized as comprising scientists and policy advisors. The self-indicated professional backgrounds of the respondents leading to the formation of the sample subgroups, confirms the initial characterization made of the composition of the selected sample. In this respect, the sample subgroups also seem to be a sensible division of the aggregate sample.
2.2. Survey Design and Content
The survey aimed to have experts assess the importance and uncertainty of climatic and non-climatic drivers of infectious disease risk in Western Europe. A survey was used as this is a suitable and efficient method for a qualitative assessment based on expert opinions and perceptions [
30]. The survey design included closed questions, predominantly in a Likert-scale format, and optional open questions. Each closed question provided a possibility to leave it open (“no opinion/do not know”) and to add more items which could then be assessed as well. All definitions could be viewed by the respondents at all times during the survey process. The survey was administered online, and generated descriptive information, nominal, ordinal and some ratio/interval data. Survey methods are prone to several common limitations, which were taken into account during the design and implementation of this study. For instance, the risk of misunderstanding of the wording used [
30] was reduced by using vocabulary familiar to experts and making definitions available at all times during the survey process. The lower quality of responses received is another potential risk of surveys, which was limited by offering a “no opinion/do not know” option.
The survey structure was the following: the assessment of
- (a)
the relative importance of climatic drivers of infectious disease risk, for each type of infectious disease risk;
- (b)
the degree of uncertainty in the future development of each climatic driver;
- (c)
the relative importance of non-climatic drivers of infectious disease risk;
- (d)
the uncertainty in the future development of each non-climatic driver; and lastly
- (e)
the relative importance of each non-climatic driver compared to climate change as a driver of infectious disease risk.
In part (a) for the assessment of the importance of climatic drivers for infectious disease risk, “importance” is defined as: the relative impact/importance of each driver for future infectious disease risk. Does the way in which the driver evolves make a major difference in increasing or decreasing the overall infectious disease risk, or does it make a relatively minor difference? [
32]. The following climatic drivers were included in the survey: temperature change, precipitation change, humidity change, climate change induced habitat change, and increase in frequency of extreme weather events. Infectious disease risk is specified in broad types: water-related infectious disease risk, food-related infectious disease risk, vector-borne disease risk excluding zoonoses, and risk of zoonoses [
32]. Here a zoonosis is defined as: “[…] any disease or infection that is naturally transmissible from vertebrate animals to humans. Animals thus play an essential role in maintaining zoonotic infections in nature. Zoonoses may be bacterial, viral, or parasitic, or may involve unconventional agents [
33].”
In the next part, experts assessed the degree of uncertainty in the future development of each climatic driver for infectious disease risk. For the purpose of this question, uncertainty has been defined as: Degree of uncertainty in each driver. How much variation is there in the range of possible ways in which the driver could evolve? Is there a great deal of uncertainty in this, or relatively little? [
32].
For the following parts of the survey (c) and (d), non-climatic drivers were assessed. A conceptual analysis for the identification of potential non-climatic drivers of infectious disease risk was conducted using relevant background studies and literature (see amongst others [
6,
11,
34,
35,
36]). After that a selection of non-climatic drivers was made for inclusion in the survey, according to their potential importance in a European context. The non-climatic drivers are organized in domains: ecological, economic and agricultural, technological, institutional, and socio-cultural. The survey included the same questions as for the climatic drivers, using the same definitions for importance and uncertainty.
Finally, the non-climatic drivers were compared to climate change as an aggregate driver for infectious disease risk in terms of relative importance, using the same definition for importance.
2.3. Survey Analysis
The resulting survey data were analyzed using descriptive statistics. The statistics performed are appropriate for the ordinal data obtained from Likert-scale questions. Thus, for the analysis of central tendency and variability median, mode, range, and inter-quartile range are used (see e.g., [
30]). Moreover, the smaller sample size and non-probabilistic sampling method were taken into account for the analysis. Uncompleted surveys were excluded from the analysis. For the analysis, the “no opinion/do not know” responses were assumed to be distributed proportionally amongst the respondents, and therefore were excluded in order to circumvent an inflation of the actual resulting responses [
30].
In order to explore the experts’ opinions according to the experts’ self-indicated professional background, all descriptive analyses were done for the aggregate sample as well as for the two sample groups “Policy” and “Science”, described earlier.
3. Results of the Survey
In this section, the results of the survey analysis are presented in the form of descriptive statistics.
3.1. Expert Assessment of the Relative Importance of Climatic Drivers for Infectious Disease Risk
Through analysis of the survey results the perspectives of the expert sample on the relative importance of climatic drivers for infectious disease risk types could be obtained. The results are first presented of the aggregate sample analysis in
Figure 1a–d, and thereafter of the two sample groups “Policy” and “Science” in
Figure 2a–h.
