
Advances in Sjögren’s Syndrome Dry Eye Diagnostics: Biomarkers and Biomolecules beyond Clinical Symptoms


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Overview of Sjögren’s Syndrome Dry Eye
2.1. Classification
2.2. Prevalence
2.3. Pathogenesis
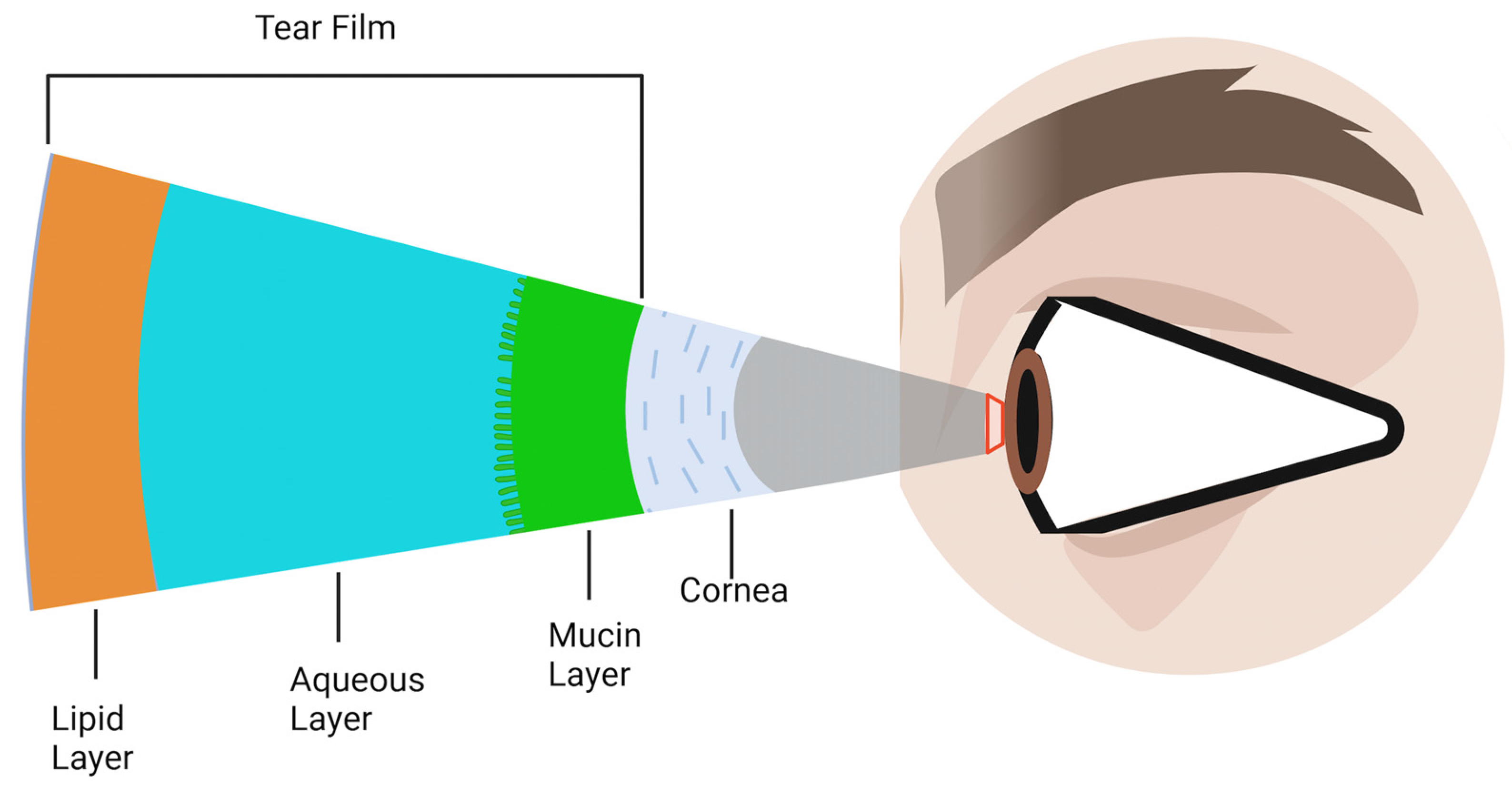
- Meibomian gland dysfunction coupled with subsequent or eventual atrophy diminishes the tear film’s lipid layer, escalating evaporation.
- The mucin layer of the tear film is compromised due to goblet cell apoptosis, resulting in reduced wettability.
- The degeneration of epithelial cells, on the other hand, causes a loss of microvilli, further exacerbating the wettability issue.
- A neurogenic inflammation of the lacrimal gland further accentuates the aqueous tear deficiency.
- Moreover, corneal nerve disturbances diminish corneal sensation and the blinking reflex.
2.4. Clinical Manifestations
2.4.1. Ocular Manifestations of SS
2.4.2. Glandular Manifestations of SS
3. Current Diagnostic Challenges in Clinical Settings
- The high prevalence of symptoms like dry eye and mouth often masks the underlying SS, posing a challenge for clinicians [4].
