
A Systematic Review on Cannabinoids for Neuropathic Pain Administered by Routes Other than Oral or Inhalation

 ,
,  and
and
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
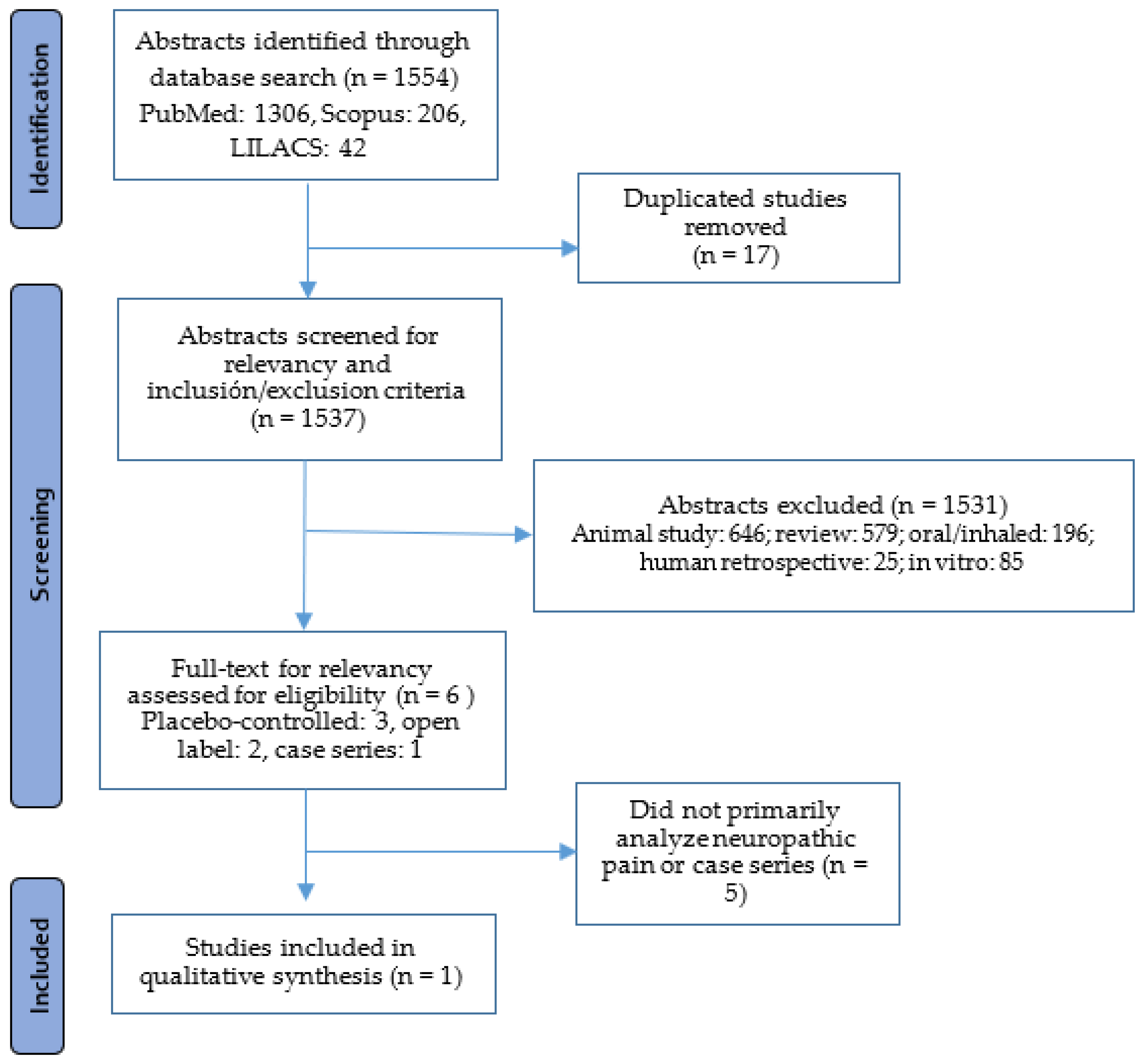
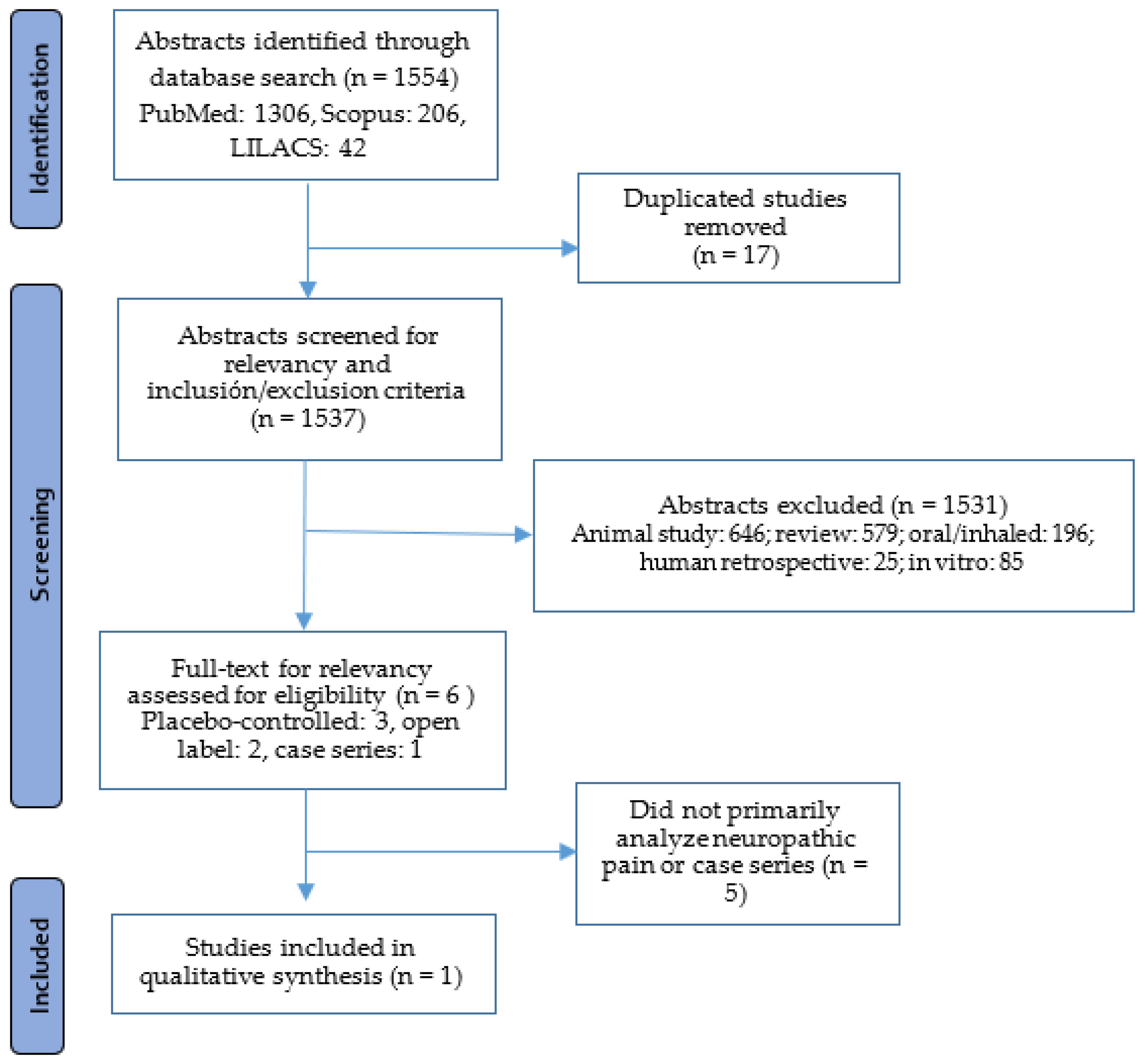
4.1. Search Eligibility Criteria and Search Strategy
4.2. Selection of Studies, Data Extraction and Risk of Bias
4.3. Measures of Treatment Effect
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Meyers, J.L.; Madhwani, S.; Rausch, D.; Candrilli, S.D.; Krishnarajah, G.; Yan, S. Analysis of real-world health care costs among immunocompetent patients aged 50 years or older with herpes zoster in the United States. Hum. Vaccines Immunother. 2017, 13, 1861–1872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matthews, S.; De Maria, A.; Passamonti, M.; Ristori, G.; Loiacono, I.; Puggina, A.; Curran, D. The Economic Burden and Impact on Quality of Life of Herpes Zoster and Postherpetic Neuralgia in Individuals Aged 50 Years or Older in Italy. Open Forum Infect. Dis. 2019, 6, ofz007. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.-Y.; Fan, B.-F.; Yang, F.; DiBonaventura, M.; Chen, Y.-X.; Li, R.-Y.; King-Concialdi, K.; Kudel, I.; Hlavacek, P.; Hopps, M.; et al. Patient and economic burdens of postherpetic neuralgia in China. Clinicoeconomics Outcomes Res. 2019, 11, 539–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bridgeman, M.B.; Abazia, D.T. Medicinal Cannabis: History, Pharmacology, And Implications for the Acute Care Setting. Pharm. Ther. 2017, 42, 180–188. [Google Scholar]
- Di Marzo, V.; Piscitelli, F. The Endocannabinoid System and its Modulation by Phytocannabinoids. Neurotherapeutics 2015, 12, 692–698. [Google Scholar] [CrossRef]
- Mechoulam, R.; Parker, L.A. The endocannabinoid system and the brain. Annu. Rev. Psychol. 2013, 64, 21–47. [Google Scholar] [CrossRef] [Green Version]
- Allan, G.M.; Finley, C.R.; Ton, J.; Perry, D.; Ramji, J.; Crawford, K.; Lindblad, A.J.; Korownyk, C.; Kolber, M.R. Systematic review of systematic reviews for medical cannabinoids: Pain, nausea and vomiting, spasticity, and harms. Can. Fam. Physician 2018, 64, e78–e94. [Google Scholar]
- Silvestro, S.; Mammana, S.; Cavalli, E.; Bramanti, P.; Mazzon, E. Use of Cannabidiol in the Treatment of Epilepsy: Efficacy and Security in Clinical Trials. Molecules 2019, 24, 1459. [Google Scholar] [CrossRef] [Green Version]
- Nicholson, B.; Verma, S. Comorbidities in chronic neuropathic pain. Pain Med. 2004, 5 (Suppl. 1), S9–S27. [Google Scholar] [CrossRef]
- IASP. International Association for the Study of Pain Terminology. Available online: https://www.iasp-pain.org/resources/terminology/#neuropathic-pain (accessed on 8 November 2021).
- van Hecke, O.; Austin, S.K.; Khan, R.A.; Smith, B.H.; Torrance, N. Neuropathic pain in the general population: A systematic review of epidemiological studies. Pain 2014, 155, 654–662. [Google Scholar] [CrossRef]