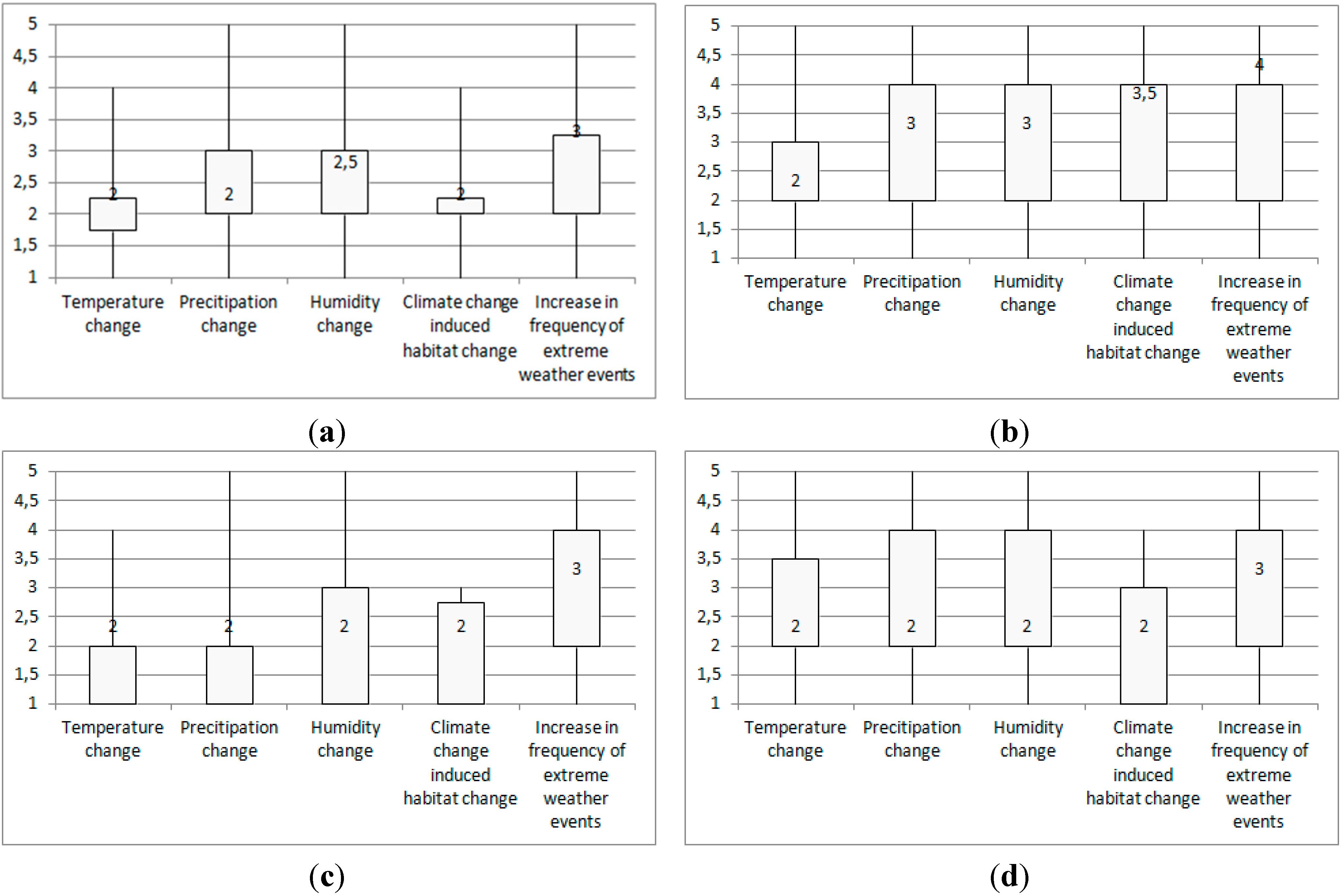
Figure 1a–d shows the results of the aggregate expert sample’s assessment of the relative importance of the climatic drivers for each type of infectious disease risk.
Figure 1.
Box plots of the aggregate sample assessment of the relative importance of climatic drivers for each type of infectious disease risk (a) Water-related infectious disease risk; (b) Food-related infectious disease risk; (c) Vector-borne disease risk (excluding zoonoses); (d) Risk of zoonoses.
Figure 1.
Box plots of the aggregate sample assessment of the relative importance of climatic drivers for each type of infectious disease risk (a) Water-related infectious disease risk; (b) Food-related infectious disease risk; (c) Vector-borne disease risk (excluding zoonoses); (d) Risk of zoonoses.
Notes: Medians are given as numbers in the box plots; Interpretation of the median values for importance: 1 = very high importance (high importance, moderate importance, little importance) 5 = very little importance; Range = maximum value − minimum value; Interquartile range (IQR) = 3rd quartile − 1st quartile = length of box.
It can be seen that the aggregate expert sample views temperature change as highly important for all types of infectious disease risk. In addition, precipitation change and climate change induced habitat change are seen as highly important, except for food-related infectious disease risk, where these drivers are rated with moderate and