
Impact of Tumor Necrosis Factor Receptor 1 (TNFR1) Polymorphism on Dry Eye Disease

 , , ,
, , ,
Abstract
1. Introduction
2. Methods
2.1. Study Population
2.2. Data Collected
2.3. Ocular Surface Symptoms
2.4. Assessment of Corneal Sensitivity
2.5. Ocular Surface Examination
2.6. Dry Eye Categories
2.7. Genotyping and Genetic Association Analysis
2.8. Response to Anti-Inflammatory Therapy
2.9. Statistical Analysis
3. Results
3.1. Study Population
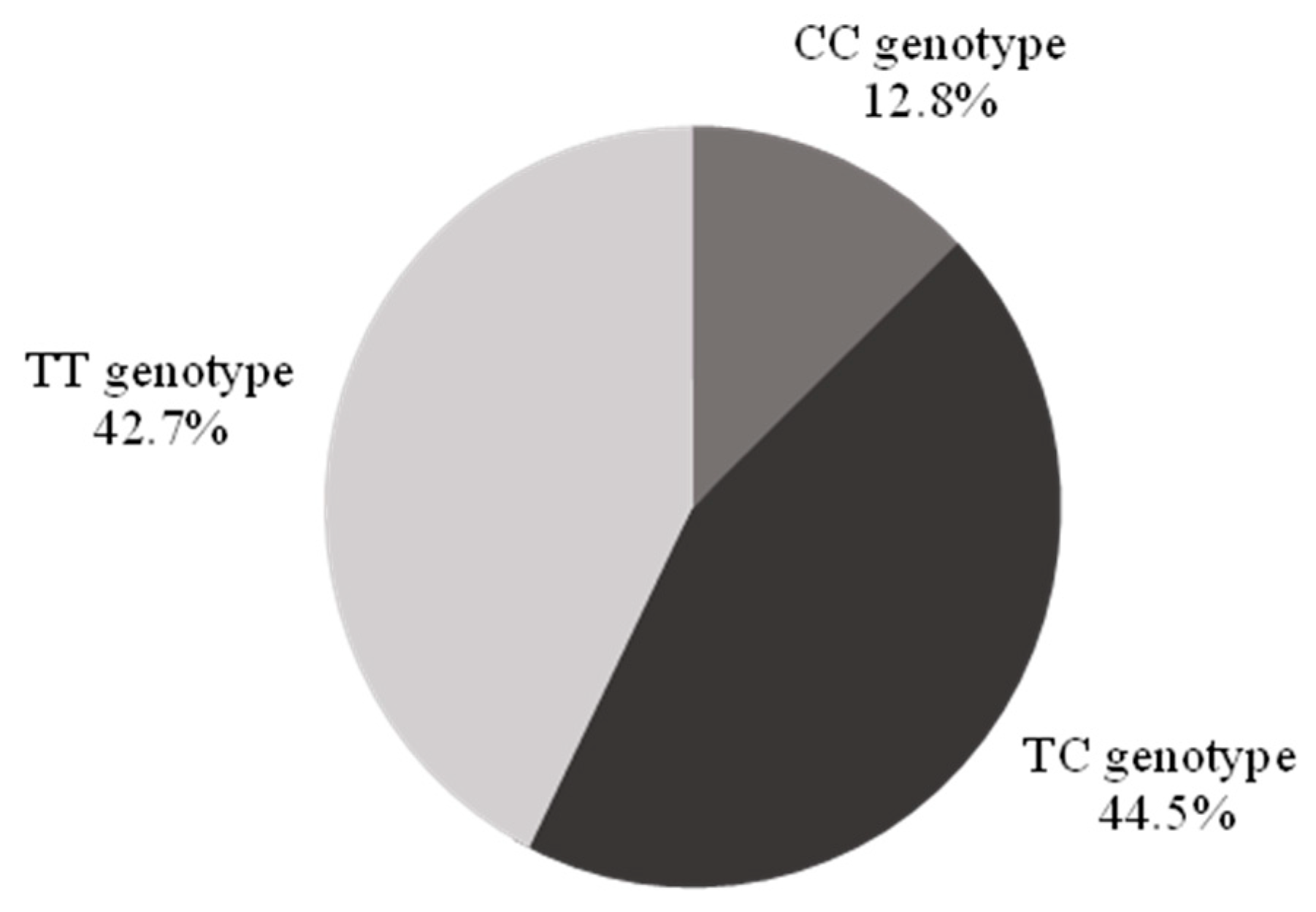
3.2. Frequency of rs1800693 Polymorphisms in the Study Population
3.3. Relationship of SNP rs1800693 to DED Symptoms and Signs
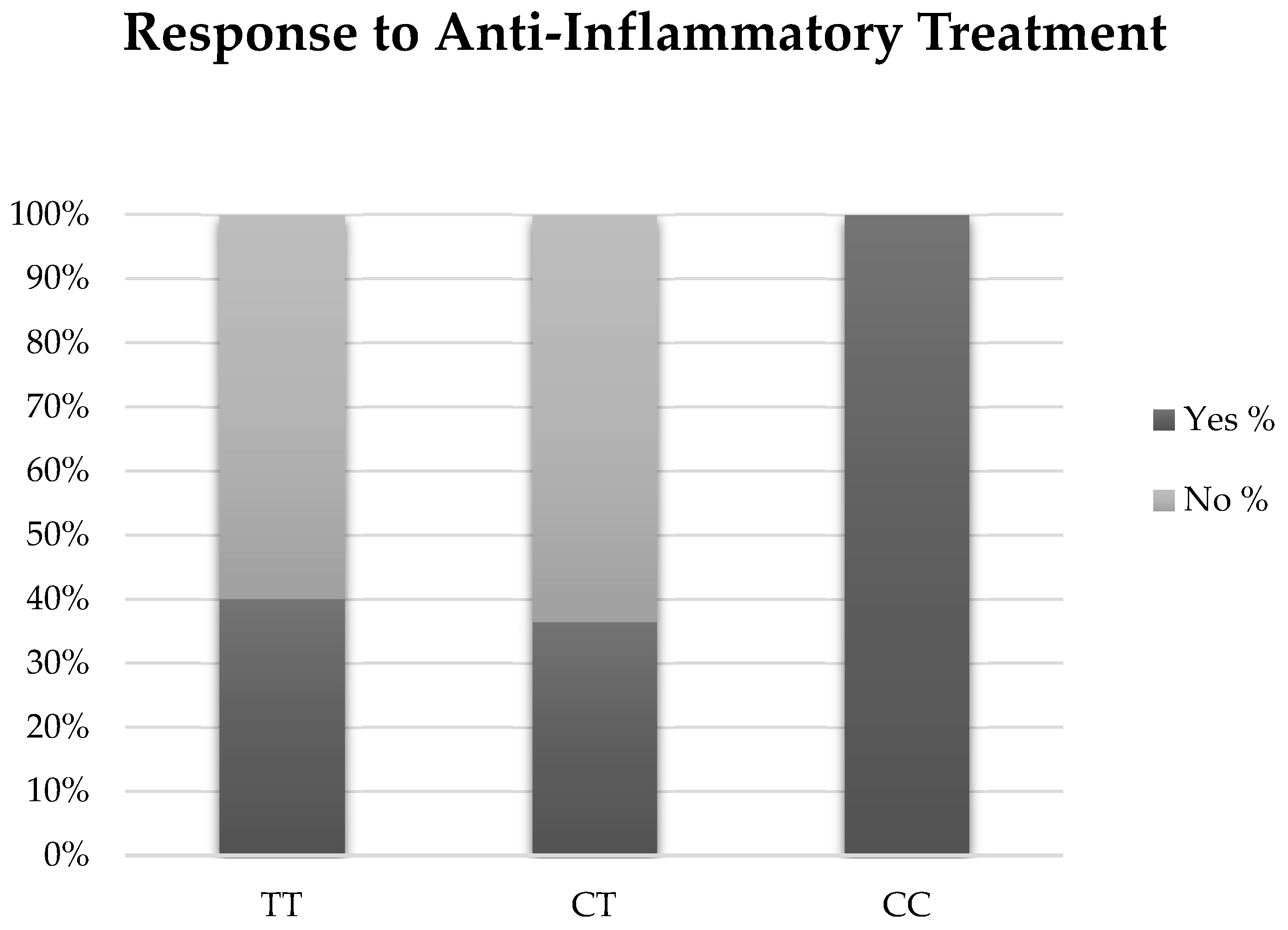
3.4. Response to Anti-Inflammatory Therapy
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wolffsohn, J.S.; Arita, R.; Chalmers, R.; Djalilian, A.; Dogru, M.; Dumbleton, K.; Gupta, P.K.; Karpecki, P.; Lazreg, S.; Pult, H.; et al. TFOS DEWS II Diagnostic Methodology report. Ocul. Surf. 2017, 15, 539–574. [Google Scholar]
- Moss, S.E.; Klein, R.; Klein, B.E. Prevalence of and risk factors for dry eye syndrome. Arch. Ophthalmol. 2000, 118, 1264–1268. [Google Scholar] [CrossRef]
- Bandeen-Roche, K.; Muñoz, B.; Tielsch, J.M.; West, S.K.; Schein, O.D. Self-reported assessment of dry eye in a population-based setting. Investig. Ophthalmol. Vis. Sci. 1997, 38, 2469–2475. [Google Scholar]
- Lin, P.Y.; Tsai, S.Y.; Cheng, C.Y.; Liu, J.H.; Chou, P.; Hsu, W.M. Prevalence of dry eye among an elderly Chinese population in Taiwan: The Shihpai Eye Study. Ophthalmology 2003, 110, 1096–1101. [Google Scholar] [CrossRef]
- Lee, A.J.; Lee, J.; Saw, S.M.; Gazzard, G.; Koh, D.; Widjaja, D.; Tan, D.T.H. Prevalence and risk factors associated with dry eye symptoms: A population based study in Indonesia. Br. J. Ophthalmol. 2002, 86, 1347–1351. [Google Scholar] [CrossRef]