- The clinical manifestations of SS are broad and non-specific, coupled with its insidious onset [11].
- A fraction of SSDE patients can exhibit no symptoms or just mild ones despite significant ocular inflammation [11].
- The paucity of dependable screening tools to discern which DED patients should undergo SS evaluation [4].
- The tendency among ophthalmologists to downplay SS’s significance, leading to fewer referrals for an SS workup [12].
3.1. Significance of Timely SS Diagnosis and Its Extraglandular and Systemic Implications
3.2. Contemporary Diagnostic Protocols
- A labial salivary gland biopsy displaying focal lymphocytic sialadenitis and a focus score of 1 or more foci per 4 mm2 is awarded 3 points.
- The presence of autoantibodies, notably anti-Ro or anti-La, is attributed 3 points.
- An ocular staining score of 5 or higher, or a van Bijsterveld score of 4 or higher in at least one eye, receives 1 point.
- A Schirmer’s test result of 5 mm/5 min or lower in at least one eye earns 1 point.
- An unstimulated whole saliva flow rate of 0.1 mL/min or lower is given 1 point.
- Serological markers, including anti-RO/SSA, anti-La/SSB antibodies, ANA, and rheumatoid factor (RF), present limitations in SS screening due to their suboptimal sensitivity. Notably, ANA titers demonstrate approximately 80% reliability for SS [25], with a peak sensitivity of 68.3% [26]. Rheumatoid factor manifests in approximately 51% of SS patients [27], with a recorded sensitivity of 53% [28]. Additionally, during the disease’s initial stages, these autoantibodies may remain undetectable. Studies have indicated sensitivity ranges of 69–77% for anti-RO/SSA and 39–44% for anti-La/SSB antibodies [29].
- Both the saliva flow rate and Schirmer’s test are infrequently administered in clinical environments. Their specificity for SS is debated [9], and they are time-consuming and often deemed impractical for busy ophthalmological and dental practices.
- The utilization of the van Bijsterveld score (VBS) and ocular staining score (OSS) systems is limited among ophthalmologists. One significant concern is the use of rose bengal, which, when available in strip form, demonstrates limited effectiveness. Moreover, while rose bengal can be compounded into drops, this formulation is not only challenging to procure but also causes considerable discomfort to patients. These issues, combined with the scarcity of lissamine green in numerous eye clinics, further restrict the widespread utilization of these scoring systems. Additionally, a high OSS does not exclusively indicate SSDE, as it can also be observed in NSSDE [9].
- The minor salivary gland biopsy demonstrates low sensitivity for early SS. Even though most patients tolerate this procedure, complications such as hemorrhage, infection, paresthesia, and mucocele formation can occur [30].
3.3. Rheumatologic Workup
- The anti-Ro/SSA and anti-La/SSB, which are hallmarks of SS [31].
- The potential presence of rheumatoid factor and antinuclear antibodies (ANAs) [28].
- While anticitrullinated peptide antibodies (ACPAs) are typically linked to rheumatoid arthritis, they can be detected in approximately 10% of SS patients [32].
- Centromere antibodies (ACAs) appear in an estimated 7% of individuals with SS and have associations with Raynaud disease and scleroderma [33].
- Antimitochondrial antibodies (AMAs), found in approximately 7% of patients, correlate with primary biliary cholangitis [34].
3.4. Advanced Imaging Modalities
3.4.1. In Vivo Confocal Microscopy (IVCM)
3.4.2. Meibography
3.4.3. Imaging of the Lacrimal Gland (MRI/CT/US)
4. Novel Diagnostic Methods
4.1. Serum Analysis
4.1.1. Serum Proteomics
4.1.2. Novel Candidate Serum Antibody
4.1.3. Serum Exosomes
4.1.4. Androgen Deficiency
4.1.5. Vitamin D Deficiency
4.2. Saliva Analysis
4.2.1. Salivary Proteomics
4.2.2. Salivary Exosomes
4.2.3. Signaling Pathways
4.3. Tear Analysis
4.3.1. Tear Proteomics
4.3.2. Signaling Pathways
4.3.3. Tear Osmolarity
4.3.4. Tear Ferning
4.3.5. Barriers to Clinical Translation: The Gap between Innovation and Implementation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Akpek, E.K.; Bunya, V.Y.; Saldanha, I.J. Sjögren’s Syndrome: More Than Just Dry Eye. Cornea 2019, 38, 658–661. [Google Scholar] [CrossRef] [PubMed]