- Campbell, J.N.; Meyer, R.A. Mechanisms of neuropathic pain. Neuron 2006, 52, 77–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansson, P. Neuropathic pain: Clinical characteristics and diagnostic workup. Eur. J. Pain 2002, 6, 47–50. [Google Scholar] [CrossRef] [PubMed]
- Smith, H.S.; Sang, C.N. The evolving nature of neuropathic pain: Individualizing treatment. Eur. J. Pain 2002, 6 (Suppl. B), 13–18. [Google Scholar] [CrossRef]
- Bates, D.; Schultheis, B.C.; Hanes, M.C.; Jolly, S.M.; Chakravarthy, K.V.; Deer, T.R.; Levy, R.M.; Hunter, C.W. A Comprehensive Algorithm for Management of Neuropathic Pain. Pain Med. 2019, 20, S2–S12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, R.A.; Chi, C.C.; Wiffen, P.J.; Derry, S.; Rice, A.S. Oral nonsteroidal anti-inflammatory drugs for neuropathic pain. Cochrane Database Syst. Rev. 2015, 10, CD010902. [Google Scholar] [CrossRef]
- Derry, S.; Sven-Rice, A.; Cole, P.; Tan, T.; Moore, R.A. Topical capsaicin (high concentration) for chronic neuropathic pain in adults. Cochrane Database Syst. Rev. 2013, 1, CD007393. [Google Scholar] [CrossRef] [Green Version]
- Knezevic, N.N.; Tverdohleb, T.; Nikibin, F.; Knezevic, I.; Candido, K.D. Management of chronic neuropathic pain with single and compounded topical analgesics. Pain Manag. 2017, 7, 537–558. [Google Scholar] [CrossRef]
- Kocot-Kępska, M.; Zajączkowska, R.; Mika, J.; Kopsky, D.J.; Wordliczek, J.; Dobrogowski, J.; Przeklasa-Muszyńska, A. Topical Treatments and Their Molecular/Cellular Mechanisms in Patients with Peripheral Neuropathic Pain-Narrative Review. Pharmaceutics 2021, 13, 450. [Google Scholar] [CrossRef]
- Rowbotham, M.C.; Davies, P.S.; Verkempinck, C.; Galer, B.S. Lidocaine patch: Double-blind controlled study of a new treatment method for post-herpetic neuralgia. Pain 1996, 65, 39–44. [Google Scholar] [CrossRef]
- Sansone, P.; Passavanti, M.B.; Fiorelli, A.; Aurilio, C.; Colella, U.; De Nardis, L.; Donatiello, V.; Pota, V.; Pace, M.C. Efficacy of the topical 5% lidocaine medicated plaster in the treatment of chronic post-thoracotomy neuropathic pain. Pain Manag. 2017, 7, 189–196. [Google Scholar] [CrossRef]
- Lunn, M.P.; Hughes, R.A.; Wiffen, P.J. Duloxetine for treating painful neuropathy, chronic pain or fibromyalgia. Cochrane Database Syst. Rev. 2014, 1, CD007115. [Google Scholar] [CrossRef]
- Moore, R.A.; Straube, S.; Wiffen, P.J.; Derry, S.; McQuay, H.J. Pregabalin for acute and chronic pain in adults. Cochrane Database Syst. Rev. 2009, 3, CD007076. [Google Scholar] [CrossRef] [PubMed]
- Gaskell, H.; Derry, S.; Stannard, C.; Moore, R.A. Oxycodone for neuropathic pain in adults. Cochrane Database Syst. Rev. 2016, 7, CD010692. [Google Scholar] [CrossRef] [PubMed]