- Pouyeh, B.; Viteri, E.; Feuer, W.; Lee, D.J.; Florez, H.; Fabian, J.A.; Perez, V.L.; Galor, A. Impact of ocular surface symptoms on quality of life in a United States veterans affairs population. Am. J. Ophthalmol. 2012, 153, 1061–1066.e3. [Google Scholar] [CrossRef]
- Galor, A.; Kumar, N.; Feuer, W.; Lee, D.J. Environmental factors affect the risk of dry eye syndrome in a United States veteran population. Ophthalmology 2014, 121, 972–973. [Google Scholar] [CrossRef]
- Vehof, J.; Wang, B.; Kozareva, D.; Hysi, P.G.; Snieder, H.; Hammond, C.J. The heritability of dry eye disease in a female twin cohort. Investig. Ophthalmol. Vis. Sci. 2014, 55, 7278–7283. [Google Scholar] [CrossRef]
- Imgenberg-Kreuz, J.; Rasmussen, A.; Sivils, K.; Nordmark, G. Genetics and epigenetics in primary Sjögren’s syndrome. Rheumatology (Oxford) 2021, 60, 2085–2098. [Google Scholar] [CrossRef]
- Stern, M.E.; Pflugfelder, S.C. Inflammation in dry eye. Ocul. Surf. 2004, 2, 124–130. [Google Scholar] [CrossRef]
- Gregory, A.P.; Dendrou, C.A.; Attfield, K.E.; Haghikia, A.; Xifara, D.K.; Butter, F.; Poschmann, G.; Kaur, G.; Lambert, L.; Leach, O.A.; et al. TNF receptor 1 genetic risk mirrors outcome of anti-TNF therapy in multiple sclerosis. Nature 2012, 488, 508–511. [Google Scholar] [CrossRef]
- Sugita, S.; Takase, H.; Taguchi, C.; Mochizuki, M. The role of soluble TNF receptors for TNF-alpha in uveitis. Investig. Ophthalmol. Vis. Sci. 2007, 48, 3246–3252. [Google Scholar] [CrossRef]
- Sakimoto, T.; Ohnishi, T.; Ishimori, A. Significance of ectodomain shedding of TNF receptor 1 in ocular surface. Investig. Ophthalmol. Vis. Sci. 2014, 55, 2419–2423. [Google Scholar] [CrossRef]
- Perez, V.L. Variant in The TNFRl Gene Associated with Response to Topical Anti-TNFα Antibody Fragment OCS-02 in Patients with Dry Eye Disease. Investig. Ophthalmol. Vis. Sci. 2021, 62, 921. [Google Scholar]
- Chalmers, R.L.; Begley, C.G.; Caffery, B. Validation of the 5-Item Dry Eye Questionnaire (DEQ-5): Discrimination across self-assessed severity and aqueous tear deficient dry eye diagnoses. Cont. Lens. Anterior Eye 2010, 33, 55–60. [Google Scholar] [CrossRef]
