

Investigation of the Effectiveness of the Robotic ReStore Soft Exoskeleton in the Development of Early Mobilization, Walking, and Coordination of Stroke Patients: A Randomized Clinical Trial

 ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
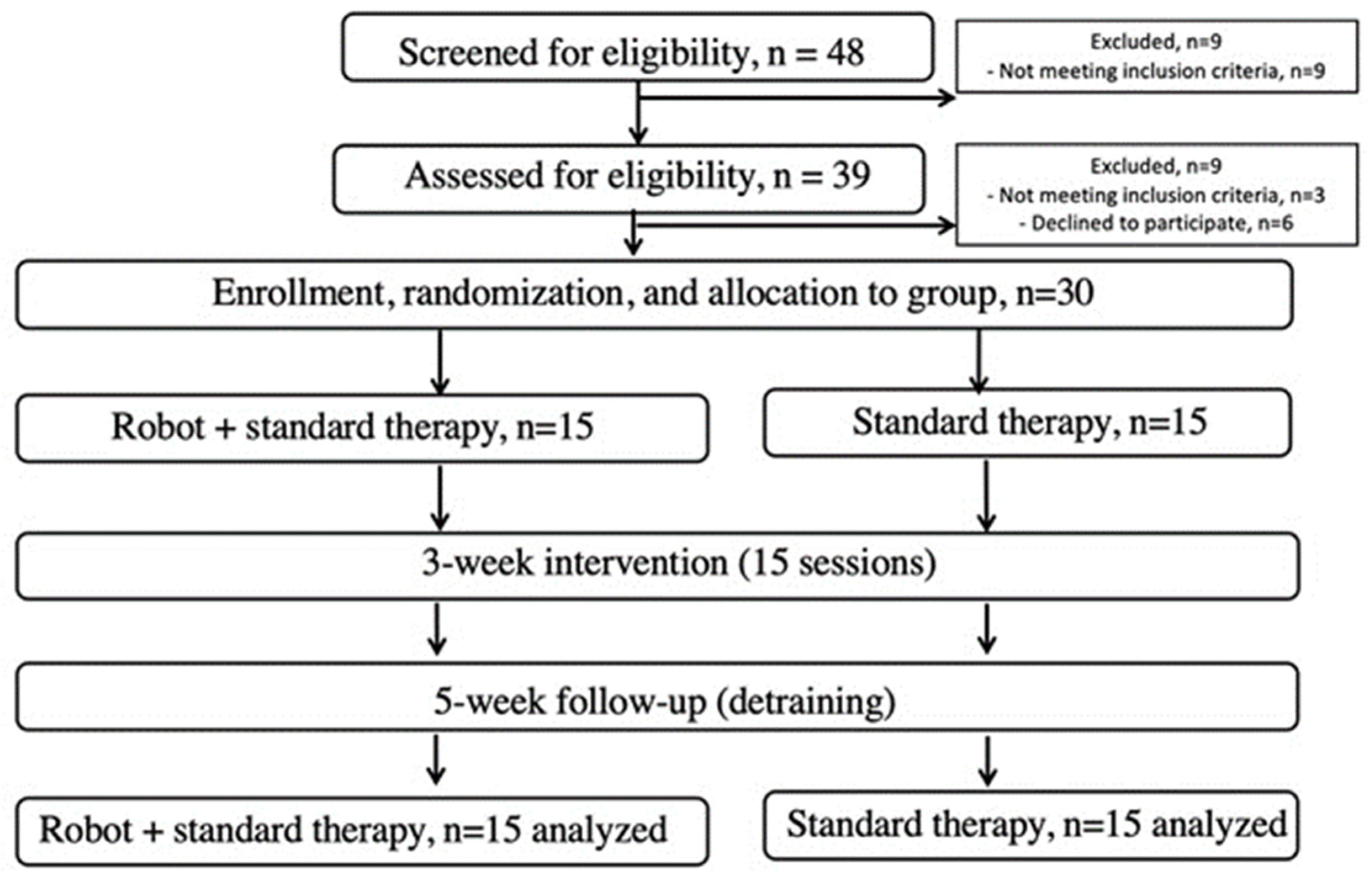
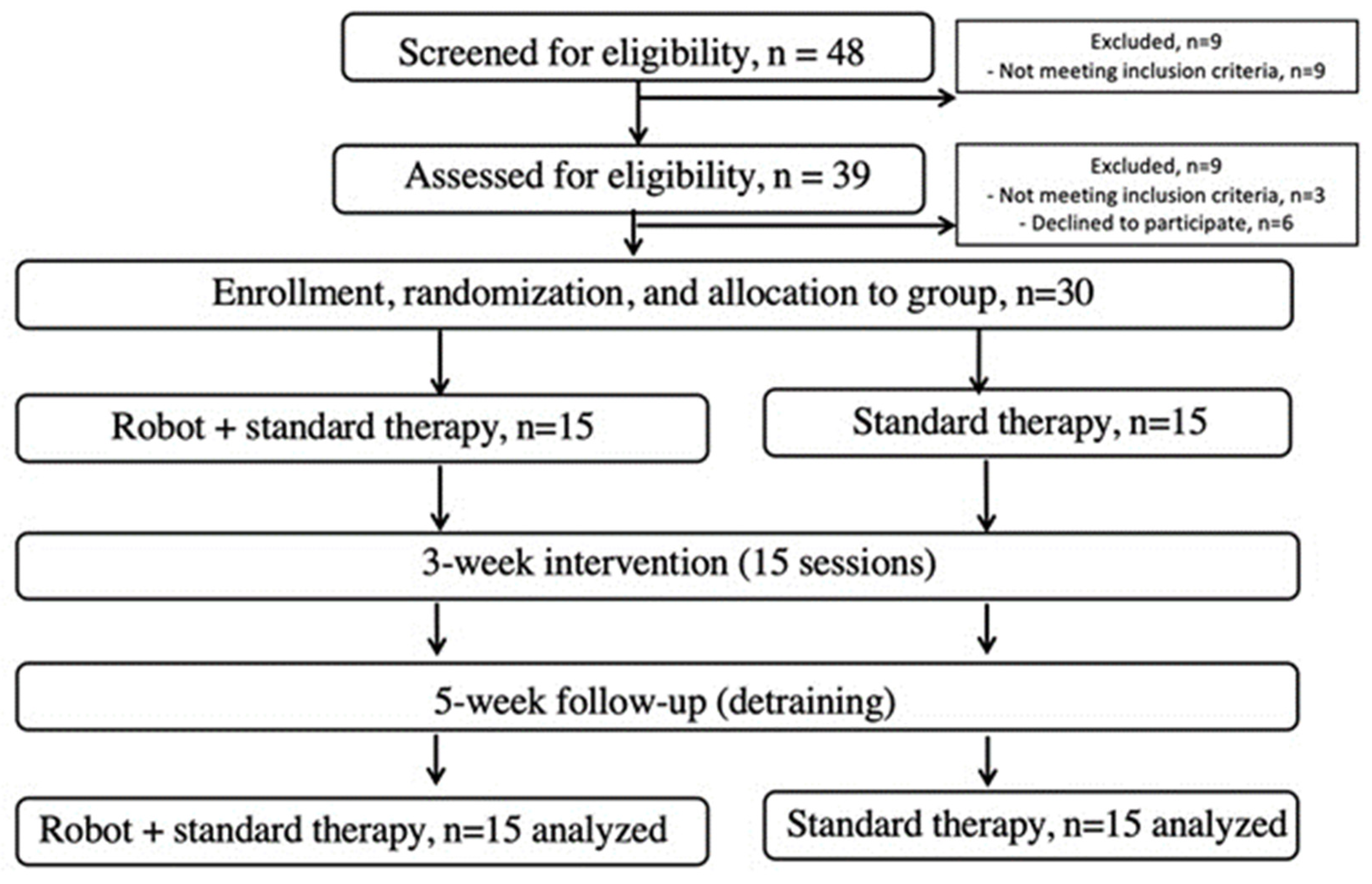
