

Circulating, Extracellular Vesicle-Associated Tissue Factor in Cancer Patients with and without Venous Thromboembolism

 ,
,  , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Subject and Study Design
2.2. Diagnosis of VTE
2.3. EV Isolation from Patients Blood and Analysis of EV-TF, Plasmatic TF, and Cytokine Concentration
2.4. Statistical Analysis
3. Results
3.1. Study Population
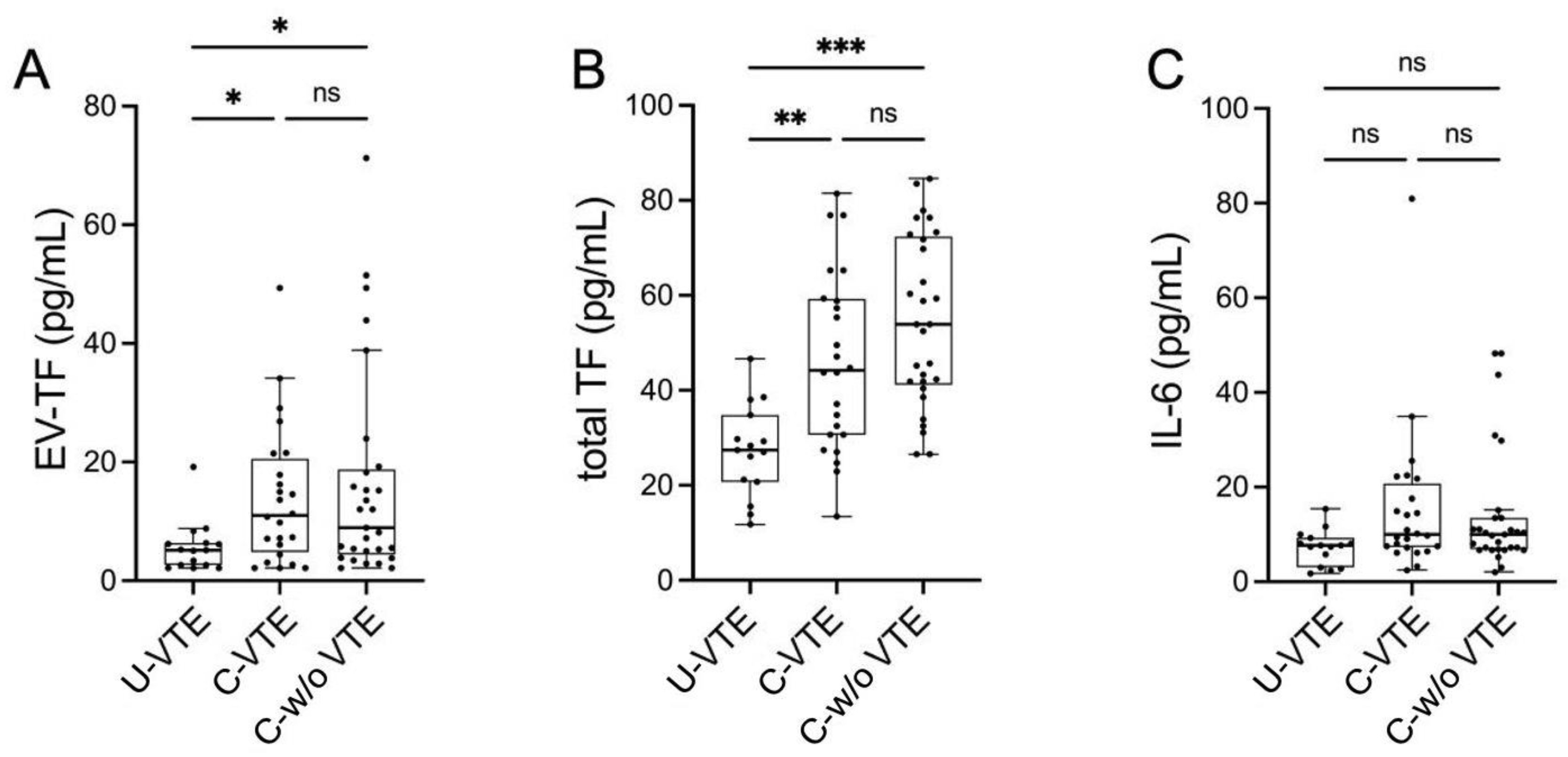
3.2. Prothrombotic Activity
3.3. Circulating IL-6 Levels
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Konstantinides, S.V.; Meyer, G.; Becattini, C.; Bueno, H.; Geersing, G.-J.; Harjola, V.-P.; Huisman, M.V.; Humbert, M.; Jennings, C.S.; Jiménez, D.; et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur. Heart J. 2020, 41, 543–603. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, A.; Brunson, A.; Adesina, O.; Keegan, T.H.M.; Wun, T. The incidence of cancer-associated thrombosis is increasing over time. Blood Adv. 2022, 6, 307–320. [Google Scholar] [CrossRef]
- Khorana, A.A.; Mackman, N.; Falanga, A.; Pabinger, I.; Noble, S.; Ageno, W.; Moik, F.; Lee, A.Y.Y. Cancer-associated venous thromboembolism. Nat. Rev. Dis. Primers 2022, 8, 11. [Google Scholar] [CrossRef] [PubMed]
- Akhmerov, A.; Parimon, T. Extracellular Vesicles, Inflammation, and Cardiovascular Disease. Cells 2022, 11, 2229. [Google Scholar] [CrossRef] [PubMed]
- Geddings, J.E.; Mackman, N. Tumor-derived tissue factor-positive microparticles and venous thrombosis in cancer patients. Blood 2013, 122, 1873–1880. [Google Scholar] [CrossRef] [PubMed]
- Nieri, D.; Neri, T.; Petrini, S.; Vagaggini, B.; Paggiaro, P.; Celi, A. Cell-derived microparticles and the lung. Eur. Respir. Rev. 2016, 25, 266–277. [Google Scholar] [CrossRef] [PubMed]
- Hisada, Y.; Mackman, N. Tissue Factor and Cancer: Regulation, Tumor Growth, and Metastasis. Semin. Thromb. Hemost. 2019, 45, 385–395. [Google Scholar] [CrossRef] [PubMed]
- Hisada, Y.; Mackman, N. Tissue Factor and Extracellular Vesicles: Activation of Coagulation and Impact on Survival in Cancer. Cancers 2021, 13, 3839. [Google Scholar] [CrossRef] [PubMed]
- Palacios-Acedo, A.L.; Mège, D.; Crescence, L.; Dignat-George, F.; Dubois, C.; Panicot-Dubois, L. Platelets, Thrombo-Inflammation, and Cancer: Collaborating With the Enemy. Front. Immunol. 2019, 10, 1805. [Google Scholar] [CrossRef] [PubMed]
- Mack, A.; Vanden Hoek, T.; Du, X. Thromboinflammation and the Role of Platelets. Arterioscler. Thromb. Vasc. Biol. 2024, 44, 1175–1180. [Google Scholar] [CrossRef]
- Wang, Y.; Golden, J.B.; Fritz, Y.; Zhang, X.; Diaconu, D.; Camhi, M.I.; Gao, H.; Dawes, S.M.; Xing, X.; Ganesh, S.K.; et al. Interleukin 6 regulates psoriasiform inflammation-associated thrombosis. JCI Insight 2016, 1, e89384. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.E.; O’Keefe, R.A.; Grandis, J.R. Targeting the IL-6/JAK/STAT3 signalling axis in cancer. Nat. Rev. Clin. Oncol. 2018, 15, 234–248. [Google Scholar] [CrossRef]