- Schiffman, R.M.; Christianson, M.D.; Jacobsen, G.; Hirsch, J.D.; Reis, B.L. Reliability and validity of the Ocular Surface Disease Index. Arch. Ophthalmol. 2000, 118, 615–621. [Google Scholar] [CrossRef]
- Farhangi, M.; Feuer, W.; Galor, A.; Bouhassira, D.; Levitt, R.C.; Sarantopoulos, C.D.; Felix, E.R. Modification of the Neuropathic Pain Symptom Inventory for use in eye pain (NPSI-Eye). Pain 2019, 160, 1541–1550. [Google Scholar] [CrossRef]
- Belmonte, C.; Acosta, M.C.; Schmelz, M.; Gallar, J. Measurement of corneal sensitivity to mechanical and chemical stimulation with a CO2 esthesiometer. Investig. Ophthalmol. Vis. Sci. 1999, 40, 513–519. [Google Scholar]
- Situ, P.; Simpson, T.L.; Fonn, D. Eccentric variation of corneal sensitivity to pneumatic stimulation at different temperatures and with CO2. Exp. Eye Res. 2007, 85, 400–405. [Google Scholar] [CrossRef]
- Perneger, T.V. What’s wrong with Bonferroni adjustments. BMJ 1998, 316, 1236–1238. [Google Scholar] [CrossRef]
- Yoon, K.C.; Jeong, I.Y.; Park, Y.G.; Yang, S.Y. Interleukin-6 and tumor necrosis factor-alpha levels in tears of patients with dry eye syndrome. Cornea 2007, 26, 431–437. [Google Scholar] [CrossRef]
- Sung, M.S.; Li, Z.; Cui, L.; Choi, J.S.; Choi, W.; Park, M.J.; Park, S.H.; Yoon, K.C. Effect of Topical 5-Aminoimidazole-4-carboxamide-1-β-d-Ribofuranoside in a Mouse Model of Experimental Dry Eye. Investig. Ophthalmol. Vis. Sci. 2015, 56, 3149–3158. [Google Scholar] [CrossRef]
- Abidi, A.; Shukla, P.; Ahmad, A. Lifitegrast: A novel drug for treatment of dry eye disease. J. Pharmacol. Pharmacother. 2016, 7, 194–198. [Google Scholar] [CrossRef]
