
Development of a 4-DoF Active Upper Limb Orthosis




Abstract
:1. Introduction
2. Materials and Methods
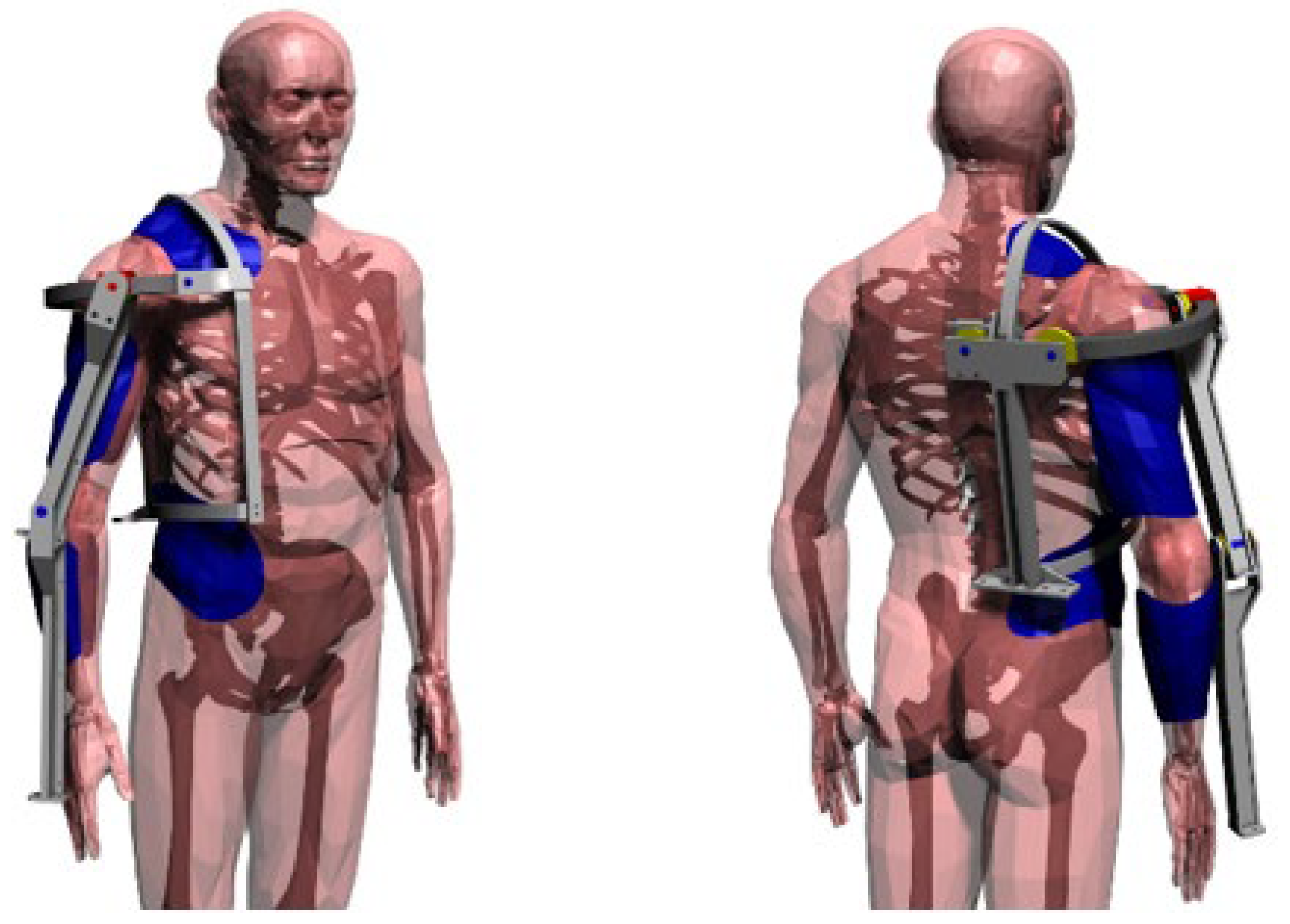
2.1. Mechanical Design of the Orthosis
2.1.1. Technical Specification, Functional Design
- Simple and low-cost design;
- Able to give more power to the movement of the upper arm;
- Sufficient power to move the hand with no aid from the biological muscles;
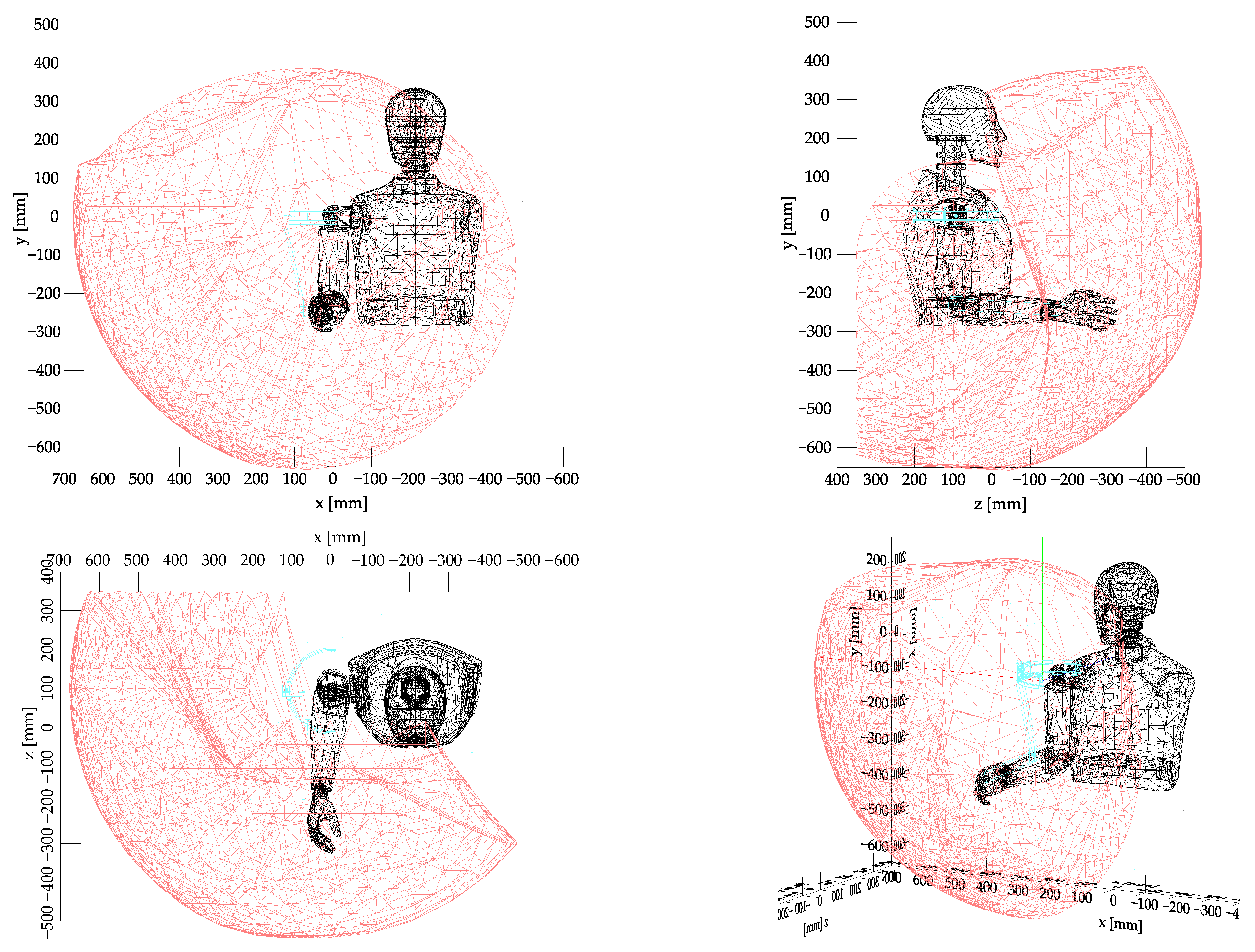
- The working volume for the hand is as large as possible to fit with activities of daily living;
- A payload of 5 N;
- Easy to wear and comfortable;
- Attention is paid to user acceptability.