little importance respectively. Increase in frequency of extreme weather events is overall rated to be least relevant; expert assessments show moderate importance for water-related and vector-borne infectious diseases and zoonoses, and even little importance for food-related infectious disease risk. With use of the interquartile range (hereafter IQR) a closer look can be taken at the variability of the expert opinions. The experts show little variance in their opinions on temperature change, precipitation change, and humidity change, as well as for water-related infectious disease risk and vector-borne disease risk excluding zoonoses. Overall, most variation amongst expert assessments, based on the IQR, can be found for the climatic driver increase in frequency of extreme weather events, and the infectious disease type risk of zoonoses.
The same analysis was done for the two sample groups “Policy” and “Science”. In
Figure 2a–h, the assessment of the relative importance of climatic drivers for each type of infectious disease risk given by the two sample groups can be found.
Figure 2.
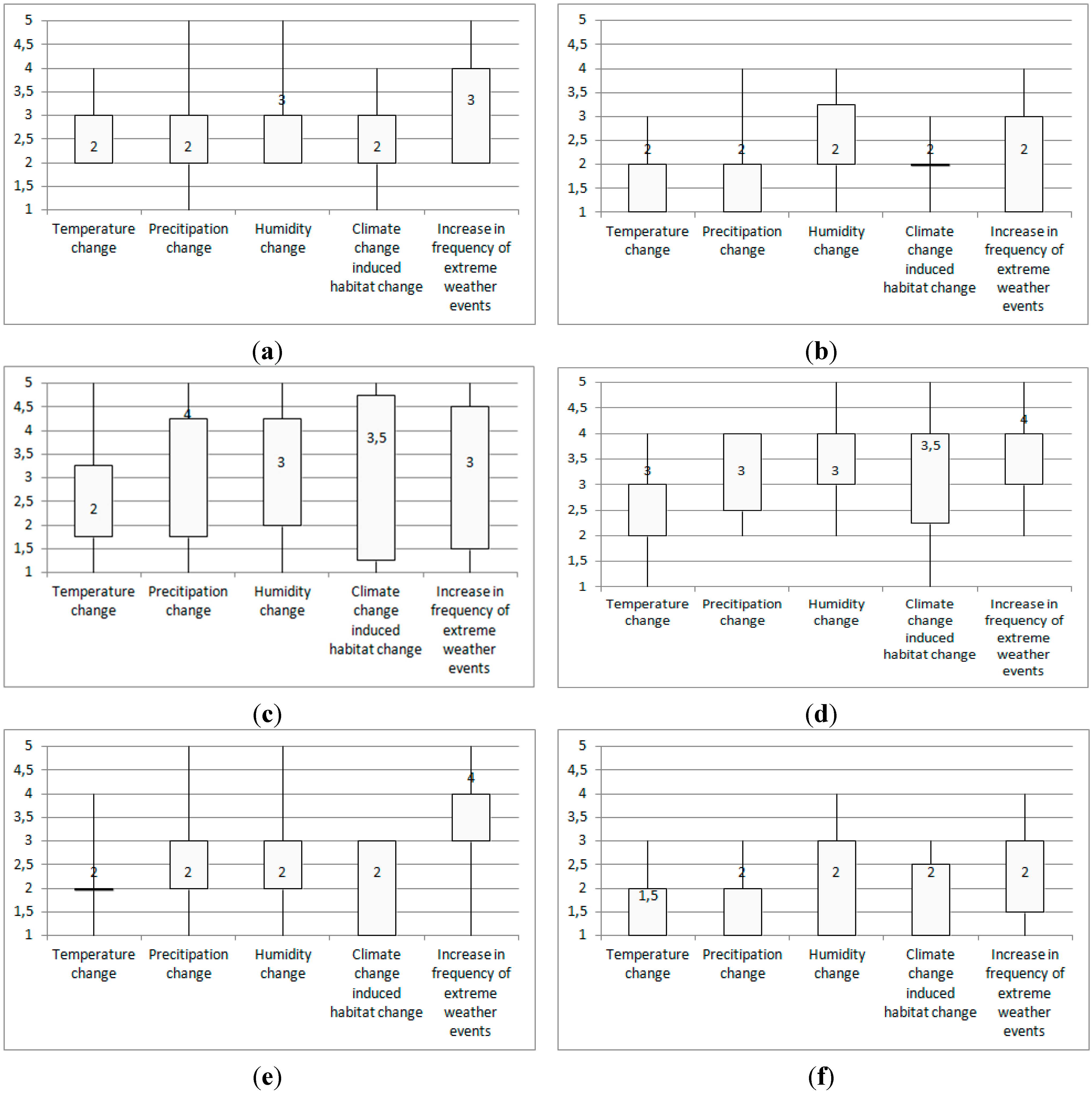
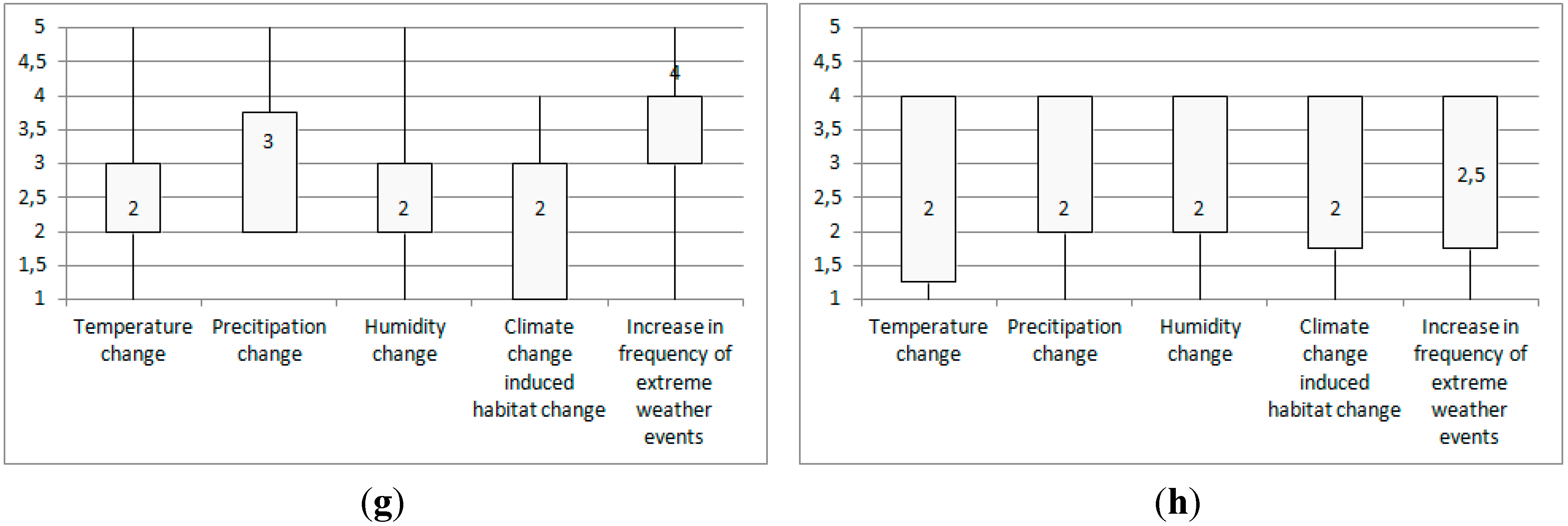
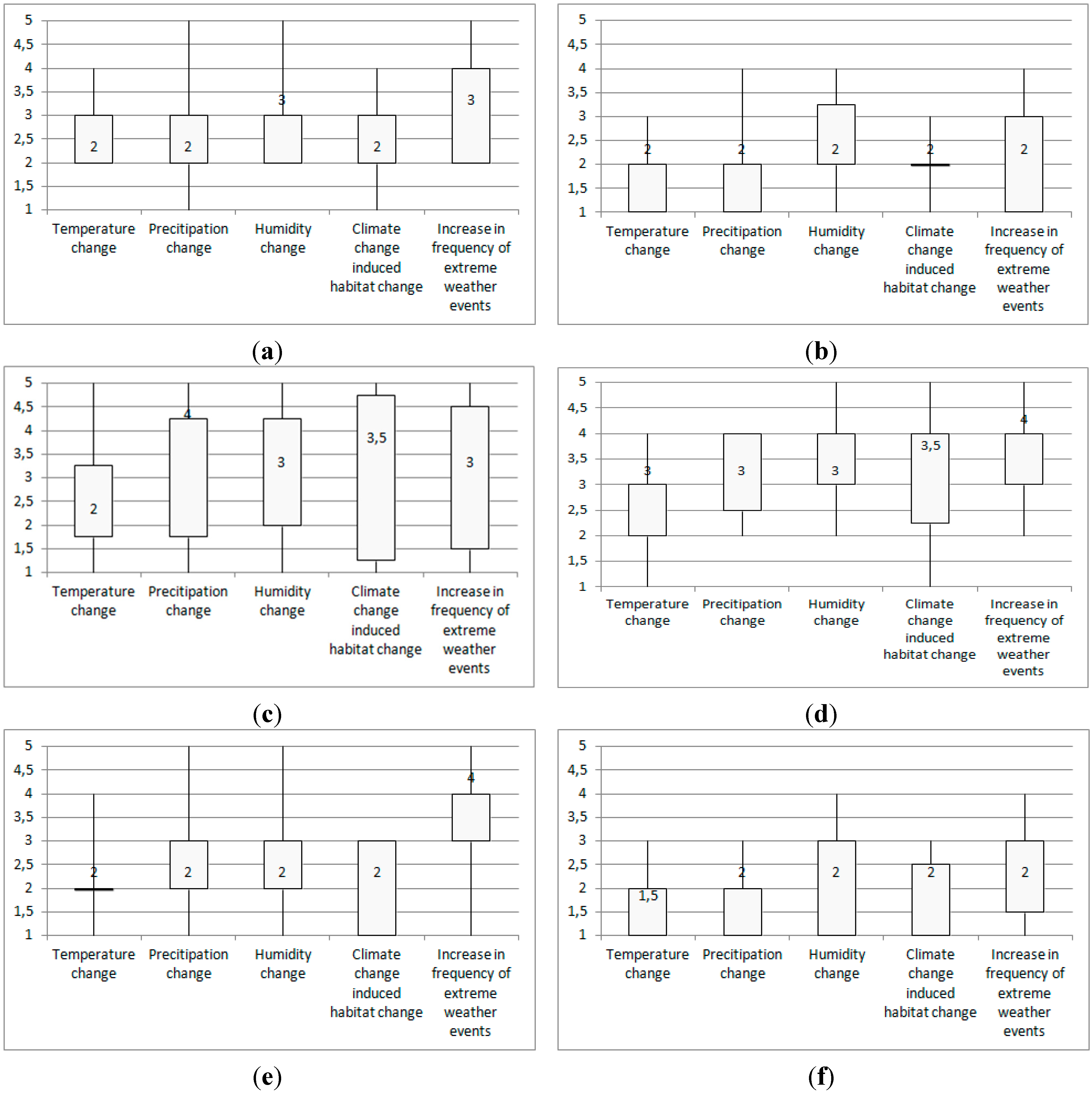
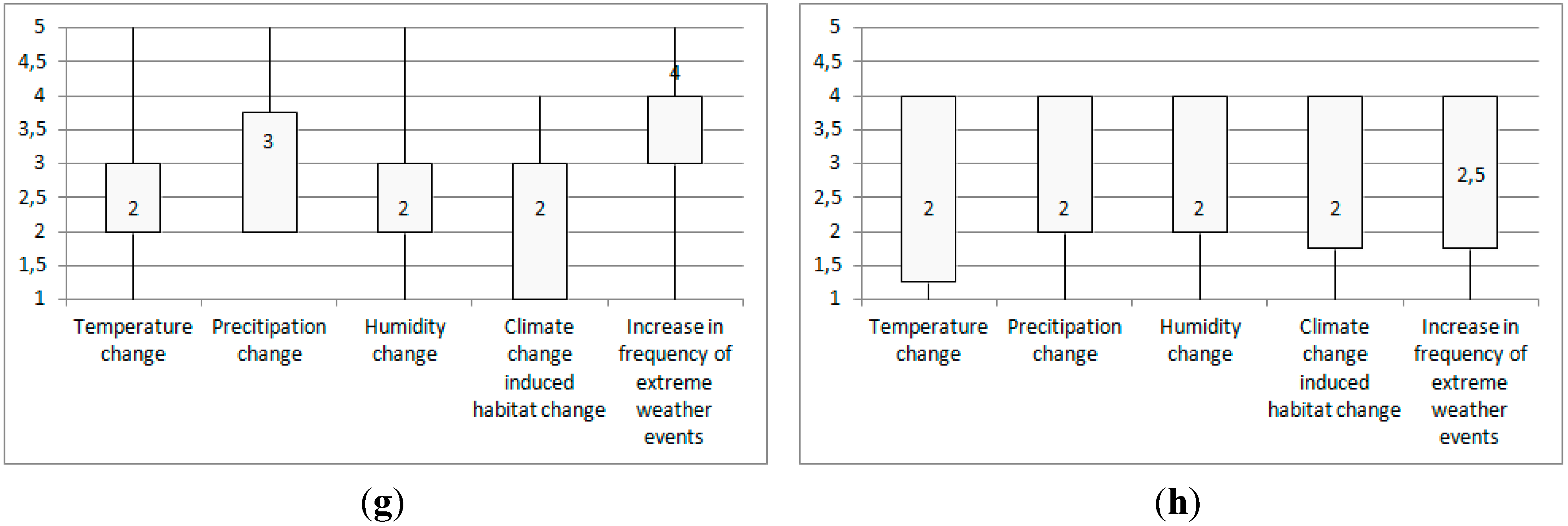