2.1. Participants and Design
2.2. Outcomes
2.2.1. Primary Outcomes
2.2.2. Secondary Outcomes
2.3. Intervention
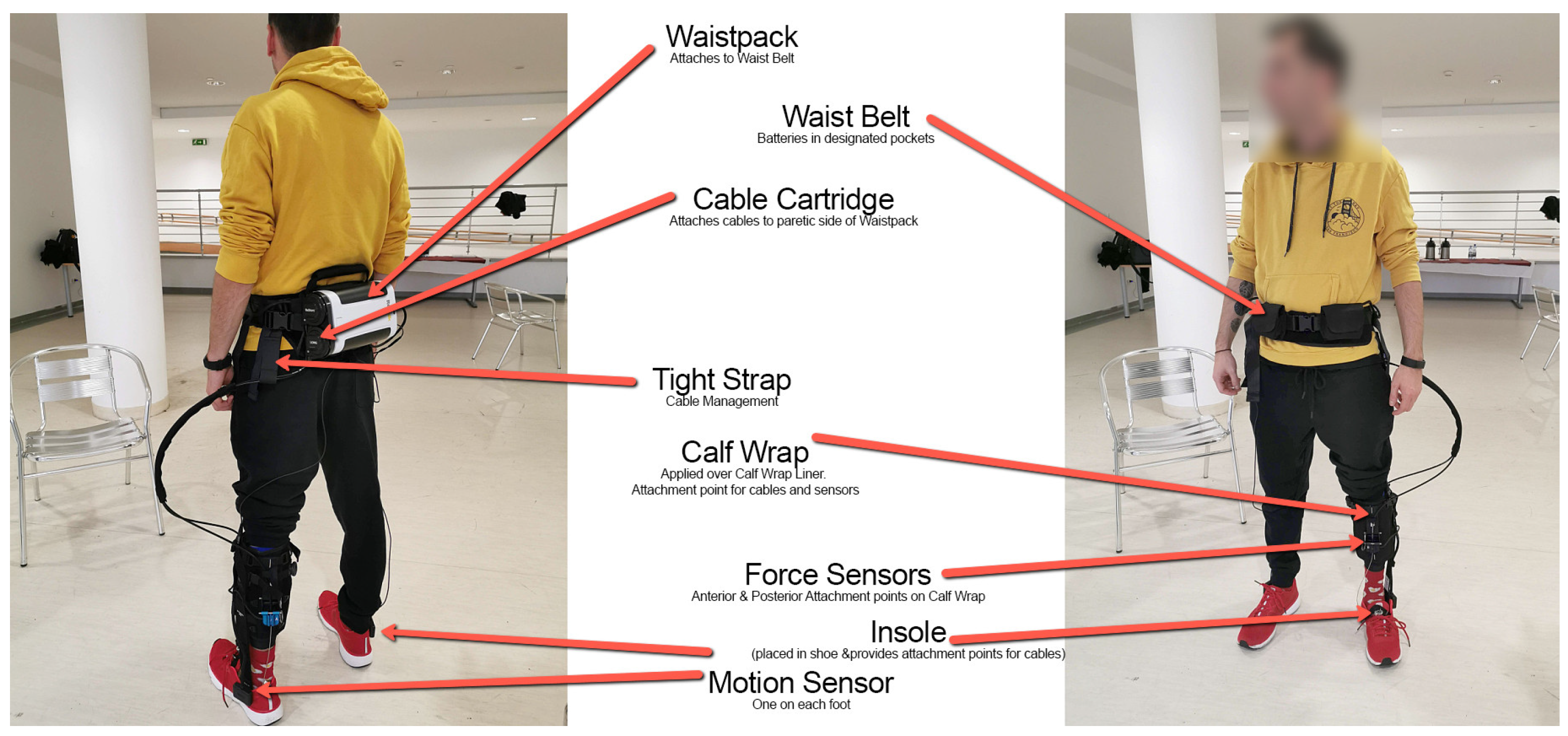
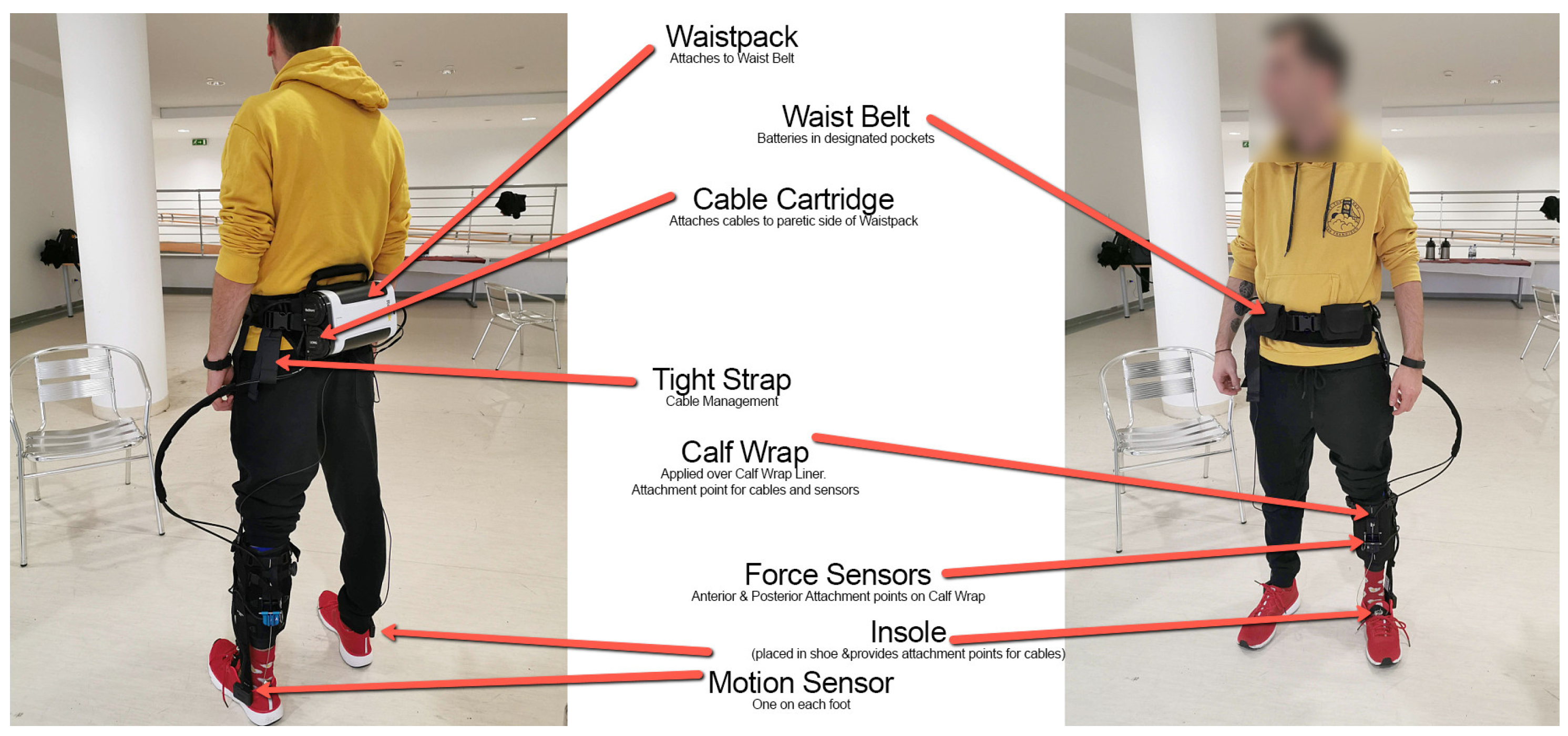
2.3.1. Robot-Assisted Gait Therapy (ROB) Group
2.3.2. Standard Therapy Treatment (STT) Group
2.4. Statistical Analyses
3. Results
3.1. Baseline Characteristics
3.2. Intervention Effects
3.3. Primary Outcome
3.4. Secondary Outcomes
4. Discussion
5. Limitations
6. Conclusions
7. Suppliers
- MediTECH Electronic GmbH, 95
- ReWalk system: Restore, soft exoskeleton
- Statistical Package for the Social Sciences, SPSS, version 22; IBM.