- Arm length a3: 260 mm;
- Forearm length a4: 340 mm;
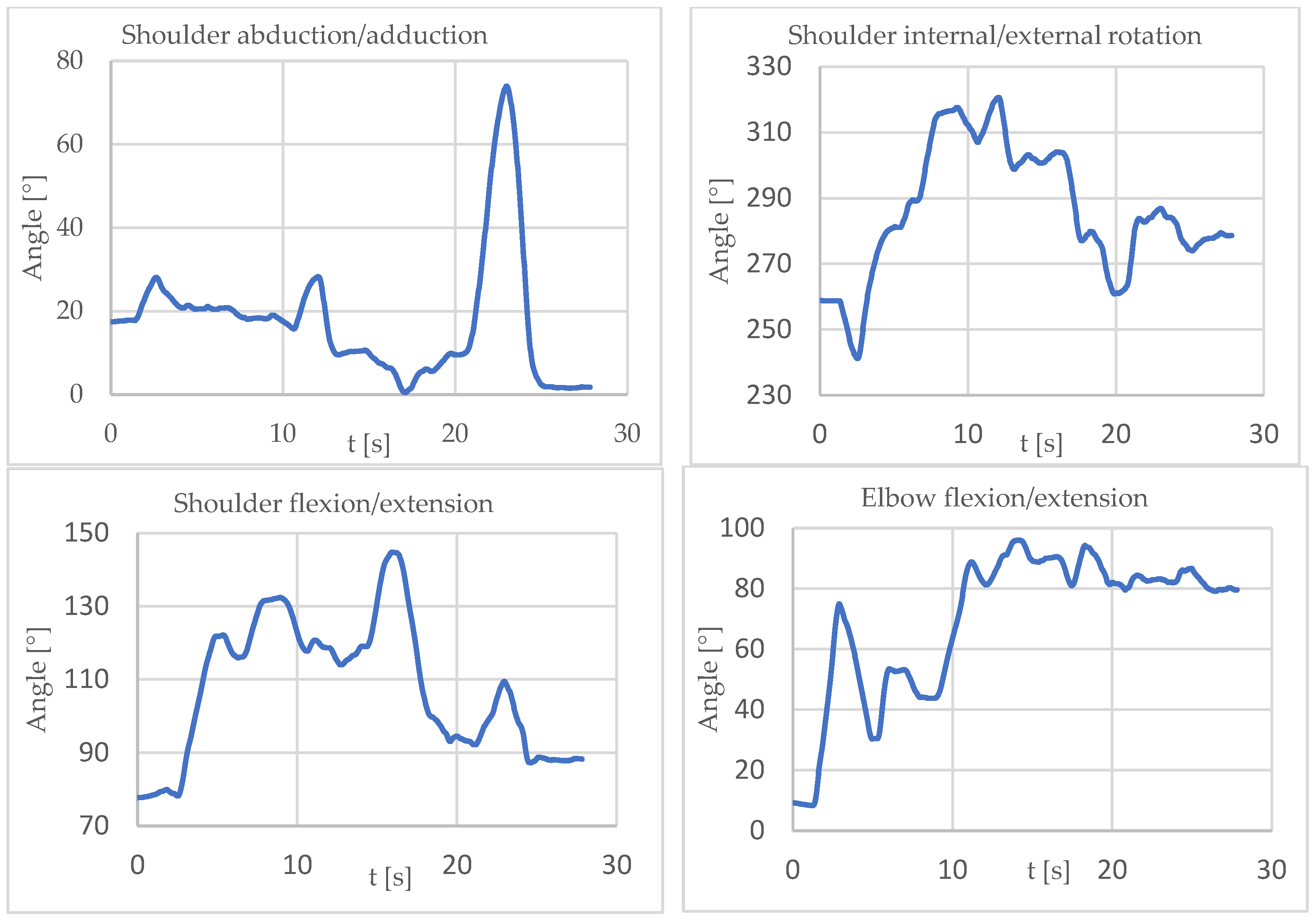
- Shoulder abduction–adduction: 10° < θ1 < 80°
- Shoulder external–internal rotation: 240° < θ2 < 330°
- Shoulder flexion–extension: 70° < θ3 < 150°
- Elbow flexion–extension: 0° < θ4 < 130°
- Force on the end effector, F, 5 N, directed and pointing as gravity force.
2.1.2. Direct Kinematic Model Domain Analysis
2.1.3. Dynamic Model
2.1.4. Actuators, Transmissions
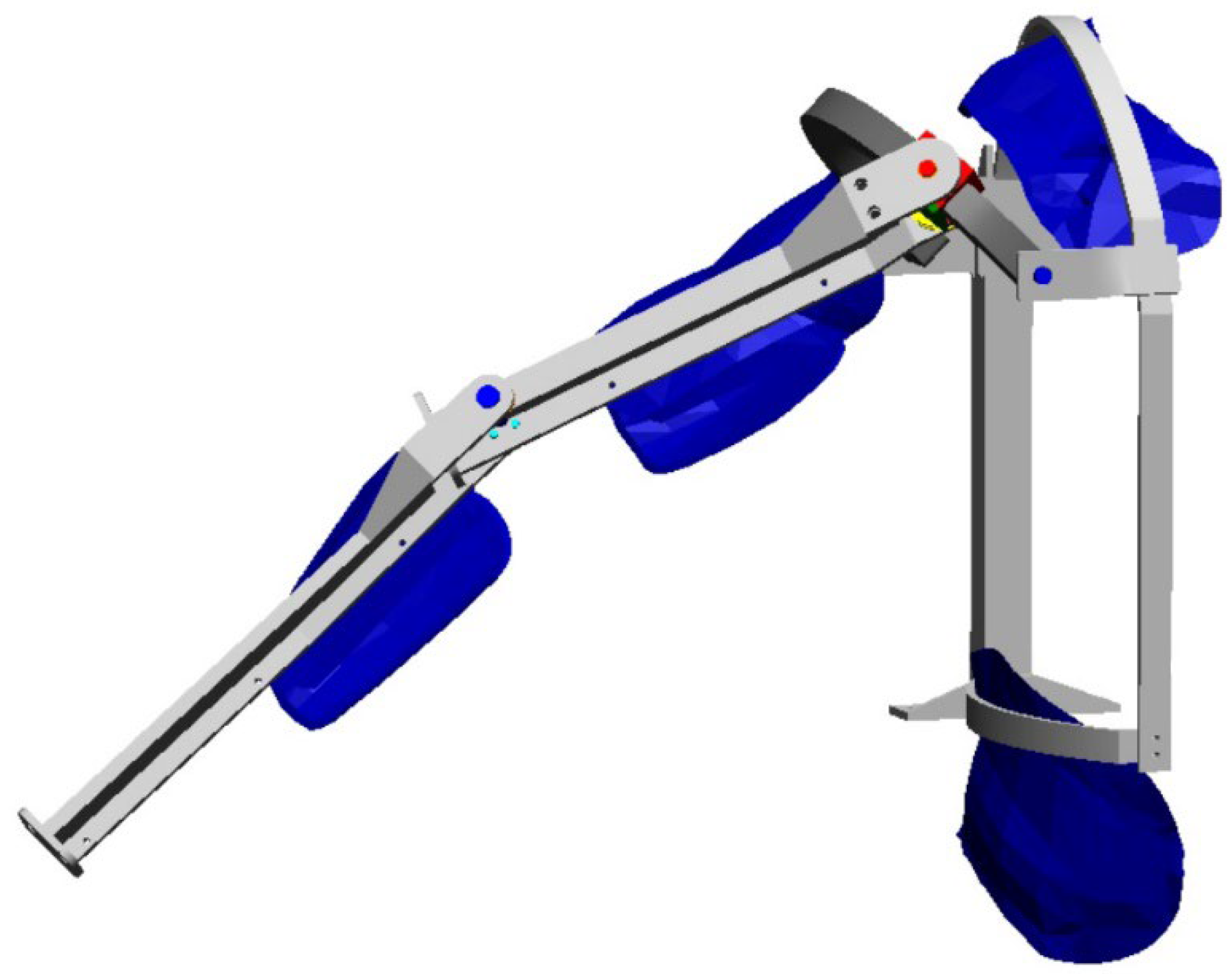
2.1.5. Detailed Design