Box plots of the assessments of the two sample groups “Policy” and “Science” of the relative importance of climatic drivers for each type of infectious disease risk (a) Water-related infectious disease risk, sample group “Policy”; (b) Water-related infectious disease risk, sample group “Science”; (c) Food-related infectious disease risk, sample group “Policy”; (d) Food-related infectious disease risk, sample group “Science”; (e) Vector-borne disease risk (excluding zoonoses), sample group “Policy”; (f) Vector-borne disease risk (excluding zoonoses), sample group “Science”; (g) Risk of zoonoses, sample group “Policy”; (h) Risk of zoonoses, sample group “Science”.
Figure 2.
Box plots of the assessments of the two sample groups “Policy” and “Science” of the relative importance of climatic drivers for each type of infectious disease risk (a) Water-related infectious disease risk, sample group “Policy”; (b) Water-related infectious disease risk, sample group “Science”; (c) Food-related infectious disease risk, sample group “Policy”; (d) Food-related infectious disease risk, sample group “Science”; (e) Vector-borne disease risk (excluding zoonoses), sample group “Policy”; (f) Vector-borne disease risk (excluding zoonoses), sample group “Science”; (g) Risk of zoonoses, sample group “Policy”; (h) Risk of zoonoses, sample group “Science”.
![]()
![]()
Notes: Medians are given as numbers in the box plots. Interpretation of the median values for importance: 1 = very high importance (high importance, moderate importance, little importance) 5 = very little importance; Range = maximum value − minimum value; Interquartile range (IQR) = 3rd quartile − 1st quartile = length of box.