- Nieri, D.; Morani, C.; De Francesco, M.; Gaeta, R.; Niceforo, M.; De Santis, M.; Giusti, I.; Dolo, V.; Daniele, M.; Papi, A.; et al. Enhanced prothrombotic and proinflammatory activity of circulating extracellular vesicles in acute exacerbations of chronic obstructive pulmonary disease. Respir. Med. 2024, 223, 107563. [Google Scholar] [CrossRef] [PubMed]
- Scalise, V.; Lombardi, S.; Sanguinetti, C.; Nieri, D.; Pedrinelli, R.; Celi, A.; Neri, T. A novel prothrombotic role of proprotein convertase subtilisin kexin 9: The generation of procoagulant extracellular vesicles by human mononuclear cells. Mol. Biol. Rep. 2022, 49, 4129–4134. [Google Scholar] [CrossRef] [PubMed]
- Tesselaar, M.E.T.; Romijn, F.P.H.T.M.; Van Der Linden, I.K.; Prins, F.A.; Bertina, R.M.; Osanto, S. Microparticle-associated tissue factor activity: A link between cancer and thrombosis? J. Thromb. Haemost. 2007, 5, 520–527. [Google Scholar] [CrossRef]
- Tesselaar, M.E.T.; Romijn, F.P.H.T.M.; van der Linden, I.K.; Bertina, R.M.; Osanto, S. Microparticle-associated tissue factor activity in cancer patients with and without thrombosis. J. Thromb. Haemost. 2009, 7, 1421–1423. [Google Scholar] [CrossRef]
- Woei-A-Jin, F.J.S.H.; Tesselaar, M.E.T.; Garcia Rodriguez, P.; Romijn, F.P.H.T.M.; Bertina, R.M.; Osanto, S. Tissue factor-bearing microparticles and CA19.9: Two players in pancreatic cancer-associated thrombosis? Br. J. Cancer 2016, 115, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Hisada, Y.; Thålin, C.; Lundström, S.; Wallén, H.; Mackman, N. Comparison of microvesicle tissue factor activity in non-cancer severely ill patients and cancer patients. Thromb. Res. 2018, 165, 1–5. [Google Scholar] [CrossRef]
- Campello, E.; Spiezia, L.; Radu, C.M.; Bulato, C.; Castelli, M.; Gavasso, S.; Simioni, P. Endothelial, platelet, and tissue factor-bearing microparticles in cancer patients with and without venous thromboembolism. Thromb. Res. 2011, 127, 473–477. [Google Scholar] [CrossRef] [PubMed]
- Zwicker, J.I.; Liebman, H.A.; Neuberg, D.; Lacroix, R.; Bauer, K.A.; Furie, B.C.; Furie, B. Tumor-derived tissue factor-bearing microparticles are associated with venous thromboembolic events in malignancy. Clin. Cancer Res. 2009, 15, 6830–6840. [Google Scholar] [CrossRef] [PubMed]
- Koizume, S.; Miyagi, Y. Tissue factor in cancer-associated thromboembolism: Possible mechanisms and clinical applications. Br. J. Cancer 2022, 127, 2099–2107. [Google Scholar] [CrossRef]