- Murphy, C.J.; Bentley, E.; Miller, P.E.; McIntyre, K.; Leatherberry, G.; Dubielzig, R.; Giuliano, E.; Moore, C.P.; Phillips, T.E.; Smith, P.B.; et al. The pharmacologic assessment of a novel lymphocyte function-associated antigen-1 antagonist (SAR 1118) for the treatment of keratoconjunctivitis sicca in dogs. Investig. Ophthalmol. Vis. Sci. 2011, 52, 3174–3180. [Google Scholar] [CrossRef]
- Idriss, H.T.; Naismith, J.H. TNF alpha and the TNF receptor superfamily: Structure-function relationship(s). Microsc. Res. Tech. 2000, 50, 184–195. [Google Scholar] [CrossRef]
- Van Zee, K.J.; Kohno, T.; Fischer, E.; Rock, C.S.; Moldawer, L.L.; Lowry, S.F. Tumor necrosis factor soluble receptors circulate during experimental and clinical inflammation and can protect against excessive tumor necrosis factor alpha in vitro and in vivo. Proc. Natl. Acad. Sci. USA 1992, 89, 4845–4849. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Genotype | ||||
|---|---|---|---|---|
| TT (n = 140) | TC (n = 146) | CC (n = 42) | p-Value | |
| Demographics | ||||
| Age (mean± standard deviation (SD)), years | 60.8 ± 9.4 | 61.4 ± 9.9 | 65.3 ± 9.8 | 0.01 |
| Sex, male %, (n) | 92.1% (129) | 91.1% (133) | 92.9% (39) | 0.91 |
| White, Non-Hispanic % (n) | 34.6% (27) | 50.0% (39) | 15.4% (12) | 0.11 |
| Black, Non-Hispanic % (n) | 45.3% (81) | 40.8% (73) | 14.0% (25) | |
| White, Hispanic % (n) | 42.4% (28) | 50.0% (33) | 7.6% (5) | |
| Black, Hispanic % (n) | 100.0% (4) | 0% (0) | 0% (0) | |
| Comorbidities, % (n) | ||||
| Smoking (current) | 40.0% (56) | 38.4% (56) | 42.9% (18) | 0.98 |
| Hypertension | 67.9% (95) | 71.2% (104) | 69.0% (29) | 0.82 |
| Hypercholesterolemia | 58.6% (82) | 56.8% (83) | 50.0% (21) | 0.62 |
| PTSD | 17.9% (25) | 19.9% (29) | 33.3% (14) | 0.09 |
| Depression | 65.0% (91) | 56.8% (83) | 52.4% (22) | 0.22 |
| Arthritis | 51.8% (72) | 46.6% (68) | 43.9% (18) | 0.56 |
| Sleep Apnea | 23.6% (33) | 21.2% (31) | 23.8% (10) | 0.88 |
| BPH | 16.4% (23) | 17.1% (25) | 19.0% (8) | 0.93 |
| Rosacea | 3.6% (5) | 1.4% (2) | 4.8% (2) | 0.36 |
| Hepatitis C | 11.4% (16) | 11.0% (16) | 2.4% (1) | 0.21 |