- Wu, K.Y.; Kulbay, M.; Tanasescu, C.; Jiao, B.; Nguyen, B.H.; Tran, S.D. An Overview of the Dry Eye Disease in Sjögren’s Syndrome Using Our Current Molecular Understanding. Int. J. Mol. Sci. 2023, 24, 1580. [Google Scholar] [CrossRef] [PubMed]
- Bjordal, O.; Norheim, K.B.; Rødahl, E.; Jonsson, R.; Omdal, R. Primary Sjögren’s Syndrome and the Eye. Surv. Ophthalmol. 2020, 65, 119–132. [Google Scholar] [CrossRef] [PubMed]
- Qin, B.; Wang, J.; Yang, Z.; Yang, M.; Ma, N.; Huang, F.; Zhong, R. Epidemiology of Primary Sjögren’s Syndrome: A Systematic Review and Meta-Analysis. Ann. Rheum. Dis. 2015, 74, 1983–1989. [Google Scholar] [CrossRef] [PubMed]
- Akpek, E.K.; Mathews, P.; Hahn, S.; Hessen, M.; Kim, J.; Grader-Beck, T.; Birnbaum, J.; Baer, A.N. Ocular and Systemic Morbidity in a Longitudinal Cohort of Sjögren’s Syndrome. Ophthalmology 2015, 122, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Rojas-Alcayaga, G.; Herrera, A.; Espinoza, I.; Rios-Erazo, M.; Aguilar, J.; Leiva, L.; Shakhtur, N.; Wurmann, P.; Geenen, R. Illness Experience and Quality of Life in Sjögren Syndrome Patients. Int. J. Environ. Res. Public. Health 2022, 19, 10969. [Google Scholar] [CrossRef] [PubMed]
- Nair, J.; Singh, T. Sjogren’s Syndrome: Review of the Aetiology, Pathophysiology a Potential Therapeutic Interventions. J. Clin. Exp. Dent. 2017, 9, e584–e589. [Google Scholar] [CrossRef][Green Version]
- Huang, Y.; Cheng, Q.; Jiang, C.; An, S.; Xiao, L.; Gou, Y.; Yu, W.; Lei, L.; Chen, Q.; Wang, Y.; et al. The Immune Factors Involved in the Pathogenesis, Diagnosis, and Treatment of Sjogren’s Syndrome. Clin. Dev. Immunol. 2013, 2013, 160491. [Google Scholar] [CrossRef]
- Caban, M.; Omulecki, W.; Latecka-Krajewska, B. Dry Eye in Sjögren’s Syndrome—Characteristics and Therapy. Eur. J. Ophthalmol. 2022, 32, 3174–3184. [Google Scholar] [CrossRef]
- Dong, L.; Chen, Y.; Masaki, Y.; Okazaki, T.; Umehara, H. Possible Mechanisms of Lymphoma Development in Sjogren’s Syndrome. Curr. Immunol. Rev. 2013, 9, 13–22. [Google Scholar] [CrossRef]
- Kang, Y.S.; Lee, H.S.; Li, Y.; Choi, W.; Yoon, K.C. Manifestation of Meibomian Gland Dysfunction in Patients with Sjögren’s Syndrome, Non-Sjögren’s Dry Eye, and Non-Dry Eye Controls. Int. Ophthalmol. 2018, 38, 1161–1167. [Google Scholar] [CrossRef] [PubMed]
- Bunya, V.Y.; Fernandez, K.B.; Ying, G.-S.; Massaro-Giordano, M.; Macchi, I.; Sulewski, M.E.; Hammersmith, K.M.; Nagra, P.K.; Rapuano, C.J.; Orlin, S.E. Survey of Ophthalmologists Regarding Practice Patterns for Dry Eye and Sjogren Syndrome. Eye Contact Lens 2018, 44, S196. [Google Scholar] [CrossRef] [PubMed]
- Vivino, F.B.; Minerva, P.; Huang, C.H.; Orlin, S.E. Corneal Melt as the Initial Presentation of Primary Sjögren’s Syndrome. J. Rheumatol. 2001, 28, 379–382. [Google Scholar] [PubMed]
- Braithwaite, T.; Adderley, N.J.; Subramanian, A.; Galloway, J.; Kempen, J.H.; Gokhale, K.; Cope, A.P.; Dick, A.D.; Nirantharakumar, K.; Denniston, A.K. Epidemiology of Scleritis in the United Kingdom From 1997 to 2018: Population-Based Analysis of 11 Million Patients and Association Between Scleritis and Infectious and Immune-Mediated Inflammatory Disease. Arthritis Rheumatol. 2021, 73, 1267–1276. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, J.T.; Bennett, R.M. Chronic Anterior and Posterior Uveitis and Primary Sjögren’s Syndrome. Am. J. Ophthalmol. 1987, 104, 346–352. [Google Scholar] [CrossRef]
- Sun, J.-Y.; Liu, Z.; Zhao, P.; Liu, T. Optic Neuritis as an Initial Presentation of Primary Sjögren Syndrome: A Case Report and Literature Review. Medicine 2016, 95, e5194. [Google Scholar] [CrossRef]
- Pflugfelder, S.C. Tear Dysfunction and the Cornea: LXVIII Edward Jackson Memorial Lecture. Am. J. Ophthalmol. 2011, 152, 900–909.e1. [Google Scholar] [CrossRef]
- Foulks, G.N.; Forstot, S.L.; Donshik, P.C.; Forstot, J.Z.; Goldstein, M.H.; Lemp, M.A.; Nelson, J.D.; Nichols, K.K.; Pflugfelder, S.C.; Tanzer, J.M.; et al. Clinical Guidelines for Management of Dry Eye Associated with Sjögren Disease. Ocul. Surf. 2015, 13, 118–132. [Google Scholar] [CrossRef]
- Haralampos, M.; Clio, M. Sjögren’s Syndrome. Available online: https://accessmedicine.mhmedical.com/content.aspx?sectionid=263362529&bookid=3095 (accessed on 16 October 2023).