- Brisson, A.R.; Tan, S.; Linares, R.; Gounou, C.; Arraud, N. Extracellular vesicles from activated platelets: A semiquantitative cryo-electron microscopy and immuno-gold labeling study. Platelets 2017, 28, 263–271. [Google Scholar] [CrossRef]
- Sánchez-López, V.; Gao, L.; Ferrer-Galván, M.; Arellano-Orden, E.; Elías-Hernández, T.; Jara-Palomares, L.; Asensio-Cruz, M.I.; Castro-Pérez, M.J.; Rodríguez-Martorell, F.J.; Lobo-Beristain, J.L.; et al. Differential biomarker profiles between unprovoked venous thromboembolism and cancer. Ann. Med. 2020, 52, 310–320. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, S.; Koizume, S.; Takahashi, T.; Ueno, M.; Oishi, R.; Nagashima, S.; Sano, Y.; Fukushima, T.; Tezuka, S.; Morimoto, M.; et al. Tissue factor and its procoagulant activity on cancer-associated thromboembolism in pancreatic cancer. Cancer Sci. 2021, 112, 4679–4691. [Google Scholar] [CrossRef] [PubMed]
- Khorana, A.A.; Francis, C.W.; Menzies, K.E.; Wang, J.-G.; Hyrien, O.; Hathcock, J.; Mackman, N.; Taubman, M.B. Plasma tissue factor may be predictive of venous thromboembolism in pancreatic cancer. J. Thromb. Haemost. 2008, 6, 1983–1985. [Google Scholar] [CrossRef] [PubMed]
- Reddel, C.J.; Allen, J.D.; Ehteda, A.; Taylor, R.; Chen, V.M.Y.; Curnow, J.L.; Kritharides, L.; Robertson, G. Increased thrombin generation in a mouse model of cancer cachexia is partially interleukin-6 dependent. J. Thromb. Haemost. 2017, 15, 477–486. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhang, Z.; Wei, R.; Miao, X.; Sun, S.; Liang, G.; Chu, C.; Zhao, L.; Zhu, X.; Guo, Q.; et al. IL (Interleukin)-6 Contributes to Deep Vein Thrombosis and Is Negatively Regulated by miR-338-5p. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 323–334. [Google Scholar] [CrossRef]
- Salemi, R.; Gattuso, G.; Tomasello, B.; Lavoro, A.; Gaudio, A.; Libra, M.; Signorelli, S.S.; Candido, S. Co-Occurrence of Interleukin-6 Receptor Asp358Ala Variant and High Plasma Levels of IL-6: An Evidence of IL-6 Trans-Signaling Activation in Deep Vein Thrombosis (DVT) Patients. Biomolecules 2022, 12, 681. [Google Scholar] [CrossRef] [PubMed]
- Salet, D.M.; Bekkering, S.; Middeldorp, S.; van den Hoogen, L. Targeting thromboinflammation in antiphospholipid syndrome. J. Thromb. Haemost. 2023, 21, 744–757. [Google Scholar] [CrossRef]
- Hisada, Y.; Mackman, N. Cancer cell-derived tissue factor-positive extracellular vesicles: Biomarkers of thrombosis and survival. Curr. Opin. Hematol. 2019, 26, 349–356. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| U-VTE (n = 15) | C-VTE (n = 24) | C-w/o VTE (n = 29) | p | |
|---|---|---|---|---|
| Sex (M/F) | 9/6 | 11/13 | 16/13 | NS |
| Age, years [missing values] | 70.5 ± 13.8 [0] | 66.9 ± 12.0 [0] | 69.6 ± 9.6 [0] | NS |
| BMI, kg/m2 [missing values] | 27.7 ± 3.8 [5] | 24.6 ± 4.6 [3] | 24.7 ± 4.8 [0] | NS |