- Elmofty, D.H.; Anitescu, M.; Buvanendran, A. Best practices in the treatment of neuropathic pain. Pain Manag. 2013, 3, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.P.; Vase, L.; Hooten, W.M. Chronic pain: An update on burden, best practices, and new advances. Lancet 2021, 397, 2082–2097. [Google Scholar] [CrossRef]
- Cristino, L.; Bisogno, T.; Di Marzo, V. Cannabinoids and the expanded endocannabinoid system in neurological disorders. Nat. Rev. Neurol. 2020, 16, 9–29. [Google Scholar] [CrossRef]
- Mackie, K. Cannabinoid receptors: Where they are and what they do. J. Neuroendocrinol. 2008, 20 (Suppl. 1), 10–14. [Google Scholar] [CrossRef]
- Colloca, L.; Ludman, T.; Bouhassira, D.; Baron, R.; Dickenson, A.H.; Yarnitsky, D.; Freeman, R.; Truini, A.; Attal, N.; Finnerup, N.B.; et al. Neuropathic pain. Nat. Rev. Dis. Primers 2017, 3, 17002. [Google Scholar] [CrossRef] [Green Version]
- Johal, H.; Devji, T.; Chang, Y.; Simone, J.; Vannabouathong, C.; Bhandari, M. Cannabinoids in Chronic Non-Cancer Pain: A Systematic Review and Meta-Analysis. Clin. Med. Insights Arthritis Musculoskelet. Disord. 2020, 13, 1179544120906461. [Google Scholar] [CrossRef] [Green Version]
- Xu, D.H.; Cullen, B.D.; Tang, M.; Fang, Y. The Effectiveness of Topical Cannabidiol Oil in Symptomatic Relief of Peripheral Neuropathy of the Lower Extremities. Curr. Pharm. Biotechnol. 2020, 21, 390–402. [Google Scholar] [CrossRef]
- Stella, B.; Baratta, F.; Della Pepa, C.; Arpicco, S.; Gastaldi, D.; Dosio, F. Cannabinoid Formulations and Delivery Systems: Current and Future Options to Treat Pain. Drugs 2021, 81, 1513–1557. [Google Scholar] [CrossRef]
- Maida, V.; Shi, R.B.; Fazzari, F.G.T.; Zomparelli, L. Topical cannabis-based medicines—A novel paradigm and treatment for non-uremic calciphylaxis leg ulcers: An open label trial. Int. Wound J. 2020, 17, 1508–1516. [Google Scholar] [CrossRef]
- Maayah, Z.H.; Takahara, S.; Ferdaoussi, M.; Dyck, J.R.B. The molecular mechanisms that underpin the biological benefits of full-spectrum cannabis extract in the treatment of neuropathic pain and inflammation. Biochim. Biophys. Acta (BBA) Mol. Basis Dis. 2020, 1866, 165771. [Google Scholar] [CrossRef]
- Dopkins, N.; Miranda, K.; Wilson, K.; Holloman, B.L.; Nagarkatti, P.; Nagarkatti, M. Effects of Orally Administered Cannabidiol on Neuroinflammation and Intestinal Inflammation in the Attenuation of Experimental Autoimmune Encephalomyelitis. J. Neuroimmune Pharmacol. 2021, 1–18. [Google Scholar] [CrossRef]
- Mücke, M.; Phillips, T.; Radbruch, L.; Petzke, F.; Häuser, W. Cannabis-based medicines for chronic neuropathic pain in adults. Cochrane Database Syst. Rev. 2018, 3, Cd012182. [Google Scholar]
- Joshi, N.; Onaivi, E.S. Endocannabinoid System Components: Overview and Tissue Distribution. Adv. Exp. Med. Biol. 2019, 1162, 1–12. [Google Scholar]