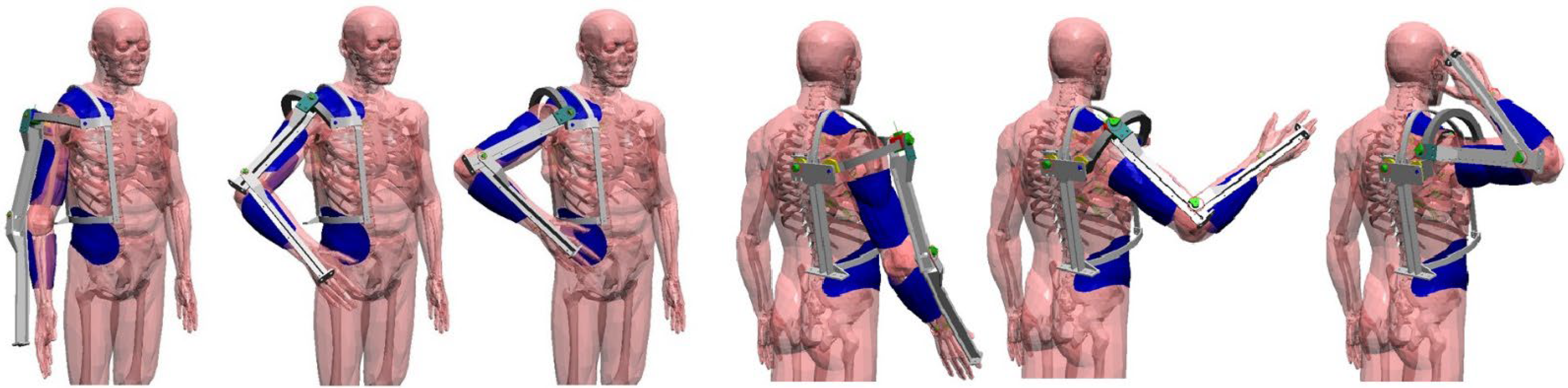
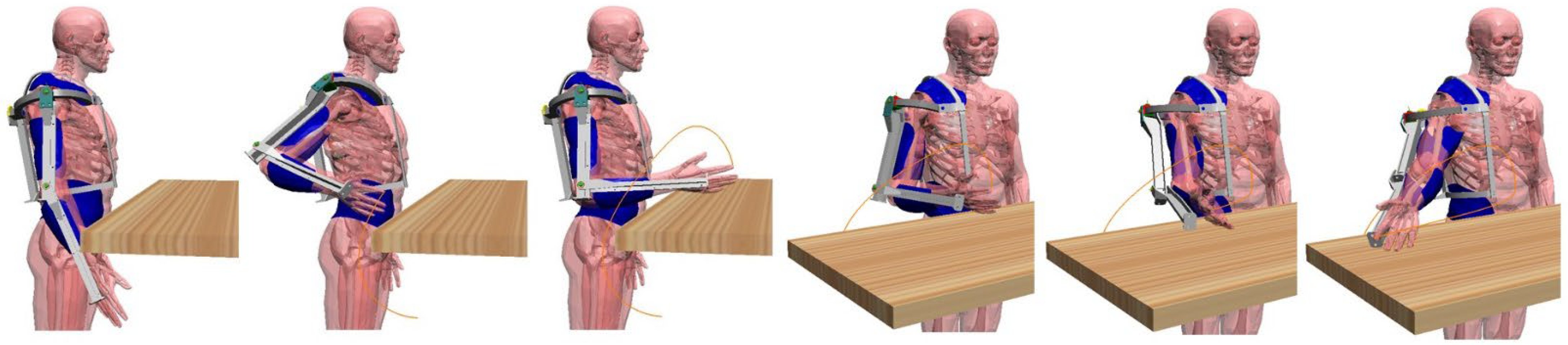
2.1.6. Multibody Model
- Eating, drinking, taking care of yourself (wash your face, comb your hair, brush your teeth, etc.);
- Grasping an object high above your head;
- Touching your shoulder;
- Touching your back;
- Touching the nape of the neck;
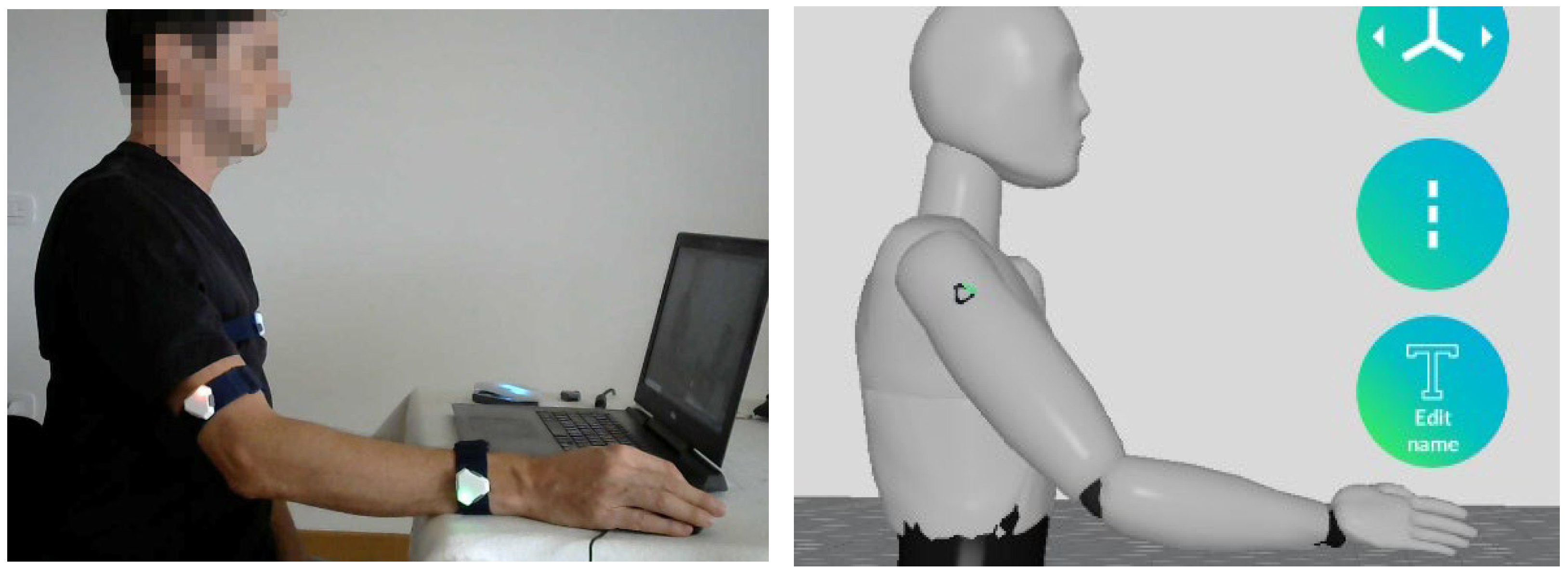
- Reaching the areas of a desk at which you are seated in order to carry out work activities such as reading, writing, and working on the computer.