| Devices and Medications, % (n) | ||||
| CPAP | 7.1% (10) | 4.1% (6) | 4.8% (2) | 0.52 |
| NSAIDs | 36.4% (51) | 31.5% (46) | 35.7% (15) | 0.66 |
| ASA | 44.3% (62) | 41.8% (61) | 38.1% (16) | 0.76 |
| Fish Oil | 10.7% (15) | 10.3% (15) | 9.5% (4) | 0.97 |
| Multivitamins | 52.1% (73) | 45.9% (67) | 59.5% (25) | 0.25 |
| Beta Blockers | 17.9% (25) | 17.1% (25) | 19.0% (8) | 0.96 |
| Statins | 54.3% (76) | 47.9% (70) | 31.0% (13) | 0.03 |
| Antidepressants | 46.4% (65) | 48.6% (71) | 45.2% (19) | 0.90 |
| Anxiolytics | 47.9% (67) | 45.9% (67) | 50.0% (21) | 0.88 |
| Analgesics | 64.0% (89) | 61.6% (90) | 66.7% (28) | 0.82 |
| Antihistamines | 22.1% (31) | 21.2% (31) | 9.5% (4) | 0.18 |
| Sildenafil | 30.7% (43) | 25.3% (37) | 50.0% (21) | 0.01 |
| Genotype | ||||
|---|---|---|---|---|
| TT (n = 140) | TC (n = 146) | CC (n = 42) | p-Value | |
| DED and ocular pain symptoms quantified by questionnaires (mean ± SD) | ||||
| DEQ-5 (range 0–22) | 10.99 ± 5.35 | 11.45 ± 5.11 | 11.19 ± 4.98 | 0.76 |
| OSDI (range 0–100) | 35.96 ± 24.99 | 34.94 ± 23.89 | 32.69 ± 24.18 | 0.75 |
| NRS (range 0–10) | 3.22 ± 2.63 | 3.21 ± 2.65 | 2.88 ± 2.61 | 0.75 |
| NPSI-Eye (range 0–40) | 21.40 ± 21.59 | 19.65 ± 20.86 | 18.38 ± 23.27 | 0.66 |
| Corneal sensation (value from right eye) (mean ± SD) | ||||
| Belmonte Esthesiometer (mL/min, range 0–200) | 84.04 ± 39.71 | 83.49 ± 40.92 | 102.55 ± 67.10 | 0.045 |
| Dry eye signs (value from more severely affected eye) (mean ± SD) | ||||
| InflammaDry (range 0–3) | 0.60 ± 0.72 | 0.70 ± 0.80 | 0.85 ± 0.99 | 0.23 |
| Upper eyelid laxity (range 0–2) | 0.59 ± 0.68 | 0.67 ± 0.69 | 0.71 ± 0.75 | 0.55 |
| Lower eyelid laxity (range 0–2) | 0.52 ± 0.60 | 0.46 ± 0.62 | 0.56 ± 0.67 | 0.58 |
| Anterior blepharitis (range 0–3) | 0.49 ± 0.60 | 0.51 ± 0.63 | 0.68 ± 0.78 | 0.46 |
| Eyelid vascularity (range 0–3) | 0.55± 0.78 | 0.57± 0.72 | 0.57 ± 0.80 | 0.98 |
| MG plugging (range 0–3) | 1.74 ± 0.90 | 1.79 ± 0.96 | 1.52 ± 0.67 | 0.25 |