| Total WBC, mL−1 [missing values] | 8010 (2640) [0] | 7745 (6150) [0] | 9520 (5140) [0] | NS |
| Neutrophils, mL−1 [missing values] | 5594 (2843) [0] | 5519 (5304) [0] | 6120 (4170) [0] | NS |
| Lymphocytes, mL−1 [missing values] | 1800 (1154) [0] | 1309 (777) [0] | 1320 (1010) [0] | NS |
| Hemoglobin, g/dL [missing values] | 14.8 (2.1) [0] | 11.3 (2.2) [0] | 11.6 (1.4) [0] | <0.001 U-VTE vs. C-VTE <0.001 U-VTE vs. C-w/o VTE |
| Hematocrit, % [missing values] | 42.0 (5.3) | 33.7 (6.8) | 35.3 (4.6) | <0.001 U-VTE vs. C-VTE <0.001 U-VTE vs. C-w/o VTE |
| Platelets, ×103/mL [missing values] | 194 (65) [0] | 218 (100) [0] | 265 (125) [0] | NS |
| aPTT, s [missing values] | 29.4 (3.2) [1] | 28.1 (3.9) [2] | 27.6 (5.5) [2] | NS |
| INR [missing values] | 1.02 (0.08) [1] | 1.12 (0.20) [1] | 1.07 (0.20) [2] | NS |
| Creatinine, mg/dL [missing values] | 0.98 ± 0.24 [0] | 0.88 ± 0.31 [0] | 0.86 ± 0.31 [0] | NS |
| eGFR, mL/min/1.73 m2 [missing values] | 84.6 ± 29.8 [2] | 81.0 ± 29.5 [2] | 81.9 ± 35.6 [0] | NS |
| Site of Primary Cancer | C-VTE (n = 24) | C-w/o VTE (n = 29) |
|---|---|---|
| Blood, n | 2 | 0 |
| Prostate, n | 0 | 1 |
| Lung, n | 9 | 20 |
| Kidney, n | 5 | 0 |
| Pancreas, n | 3 | 2 |
| Colon, n | 2 | 1 |
| Ovary, n | 1 | 0 |
| Melanoma, n | 1 | 0 |
| Breast, n | 1 | 2 |
| Liver and biliary tract, n | 0 | 2 |
| Cardias, n | 0 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lami, V.; Nieri, D.; Pagnini, M.; Gattini, M.; Donati, C.; De Santis, M.; Cipriano, A.; Bazzan, E.; Sbrana, A.; Celi, A.; et al. Circulating, Extracellular Vesicle-Associated Tissue Factor in Cancer Patients with and without Venous Thromboembolism. Biomolecules 2025, 15, 83. https://doi.org/10.3390/biom15010083
Lami V, Nieri D, Pagnini M, Gattini M, Donati C, De Santis M, Cipriano A, Bazzan E, Sbrana A, Celi A, et al. Circulating, Extracellular Vesicle-Associated Tissue Factor in Cancer Patients with and without Venous Thromboembolism. Biomolecules. 2025; 15(1):83. https://doi.org/10.3390/biom15010083
Chicago/Turabian StyleLami, Valentina, Dario Nieri, Marta Pagnini, Mario Gattini, Claudia Donati, Mariella De Santis, Alessandro Cipriano, Erica Bazzan, Andrea Sbrana, Alessandro Celi, and et al. 2025. "Circulating, Extracellular Vesicle-Associated Tissue Factor in Cancer Patients with and without Venous Thromboembolism" Biomolecules 15, no. 1: 83. https://doi.org/10.3390/biom15010083
APA StyleLami, V., Nieri, D., Pagnini, M., Gattini, M., Donati, C., De Santis, M., Cipriano, A., Bazzan, E., Sbrana, A., Celi, A., & Neri, T. (2025). Circulating, Extracellular Vesicle-Associated Tissue Factor in Cancer Patients with and without Venous Thromboembolism. Biomolecules, 15(1), 83. https://doi.org/10.3390/biom15010083