Several differences between the groups “Science” and “Policy” can be found. Humidity change and increase in frequency of extreme weather events as drivers of water-related infectious disease risk are seen as moderately important by the “Policy” group but as highly important by the “Science” group. For food-related infectious disease risk the two groups are in disagreement regarding the importance of temperature change (“Policy”: high importance; “Science”: moderate importance); precipitation change (“Policy”: little importance; “Science”: moderate importance); and increase in frequency of extreme weather events (“Policy”: moderate importance; “Science”: little importance). The importance of temperature change for vector-borne disease risk excluding zoonoses is assessed to be high by the “Policy” group; and high to very high by the “Science” group. Moreover, the importance of increase in frequency of extreme weather events for this disease risk is rated to be of little importance by the “Policy” group, and of high importance by the “Science” group. For the risk of zoonoses the two groups differ in their assessment of the importance of precipitation change: “Science” rates this to be high, and “Policy” to be moderate. Lastly, for the importance of increase in extreme weather events the results of the two groups differ quite notably: “Science” rating this to be of high to moderate importance, and “Policy” viewing this as having little importance. For all other values, which are the majority, the same assessments result from the two groups. This means that both groups assess the following climatic drivers to be highly important: temperature change for water-related infectious disease risk and zoonoses; precipitation change for water-related infectious disease risk and vector-borne disease risk; humidity change for vector-borne disease risk and zoonoses; and finally, climate change induced habitat change for water-related infectious disease risk, vector-borne infectious disease risk, and zoonoses. In sum, it can be seen that the opinions on the importance of increase in frequency of extreme weather events differ mostly for all disease types between the two groups. Most agreement between the two groups’ assessments can be found for the importance of climate change induced habitat change, where all the ratings are the same between groups for all disease types, and the importance of humidity change where the ratings are the same for all but one disease type, namely water-related infectious disease risk.
The IQRs indicate that both the groups “Science” and “Policy” show much agreement within each group regarding water-related infectious disease risk and vector-borne disease risk excluding zoonoses. The variation in expert opinions for food-related infectious disease risk is high for the group “Policy”. For zoonoses, the groups alternately show higher and lower IQRs.
3.2. Expert Assessment of the Degree of Uncertainty in the Future Development of Each Climatic Driver
Next, the degree of uncertainty in the future development of each climatic driver was assessed. The analyses for both the aggregate sample as well as the two sample groups “Science” and “Policy” are presented in
Table 1.
Table 1.
Assessment results of the degree of uncertainty in the future development of each climatic driver, for the aggregate sample and the two sample groups “Policy” and “Science”.
Table 1.
Assessment results of the degree of uncertainty in the future development of each climatic driver, for the aggregate sample and the two sample groups “Policy” and “Science”.
| Assessment of Uncertainty |
|---|
| Aggregate Sample | Sample Group “Policy” | Sample Group “Science” |
|---|
| Climatic drivers | Median | IQR a | Median | IQR | Median | IQR |
| Temperature change | 3 | 1 | 3 | 2.25 | 3 | 1 |
| Precipitation change | 3 | 1 | 3 | 1.25 | 3 | 1 |
| Humidity change | 2 | 1 | 3 | 1 | 2 | 1 |
| Climate change induced habitat change | 2 | 1 | 2 | 1 | 2 | 1 |
| Increase in frequency of extreme weather events | 3 | 1 | 2 | 2.25 | 3 | 1 |
From the analysis of the aggregate sample, it can be gathered that temperature change, precipitation change, and increase in frequency of extreme weather events are seen as being moderately uncertain in their future development. Experts assign high uncertainty in future development for the climatic drivers humidity change and climate change induced habitat change. The IQR’s are low for these results, pointing to relatively little variability in expert opinions in the aggregate sample.
The same analysis was done for the two sample groups “Science” and “Policy”. It can be seen that the two groups “Science” and “Policy” agree with regards to the degree of uncertainty in the future development of temperature change, precipitation change, and climate change induced habitat change. The group “Policy” sees the increase in frequency of extreme weather events as being more uncertain (high uncertainty) than the group “Science” (moderate uncertainty). The opposite holds for the uncertainty of humidity change (group “Science”: high uncertainty, group “Policy”: moderate uncertainty).
The IQRs for the group “Science” are low, indicating high agreement amongst experts on uncertainty. The group “Policy” has relatively higher IQRs, thus a higher variability in their responses on uncertainty. Particularly, a high degree of divergence can be found in their opinions on temperature change and frequency of extreme weather events.
3.3. Expert Assessment of the Relative Importance of Non-Climatic Drivers for Infectious Disease Risk
The expert survey also included selected non-climatic drivers of infectious disease risk, which were assessed in terms of their relative importance for infectious disease risk.
Table 2 shows the results of the expert assessment of the relative importance of non-climatic drivers of infectious disease risk, both for the aggregate sample and the two sample groups “Science” and “Policy”.
Table 2.
Assessment results of the relative importance of non-climatic drivers of infectious disease risk, for the aggregate expert sample and for the two sample groups “Policy” and “Science”.
Table 2.
Assessment results of the relative importance of non-climatic drivers of infectious disease risk, for the aggregate expert sample and for the two sample groups “Policy” and “Science”.