- Di Pascuale, M.A.; Liu, T.-S.; Trattler, W.; Tseng, S.C.G. Lipid Tear Deficiency in Persistent Dry Eye after Laser in Situ Keratomileusis and Treatment Results of New Eye-Warming Device. J. Cataract Refract. Surg. 2005, 31, 1741. [Google Scholar] [CrossRef]
- Albietz, J.M.; Lenton, L.M.; Mclennan, S.G. Dry Eye after LASIK: Comparison of Outcomes for Asian and Caucasian Eyes. Clin. Exp. Optom. 2005, 88, 89–96. [Google Scholar] [CrossRef]
- Saadat, D.; Dresner, S.C. Safety of Blepharoplasty in Patients With Preoperative Dry Eyes. Arch. Facial Plast. Surg. 2004, 6, 101–104. [Google Scholar] [CrossRef] [PubMed]
- Seror, R.; Theander, E.; Brun, J.G.; Ramos-Casals, M.; Valim, V.; Dörner, T.; Bootsma, H.; Tzioufas, A.; Solans-Laqué, R.; Mandl, T.; et al. Validation of EULAR Primary Sjögren’s Syndrome Disease Activity (ESSDAI) and Patient Indexes (ESSPRI). Ann. Rheum. Dis. 2015, 74, 859–866. [Google Scholar] [CrossRef] [PubMed]
- Shiboski, C.H.; Shiboski, S.C.; Seror, R.; Criswell, L.A.; Labetoulle, M.; Lietman, T.M.; Rasmussen, A.; Scofield, H.; Vitali, C.; Bowman, S.J.; et al. 2016 American College of Rheumatology/European League Against Rheumatism Classification Criteria for Primary Sjögren’s Syndrome: A Consensus and Data-Driven Methodology Involving Three International Patient Cohorts. Arthritis Rheumatol. 2017, 69, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Haga, H.J.; Hulten, B.; Bolstad, A.I.; Ulvestad, E.; Jonsson, R. Reliability and Sensitivity of Diagnostic Tests for Primary Sjögren’s Syndrome. J. Rheumatol. 1999, 26, 604–608. [Google Scholar] [PubMed]
- Tan, E.M.; Feltkamp, T.E.W.; Smolen, J.S.; Butcher, B.; Dawkins, R.; Fritzler, M.J.; Gordon, T.; Hardin, J.A.; Kalden, J.R.; Lahita, R.G.; et al. Range of antinuclear antibodies in “healthy” individuals. Arthritis Rheum. 1997, 40, 1601–1611. [Google Scholar] [CrossRef] [PubMed]
- Pecani, A.; Alessandri, C.; Spinelli, F.R.; Priori, R.; Riccieri, V.; Di Franco, M.; Ceccarelli, F.; Colasanti, T.; Pendolino, M.; Mancini, R.; et al. Prevalence, Sensitivity and Specificity of Antibodies against Carbamylated Proteins in a Monocentric Cohort of Patients with Rheumatoid Arthritis and Other Autoimmune Rheumatic Diseases. Arthritis Res. Ther. 2016, 18, 276. [Google Scholar] [CrossRef]
- Theander, E.; Jonsson, R.; Sjöström, B.; Brokstad, K.; Olsson, P.; Henriksson, G. Prediction of Sjögren’s Syndrome Years Before Diagnosis and Identification of Patients with Early Onset and Severe Disease Course by Autoantibody Profiling. Arthritis Rheumatol. 2015, 67, 2427–2436. [Google Scholar] [CrossRef]
- Veenbergen, S.; Kozmar, A.; van Daele, P.L.A.; Schreurs, M.W.J. Autoantibodies in Sjögren’s Syndrome and Its Classification Criteria. J. Transl. Autoimmun. 2022, 5, 100138. [Google Scholar] [CrossRef]
- Liao, R.; Yang, H.-T.; Li, H.; Liu, L.-X.; Li, K.; Li, J.-J.; Liang, J.; Hong, X.-P.; Chen, Y.-L.; Liu, D.-Z. Recent Advances of Salivary Gland Biopsy in Sjögren’s Syndrome. Front. Med. 2022, 8, 792593. [Google Scholar] [CrossRef]
- Fayyaz, A.; Kurien, B.T.; Scofield, H. Autoantibodies in Sjögren’s Syndrome. Rheum. Dis. Clin. N. Am. 2016, 42, 419–434. [Google Scholar] [CrossRef]
- Molano-González, N.; Olivares-Martínez, E.; Anaya, J.; Hernández-Molina, G. Anti-Citrullinated Protein Antibodies and Arthritis in Sjögren’s Syndrome: A Systematic Review and Meta-Analysis. Scand. J. Rheumatol. 2019, 48, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Bournia, V.-K.K.; Diamanti, K.D.; Vlachoyiannopoulos, P.G.; Moutsopoulos, H.M. Anticentromere Antibody Positive Sjögren’s Syndrome: A Retrospective Descriptive Analysis. Arthritis Res. Ther. 2010, 12, R47. [Google Scholar] [CrossRef] [PubMed]