- Almogi-Hazan, O.; Or, R. Cannabis, the Endocannabinoid System and Immunity-the Journey from the Bedside to the Bench and Back. Int. J. Mol. Sci. 2020, 21, 4448. [Google Scholar] [CrossRef]
- Wang, L.; Hong, P.J.; May, C.; Rehman, Y.; Oparin, Y.; Hong, C.J.; Hong, B.Y.; AminiLari, M.; Gallo, L.; Kaushal, A.; et al. Medical cannabis or cannabinoids for chronic non-cancer and cancer related pain: A systematic review and meta-analysis of randomised clinical trials. Bmj 2021, 374, n1034. [Google Scholar] [CrossRef]
- Jensen, B.; Chen, J.; Furnish, T.; Wallace, M. Medical Marijuana and Chronic Pain: A Review of Basic Science and Clinical Evidence. Curr. Pain Headache Rep. 2015, 19, 50. [Google Scholar] [CrossRef]
- Nielsen, S.; Germanos, R.; Weier, M.; Pollard, J.; Degenhardt, L.; Hall, W.; Buckley, N.; Farrell, M. The Use of Cannabis and Cannabinoids in Treating Symptoms of Multiple Sclerosis: A Systematic Review of Reviews. Curr. Neurol. Neurosci. Rep. 2018, 18, 8. [Google Scholar] [CrossRef]
- Friedman, D.; French, J.A.; Maccarrone, M. Safety, efficacy, and mechanisms of action of cannabinoids in neurological disorders. Lancet Neurol. 2019, 18, 504–512. [Google Scholar] [CrossRef]
- Paudel, K.S.; Hammell, D.C.; Agu, R.U.; Valiveti, S.; Stinchcomb, A.L. Cannabidiol bioavailability after nasal and transdermal application: Effect of permeation enhancers. Drug Dev. Ind. Pharm. 2010, 36, 1088–1097. [Google Scholar] [CrossRef] [PubMed]
- Hagenbach, U.; Luz, S.; Ghafoor, N.; Berger, J.M.; Grotenhermen, F.; Brenneisen, R.; Mäder, M. The treatment of spasticity with Delta9-tetrahydrocannabinol in persons with spinal cord injury. Spinal Cord 2007, 45, 551–562. [Google Scholar] [CrossRef] [PubMed]
- Phan, N.Q.; Siepmann, D.; Gralow, I.; Ständer, S. Adjuvant topical therapy with a cannabinoid receptor agonist in facial postherpetic neuralgia. J. Dtsch. Dermatol. Ges. 2010, 8, 88–91. [Google Scholar] [CrossRef]
- Eskander, J.P.; Spall, J.; Spall, A.; Shah, R.V.; Kaye, A.D. Cannabidiol (CBD) as a treatment of acute and chronic back pain: A case series and literature review. J. Opioid Manag. 2020, 16, 215–218. [Google Scholar] [CrossRef]
- Jain, A.K.; Ryan, J.R.; McMahon, F.G.; Smith, G. Evaluation of intramuscular levonantradol and placebo in acute postoperative pain. J. Clin. Pharmacol. 1981, 21, 320s–326s. [Google Scholar] [CrossRef]
- Schindler, E.A.D.; Schnakenberg Martin, A.M.; Sewell, R.A.; Ranganathan, M.; DeForest, A.; Pittman, B.P.; Perrino, A., Jr.; D’Souza, D.C. In an exploratory randomized, double-blind, placebo-controlled, cross-over study, psychoactive doses of intravenous delta-9-tetrahydrocannabinol fail to produce antinociceptive effects in healthy human volunteers. Psychopharmacology 2020, 237, 3097–3107. [Google Scholar] [CrossRef]