| Assessment of Importance |
|---|
| Aggregate Sample | Sample Group “Policy” | Sample Group “Science” |
|---|
| Ecological (non-climatic) drivers | Median | IQR b | Median | IQR | Median | IQR |
| Land use change | 2 | 1 | 2 | 1 | 2 | 1 |
| Microbial evolution | 2 | 1 | 2.50 | 2 | 2 | 1 |
| Pollution | 3 | 2 | 4 | 1 | 3 | 2 |
| Urban greening | 3 | 0 | 3 | 0 | 3 | 0 |
| Economic and agricultural drivers | Median | IQR | Median | IQR | Median | IQR |
| Increased movement of goods | 2 | 1 | 2 | 1 | 2 | 1 |
| Increased farm scale and scope | 2 | 1 | 2 | 1 | 2 | 1 |
| Increased organic farming | 3 | 1 | 3 | 1 | 3 | 1 |
| Technological drivers | Median | IQR | Median | IQR | Median | IQR |
| Globalized food supply chains | 2 | 0.75 | 2 | 1 | 2 | 1 |
| Widespread use of antibiotics | 2 | 1 | 2 | 1 | 2 | 1 |
| Capacity to detect, prevent, and treat diseases | 2 | 1 | 2 | 1 | 2 | 1 |
| Institutional drivers | Median | IQR | Median | IQR | Median | IQR |
| Decreased public health care structures | 2 | 1.75 | 2 | 1 | 2 | 2 |
| Limitations to and reduction in prevention Programs | 2 | 0 | 2 | 0 | 2 | 1 |
| Move towards privatization of health sector | 3 | 2 | 3 | 2 | 3 | 1 |
| Socio-cultural drivers | Median | IQR | Median | IQR | Median | IQR |
| Increased movement of people | 2 | 0.25 | 2 | 1 | 2 | 0 |
| Aging population | 2 | 2 | 2 | 2 | 2.50 | 2 |
| Incidence of chronic diseases | 3 | 2 | 3 | 2 | 3 | 1 |
| Sexual behavior | 3 | 1 | 3 | 0.50 | 2 | 1 |
| Intravenous drug use | 3 | 1 | 4 | 2 | 3 | 0.75 |
From the results for the aggregate sample in
Table 2 it can be seen that a large part of the non-climatic drivers are rated to be of high importance for infectious disease risk. Drivers such as pollution, urban greening, and increased organic farming are seen as having moderate importance. When looking at the relating IQRs, it can be seen that relatively more variability in the aggregate expert sample’s responses can be ascertained for the importance of pollution, move towards privatization of health sector, aging population, and incidence of chronic diseases.
The same analyses were performed for the two groups “Science” and “Policy”. The median results for both groups for relative importance of non-climatic drivers are largely similar. Some main differences can be observed. The group “Policy” rates pollution to have little importance as opposed to moderate importance resulting from the group “Science”. The group “Science” considers sexual behavior as being highly important as opposed to moderately important resulting from the group “Policy”. Moreover, the group “Policy” also indicates intravenous drug use to be of little importance, whereas the group “Science” views this as moderately important. The IQRs for the responses given by the two sample groups are relatively low, indicating high agreement amongst the experts within each group. More variability in experts’ responses of the sample group “Science” could be found for pollution, decreased public health care structures, and aging population. For the group “Policy” more variability can be seen for microbial evolution, increased movement of goods, move towards privatization of health sector, aging population, chronic diseases, and intravenous drug use. So overall, for more non-climatic drivers a relatively higher variability could be found in the responses of the group “Policy”.
3.4. Expert Assessment of the Degree of Uncertainty in the Future Development of Each Non-Climatic Driver
The expert sample also assessed the degree of uncertainty in the future development of each non-climatic driver.
Table 3 presents these results for the aggregate sample and the two sample groups “Science” and “Policy”.
Regarding the results of the aggregate sample, in
Table 3 it can be found that only microbial evolution is indicated to be highly uncertain in its future development. Many drivers are rated to be moderately uncertain in their future development, amongst which are land use change, increased farm scale and scope, and limitations to and reduction in prevention programs. Moreover, quite a significant amount of drivers received a rating of little uncertainty, including widespread use of antibiotics, decreased public health care structures, aging population, and incidence of chronic diseases. The IQR’s and thus the differences in expert opinions within the aggregate sample are relatively higher for the uncertainty of increased movement of goods, increased organic farming, and capacity to detect, prevent, and treat diseases.
When taking a look at the assessment of uncertainty by the two sample groups “Policy” and “Science”, the following can be seen. The groups show notably different results in their median uncertainty ratings for increased movement of goods, decreased public health care structures, limitations to and reductions in prevention programs, and incidence of chronic diseases. For all technological drivers the two groups agree in their assessments. The IQRs for the group “Science” are low, indicating much agreement in expert opinion in this group. An exception is found for the uncertainty of the move towards privation of the health sector which has a higher IQR and therefore larger variability amongst expert opinions in the group “Science”. With regards to the IQRs found for the group “Policy”, it becomes clear that the experts show less consensus on the uncertainty of microbial evolution, the increased movement of goods, globalized food supply chains, aging population, sexual behavior, and intravenous drug use.
Table 3.
Assessment results of the degree of uncertainty in the future development of each non-climatic driver, for the aggregate expert sample and for the two sample groups “Policy” and “Science”.
Table 3.
Assessment results of the degree of uncertainty in the future development of each non-climatic driver, for the aggregate expert sample and for the two sample groups “Policy” and “Science”.
| Assessment of Uncertainty |
|---|
| Aggregate Sample | Sample Group “Policy” | Sample Group “Science” |
|---|
| Ecological (non-climatic) drivers | Median | IQR c | Median | IQR | Median | IQR |
| Land use change | 3 | 0.75 | 3 | 1 | 3 | 0 |
| Microbial evolution | 2 | 1.50 | 2 | 1.50 | 2.50 | 1.75 |
| Pollution | 3 | 1 | 3 | 2 | 3.50 | 1.75 |
| Urban greening | 3 | 1 | 3 | 1.25 | 3 | 1 |
| Economic and agricultural drivers | Median | IQR | Median | IQR | Median | IQR |
| Increased movement of goods | 4 | 2 | 3 | 2.25 | 4 | 1.50 |
| Increased farm scale and scope | 3 | 1.25 | 3 | 1 | 3 | 1 |
| Increased organic farming | 3 | 2 | 2.50 | 1.75 | 3 | 1 |
| Technological drivers | Median | IQR | Median | IQR | Median | IQR |
| Globalized food supply chains | 3 | 1.75 | 3 | 2 | 3 | 1 |
| Widespread use of antibiotics | 4 | 1 | 4 | 1 | 4 | 1.50 |
| Capacity to detect, prevent, and treat diseases | 3 | 2 | 3 | 1.25 | 3 | 1.50 |
| Institutional drivers | Median | IQR | Median | IQR | Median | IQR |
| Decreased public health care structures | 4 | 1 | 3 | 1.25 | 4 | 0.50 |
| Limitations to and reduction in prevention Programs | 3 | 1 | 4 | 1.50 | 3 | 1 |
| Move towards privatization of health sector | 3 | 1 | 2.50 | 1 | 3 | 2 |
| Socio-cultural drivers | Median | IQR | Median | IQR | Median | IQR |
| Increased movement of people | 4 | 1 | 4 | 1 | 4 | 1 |
| Aging population | 4 | 1 | 4 | 2 | 4 | 1 |
| Incidence of chronic diseases | 4 | 1 | 3 | 1 | 4 | 1 |
| Sexual behavior | 4 | 1 | 3.50 | 3 | 4 | 1 |
| Intravenous drug use | 4 | 1 | 4 | 2.50 | 3.50 | 1 |
3.5. Expert Assessment of the Relative Importance of Non-Climatic Drivers Compared to Climate Change
Finally, the experts assessed the relative importance of each non-climatic driver compared to climate change as an aggregate driver for infectious disease risk. The results of this assessment are shown in
Table 4 for the aggregate sample and the two sample group “Science” and “Policy”.