- Scofield, R.H.; Fayyaz, A.; Kurien, B.T.; Koelsch, K.A. Prognostic Value of Sjögren’s Syndrome Autoantibodies. J. Lab. Precis. Med. 2018, 3, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Luzu, J.; Labbé, A.; Réaux-Le Goazigo, A.; Rabut, G.; Liang, H.; Dupas, B.; Blautain, B.; Sène, D.; Baudouin, C. In Vivo Confocal Microscopic Study of Corneal Innervation in Sjögren’s Syndrome with or without Small Fiber Neuropathy. Ocul. Surf. 2022, 25, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Noh, S.R.; Chung, J.L.; Lee, J.M.; Seo, K.Y.; Koh, K. Meibomian Gland Atrophy with Duration of Sjogren’s Syndrome in Adult Females. Int. Ophthalmol. 2022, 42, 191–200. [Google Scholar] [CrossRef] [PubMed]
- Schäfer, V.S.; Schmidt, W.A. Ultraschalldiagnostik beim Sjögren-Syndrom. Z. Rheumatol. 2017, 76, 589–594. [Google Scholar] [CrossRef] [PubMed]
- Muntean, D.D.; Bădărînză, M.; Ștefan, P.A.; Lenghel, M.L.; Rusu, G.M.; Csutak, C.; Coroian, P.A.; Lupean, R.A.; Fodor, D. The Diagnostic Value of MRI-Based Radiomic Analysis of Lacrimal Glands in Patients with Sjögren’s Syndrome. Int. J. Mol. Sci. 2022, 23, 10051. [Google Scholar] [CrossRef] [PubMed]
- Chang, A.Y.; Purt, B. Biochemistry, Tear Film. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Masli, S.; Akpek, E.K. Reduced Tear Thrombospondin-1/Matrix Metalloproteinase-9 Ratio Can Aid in Detecting Sjögren’s Syndrome Etiology in Patients with Dry Eye. Clin. Transl. Sci. 2022, 15, 1999–2009. [Google Scholar] [CrossRef]
- Kamounah, S.; Sembler-Møller, M.L.; Nielsen, C.H.; Pedersen, A.M.L. Sjögren’s Syndrome: Novel Insights from Proteomics and miRNA Expression Analysis. Front. Immunol. 2023, 14, 1183195. [Google Scholar] [CrossRef]
- Liang, Y.; Yang, Z.; Qin, B.; Zhong, R. Primary Sjögren’s Syndrome and Malignancy Risk: A Systematic Review and Meta-Analysis. Ann. Rheum. Dis. 2014, 73, 1151–1156. [Google Scholar] [CrossRef]
- Bunya, V.Y.; Bhosai, S.J.; Heidenreich, A.M.; Kitagawa, K.; Larkin, G.B.; Lietman, T.M.; Gaynor, B.D.; Akpek, E.K.; Massaro-Giordano, M.; Srinivasan, M.; et al. Association of Dry Eye Tests With Extraocular Signs Among 3514 Participants in the Sjögren’s Syndrome International Registry. Am. J. Ophthalmol. 2016, 172, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Sembler-Møller, M.L.; Belstrøm, D.; Locht, H.; Pedersen, A.M.L. Proteomics of Saliva, Plasma, and Salivary Gland Tissue in Sjögren’s Syndrome and Non-Sjögren Patients Identify Novel Biomarker Candidates. J. Proteom. 2020, 225, 103877. [Google Scholar] [CrossRef] [PubMed]
- Barrientos, R.T.; Godín, F.; Rocha-De-Lossada, C.; Soifer, M.; Sánchez-González, J.-M.; Moreno-Toral, E.; González, A.-L.; Zein, M.; Larco, P.; Mercado, C.; et al. Ophthalmological Approach for the Diagnosis of Dry Eye Disease in Patients with Sjögren’s Syndrome. Life 2022, 12, 1899. [Google Scholar] [CrossRef] [PubMed]
- Padern, G.; Duflos, C.; Ferreira, R.; Assou, S.; Guilpain, P.; Maria, A.T.J.; Goulabchand, R.; Galea, P.; Jurtela, M.; Jorgensen, C.; et al. Identification of a Novel Serum Proteomic Signature for Primary Sjögren’s Syndrome. Front. Immunol. 2021, 12, 631539. [Google Scholar] [CrossRef] [PubMed]