- Boychuk, D.G.; Goddard, G.; Mauro, G.; Orellana, M.F. The effectiveness of cannabinoids in the management of chronic nonmalignant neuropathic pain: A systematic review. J. Oral Facial Pain Headache 2015, 29, 7–14. [Google Scholar] [CrossRef] [Green Version]
- Meng, H.; Johnston, B.; Englesakis, M.; Moulin, D.E.; Bhatia, A. Selective Cannabinoids for Chronic Neuropathic Pain: A Systematic Review and Meta-analysis. Anesth. Analg. 2017, 125, 1638–1652. [Google Scholar]
- Dykukha, I.; Malessa, R.; Essner, U.; Überall, M.A. Nabiximols in Chronic Neuropathic Pain: A Meta-Analysis of Randomized Placebo-Controlled Trials. Pain Med. 2021, 22, 861–874. [Google Scholar] [CrossRef]
- Vecchio, D.; Varrasi, C.; Virgilio, E.; Spagarino, A.; Naldi, P.; Cantello, R. Cannabinoids in multiple sclerosis: A neurophysiological analysis. Acta Neurol. Scand. 2020, 142, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Markovà, J.; Essner, U.; Akmaz, B.; Marinelli, M.; Trompke, C.; Lentschat, A.; Vila, C. Sativex® as add-on therapy vs. further optimized first-line ANTispastics (SAVANT) in resistant multiple sclerosis spasticity: A double-blind, placebo-controlled randomised clinical trial. Int. J. Neurosci. 2019, 129, 119–128. [Google Scholar] [CrossRef]
- Devinsky, O.; Patel, A.D.; Cross, J.H.; Villanueva, V.; Wirrell, E.C.; Privitera, M.; Greenwood, S.M.; Roberts, C.; Checketts, D.; VanLandingham, K.E.; et al. Effect of Cannabidiol on Drop Seizures in the Lennox-Gastaut Syndrome. N. Engl. J. Med. 2018, 378, 1888–1897. [Google Scholar] [CrossRef] [Green Version]
- Patel, A.D.; Mazurkiewicz-Bełdzińska, M.; Chin, R.F.; Gil-Nagel, A.; Gunning, B.; Halford, J.J.; Mitchell, W.; Scott Perry, M.; Thiele, E.A.; Weinstock, A.; et al. Long-term safety and efficacy of add-on cannabidiol in patients with Lennox-Gastaut syndrome: Results of a long-term open-label extension trial. Epilepsia 2021, 62, 2228–2239. [Google Scholar] [CrossRef]
- Devinsky, O.; Patel, A.D.; Thiele, E.A.; Wong, M.H.; Appleton, R.; Harden, C.L.; Greenwood, S.; Morrison, G.; Sommerville, K. Randomized, dose-ranging safety trial of cannabidiol in Dravet syndrome. Neurology 2018, 90, e1204–e1211. [Google Scholar] [CrossRef] [Green Version]
- Miller, I.; Scheffer, I.E.; Gunning, B.; Sanchez-Carpintero, R.; Gil-Nagel, A.; Perry, M.S.; Saneto, R.P.; Checketts, D.; Dunayevich, E.; Knappertz, V. Dose-Ranging Effect of Adjunctive Oral Cannabidiol vs Placebo on Convulsive Seizure Frequency in Dravet Syndrome: A Randomized Clinical Trial. JAMA Neurol. 2020, 77, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.A.; Azariah, F.; Lavender, V.T.; Stoner, N.S.; Bettiol, S. Cannabinoids for nausea and vomiting in adults with cancer receiving chemotherapy. Cochrane Database Syst. Rev. 2015, 2015, Cd009464. [Google Scholar]
- Badowski, M.E.; Yanful, P.K. Dronabinol oral solution in the management of anorexia and weight loss in AIDS and cancer. Ther. Clin. Risk Manag. 2018, 14, 643–651. [Google Scholar] [CrossRef] [Green Version]