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ROB | Robot-Assisted Gait Therapy |
| STT | Standard Therapy Treatment |
| MRS | Modified Rankin Scale |
| BI | Barthel Index |
| BBS | Berg Balance Scale |
| 6MWT | 6 Minute Walk Test |
| CT | Computed Tomography |
| MRI | Magnetic Resonance Imaging |
| rSBP | Resting Systolic Blood Pressure |
| IT | Inertial Technology |
| PwST | Patients with Stroke |
| ReStore Soft Exo Suit | Robotic Exoskeleton Device |
| ReWalk | Manufacturer of Robotic Exoskeleton |
| cm | Centimeters |
| m | Meters |
| m/s | Meters per Second |
| min | Minutes |
| SD | Standard Deviation |
| G*Power | Statistical Power Analysis Software |
| η2 | Eta-squared (Effect Size) |
| PSdep | Probability of Superiority for Dependent Samples |
| NEC | Eyes Closed |
| STT | Soft Exoskeleton |
References
- Esquenazi, A.; Talaty, M.; Packel, A.; Saulino, M. The ReWalk powered exoskeleton to restore ambulatory function to individuals with thoracic-level motor-complete spinal cord injury. Am. J. Phys. Med. Rehabil. 2013, 92, 617–624. [Google Scholar] [CrossRef]
- Shi, D.; Zhang, W.; Zhang, W.; Ding, X. A Review on Lower Limb Rehabilitation Exoskeleton Robots. Chin. J. Mech. Eng. 2019, 32, 74. [Google Scholar] [CrossRef]
- Fichtinger, G.; Troccaz, J.; Haidegger, T. Image-Guided Interventional Robotics: Lost in Translation? Proc. IEEE 2022, 110, 932–950. [Google Scholar] [CrossRef]
- Haidegger, T.; Speidel, S.; Stoyanov, D.; Satava, R.M. Robot-assisted minimally invasive surgery—Surgical robotics in the data age. Proc. IEEE 2022, 110, 835–846. [Google Scholar] [CrossRef]
- Haidegger, T.; Mai, V.; Mörch, C.; Boesl, D.; Jacobs, A.; Rao, R.B.; Khamis, A.; Lach, L.; Vanderborght, B. Robotics: Enabler and inhibitor of the Sustainable Development Goals. Sustain. Prod. Consum. 2023, 43, 422–434. [Google Scholar] [CrossRef]
- Han, S.; Wang, H.; Yu, H. Human–Robot Interaction Evaluation-Based AAN Control for Upper Limb Rehabilitation Robots Driven by Series Elastic Actuators. IEEE Trans. Robot. 2023, 39, 3437–3451. [Google Scholar] [CrossRef]
- Tollár, J.; Vetrovsky, T.; Széphelyi, K.; Csutorás, B.; Prontvai, N.; Ács, P.; Hortobágyi, T. Effects of 2-year-long Maintenance Training and Detraining on 558 Subacute Ischemic Stroke Patients’; Clinical-Motor Symptoms. Med. Sci. Sports Exerc. 2022, 55, 607–613. [Google Scholar] [CrossRef]
- Kim, H.; Lee, S.; Yoon, B. Effects of wearable robot-assisted gait training on walking ability and quality in individuals with stroke: A systematic review and meta-analysis. Clin. Rehabil. 2019, 33, 1315–1328. [Google Scholar]
- Cai, L.; Chen, C.; Chen, Y.; Wu, J. Exoskeleton rehabilitation robot training methods for stroke rehabilitation: A systematic review. J. Neuroeng. Rehabil. 2018, 15, 1–15. [Google Scholar]
- Loureiro, R.C.; Collin, C.A.; Harwin, W.S. Upper limb robot mediated stroke therapy—GENTLE/s approach. Auton. Robot. 2019, 43, 733–746. [Google Scholar]