2.2. Control System
2.2.1. Hardware
2.2.2. Control Strategy
3. Results
3.1. Multibody Model
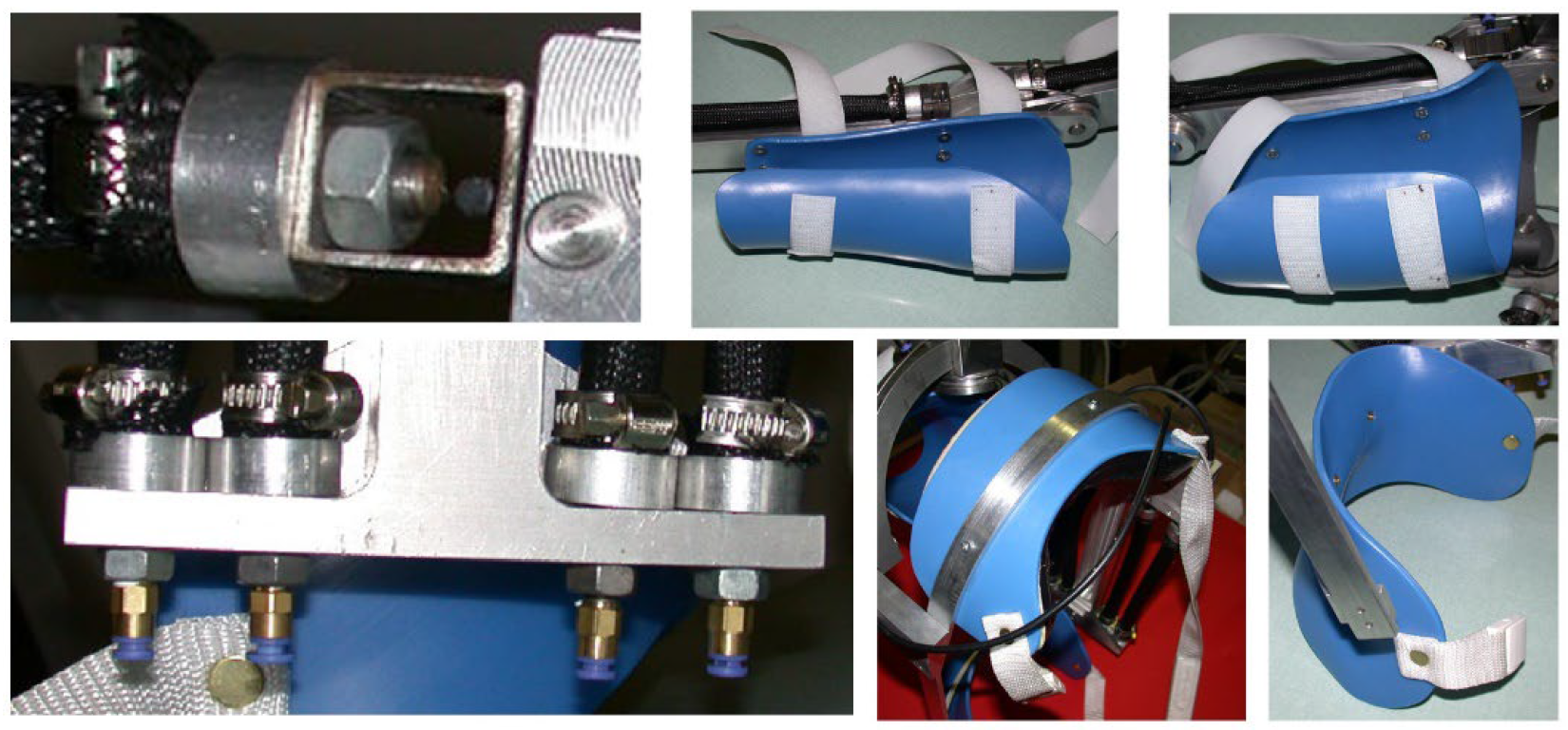
3.2. Orthosis Prototype
3.3. First Experimental Tests
4. Discussion
5. Conclusions and Future Development
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Majidi, C. Soft Robotics: A Perspective—Current Trends and Prospects for the Future. Soft Robot. 2014, 1, 5–11. [Google Scholar] [CrossRef]
- Shiomi, M.; Nakagawa, K.; Shinozawa, K.; Matsumura, R.; Ishiguro, H.; Hagita, N. Does A Robot’s Touch Encourage Human Effort? Int. J. Soc. Robot. 2017, 9, 5–15. [Google Scholar] [CrossRef]
- Antonelli, M.G.; Zobel, P.B.; D’ambrogio, W.; Durante, F. Design methodology for a novel bending pneumatic soft actuator for kinematically mirroring the shape of objects. Actuators 2020, 9, 113. [Google Scholar] [CrossRef]
- Banerjee, H.; Tse, Z.T.H.; Ren, H. Soft robotics with compliance and adaptation for biomedical applications and forthcoming challenges. Int. J. Robot. Autom. 2018, 33, 69–80. [Google Scholar] [CrossRef] [Green Version]
- Shintake, J.; Cacucciolo, V.; Floreano, D.; Shea, H. Soft Robotic Grippers. Adv. Mater. 2018, 30, 1707035. [Google Scholar] [CrossRef] [Green Version]
- Antonelli, M.G.; D’Ambrogio, W.; Durante, F. Development of a pneumatic soft actuator as a hand finger for a collaborative robot. In Proceedings of the ICMSCE International Conference, Amsterdam, The Netherlands, 22–23 February 2018; pp. 67–71. [Google Scholar] [CrossRef]
- Yang, Y.; Chen, Y.; Li, Y.; Chen, M.Z.Q.; Wei, Y. Bioinspired robotic fingers based on pneumatic actuator and 3D printing of smart material. Soft Robot. 2017, 4, 147–162. [Google Scholar] [CrossRef]
- Antonelli, M.G.; Zobel, P.B.; Durante, F.; Raparelli, T. Additive manufacturing applications on flexible actuators for active orthoses and medical devices. J. Healthc. Eng. 2019, 2019, 5659801. [Google Scholar] [CrossRef] [Green Version]
- Ellis, M.D.; Sukal, T.; DeMott, T.; Dewald, J.P.A. ACT 3D Exercise targets gravity-induced discoordination and improves reaching work area in individuals with stroke. In Proceedings of the IEEE 10th International Conference on Rehabilitation Robotics ICORR. Noordwijk, The Netherlands, 13–15 June 2007; pp. 890–895. [Google Scholar]
- Ju, M.S.; Lin, C.C.K.; Lin, D.H.; Hwang, I.S.; Chen, S.M. A rehabilitation robot with force-position hybrid fuzzy controller: Hybrid fuzzy control of rehabilitation robot. Ieee Trans. Neural Syst. Rehabil. Eng. 2005, 13, 349–358. [Google Scholar] [CrossRef]
- Micera, S.; Carrozza, M.; Guglielmelli, E.; Cappiello, G.; Zaccone, F.; Freschi, C.; Colombo, R.; Mazzone, A.; Delconte, C.; Pisano, F.; et al. A simple robotic system for neurorehabilitation. Auton. Robot. 2005, 19, 271–284. [Google Scholar] [CrossRef]
- Sulzer, J.S.; Peshkin, M.A.; Patton, J.L. Design of a Mobile, Inexpensive Device for Upper Extremity Rehabilitation at Home. In Proceedings of the IEEE 10th International Conference on Rehabilitation Robotics (ICORR). Noordwijk, The Netherlands, 13–15 June 2007; pp. 933–937. [Google Scholar]
- Hesse, S.; Schulte-Tigges, G.; Konrad, M.; Bardeleben, A.; Werner, C. Robot-assisted arm trainer for the passive and active practice of bilateral forearm and wrist movements in hemiparetic subjects. Arch. Phys. Med. Rehabil. 2003, 84, 915–920. [Google Scholar] [CrossRef]
- Palsbo, S.E.; Hood-Szivek, P. Effect of robotic-assisted three-dimensional repetitive motion to improve handmotor function and control in children with handwriting deficits: A nonrandomized phase 2 device trial. Am. J. Occup. 2012, 66, 682–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, M.; Wisneski, K.; Anderson, J.; Nathan, D.; Smith, R. Development of ADLER: The activities of daily living exercise robot. In Proceedings of the 1st IEEE/RAS-EMBS International Conference on Biomedical Robotics and Biomechatronics, BioRobotics, Pisa, Italy, 20–22 February 2006; pp. 881–886. [Google Scholar]
- Fluet, G.G.; Qiu, Q.; Saleh, S.; Ramirez, D.; Adamovich, S.; Kelly, D.; Parikh, H. Robot-assisted virtual rehabilitation (NJIT-RAVR) system for children with upper extremity hemiplegia. In Proceedings of the Virtual Rehabilitation International Conference. Haifa, Israel, 29 June–2 July 2009; pp. 189–192. [Google Scholar]
- Rosati, G.; Zanotto, D.; Secoli, R.; Rossi, A. Design and control of two planar cable-driven robots for upper-limb neurorehabilitation. In Proceedings of the IEEE International Conference on Rehabilitation Robotics ICORR. Kyoto, Japan, 23–26 June 2009; pp. 560–565. [Google Scholar]
- Kiguchi, K.; Esaki, R.; Tsuruta, T.; Watanabe, K.; Fukuda, T. An exoskeleton system for elbow joint motion rehabilitation. In Proceedings of the IEEE/ASME International Conference on Advanced IntelligentMechatronics (AIM). Volume 2, Port Island, Japan, 20–24 July 2003; pp. 1228–1233. [Google Scholar]
- Rosen, J.; Brand, M.; Fuchs, M.B.; Arcan, M. A myosignal-based powered exoskeleton system. Ieee Trans. Syst. Man Cybern. Part A Syst. Hum. 2001, 31, 210–222. [Google Scholar] [CrossRef] [Green Version]
- Durante, F.; Zobel, P.B.; Raparelli, T. Development of an active orthosis for inferior limb with light structure. Mechanisms and Machine Science. In Proceedings of the International Conference on Robotics in Alpe-Adria Danube Region, Torino, Italy, 21–22 June 2017; pp. 833–841. [Google Scholar] [CrossRef]