Table 4.
Assessment results of the relative importance of each non-climatic driver compared to climate change as a driver of infectious disease risk, for the aggregate sample and for the two sample groups “Policy” and “Science”.
Table 4.
Assessment results of the relative importance of each non-climatic driver compared to climate change as a driver of infectious disease risk, for the aggregate sample and for the two sample groups “Policy” and “Science”.
| Importance of Non-Climatic Drivers Compared to Climate Change |
|---|
| Aggregate Sample | Sample Group “Policy” | Sample Group “Science” |
|---|
| Ecological (non-climatic) drivers | Median | IQR d | Median | IQR | Median | IQR |
| Land use change | 1 | 1 | 1 | 0.50 | 1 | 1 |
| Microbial evolution | 1 | 1 | 1.50 | 1 | 1 | 1 |
| Pollution | 2 | 1 | 2 | 0 | 2 | 1 |
| Urban greening | 2 | 0 | 2 | 0 | 2 | 0.25 |
| Economic and agricultural drivers | Median | IQR | Median | IQR | Median | IQR |
| Increased movement of goods | 1 | 1 | 1 | 1 | 1 | 1 |
| Increased farm scale and scope | 1 | 1 | 1 | 1 | 1 | 1 |
| Increased organic farming | 2 | 1 | 2 | 1 | 2 | 1 |
| Technological drivers | Median | IQR | Median | IQR | Median | IQR |
| Globalized food supply chains | 1 | 1 | 1 | 1 | 1 | 1 |
| Widespread use of antibiotics | 1 | 0 | 1 | 0 | 1 | 0 |
| Capacity to detect, prevent, and treat diseases | 1 | 1 | 2 | 1 | 1 | 1 |
| Institutional drivers | Median | IQR | Median | IQR | Median | IQR |
| Decreased public health care structures | 1 | 1 | 1 | 1 | 1 | 0.75 |
| Limitations to and reduction in prevention Programs | 1 | 1 | 1.50 | 1 | 1 | 1 |
| Move towards privatization of health sector | 2 | 0 | 2 | 0 | 2 | 1 |
| Socio-cultural drivers | Median | IQR | Median | IQR | Median | IQR |
| Increased movement of people | 1 | 1 | 1 | 1 | 1 | 0.50 |
| Aging population | 1 | 1 | 1.50 | 1 | 1 | 1 |
| Incidence of chronic diseases | 2 | 1 | 2 | 0.50 | 1 | 1 |
| Sexual behavior | 1.50 | 1 | 2 | 1 | 1 | 1 |
| Intravenous drug use | 2 | 0 | 2 | 0.25 | 2 | 0.50 |
The aggregate sample’s results show that climate change is seen as a more important driver for infectious disease risk than the following non-climatic drivers: pollution, urban greening, increased organic farming, incidence of chronic diseases, intravenous drug use, and the move towards privatization of the health sector. According to the aggregate sample, most non-climatic drivers are more important than climate change. For the technological domain, all drivers tested are rated as more important than climate change. The results of the aggregate sample show low to very low IQRs, meaning that the experts’ opinions vary little.
The same analysis was done for the two groups “Policy” and “Science”. The two sample groups mostly agree in their assessment of the importance of non-climatic drivers compared to climate change. With regards to capacity to detect, prevent, and treat diseases, the group “Policy” sees this as less important than climate change, and the group “Science” as more important than climate change. The same disagreement can be found for incidence of chronic diseases and sexual behavior. For both sample groups the IQRs are low, pointing towards much agreement amongst expert opinions within each group.
4. Discussion and Conclusions
The results of the survey reveal information on the opinions of the expert sample on the importance, uncertainty, and comparative importance of climatic and non-climatic drivers for infectious disease risk in Western Europe. Moreover, the expert opinions were further explored by conducting all analyses for two sample subgroups “Science” and “Policy”.
The aggregate sample and sample group analyses in summary yield several key results. The aggregate sample views all climatic drivers as highly important for all types of infectious disease risk, except for the driver increase in extreme weather events which is rated to have moderate to little importance. For food-related infectious disease risk, the climatic drivers receive relatively lower ratings for importance. For this disease type, the experts might perceive non-climatic drivers of potential importance for explaining food-related infectious disease risk. Regarding this, in an open section, one of the respondents remarks that the control on food production, as well as the preservation of food are relevant for food-related disease outcomes, and can prevent the climatic effects. Related research also emphasizes the significance of non-climatic factors such as food safety standards, food handling and storage, and food production and processing for food-borne disease outcomes besides climate change. Non-climatic drivers might even counteract the effects of climatic drivers such as temperature change [
6,
11,
22]. The aggregate expert sample opinions converge greatly for temperature change, precipitation change, and humidity change, but less so for the climatic driver increase in frequency of extreme weather events. For water-related and vector-borne disease risks, high agreement amongst experts is found. The experts agree less on the importance of the climatic drivers for zoonoses and food-related disease types. The relationships between climate change and zoonoses as well as climate change and food-related infectious diseases are shown to be complex as impacts of climatic and non-climatic developments, such as human behavior and regulations, act together. More research on the role climate change plays in these disease outcomes is needed [
6,
37]. This lack of knowledge and the remaining uncertainties on these relationships might be an underlying cause for the variations found amongst expert opinions. One respondent also confirms this in a comment, stating that many climatic and non-climatic factors impact zoonoses, which makes it difficult to assess the impact of climatic drivers.
The assessment of importance of climatic drivers for infectious disease risk has also been analyzed for the two sample groups “Policy” and “Science”. The groups show much agreement in their assessments. Most disagreement is found for the importance of frequency of extreme weather events for all disease types. Most agreement between the two groups is found for the importance of climate change induced habitat change and humidity change. Within each sample group, there is much agreement in assessments for water-related and vector-born infectious disease risks.