- Jonsson, R.; Brokstad, K.A.; Jonsson, M.V.; Delaleu, N.; Skarstein, K. Current Concepts on Sjögren’s Syndrome—Classification Criteria and Biomarkers. Eur. J. Oral Sci. 2018, 126, 37–48. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, A.; Farine, H.; Keller, M.P.; Sebastian, A.; Kozera, L.; Welford, R.W.D.; Strasser, D.S. Immunoaffinity Targeted Mass Spectrometry Analysis of Human Plasma Samples Reveals an Imbalance of Active and Inactive CXCL10 in Primary Sjögren’s Syndrome Disease Patients. J. Proteome Res. 2020, 19, 4196–4209. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Sun, X.; Zhang, X.; Yang, Y.; Jia, R.; Liu, X.; Li, R.; Liu, Y.; Li, Z. Establishment of a Novel Diagnostic Model for Sjögren’s Syndrome by Proteomic Fingerprinting. Clin. Rheumatol. 2014, 33, 1745–1750. [Google Scholar] [CrossRef]
- Kim, Y.J.; Yeon, Y.; Lee, W.J.; Shin, Y.U.; Cho, H.; Sung, Y.-K.; Kim, D.R.; Lim, H.W.; Kang, M.H. Comparison of MicroRNA Expression in Tears of Normal Subjects and Sjögren Syndrome Patients. Investig. Ophthalmol. Vis. Sci. 2019, 60, 4889–4895. [Google Scholar] [CrossRef]
- Bunya, V.Y.; Ying, G.-S.; Maguire, M.G.; Kuklinski, E.; Lin, M.C.; Peskin, E.; Asbell, P.A.; The DREAM Study Research Group. Prevalence of Novel Candidate Sjogren Syndrome Autoantibodies in the Dry Eye Assessment and Management (DREAM) Study. Cornea 2018, 37, 1425. [Google Scholar] [CrossRef]
- Zhao, J.; An, Q.; Zhu, X.; Yang, B.; Gao, X.; Niu, Y.; Zhang, L.; Xu, K.; Ma, D. Research Status and Future Prospects of Extracellular Vesicles in Primary Sjögren’s Syndrome. Stem Cell Res. Ther. 2022, 13, 230. [Google Scholar] [CrossRef]
- Kakan, S.S.; Janga, S.R.; Cooperman, B.; Craig, D.W.; Edman, M.C.; Okamoto, C.T.; Hamm-Alvarez, S.F. Small RNA Deep Sequencing Identifies a Unique miRNA Signature Released in Serum Exosomes in a Mouse Model of Sjögren’s Syndrome. Front. Immunol. 2020, 11, 1475. [Google Scholar] [CrossRef]
- Vehof, J.; Hysi, P.G.; Hammond, C.J. A Metabolome-Wide Study of Dry Eye Disease Reveals Serum Androgens as Biomarkers. Ophthalmology 2017, 124, 505–511. [Google Scholar] [CrossRef]
- Sullivan, D.A.; Bélanger, A.; Cermak, J.M.; Bérubé, R.; Papas, A.S.; Sullivan, R.M.; Yamagami, H.; Dana, M.R.; Labrie, F. Are Women with Sjögren’s Syndrome Androgen-Deficient? J. Rheumatol. 2003, 30, 2413–2419. [Google Scholar]
- Bizzarro, A.; Valentini, G.; Martino, G.D.; Daponte, A.; De bellis, A.; Iacono, G. Influence of Testosterone Therapy on Clinical and Immunological Features of Autoimmune Diseases Associated with Klinefelter’s Syndrome. J. Clin. Endocrinol. Metab. 1987, 64, 32–36. [Google Scholar] [CrossRef]
- Golebiowski, B.; Badarudin, N.; Eden, J.; Gerrand, L.; Robinson, J.; Liu, J.; Hampel, U.; You, J.; Stapleton, F. The Effects of Transdermal Testosterone and Oestrogen Therapy on Dry Eye in Postmenopausal Women: A Randomised, Placebo-Controlled, Pilot Study. Br. J. Ophthalmol. 2017, 101, 926–932. [Google Scholar] [CrossRef]
- Athanassiou, P.; Mavragani, C.; Athanassiou, L.; Kostoglou-Athanassiou, I.; Koutsilieris, M. Vitamin D Deficiency in Primary Sjögren’s Syndrome: Association with Clinical Manifestations and Immune Activation Markers. Mediterr. J. Rheumatol. 2022, 33, 106. [Google Scholar] [CrossRef]
- Radić, M.; Kolak, E.; Đogaš, H.; Gelemanović, A.; Bučan Nenadić, D.; Vučković, M.; Radić, J. Vitamin D and Sjögren’s Disease: Revealing the Connections—A Systematic Review and Meta-Analysis. Nutrients 2023, 15, 497. [Google Scholar] [CrossRef]