- Ertas, I.H.; Hocaoglu, E.; Barkana, D.E.; Patoglu, V. Finger exoskeleton for treatment of tendon injuries. In Proceedings of the IEEE International Conference on Rehabilitation Robotics (ICORR). Kyoto, Japan, 23–26 June 2009; pp. 194–201. [Google Scholar]
- Sacco, K.; Belforte, G.; Eula, G.; Raparelli, T.; Sirolli, S.; Geda, E.; Geminiani, G.C.; Virgilio, R.; Zettin, M.P.I.G.R.O. An active exoskeleton for robotic neurorehabilitation training driven by an electro-pneumatic control. Mech. Mach. Sci. 2018, 49, 845–853. [Google Scholar] [CrossRef]
- Sarakoglou, I.; Tsagarakis, N.G.; Caldwell, D.G. Occupational and physical therapy using a hand exoskeleton based exerciser. In Proceedings of the IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS), Sendai, Japan, 28 September–2 October 2004; pp. 2973–2978. [Google Scholar]
- Pignolo, L.; Dolce, G.; Basta, G.; Lucca, L.F.; Serra, S.; Sannita, W.G. Upper limb rehabilitation after stroke: ARAMIS a “robo-mechatronic” innovative approach and prototype. In Proceedings of the 4th IEEE RAS & EMBS International Conference in Biomedical Robotics and Biomechatronics (BioRob), Rome, Italy, 24–27 June 2012; pp. 1410–1414. [Google Scholar]
- Kawasaki, H.; Ito, S.; Ishigure, Y.; Nishimoto, Y.; Aoki, T.; Mouri, T.; Sakaeda, H.; Abe, M. Development of a Hand Motion Assist Robot for Rehabilitation Therapy by Patient Self-Motion Control. In Proceedings of the IEEE 10th International Conference on Rehabilitation Robotics (ICORR). Noordwijk, Netherlands, 13–15 June 2007; pp. 234–240. [Google Scholar]
- Li, Q.; Wang, D.; Du, Z.; Song, Y.; Sun, L. sEMG Based Control for 5 DOF Upper Limb Rehabilitation Robot System. In Proceedings of the IEEE International Conference on Robotics and Biomimetics (ROBIO), Kunming, China, 17–20 December 2006; pp. 1305–1310. [Google Scholar]
- Mayr, A.; Kofler, M.; Saltuari, L. ARMOR: An electromechanical robot for upper limb training following stroke. A prospective randomised controlled pilot study. Handchir Mikrochir Plast Chir. 2008, 40, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Gaponov, I.; Popov, D.; Lee, S.J.; Ryu, J.H. Auxilio: A portable cable-driven exosuit for upper extremity assistance. International J. Control Autom. Syst. 2017, 15, 73–84. [Google Scholar] [CrossRef]
- Cheng, H.S.; Ju, M.S.; Lin, C.C.K. Improving elbow torque output of stroke patients with assistive torque controlled by EMG signals. J. Biomech. Eng. 2003, 125, 881–886. [Google Scholar] [CrossRef]
- Vanderniepen, I.; Van Ham, R.; Van Damme, M.; Versluys, R.; Lefeber, D. Orthopaedic rehabilitation: A powered elbow orthosis using compliant actuation. In Proceedings of the IEEE International Conference on Rehabilitation Robotics (ICORR). Kyoto, Japan, 23–26 June 2009; pp. 172–177. [Google Scholar]
- Song, R.; Tong, K.Y.; Hu, X.L.; Zheng, X.J. Myoelectrically Controlled Robotic System That Provide Voluntary Mechanical Help for Persons after Stroke. In Proceedings of the IEEE 10th International Conference on Rehabilitation Robotics (ICORR), Noordwijk, The Netherlands, 13–15 June 2007; pp. 246–249. [Google Scholar]
- Turner, M.; Gomez, D.; Tremblay, M.; Cutkosky, M. Preliminary tests of an arm-grounded haptic feedback device in telemanipulation. In Proceedings of the the ASME Dynamic Systems and Control Division. Volume 64, Anaheim, CA, USA, 15-20 November 1998; pp. 145–149. [Google Scholar]
- Mali, U.; Munih, M. HIFE-haptic interface for finger exercise. Mechatron. Ieee/Asme Trans. 2006, 11, 93–102. [Google Scholar] [CrossRef]
- Hesse, S.; Kuhlmann, H.; Wilk, J.; Tomelleri, C.; Kirker, S.G.B. A new electromechanical trainer for sensorimotor rehabilitation of paralysed fingers: A case series in chronic and acute stroke patients. J. Neuroeng. Rehabil. 2008, 5, 21. [Google Scholar] [CrossRef]
- Rotella, M.F.; Reuther, K.E.; Hofmann, C.L.; Hage, E.B.; BuSha, B.F. An Orthotic Hand-Assistive Exoskeleton for Actuated Pinch and Grasp. In Proceedings of the Bioengineering Conference, IEEE 35th Annual Northeast, Boston, MA, USA, 3–5 April 2009; pp. 1–2. [Google Scholar]
- Wege, A.; Hommel, G. Development and control of a hand exoskeleton for rehabilitation of hand injuries. In Proceedings of the International Conference on Intelligent Robots and Systems (IROS 2005), Edmonton, Canada, 2–6 August 2005; pp. 3046–3051. [Google Scholar]
- Burgar, C.G.; Lum, P.S.; Shor, P.C.; Van der Loos, H.F.M. Development of robots for rehabilitation therapy: The Palo Alto VA/Stanford experience. J. Rehabil. Res. Dev. 2000, 37, 663–673. [Google Scholar]
- Amirabdollahian, F.; Loureiro, R.; Gradwell, E.; Collin, C.; Harwin, W.; Johnson, G. Multivariate analysis of the Fugl-Meyer outcome measures assessing the effectiveness of GENTLE/S robot-mediated stroke therapy. J. Neuroeng. Rehabil. 2007, 4, 4. [Google Scholar] [CrossRef]
- Perry, J.C.; Rosen, J.; Burns, S. Upper-limb powered exoskeleton design. Ieee/Asme Trans. Mechatron. 2007, 12, 408–417. [Google Scholar] [CrossRef]
- Mihelj, M.; Podobnik, J.; Munih, M. HEnRiE-Haptic environment for reaching and grasping exercise. In Proceedings of the 2nd IEEE RAS & EMBS International Conference on Biomedical Robotics and Biomechatronics (BioRob), Scottsdale, AZ, USA, 19–22 October 2008; pp. 907–912.