- First, L.; Douglas, W.; Habibi, B.; Singh, J.R.; Sein, M.T. Cannabis Use and Low-Back Pain: A Systematic Review. Cannabis Cannabinoid Res. 2020, 5, 283–289. [Google Scholar] [CrossRef]
- Haanpää, M.; Attal, N.; Backonja, M.; Baron, R.; Bennett, M.; Bouhassira, D.; Cruccu, G.; Hansson, P.; Haythornthwaite, J.A.; Iannetti, G.D.; et al. NeuPSIG guidelines on neuropathic pain assessment. Pain 2011, 152, 14–27. [Google Scholar] [CrossRef]
- Bennett, M.I.; Attal, N.; Backonja, M.M.; Baron, R.; Bouhassira, D.; Freynhagen, R.; Scholz, J.; Tölle, T.R.; Wittchen, H.U.; Jensen, T.S. Using screening tools to identify neuropathic pain. Pain 2007, 127, 199–203. [Google Scholar] [CrossRef]
- Torrance, N.; Smith, B.H.; Bennett, M.I.; Lee, A.J. The epidemiology of chronic pain of predominantly neuropathic origin. Results from a general population survey. J. Pain 2006, 7, 281–289. [Google Scholar] [CrossRef]
- Freynhagen, R.; Baron, R.; Gockel, U.; Tölle, T.R. painDETECT: A new screening questionnaire to identify neuropathic components in patients with back pain. Curr. Med. Res. Opin. 2006, 22, 1911–1920. [Google Scholar] [CrossRef]
- Bouhassira, D.; Attal, N.; Alchaar, H.; Boureau, F.; Brochet, B.; Bruxelle, J.; Cunin, G.; Fermanian, J.; Ginies, P.; Grun-Overdyking, A.; et al. Comparison of pain syndromes associated with nervous or somatic lesions and development of a new neuropathic pain diagnostic questionnaire (DN4). Pain 2005, 114, 29–36. [Google Scholar] [CrossRef]
- Jensen, M.P. Using pain quality assessment measures for selecting analgesic agents. Clin. J. Pain 2006, 22, S9–S13. [Google Scholar] [CrossRef]
- Galer, B.S.; Jensen, M.P. Development and preliminary validation of a pain measure specific to neuropathic pain: The Neuropathic Pain Scale. Neurology 1997, 48, 332–338. [Google Scholar] [CrossRef]
- Higgins, J.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A.; Flemyng, E. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.2; (Updated February 2021): Cochrane, 2021; John Wiley & Sons: Chichester, UK, 2021; Available online: www.training.cochrane.org/handbook (accessed on 15 November 2021).
- Dworkin, R.H.; Turk, D.C.; Peirce-Sandner, S.; Baron, R.; Bellamy, N.; Burke, L.B.; Chappell, A.; Chartier, K.; Cleeland, C.S.; Costello, A.; et al. Research design considerations for confirmatory chronic pain clinical trials: IMMPACT recommendations. Pain 2010, 149, 177–193. [Google Scholar] [CrossRef]
- Dworkin, R.H.; Turk, D.C.; Wyrwich, K.W.; Beaton, D.; Cleeland, C.S.; Farrar, J.T.; Haythornthwaite, J.A.; Jensen, M.P.; Kerns, R.D.; Ader, D.N.; et al. Interpreting the clinical importance of treatment outcomes in chronic pain clinical trials: IMMPACT recommendations. J. Pain 2008, 9, 105–121. [Google Scholar] [CrossRef]