- Aqrawi, L.A.; Galtung, H.K.; Vestad, B.; Øvstebø, R.; Thiede, B.; Rusthen, S.; Young, A.; Guerreiro, E.M.; Utheim, T.P.; Chen, X.; et al. Identification of Potential Saliva and Tear Biomarkers in Primary Sjögren’s Syndrome, Utilising the Extraction of Extracellular Vesicles and Proteomics Analysis. Arthritis Res. Ther. 2017, 19, 14. [Google Scholar] [CrossRef]
- Jung, J.-Y.; Kim, J.-W.; Kim, H.-A.; Suh, C.-H. Salivary Biomarkers in Patients with Sjögren’s Syndrome—A Systematic Review. Int. J. Mol. Sci. 2021, 22, 12903. [Google Scholar] [CrossRef]
- Das, N.; Menon, N.G.; de Almeida, L.G.N.; Woods, P.S.; Heynen, M.L.; Jay, G.D.; Caffery, B.; Jones, L.; Krawetz, R.; Schmidt, T.A.; et al. Proteomics Analysis of Tears and Saliva From Sjogren’s Syndrome Patients. Front. Pharmacol. 2021, 12, 787193. [Google Scholar] [CrossRef]
- Nilsson, A.; Tufvesson, E.; Hesselstrand, R.; Olsson, P.; Wollmer, P.; Mandl, T. Increased B-Cell Activating Factor, Interleukin-6, and Interleukin-8 in Induced Sputum from Primary Sjögren’s Syndrome Patients. Scand. J. Rheumatol. 2019, 48, 149–156. [Google Scholar] [CrossRef]
- Chen, X.; Wu, H.; Wei, W. Advances in the Diagnosis and Treatment of Sjogren’s Syndrome. Clin. Rheumatol. 2018, 37, 1743–1749. [Google Scholar] [CrossRef] [PubMed]
- Kapsogeorgou, E.K.; Abu-Helu, R.F.; Moutsopoulos, H.M.; Manoussakis, M.N. Salivary Gland Epithelial Cell Exosomes: A Source of Autoantigenic Ribonucleoproteins. Arthritis Rheum. 2005, 52, 1517–1521. [Google Scholar] [CrossRef] [PubMed]
- Michael, A.; Bajracharya, S.; Yuen, P.; Zhou, H.; Star, R.; Illei, G.; Alevizos, I. Exosomes from Human Saliva as a Source of microRNA Biomarkers. Oral Dis. 2010, 16, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Alevizos, I.; Alexander, S.; Turner, R.J.; Illei, G.G. MicroRNA expression profiles as biomarkers of minor salivary gland inflammation and dysfunction in Sjögren’s syndrome. Arthritis Rheum. 2011, 63, 535–544. [Google Scholar] [CrossRef]
- Aqrawi, L.A.; Galtung, H.K.; Guerreiro, E.M.; Øvstebø, R.; Thiede, B.; Utheim, T.P.; Chen, X.; Utheim, Ø.A.; Palm, Ø.; Skarstein, K.; et al. Proteomic and Histopathological Characterisation of Sicca Subjects and Primary Sjögren’s Syndrome Patients Reveals Promising Tear, Saliva and Extracellular Vesicle Disease Biomarkers. Arthritis Res. Ther. 2019, 21, 181. [Google Scholar] [CrossRef]
- Gallo, A.; Jang, S.-I.; Ong, H.L.; Perez, P.; Tandon, M.; Ambudkar, I.; Illei, G.; Alevizos, I. Targeting the Ca2+ Sensor STIM1 by Exosomal Transfer of Ebv-miR-BART13-3p Is Associated with Sjögren’s Syndrome. eBioMedicine 2016, 10, 216–226. [Google Scholar] [CrossRef]
- Yamashiro, K.; Hamada, T.; Mori, K.; Nishi, K.; Nakamura, M.; Beppu, M.; Tanaka, A.; Hijioka, H.; Kamikawa, Y.; Sugiura, T. Exosome-Derived microRNAs from Mouthrinse Have the Potential to Be Novel Biomarkers for Sjögren Syndrome. J. Pers. Med. 2022, 12, 1483. [Google Scholar] [CrossRef]
- Huang, Y.; Li, R.; Ye, S.; Lin, S.; Yin, G.; Xie, Q. Recent Advances in the Use of Exosomes in Sjögren’s Syndrome. Front. Immunol. 2020, 11, 1509. [Google Scholar] [CrossRef]
- Hsiao, Y.-T.; Huang, Y.-T.; Yu, H.-J.; Fang, P.-C.; Kuo, M.-T. Tear Proteomics Approach to Distinguishing Primary from Secondary Sjögren’s Syndrome for Dry Eye Patients with Long-Term Instillation of Eyedrops. Int. J. Mol. Sci. 2022, 23, 15239. [Google Scholar] [CrossRef]
- Akpek, E.K.; Wu, H.Y.; Karakus, S.; Zhang, Q.; Masli, S. Differential Diagnosis of Sjögren Versus Non-Sjögren Dry Eye Through Tear Film Biomarkers. Cornea 2020, 39, 991. [Google Scholar] [CrossRef] [PubMed]