- Sasaki, D.; Noritsugu, T.; Takaiwa, M. Development of Active Support Splint driven by Pneumatic Soft Actuator (ASSIST). In Proceedings of the IEEE International Conference on Robotics and Automation (ICRA), Barcelona, Spain, 18–22 April 2005; pp. 520–525. [Google Scholar]
- Kline, T.; Kamper, D.; Schmit, B. Control system for pneumatically controlled glove to assist in grasp activities. In Proceedings of the 9th International Conference on Rehabilitation Robotics ICORR, Chicago, IL, USA, 28 June–1 July 2005; pp. 78–81. [Google Scholar]
- Lucas, L.; Di Cicco, M.; Matsuoka, Y. An EMG-controlled hand exoskeleton for natural pinching. J. Robot Mechatron. 2004, 16, 482–488. [Google Scholar] [CrossRef] [Green Version]
- Bouzit, M.; Burdea, G.; Popescu, G.; Boian, R. The Rutgers Master II-new design force-feedback glove. IEEE/ASME Trans. Mechatron. 2002, 7, 256–263. [Google Scholar] [CrossRef] [Green Version]
- Klein, J.; Spencer, S.; Allington, J.; Bobrow, J.E.; Reinkensmeyer, D.J. Optimization of a parallel shouldermechanism to achieve a high-force, low-mass, robotic-arm exoskeleton. Ieee Trans. Robot. 2010, 26, 710–715. [Google Scholar] [CrossRef]
- Takahashi, C.D.; Der-Yeghiaian, L.; Le, V.; Motiwala, R.R.; Cramer, S.C. Robot-based handmotor therapy after stroke. Brain 2008, 131, 425–437. [Google Scholar] [CrossRef]
- Pylatiuk, C.; Kargov, A.; Gaiser, I.; Werner, T.; Schulz, S.; Bretthauer, G. Design of a flexible fluidic actuation system for a hybrid elbow orthosis. In Proceedings of the IEEE International Conference on Rehabilitation Robotics (ICORR), Kyoto, Japan, 23–26 June 2009; pp. 167–171. [Google Scholar]
- Stienen, A.; Hekman, E.; Prange, G.; Jannink, M.; Aalsma, A.; van der Helm, F.; van der Kooij, H. Dampace: Design of an exoskeleton for force-coordination training in upper-extremity rehabilitation. J. Med Devices 2009, 3, 10. [Google Scholar] [CrossRef]
- Stienen, A.H.A.; Hekman, E.E.G.; ter Braak, H.; Aalsma, A.M.M.; van der Helm, F.C.T.; van der Kooij, H. Design of a rotational hydro-elastic actuator for an active upper-extremity rehabilitation exoskeleton. In Proceedings of the 2nd IEEE RAS & EMBS International Conference on Biomedical Robotics and Biomechatronics (BioRob), Scottsdale, AZ, USA, 19–22 October 2008; pp. 881–888. [Google Scholar]
- Umemura, A.; Saito, Y.; Fujisaki, K. A study on power-assisted rehabilitation robot arms operated by patient with upper limb disabilities. In Proceedings of the IEEE International Conference on Rehabilitation Robotics (ICORR), Kyoto, Japan, 23–26 June 2009; pp. 451–456. [Google Scholar]
- Winter, S.H.; Bouzit, M. Use of Magnetorheological fluid in a force feedback glove. Ieee Trans. Neural Syst. Rehabil. Eng. 2007, 15, 2–8. [Google Scholar] [CrossRef]
- Oda, K.; Isozumi, S.; Ohyama, Y.; Tamida, K.; Kikuchi, T.; Furusho, J. Development of isokinetic and iso-contractile exercisemachine MEM-MRB using MR brake. In Proceedings of the IEEE International Conference on Rehabilitation Robotics (ICORR), Kyoto, Japan, 23–26 June 2009; pp. 6–11. [Google Scholar]
- Khanicheh, A.; Mintzopoulos, D.; Weinberg, B.; Tzika, A.A.; Mavroidis, C. MR_CHIROD v.2: Magnetic resonance compatible smart hand rehabilitation device for brain imaging. Ieee Trans. Neural Syst. Rehabil. Eng. 2008, 16, 91–98. [Google Scholar] [CrossRef]
- Pedrocchi, A.; Ferrante, S.; Ambrosini, E.; Gandolla, M.; Casellato, C.; Schauer, T.; Klauer, C.; Pascual, J.; Vidaurre, C.; Gfoehler, M.; et al. MUNDUS project: MUltimodal Neuroprosthesis for daily upper limb support. J. Neuroeng. Rehabil. 2013, 10, 66. [Google Scholar] [CrossRef]
- Nathan, D.E.; Johnson, M.J.; McGuire, J. Feasibility of integrating FES grasp assistance with a task-oriented robot-assisted therapy environment: A case study. In Proceedings of the 2nd IEEE RAS & EMBS International Conference on Biomedical Robotics and Biomechatronics (BioRob), Scottsdale, AZ, USA, 19–22 October 2008; pp. 807–812. [Google Scholar]
- Kobayashi, H.; Nozaki, H. Development ofmuscle suit for supporting manual worker. In Proceedings of the IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS), San Diego, CA, USA, 29 October–2 November 2007; pp. 1769–1774. [Google Scholar]
- Xing, K.; Xu, Q.; He, J.; Wang, Y.; Liu, Z.; Huang, X. A wearable device for repetitive hand therapy. In Proceedings of the 2nd IEEE RAS & EMBS International Conference on Biomedical Robotics and Biomechatronics BioRob, Scottsdale, AZ, USA, 19–22 October 2008; pp. 919–923. [Google Scholar]
- Raparelli, T.; Zobel, P.B.; Durante, F.; Antonelli, M.; Raimondi, P.; Costanzo, G. First clinical investigation on a pneumatic lumbar unloading orthosis. In Proceedings of the IEEE/ICME International Conference on Complex Medical Engineering, CME, Beijing, China, 23–27 May 2007; Volume 4381959, pp. 1327–1330. [Google Scholar] [CrossRef]
- Gabrio Antonelli, M.; Beomonte Zobel, P.; Durante, F.; Raparelli, T. Development and pre-clinical investigation of a massage device for the low back. Int. J. Mech. Eng. Technol. 2018, 9, 742–754. [Google Scholar]
- Koeneman, E.J.; Schultz, R.S.; Wolf, S.L.; Herring, D.E.; Koeneman, J.B. A pneumatic muscle hand therapy device. Proc. Ieee Enginnering Med. Biol. Soc. 2004, 4, 2711–2713. [Google Scholar] [CrossRef]
- Balasubramanian, S.; Wei, R.; Perez, M.; Shepard, B.; Koeneman, E.; Koeneman, J.; He, J. RUPERT: An exoskeleton robot for assisting rehabilitation of arm functions. In Proceeding of International Conference on Virtual Rehabilitation, Vancouver, Canada, 25–27 August 2008; pp. 163–167. [Google Scholar]
- Tsagarakis, N.; Caldwell, D. Development and control of a "soft-actuated" exoskeleton for use in physiotherapy and training. J. Auton. Robot. 2003, 15, 21–33. [Google Scholar] [CrossRef]
- Durante, F.; Antonelli, M.G.; Beomonte Zobel, P. Development of an active exoskeleton for assisting back movements in lifting weights. Int. J. Mech. Eng. Robot. Res. 2018, 7, 353–360. [Google Scholar] [CrossRef] [Green Version]
- Chou, C.-P.; Hannaford, B. Measurement and modeling of McKibben pneumatic artificial muscles. Ieee Trans. Robot. Autom. 1996, 12, 90–102. [Google Scholar] [CrossRef] [Green Version]