- The Cochrane Collaboration. Review Manager (RevMan); The Cochrane Collaboration: London, UK, 2020. [Google Scholar]
- Busse, J.W.; Wang, L.; Kamaleldin, M.; Craigie, S.; Riva, J.J.; Montoya, L.; Mulla, S.M.; Lopes, L.C.; Vogel, N.; Chen, E.; et al. Opioids for Chronic Noncancer Pain: A Systematic Review and Meta-analysis. JAMA 2018, 320, 2448–2460. [Google Scholar] [CrossRef]
- Schünemann, H.J.; Guyatt, G.H. Commentary--goodbye M(C)ID! Hello MID, where do you come from? Health Serv. Res. 2005, 40, 593–597. [Google Scholar] [CrossRef]
- Zisapel, N.; Nir, T. Determination of the minimal clinically significant difference on a patient visual analog sleep quality scale. J. Sleep Res. 2003, 12, 291–298. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. Bmj 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Author | Design | Description | Gender | Age (yrs) | n | Outcome Pain Measures | Outcome Intervals | p Value Treatment Effect |
|---|---|---|---|---|---|---|---|---|
| Xu et al. (2020) | Single-centre, double-blind, randomized, placebo-controlled trial | Assess the efficacy of a topically delivered CBD oil in management of NP | M/F 18/11 | 35–79 | 29 | Self-reported: pain and specific sensations were evaluated using the NPS in 10 domains of pain: sharp, hot, dull, cold, sensitive, itchy, deep and surface | Baseline, 2 and 4 weeks | Overall: 0.00901 |
| Articles | Study Design | Description | Age (Years) | Size | Outcome Pain Measures | Outcome Intervals | Reason for Exclusion |
|---|---|---|---|---|---|---|---|
| Hagenbach et al. (2007) | Prospective | Assess the efficacy and side effects of oral D9-THC and rectal THC-HS in SCI patients, but the rectal arm was not performed | 29–66 | 21 | Self-reported: spasticity sum score using the MAS, self-ratings of VAS and spasticity | Baseline, 8 and 43 days | Did not assess routes other than oral or inhalation |
| Phan et al. (2009) | Prospective | Explores the analgesic efficacy of adjuvant therapy with a topical cannabinoid agonist in PHN patients with facial involvement | 48–79 | 8 | VAS | Baseline, 2 and 4 weeks | Did not include a control group |
| Eskander et al. (2020) | Retrospective | Describes the use of a hemp-derived CBD in a topical cream for the symptomatic relief in acute and chronic back pain | 40–61 | 2 | VAS | Baseline, 8 h and 4 weeks | Case report without a control group |
| Jain et al. (1981) | Prospective | Evaluation of intramuscular levonantradol and placebo in acute postoperative pain in patients with moderate to severe postoperative or trauma pain | 25.3 ± 5 30.2 ± 11 | 56 | Four point scale | Baseline, 15, 30, and 60 min, and hourly thereafter for a total of 6 h | Did not include patients with neuropathic pain |