- Huo, W.; Xia, C.; Wang, J.; Ma, X. A review of wearable lower limb exoskeletons for gait training. Disabil. Rehabil. Assist. Technol. 2020, 1–16. [Google Scholar]
- Da Silva Cameirão, M.; Bermúdez IBadia, S.; Duarte, E.; Verschure, P.F. Virtual reality-based rehabilitation speeds up functional recovery of the upper extremities after stroke: A randomized controlled pilot study in the acute phase of stroke using the Rehabilitation Gaming System. Restor. Neurol. Neurosci. 2011, 29, 287–298. [Google Scholar] [CrossRef]
- Kazerooni, H.; Steger, R. (Eds.) Exoskeletons in Rehabilitation Robotics: Tremor Suppression; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2014. [Google Scholar]
- Gorgey, A.S. Robotic exoskeletons: The current pros and cons. World J. Orthop. 2018, 9, 112. [Google Scholar] [CrossRef] [PubMed]
- Loureiro, R.C.; Harwin, W.S. Exoskeletons and active orthoses: Literature review, design examples and future directions. Med. Eng. Phys. 2016, 38, 1159–1173. [Google Scholar]
- Veneman, J.F.; Kruidhof, R.; Hekman, E.E.; Ekkelenkamp, R.; Van Asseldonk, E.H.; Van der Kooij, H. Design and evaluation of the LOPES exoskeleton robot for interactive gait rehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2007, 15, 379–386. [Google Scholar] [CrossRef] [PubMed]
- Moreno, J.C.; Castermans, T.; Hoellinger, T.; Maciejasz, P.; Dupeyron, A. The CYBERLEGs exoskeleton: An autonomous wearable robot for supporting people with mobility impairments. IEEE Robot. Autom. Mag. 2011, 18, 37–45. [Google Scholar]
- Esquenazi, A.; Talaty, M.; Jayaraman, A. Powered exoskeletons for walking assistance in persons with central nervous system injuries: A narrative review. PMR 2016, 9, 46–62. [Google Scholar] [CrossRef]
- Asbeck, A.T.; De Rossi, S.; Holt, K.G.; Walsh, C.J. A biologically inspired soft exosuit for walking assistance. Int. J. Robot. Res. 2015, 34, 744–762. [Google Scholar] [CrossRef]
- Polygerinos, P.; Galloway, K.C.; Savage, E.; Herman, M.; Walsh, C.J. EMG controlled soft robotic glove for assistance during activities of daily living. Robot. Auton. Syst. 2015, 73, 171–178. [Google Scholar]
- Park, S.; Ha, J.W.; Kim, J. Soft exosuit for hip assistance with a soft posterior module. Soft Robot. 2018, 5, 700–711. [Google Scholar]
- Panizzolo, F.A.; Galiana, I.; Asbeck, A.T.; Siviy, C.; Schmidt, K.; Holt, K.G.; Walsh, C.J. A biologically inspired multi-joint soft exosuit that can reduce the energy cost of loaded walking. J. Neuroeng. Rehabil. 2016, 13, 43. [Google Scholar] [CrossRef] [PubMed]
- Quinlivan, B.T.; Lee, S.; Malcolm, P.; Rossi, D.M.; Grimmer, M.; Siviy, C.; Karavas, N.; Wagner, D.; Asbeck, A.; Galiana, I.; et al. Assistance magnitude versus metabolic cost reductions for a tethered multiarticular soft exosuit. Sci. Robot. 2017, 2, eaah4416. [Google Scholar] [CrossRef] [PubMed]