- Antonelli, M.G.; Zobel, P.B.; D’Ambrogio, W.; Durante, F.; Raparelli, T. An analytical formula for designing McKibben pneumatic muscles. Int. J. Mech. Eng. Technol. 2018, 9, 320–337. [Google Scholar]
- Sorge, F.; Cammalleri, M. A theoretical approach to pneumatic muscle mechanics. In Proceedings of the IEEE/ASME International Conference on Advanced Intelligent Mechatronics: Mechatronics for Human Wellbeing. AIM, Wollongong, NSW, Australia, 9–12 July 2013; Volume 6584228, pp. 1021–1026. [Google Scholar] [CrossRef]
- Antonelli, M.G.; Beomonte Zobel, P.; Durante, F.; Raparelli, T. Numerical modelling and experimental validation of a McKibben pneumatic muscle actuator. J. Intell. Mater. Syst. Struct. 2017, 28, 2737–2748. [Google Scholar] [CrossRef]
- Tondu, B.; Lopez, P. Modeling and Control of McKibben Artificial Muscle Robot Actuators. Ieee Control Syst. 2000, 20, 15–38. [Google Scholar] [CrossRef]
- Antonelli, M.G.; Beomonte Zobel, P.; Durante, F.; Gaj, F. Development and testing of a grasper for NOTES powered by variable stiffness pneumatic actuation. Int. J. Med Robot. Comput. Assist. Surg. 2017, 13, e1796. [Google Scholar] [CrossRef]
- Kiguchi, K.; Iwami, K.; Yasuda, M.; Watanabe, K.; Fukuda, T. An exoskeletal robot for human shoulder joint motion assist. Ieee/Asme Trans. Mechatron. 2003, 8, 125–135. [Google Scholar] [CrossRef]
- Cozens, J.A. Robotic assistance of an active upper limb exercise in neurologically impaired patients. Iiie Trans. Reha-Bilitation Eng. 1999, 7, 254–256. [Google Scholar] [CrossRef]
- Mavroidis, C.; Nikitczuk, J.; Weinberg, B.; Danaher, G.; Jensen, K.; Pelletier, P.; Prugnarola, J.; Stuart, R.; Arango, R.; Leahey, M.; et al. Smart portable rehabilitation devices. J. Neuroenginnering Rehabil. 2005, 2, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stein, J.; Narendran, K.; McBean, J.; Krebs, K.; Hughes, R. Electromyography-controlled exoskeletal upper-limb-powered orthosis for exercise training after stroke. Am. J. Phys. Med. Rehabil. 2007, 86, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Kung, P.C.; Ju, M.S.; Lin, C.C.K. Design of a forearm rehabilitation robot. In Proceedings of the IEEE 10th International Conference on Rehabilitation Robotics ICORR, Noordwijk, The Netherlands, 12–15 June 2007; pp. 228–233. [Google Scholar]
- Loureiro, R.C.V.; Belda-Lois, J.M.; Lima, E.R.; Pons, J.L.; Sanchez-Lacuesta, J.J.; Harwin, W.S. Upper limb tremor suppression in ADL via an orthosis incorporating a controllable double viscous beam actuator. In Proceedings of the 9th International Conference on Rehabilitation Robotics ICORR, Chicago, IL, USA, 28 June–1 July 2005; pp. 119–122. [Google Scholar]
- Colombo, R.; Pisano, F.; Mazzone, A.; Delconte, C.; Micera, S.; Carrozza, M.C.; Dario, P.; Minuco, G. Design strategies to improve patientmotivation during robot-aided rehabilitation. J. Neuroeng. Rehabil. 2007, 4, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dovat, L.; Lambercy, O.; Gassert, R.; Maeder, T.; Milner, T.; Leong, T.C.; Burdet, E. HandCARE: A cable-actuated rehabilitation system to train hand function after stroke. Ieee Trans. Neural Syst. Rehabil. Eng. 2008, 16, 582–591. [Google Scholar] [CrossRef]
- Schabowsky, C.N.; Godfrey, S.B.; Holley, R.J.; Lum, P.S. Development and pilot testing of HEXORR. hand EXOskeleton rehabilitation robot. J. Neuroeng. Rehabil. 2010, 7, 36. [Google Scholar] [CrossRef] [Green Version]
- Ho, N.S.K.; Tong, K.Y.; Hu, X.L.; Fung, K.L.; Wei, X.J.; Rong, W.; Susanto, E.A. An EMG-driven exoskeleton hand robotic training device on chronic stroke subjects: Task training system for stroke rehabilitation. Proceedings of IEEE International Conference on Rehabilitation Robot, Boston, MA, USA, 29 June–1 July 2011. [Google Scholar] [CrossRef]
- Ögce, F.; Özyalçin, H. Case study: A myoelectrically controlled shoulder-elbow orthosis for unrecovered brachial plexus injury. Prosthet. Orthosis Int. 2000, 24, 252–255. [Google Scholar] [CrossRef]
- Lum, P.; Reinkensmeyer, D.; Mahoney, R.; Rymer, W.Z.; Burgar, C. Robotic devices formovement therapy after stroke: Current status and challenges to clinical acceptance. Top. Stroke Rehabil. 2002, 8, 40–53. [Google Scholar] [CrossRef] [Green Version]
- Gupta, A.; O’Malley, M.; Patoglu, V.; Burgar, C. Design, control and performance of RiceWrist: A force feedback wrist exoskeleton for rehabilitation and training. Int. J. Robot. Res. 2008, 27, 233. [Google Scholar] [CrossRef]
- Gopura, R.A.R.; Kiguchi, K. A human forearm and wristmotion assist exoskeleton robot with EMG-based Fuzzy-neuro control. In Proceedings of the 2nd IEEE RAS & EMBS International Conference on Biomedical Robotics and Biomechatronics (BioRob), Scottsdale, AZ, USA, 19–22 October 2008; pp. 550–555. [Google Scholar]
- Cordo, P.; Lutsep, H.; Cordo, L.; Wright, W.G.; Cacciatore, T.; Skoss, R. Assisted movement with enhanced sensation (AMES): Coupling motor and sensory to remediatemotor deficits in chronic stroke patients. Neurorehabilit. Neural Repair 2009, 23, 67–77. [Google Scholar] [CrossRef] [Green Version]
- Kiguchi, K.; Kose, Y.; Hayashi, Y. Task-oriented perception-assist for an upper-limb powerassist exoskeleton robot. In Proceedings of the World Automation Congress (WAC), Kobe, Japan, 19–23 September 2010; pp. 1–6. [Google Scholar]
- Gupta, A.; O’Malley, M. Design of a haptic arm exoskeleton for training and rehabilitation. Ieee Asme Trans. Mechatron. 2006, 11, 280. [Google Scholar] [CrossRef]
- Lambercy, O.; Dovat, L.; Gassert, R.; Burdet, E.; Teo, C.L.; Milner, T. A haptic knob for rehabilitation of hand function. Ieee Trans. Neural Syst. Rehabil. Eng. 2007, 15, 356–366. [Google Scholar] [CrossRef] [PubMed]
- Loureiro, R.C.V.; Harwin, W.S. Reach & Grasp Therapy: Design and Control of a 9-DOF Robotic Neuro-rehabilitation System. In Proceedings of the IEEE 10th International Conference on Rehabilitation Robotics (ICORR), Noordwijk, The Netherlands, 13–15 June 2007; pp. 757–763. [Google Scholar]
- Koceska, N.; Koceski, S.; Durante, F.; Beomonte Zobel, P.; Raparelli, T. Control architecture of a 10 DOF lower limbs exoskeleton for gait rehabilitation. Int. J. Adv. Robot. Syst. 2013, 10, 68. [Google Scholar] [CrossRef] [Green Version]