| Schindler et al. (2019) | Prospective | Psychoactive doses of intravenous D9-THC in healthy volunteers induce chemical pain and hyperalgesia with capsaicin, mechanical (von Frey filament), hot and cold (thermode), and electrical (pulse generator) | 19–51 | 6 | VAS, MPQ-SF | Before drug administration, peak drug effects, and 2 h after drug administration | Study performed in healthy subjects, did not include patients with neuropathic pain |
| Risk of Bias | Observations | |
|---|---|---|
| Random sequence generation (selection bias) | Low | |
| Allocation concealment (selection bias) | High | The authors did not provide details about the method of allocation concealment and in the baseline variables there were apparent imbalance between the CBD and placebo groups in the following variables: Gender, previous CBD use, Vibratory Sensation, and NPS domains of Intense, Sharp, Itchy, Deep, Surface. Such imbalance could be due to deficiencies in the randomization process due to insufficient concealment |
| Blinding of participants and personnel (performance bias) | Unclear | The study had an open label phase, and it is not clear how much this influenced some of the statistical analyses |
| Blinding of outcomes assessment (detection bias) | Unclear | The study had an open label phase, and it is not clear how much this influenced some of the statistical analyses |
| Incomplete outcome data (attrition bias) | High | The lost to follow-up rate was high, about 20% (3 subjects in each arm) |
| Selective outcome reporting (reporting bias) | High | When other common methods to assess the intervention effectivity, like the change of NPS scores from baseline to week 4 (end of RCT blinded phase) are performed to the study data the benefits of the intervention are not confirmed and the protocol of the study was not published before its beginning |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quintero, J.-M.; Pulido, G.; Giraldo, L.-F.; Leon, M.-X.; Diaz, L.-E.; Bustos, R.-H. A Systematic Review on Cannabinoids for Neuropathic Pain Administered by Routes Other than Oral or Inhalation. Plants 2022, 11, 1357. https://doi.org/10.3390/plants11101357
Quintero J-M, Pulido G, Giraldo L-F, Leon M-X, Diaz L-E, Bustos R-H. A Systematic Review on Cannabinoids for Neuropathic Pain Administered by Routes Other than Oral or Inhalation. Plants. 2022; 11(10):1357. https://doi.org/10.3390/plants11101357
Chicago/Turabian StyleQuintero, Jose-Manuel, German Pulido, Luis-Fernando Giraldo, Marta-Ximena Leon, Luis-Eduardo Diaz, and Rosa-Helena Bustos. 2022. "A Systematic Review on Cannabinoids for Neuropathic Pain Administered by Routes Other than Oral or Inhalation" Plants 11, no. 10: 1357. https://doi.org/10.3390/plants11101357
APA StyleQuintero, J.-M., Pulido, G., Giraldo, L.-F., Leon, M.-X., Diaz, L.-E., & Bustos, R.-H. (2022). A Systematic Review on Cannabinoids for Neuropathic Pain Administered by Routes Other than Oral or Inhalation. Plants, 11(10), 1357. https://doi.org/10.3390/plants11101357