- Yu, D.F.; Chen, Y.; Han, J.M.; Zhang, H.; Chen, X.P.; Zou, W.J.; Liang, L.Y.; Xu, C.C.; Liu, Z.G. MUC19 Expression in Human Ocular Surface and Lacrimal Gland and Its Alteration in Sjögren Syndrome Patients. Exp. Eye Res. 2008, 86, 403–411. [Google Scholar] [CrossRef] [PubMed]
- Kook, K.Y.; Jin, R.; Li, L.; Yoon, H.J.; Yoon, K.C. Tear Osmolarity and Matrix Metallopeptidase-9 in Dry Eye Associated with Sjögren’s Syndrome. Korean J. Ophthalmol. 2020, 34, 179–186. [Google Scholar] [CrossRef]
- Sambursky, R.; Davitt, W.F., III; Latkany, R.; Tauber, S.; Starr, C.; Friedberg, M.; Dirks, M.S.; McDonald, M. Sensitivity and Specificity of a Point-of-Care Matrix Metalloproteinase 9 Immunoassay for Diagnosing Inflammation Related to Dry Eye. JAMA Ophthalmol. 2013, 131, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Versura, P.; Giannaccare, G.; Vukatana, G.; Mulè, R.; Malavolta, N.; Campos, E.C. Predictive Role of Tear Protein Expression in the Early Diagnosis of Sjögren’s Syndrome. Ann. Clin. Biochem. 2018, 55, 561–570. [Google Scholar] [CrossRef]
- Shinzawa, M.; Dogru, M.; Den, S.; Ichijima, T.; Higa, K.; Kojima, T.; Seta, N.; Nomura, T.; Tsubota, K.; Shimazaki, J. Epidermal Fatty Acid-Binding Protein: A Novel Marker in the Diagnosis of Dry Eye Disease in Sjögren Syndrome. Int. J. Mol. Sci. 2018, 19, 3463. [Google Scholar] [CrossRef]
- Kim, M.; Kim, H.S.; Na, K.-S. Correlation between Tear Osmolarity and Other Ocular Surface Parameters in Primary Sjögren’s Syndrome. Korean J. Ophthalmol. 2017, 31, 25–31. [Google Scholar] [CrossRef]
- Versura, P.; Profazio, V.; Campos, E.C. Performance of Tear Osmolarity Compared to Previous Diagnostic Tests for Dry Eye Diseases. Curr. Eye Res. 2010, 35, 553–564. [Google Scholar] [CrossRef]
- Vehof, J.; Utheim, T.P.; Bootsma, H.; Hammond, C.J. Advances, Limitations and Future Perspectives in the Diagnosis and Management of Dry Eye in Sjögren’s Syndrome. Clin. Exp. Rheumatol. 2020, 38 (Suppl. 126), 301–309. [Google Scholar]
- Willcox, M.D.P.; Argüeso, P.; Georgiev, G.A.; Holopainen, J.M.; Laurie, G.W.; Millar, T.J.; Papas, E.B.; Rolland, J.P.; Schmidt, T.A.; Stahl, U.; et al. TFOS DEWS II Tear Film Report. Ocul. Surf. 2017, 15, 366–403. [Google Scholar] [CrossRef]
- Maragou, M.; Vaikousis, E.; Ntre, A.; Koronis, N.; Georgiou, P.; Hatzidimitriou, E.; Sotsiou, F.; Dantis, P. Tear and Saliva Ferning Tests in Sjögren’s Syndrome (SS). Clin. Rheumatol. 1996, 15, 125–132. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, K.Y.; Serhan, O.; Faucher, A.; Tran, S.D. Advances in Sjögren’s Syndrome Dry Eye Diagnostics: Biomarkers and Biomolecules beyond Clinical Symptoms. Biomolecules 2024, 14, 80. https://doi.org/10.3390/biom14010080
Wu KY, Serhan O, Faucher A, Tran SD. Advances in Sjögren’s Syndrome Dry Eye Diagnostics: Biomarkers and Biomolecules beyond Clinical Symptoms. Biomolecules. 2024; 14(1):80. https://doi.org/10.3390/biom14010080
Chicago/Turabian StyleWu, Kevin Y., Olivia Serhan, Anne Faucher, and Simon D. Tran. 2024. "Advances in Sjögren’s Syndrome Dry Eye Diagnostics: Biomarkers and Biomolecules beyond Clinical Symptoms" Biomolecules 14, no. 1: 80. https://doi.org/10.3390/biom14010080
APA StyleWu, K. Y., Serhan, O., Faucher, A., & Tran, S. D. (2024). Advances in Sjögren’s Syndrome Dry Eye Diagnostics: Biomarkers and Biomolecules beyond Clinical Symptoms. Biomolecules, 14(1), 80. https://doi.org/10.3390/biom14010080