- Song, R.; yu Tong, K.; Hu, X. Assistive control system using continuous myoelectric signal in robot-aided arm training for patients after stroke. Ieee Trans. Neural Syst. Rehabil. Eng. 2008, 16, 371–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tong, K.Y.; Ho, S.K.; Pang, P.K.; Hu, X.L.; Tam, W.K.; Fung, K.L.; Wei, X.J.; Chen, P.N.; Chen, M. An Intention Driven Hand Functions Task Training Robotic System. In Proceedings of the Conference IEEE Engineering in Medicine and Biology Society, Buenos Aires, Argentina, 31 August–4 September 2010; Volume 2010, pp. 3406–3409. [Google Scholar]
- Koceska, N.; Koceski, S.; Zobel, P.B.; Durante, F. Control architecture for a lower limbs rehabilitation robot system. In Proceedings of the 2008 IEEE International Conference on Robotics and Biomimetics, ROBIO, Bangkok, Thailand, 22–25 February 2009; Volume 4913131, pp. 971–976. [Google Scholar] [CrossRef]
- Fleischer, C.; Kondak, K.; Wege, A.; Kossyk, I. Research on Exoskeletons at the TU Berlin. In Proceedings of the German Workshop on Robotics, Braunschweig, Germany, 9–10 June 2009. [Google Scholar]
- Raparelli, T.; Beomonte Zobel, P.; Durante, F.; Raparelli, F. Development of a powered upper limb orthosis. In Proceedings of the 8th International Conference on Rehabilitation Robotics, ICORR, Taejon, Republic of Korea, 23-25 April 2003 (143-146). [Google Scholar]
- Craig, J.J. Introduction to Robotics: Mechanics and Control, 3rd ed.; Pearson Education: London, UK, 2005. [Google Scholar]
- Bourbonnais, F.; Bigras, P.; Bonev, I.A. Minimum-time trajectory planning and control of a pick-and-place five-bar parallel robot. Ieee/Asme Trans. Mechatron. 2014, 20, 740–749. [Google Scholar] [CrossRef]
- Wang, D.; Wu, J.; Wang, L.; Liu, Y. A Postprocessing Strategy of a 3-DOF Parallel Tool Head Based on Velocity Control and Coarse Interpolation. Ieee Trans. Ind. Electron. 2018, 65, 6333–6342. [Google Scholar] [CrossRef]
- Da Forno, R. Dal Corpo Rigido al Robot con Matlab; Mc Graw Hill Italia: Milano, Italy, 1998. [Google Scholar]
- Pheasant, S. Body Space: Anthropometry, Ergonomics and Design; Taylor & Francis: London, UK, 1986. [Google Scholar]
- Anatomylearning. Available online: https://anatomylearning.com/ (accessed on 29 August 2022).
- Durante, F.; Raparelli, T.; Beomonte Zobel, P. Two-Dof Upper Limb Rehabilitation Robot Driven by Straight Fibers Pneumatic Muscles. Bioengineering 2022, 9, 377. [Google Scholar] [CrossRef]
- Vlachos, E.; Jochum, E.; Demers, L.P. HEAT: The harmony exoskeleton self-assessment test. In Proceedings of the 2018 27th IEEE International Symposium on Robot and Human Interactive Communication (RO-MAN), Nanjing, China, 27–31 August 2018; pp. 577–582. [Google Scholar]
- Bai, S.; Christensen, S.; Islam, M.R.U. An upper-body exoskeleton with a novel shoulder mechanism for assistive applications. In Proceedings of the 2017 IEEE International Conference on Advanced Intelligent Mechatronics (AIM), Munich, Germany, 3–7 July 2017; pp. 1041–1046. [Google Scholar]
- Ebrahimi, A.; Groninger, D.; Singer, R.; Schneider, U. Control parameter optimization of the actively powered upper body exo-skeleton using subjective feedbacks. In Proceedings of the 3rd International Conference on Control, Automation and Robotics, ICCAR, Nagoya, Japan, 22–24 April 2017; pp. 432–437. [Google Scholar] [CrossRef]
- Castro, M.N.; Rasmussen, J.; Andersen, M.S.; Bai, S. A compact 3-DOF shoulder mechanism constructed with scissors linkages for exoskeleton applications. Mech. Mach. Theory 2019, 132, 264–278. [Google Scholar] [CrossRef]
- Strzelczyk, P.; Tomczewski, K.; Wrobel, K. The Middleware for an Exoskeleton Assisting Upper Limb Movement. Sensors 2022, 22, 2986. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| i | ai−1 [mm] | αi−1 [°] | di [mm] | θi [°] |
|---|---|---|---|---|
| 1 | 0 | 0 | 100 | θ1 |
| 2 | 0 | −90 | 0 | θ2 |
| 3 | 0 | −90 | 100 | θ3 |
| 4 | 260 | 0 | −42 | θ4 |
| 5 (W) | 340 | 0 | 0 | 0 |
| Link i | mi [kg] | dGi [m] | Ixi [kg m2] | Iyi [kg m2] | Izi [kg m2] |
|---|---|---|---|---|---|
| 1 | 0.19 | 0.064 | 0.0009 | 0.0019 | 0.0009 |
| 2 | 0.01 | 0.100 | 0.0000 | 0.0001 | 0.0001 |
| 3 | 2.26 + 0.28 | 0.114 | 0.0028 | 0.0277 | 0.0277 |
| 4 | 1.35 + 0.26 | 0.118 | 0.0011 | 0.0105 | 0.0105 |
| W | 0.20 | 0.047 | 0.0002 | 0.0002 | 0.0002 |
| Maximum Torque [Nm] | Minimum Torque [Nm] | |
|---|---|---|
| Shoulder abduction–adduction | 22.05 | 4 |
| Shoulder ext.–int. rotation | 28.2 | 14.1 |
| Shoulder flexion–extension | 12 | 2.4 |
| Elbow flexion–extension | 7.5 | −3.3 |
| Length | Rest Diameter | Maximum Diameter | Maximum Force | Maximum Contraction | |
|---|---|---|---|---|---|
| Shoulder flexion | 190 mm | 15 mm | 27 mm | 850 N | 76 mm |
| Shoulder abduction | 175 mm | 15 mm | 27 mm | 2 × 850 N | 70 mm |
| Shoulder rotation | 220 mm | 15 mm | 27 mm | 850 N | 88 mm |
| Elbow flexion | 175 mm | 15 mm | 27 mm | 850 N | 70 mm |
| Device | SAA | SR | SFE | EF | S. Sph. J. | Acceptability |
|---|---|---|---|---|---|---|
| (a) | 0°/45°, a | 240°/270°, a | 90°/210°, a | 0°/90°, a | ✗ | ✗ |
| (b) | 0°/90°, a | 240°/380°, p | 30°/260°, a | na, a | ✔ | ✔ |
| (c) | na, a | np | na, a | na, a | ✗ | ✔ |
| (d) | na, p | na, p | na, p | na, p | ✔ | ✔✔✔ |
| (e) | 0°/60°, a | 240°/380°, a | np | 0°/130°, a | ✗ | ✗ |
| (f) | 5°/77°, a | 250°/320°, a | 80°/127°, a | 10°/107°, a | ✔ | ✔✔ |
| (g) | 10°/80°, a | 240°/330°, a | 70°/150°, a | 0°/130°, a | ✔ | ✔✔✔ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Durante, F.; Raparelli, T.; Zobel, P.B. Development of a 4-DoF Active Upper Limb Orthosis. Robotics 2022, 11, 122. https://doi.org/10.3390/robotics11060122
Durante F, Raparelli T, Zobel PB. Development of a 4-DoF Active Upper Limb Orthosis. Robotics. 2022; 11(6):122. https://doi.org/10.3390/robotics11060122
Chicago/Turabian StyleDurante, Francesco, Terenziano Raparelli, and Pierluigi Beomonte Zobel. 2022. "Development of a 4-DoF Active Upper Limb Orthosis" Robotics 11, no. 6: 122. https://doi.org/10.3390/robotics11060122
APA StyleDurante, F., Raparelli, T., & Zobel, P. B. (2022). Development of a 4-DoF Active Upper Limb Orthosis. Robotics, 11(6), 122. https://doi.org/10.3390/robotics11060122