| MG dropout (range 0–4) | 1.47 ± 0.95 | 1.69 ± 1.16 | 1.69 ± 1.20 | 0.20 |
| Papillae (range 0–3) | 0.61 ± 0.71 | 0.55 ± 0.67 | 0.64 ± 0.85 | 0.81 |
| Conjunctivochalasis (range 0–3) | 0.50 ± 0.33 | 0.50 ± 0.33 | 0.54 ± 0.34 | 0.80 |
| TBUT, seconds | 9.04 ± 4.15 | 8.78 ± 4.64 | 9.41 ± 4.78 | 0.70 |
| Corneal staining (range 0–15) | 1.86 ± 2.22 | 2.10 ± 2.59 | 2.38 ± 2.85 | 0.44 |
| Schirmer, mm wetting at 5 min | 13.11 ± 7.46 | 12.46 ± 7.07 | 14.57 ± 7.88 | 0.26 |
| Meibum quality (range 0–4) | 1.88 ± 1.35 | 2.08 ± 1.30 | 1.95 ± 1.29 | 0.42 |
| Anti-Inflammatory Therapy | Genotypes | Total | ||
|---|---|---|---|---|
| TT (n = 16) | CT (n = 10) | CC (n = 4) | ||
| Cyclosporine 0.05% | 43.3% (13) | 26.7% (8) | 10.0% (3) | 80.0% (24) |
| Lifitegrast 5% | 10.0% (3) | 6.7% (2) | 3.3% (1) | 20.0% (6) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Acuna, K.; Choudhary, A.; Locatelli, E.; Rodriguez, D.A.; Martin, E.R.; Levitt, R.C.; Galor, A. Impact of Tumor Necrosis Factor Receptor 1 (TNFR1) Polymorphism on Dry Eye Disease. Biomolecules 2023, 13, 262. https://doi.org/10.3390/biom13020262
Acuna K, Choudhary A, Locatelli E, Rodriguez DA, Martin ER, Levitt RC, Galor A. Impact of Tumor Necrosis Factor Receptor 1 (TNFR1) Polymorphism on Dry Eye Disease. Biomolecules. 2023; 13(2):262. https://doi.org/10.3390/biom13020262
Chicago/Turabian StyleAcuna, Kelly, Anjalee Choudhary, Elyana Locatelli, Daniel A. Rodriguez, Eden R. Martin, Roy C. Levitt, and Anat Galor. 2023. "Impact of Tumor Necrosis Factor Receptor 1 (TNFR1) Polymorphism on Dry Eye Disease" Biomolecules 13, no. 2: 262. https://doi.org/10.3390/biom13020262
APA StyleAcuna, K., Choudhary, A., Locatelli, E., Rodriguez, D. A., Martin, E. R., Levitt, R. C., & Galor, A. (2023). Impact of Tumor Necrosis Factor Receptor 1 (TNFR1) Polymorphism on Dry Eye Disease. Biomolecules, 13(2), 262. https://doi.org/10.3390/biom13020262