- Ding, Y.; Panizzolo, F.A.; Siviy, C.; Malcolm, P.; Galiana, I.; Walsh, C.J. Effect of timing of hip extension assistance during loaded walking with a soft exosuit. J. Neuroeng. Rehabil. 2018, 15, 87. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and bio- medical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power for the Behavioral Sciences; Erblaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Karunakaran, K.K.; Gute, S.; Ames, G.R.; Chervin, K.; Dandola, C.M.; Nolan, J.K. Effect of robotic exoskeleton gait training during acute stroke on functional ambulation. NeuroRehabilitation 2021, 48, 493–503. [Google Scholar] [CrossRef] [PubMed]
- Bauer, M.O.; Vizi, M.B.; Galambos, P.; Szalay, T. Direct drive hand exoskeleton for robot-assisted post stroke rehabilitation. Acta Polytech. Hung. 2021, 18, 37–54. [Google Scholar] [CrossRef]
- Di Tommaso, F.; Tamburella, F.; Lorusso, M.; Gastaldi, L.; Molinari, M.; Tagliamonte, N.L. Biomechanics of Exoskeleton-Assisted Treadmill Walking. In Proceedings of the 2023 International Conference on Rehabilitation Robotics (ICORR), Singapore, 24–28 September 2023; pp. 1–6. [Google Scholar] [CrossRef]
- Chisholm, A.E.; Alamro, R.A.; Williams, A.M.M.; Lam, T. Overground vs. treadmill-based robotic gait training to improve seated balance in people with motor-complete spinal cord injury: A case report. J. Neuroeng. Rehabil. 2017, 14, 27. [Google Scholar] [CrossRef] [PubMed]
- Awad, L.N.; Esquenazi, A.; Francisco, G.E.; Nolan, K.J.; Jayaraman, A. The ReWalk ReStore™ soft robotic exosuit: A multi-site clinical trial of the safety, reliability, and feasibility of exosuit-augmented post-stroke gait rehabilitation. J. Neuroeng. Rehabil. 2020, 17, 80. [Google Scholar] [CrossRef]
- Awad, L.N.; Bae, J.; O’donnell, K.; De Rossi, S.M.; Hendron, K.; Sloot, L.H.; Kudzia, P.; Allen, S.; Holt, K.G.; Ellis, T.D.; et al. A soft robotic exosuit improves walking in patients after stroke. Sci. Transl. Med. 2017, 9, eaai9084. [Google Scholar] [CrossRef]
- Grissom, R.J.; Kim, J.J. Effect Sizes for Research: Univariate and Multivariate Applications, 2nd ed.; Routledge: London, UK, 2012. [Google Scholar]
- Tollar, J.; Nagy, F.; Csutoras, B.; Prontvai, N.; Nagy, Z.; Török, K.; Blényesi, E.; Vajda, Z.; Farkas, D.; Tóth, B.E.; et al. High Frequency and Intensity Rehabilitation in 641 Subacute Ischemic Stroke Patients. Arch. Phys. Med. Rehabil. 2021, 102, 9–18. [Google Scholar] [CrossRef]
- Calafiore, D.; Negrini, F.; Tottoli, N.; Ferraro, F.; Ozyemisci-Taskiran, O.; de Sire, A. Efficacy of robotic exoskeleton for gait rehabilitation in patients with subacute stroke: A systematic review. Eur. J. Phys. Rehabil. Med. 2021, 58, 1–8. [Google Scholar] [CrossRef]
- Postol, N.; Grissel, J.; McHugh, C.; Bivard, A.; Spratt, N.J.; Marquez, J. Effects of therapy with a free-standing robotic exoskeleton on motor function and other health indicators in people with severe mobility impairment due to chronic stroke: A quasi-controlled study. J. Rehabil. Assist. Technol. Eng. 2021, 8, 3–4. [Google Scholar] [CrossRef]