Regarding the degree of uncertainty in the future development of each climatic driver, the aggregate sample’s assessment shows that temperature change, precipitation change, and increase in frequency of extreme weather events are viewed as moderately uncertain in their future development, and humidity change and climate change induced habitat change as highly uncertain. Expert’s opinions vary little regarding the uncertainty assessments given, based on the IQRs. When looking into the opinions given by the two sample groups, agreement is found for temperature change, precipitation change, and climate change induced habitat change. More variation amongst the opinions of the group “Policy” can be found in particular for the uncertainty of the future development of temperature change and the increase in frequency of extreme weather events. The group “Science” shows high agreement amongst expert opinions.
An integrative perspective is taken on the relationship between climate change and infectious disease risk, and therefore non-climatic drivers with potential relevance for the causation of infectious disease risk in Western Europe were included for expert assessment as well. It can be seen that the aggregate expert sample assesses many non-climatic drivers to be highly important, such as land use change, increased movement of goods, and widespread use of antibiotics. Some non-climatic drivers are rated to be moderately important, such as pollution, urban greening, and the incidence of chronic diseases. The related IQRs point towards less agreement amongst expert opinions on the importance of pollution, move towards privatization of health sector, aging population, and incidence of chronic diseases. The analyses of the two sample groups’ assessments of importance show overall similar results between the two groups. Key differences between the two groups are found for pollution, sexual behavior, and intravenous drug use. The IQRs show that within both sample groups high agreement amongst experts exist. The group “Policy” shows relatively more cases of higher variation in their assessment of importance of non-climatic drivers, particularly for some of the socio-cultural drivers.
With regards to the degree of uncertainty in the future development of each non-climatic driver only microbial evolution is rated to be highly uncertain by the aggregate expert sample. Most non-climatic drivers are rated to be moderately uncertain, such as land use change, pollution, and increased organic farming. In addition, some non-climatic drivers are seen as having little uncertainty, including all socio-cultural drivers. These results might partly be related to differences in the temporal scale of change in a driver, in other words, whether a driver can change relatively faster or slower. Microbial evolution can take place relatively fast possibly giving rise to more
perceived uncertainty in its future development due to this dynamism, whereas the socio-cultural drivers assessed such as ageing population, and the incidence of chronic diseases, can only structurally change over a longer period of time, and thus making it arguably easier to predict and anticipate in the nearer future and therefore reducing their
perceived uncertainty in future development [
38]. The analysis of the two sample groups shows that the two groups differ in their assessments of increased movement of goods, decreased public health care structures, limitation to and reductions in prevention programs, and incidence of chronic diseases. For all technological drivers, the two groups are in agreement. The IQRs show that within the group “Science”, relatively high agreement amongst experts can be found. For the group “Policy” generally the IQRs are also low, except for a small number of non-climatic drivers including a significant amount of socio-cultural drivers.
Lastly, the aggregate expert sample analyses reveal that a large part of the non-climatic drivers are seen as more important than climate change as a driver for infectious disease risk. The non-climatic drivers that are found to be less important than climate change are: pollution, urban greening, increased organic farming, incidence of chronic diseases, intravenous drug use, and move towards privatization of health sector. Within the aggregate sample, experts have high agreement on this assessment. The analysis of the two sample groups “Science” and “Policy” shows high agreement within and between groups. Most disagreement is found once again for socio-cultural drivers. In addition, in this context it should be noted that the comparative importance of non-climatic and climatic drivers might vary when focusing on shorter or longer temporal scales, which is also noted by one of the respondents in a related open section. The question of the relative importance of climate change for infectious diseases and broader health outcomes in comparison to other drivers is often raised [
20,
21]. The results give an indication of how this relative importance between climatic and non-climatic drivers is viewed by the expert sample and the sample groups “Science” and “Policy”.
The results of the survey should be seen as an indication of the perspectives of Dutch experts on the importance and uncertainty of climatic and non-climatic drivers for infectious disease risk in Western Europe, based on the Dutch expert sample that participated in this study. The inherent complexity of the relationship between climate change and infectious disease outcomes makes analysis difficult and as a result research gaps remain [
6,
21]. For the investigation of issues of greater complexity and uncertainty such as climate change impacts on infectious diseases, the involvement of experts for the exploration of their perspectives can be a useful approach to gain more insights in this complexity and discover underlying values. This approach is not only deemed constructive because of this complex nature of climate change and other environmental problems, but also in relation to policy in this area [
23,
24]. For the interpretation of the results of this study it should be noted that a Dutch expert sample has been surveyed. It would be interesting to conduct similar studies involving experts from other countries in order to compare and contrast potentially prevailing perspectives on climate change and infectious disease risk in Western Europe. Another issue that should be considered for the interpretation of results is the focus on Western Europe, as disease outcomes from climate change vary across geographical locations.
The analyses of expert opinions of the two sample groups “Science” and “Policy” can point towards possible differing perspectives held in the two professional environments regarding certain drivers and/or their uncertainty and importance for infectious disease risk. The differences found between the two sample groups could be due to diversity in underlying values within each professional environment. Such a difference between experts’ views from the policy or academic field is also suggested in a study analyzing expert opinions on climate change [
39]. Further exploration of expert opinions on climate change and infectious disease risk and comparisons across professional backgrounds would be necessary in order to shed more light on possible differences and identify prevailing perspectives on this topic. In addition, the influence of other issues on the diversity of opinions should be considered, such as potential existing information asymmetries between scientific and policy communities.
Differences in opinions found between sample groups and within the aggregate sample and each sample group, can have practical implications. The findings can point towards a lack of consensus with regards to the importance or uncertainty of some of the drivers of infectious disease risk in Western Europe. Differences in expert views can play out in decision-making and policy contexts with regards to climate change and infectious disease risk. Awareness and recognition of the diversity of values creating the variety in expert opinions as well as potential other issues of influence such as information asymmetries can facilitate decision- and policy-making processes for the governance of climate change induced infectious disease risk. Policy and societal responses to climate change induced infectious disease risk which accommodate the different perspectives of a broad range of stakeholders could benefit from greater support and robustness.


{kind=link}
{kind=link}
{kind=link}