- Awad, L.N.; Kudzia, P.; Revi, D.A.; Ellis, T.D.; Walsh, C.J. Walking faster and farther with a soft robotic exosuit: Implications for post-stroke gait assistance and rehabilitation. IEEE Open J. Eng. Med. Biol. 2020, 1, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Yang, S.; Xue, Q. Lower limb rehabilitation exoskeleton robot: A review. Adv. Mech. Eng. 2021, 13, 1–17. [Google Scholar] [CrossRef]
- Sarajchi, M.; Sirlantzis, K. Pediatric Robotic Lower-Limb Exoskeleton: An Innovative Design and Kinematic Analysis. IEEE Access 2023, 11, 115219–115230. [Google Scholar] [CrossRef]
- Vassallo, C.; Zinni, G.; Maludrottu, S.; Laffranchi, M.; De Michieli, L. Stairs and ramps ascent and descent: How to design feasible gait patterns for a powered lower-limb exoskeleton. In Proceedings of the 2022 9th IEEE RAS/EMBS International Conference for Biomedical Robotics and Biomechatronics (BioRob), Seoul, Republic of Korea, 21–24 August 2022; pp. 1–6. [Google Scholar] [CrossRef]
- Pentek, M.; Zrubka, Z.; Gulacsi, L.; Weszl, M.; Czere, J.T.; Tamás, P. 10 pragmatic points to consider when performing a systematic literature review of clinical evidence on digital medical devices. Acta Polytech. Hung. 2023, 20, 110–128. [Google Scholar]
- Zah, V.; Burrell, A.; Asche, C.; Zrubka, Z. Paying for Digital Health Interventions-What Evidence is Needed? Acta Polytech. Hung. 2022, 19, 179–199. [Google Scholar] [CrossRef]
- Hölgyesi, Á.; Zrubka, Z.; Gulácsi, L.; Baji, P.; Tamás, H.; Kozlovszky, M.; Weszl, M.; Kovács, L.; Péntek, M. Robot-assisted surgery and artificial intelligence-based tumour diag-nostics: Social preferences with a representative cross-sectional survey. BMC Med. Inform. Decis. Mak. 2024, 24, 1–12, article in press. [Google Scholar]
- Eguren, D.; Contreras-Vidal, J.L. Navigating the FDA Medical Device Regulatory Pathways for Pediatric Lower Limb Exoskeleton Devices. IEEE Syst. J. 2021, 15, 2361–2368. [Google Scholar] [CrossRef]
- Bhardwaj, S.; Khan, A.A.; Muzammil, M. Lower limb rehabilitation robotics: The current understanding and technology. Work 2021, 69, 775–793. [Google Scholar] [CrossRef]
- Pană, C.F.; Popescu, D.; Rădulescu, V.M. Patent Review of Lower Limb Rehabilitation Robotic Systems by Sensors and Actuation Systems Used. Sensors 2023, 23, 6237. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Variable | ROB | STT | ||
|---|---|---|---|---|
| Mean | ±SD or n | Mean | ±SD or n | |
| N (males) | 15 | 11 | 15 | 11 |
| Age, y | 64.8 | 5.89 | 64.7 | 7.16 |
| Height, m | 1.76 | 0.06 | 1.75 | 0.07 |
| Mass, kg | 80.7 | 11.93 | 82.0 | 9.23 |
| BMI, kg·m−2 | 25.9 | 3.26 | 26.8 | 3.15 |
| Days after stroke | 5 | 0.00 | 5 | 0.00 |
| Stroke location, n | ||||
| Left hemisphere | 11 | 10 | ||
| Right hemisphere | 3 | 3 | ||
| Cerebellum | 1 | 2 | ||
| Smoking, n | ||||
| Yes | 11 | 9 | ||
| No | 4 | 6 | ||
| Alcohol, n | ||||
| Yes | 4 | 4 | ||
| No | 11 | 11 | ||
| Comorbidities, n | ||||
| Atherosclerosis | 0 | 1 | ||
| Diabetes | 2 | 2 | ||
| Fibrillation | 1 | 0 | ||
| Gastroenteritis | 1 | 0 | ||
| Hyperchol. | 1 | 0 | ||
| Hypertension | 2 | 7 | ||
| Ischemic HD | 3 | 2 | ||
| Rheumatoid a. | 1 | 2 | ||
| Pre | Post | Follow-Up | |||||
|---|---|---|---|---|---|---|---|
| Variable | Group | Mean | ±SD | Mean | ±SD | Mean | ±SD |
| Primary outcome | |||||||
| MRS (Md, IQR) | ROB | 4.0 | 1.00 | 2.0 | 0.00 | 1.0 | 1.00 |
| STT | 3.0 | 1.00 | 2.0 | 1.00 | 2.0 | 0.00 | |
| Secondary outcomes | |||||||
| Barthel Index (Md, IQR) | ROB | 60.0 | 0.00 | 80.0 | 7.50 | 80.0 | 5.00 |
| STT | 60.0 | 7.50 | 70.0 | 10.00 | 75.0 | 10.00 | |
| Berg Balance Scale | ROB | 19.9 | 2.43 | 27.1 | 3.70 | 28.5 | 3.40 |
| STT | 20.8 | 3.14 | 23.5 | 2.88 | 24.3 | 2.63 | |
| 10 m walk, m/s | ROB | 1.05 | 0.13 | 1.61 | 0.28 | 1.51 | 0.24 |
| STT | 1.06 | 0.12 | 1.34 | 0.23 | 1.40 | 0.14 | |
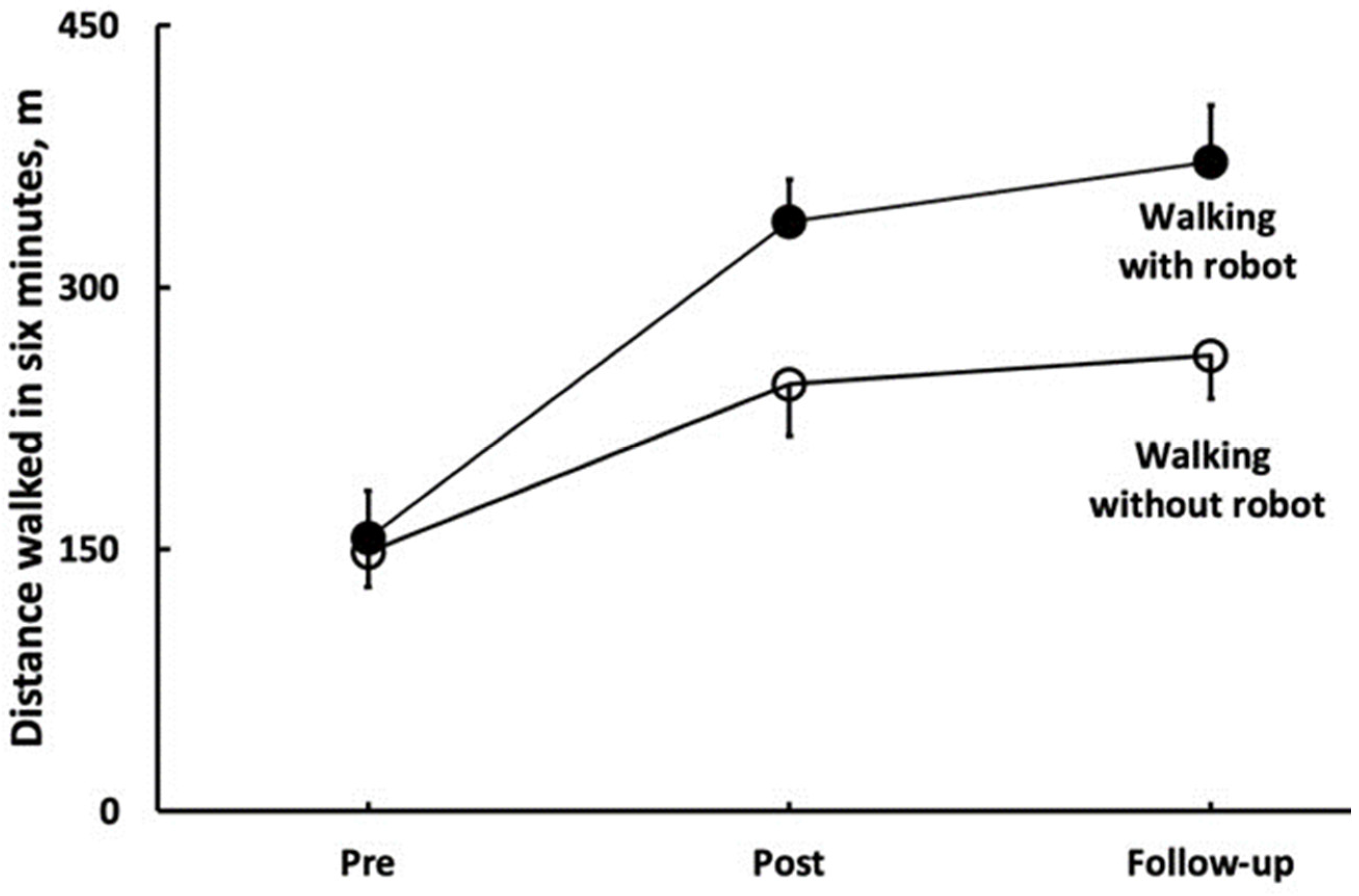
| 6 MWT, m | ROB | 148.0 | 19.71 | 244.3 | 29.57 | 260.7 | 24.63 |
| STT | 154.0 | 24.14 | 185.7 | 22.75 | 190.0 | 11.95 | |
| 6 MWT with robot, m | ROB | 156.3 | 26.81 | 337.3 | 24.32 | 372.0 | 32.11 |
| STT | - | - | - | - | - | - | |
| WEO, cm | ROB | 10.07 | 4.41 | 6.2 | 3.69 | 4.8 | 2.43 |
| STT | 10.2 | 3.84 | 7.6 | 3.27 | 6.0 | 1.89 | |
| WEC, cm | ROB | 12.4 | 3.63 | 8.4 | 3.74 | 7.7 | 2.41 |
| STT | 12.5 | 4.46 | 10.5 | 5.07 | 10.3 | 3.32 | |
| NEO, cm | ROB | 11.1 | 5.58 | 9.0 | 5.46 | 7.7 | 3.73 |
| STT | 11.8 | 3.13 | 10.2 | 4.09 | 10.3 | 4.40 | |
| NEC, cm | ROB | 13.0 | 3.43 | 11.5 | 6.21 | 10.2 | 3.86 |
| STT | 13.3 | 4.77 | 10.7 | 3.60 | 11.5 | 6.22 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kóra, S.; Bíró, A.; Prontvai, N.; Androsics, M.; Drotár, I.; Prukner, P.; Haidegger, T.; Széphelyi, K.; Tollár, J. Investigation of the Effectiveness of the Robotic ReStore Soft Exoskeleton in the Development of Early Mobilization, Walking, and Coordination of Stroke Patients: A Randomized Clinical Trial. Robotics 2024, 13, 44. https://doi.org/10.3390/robotics13030044
Kóra S, Bíró A, Prontvai N, Androsics M, Drotár I, Prukner P, Haidegger T, Széphelyi K, Tollár J. Investigation of the Effectiveness of the Robotic ReStore Soft Exoskeleton in the Development of Early Mobilization, Walking, and Coordination of Stroke Patients: A Randomized Clinical Trial. Robotics. 2024; 13(3):44. https://doi.org/10.3390/robotics13030044
Chicago/Turabian StyleKóra, Szilvia, Adrienn Bíró, Nándor Prontvai, Mónika Androsics, István Drotár, Péter Prukner, Tamás Haidegger, Klaudia Széphelyi, and József Tollár. 2024. "Investigation of the Effectiveness of the Robotic ReStore Soft Exoskeleton in the Development of Early Mobilization, Walking, and Coordination of Stroke Patients: A Randomized Clinical Trial" Robotics 13, no. 3: 44. https://doi.org/10.3390/robotics13030044
APA StyleKóra, S., Bíró, A., Prontvai, N., Androsics, M., Drotár, I., Prukner, P., Haidegger, T., Széphelyi, K., & Tollár, J. (2024). Investigation of the Effectiveness of the Robotic ReStore Soft Exoskeleton in the Development of Early Mobilization, Walking, and Coordination of Stroke Patients: A Randomized Clinical Trial. Robotics, 13(3), 44. https://doi.org/10.3390/robotics13030044