
Klotho Levels and Their Relationship with Inflammation and Survival among Alcoholic Patients

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Controls
2.2. Laboratory Testing
2.3. Statistics
3. Results
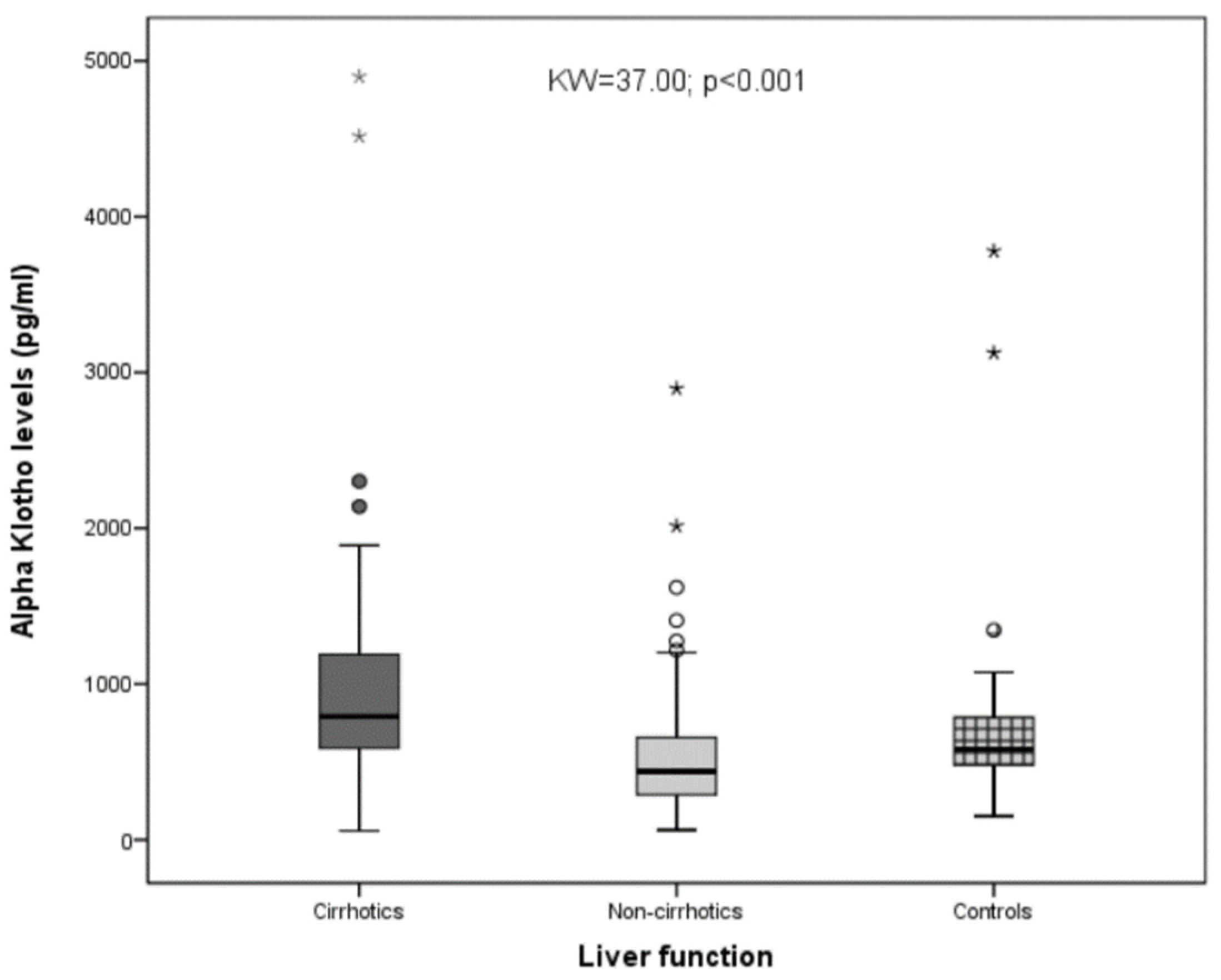
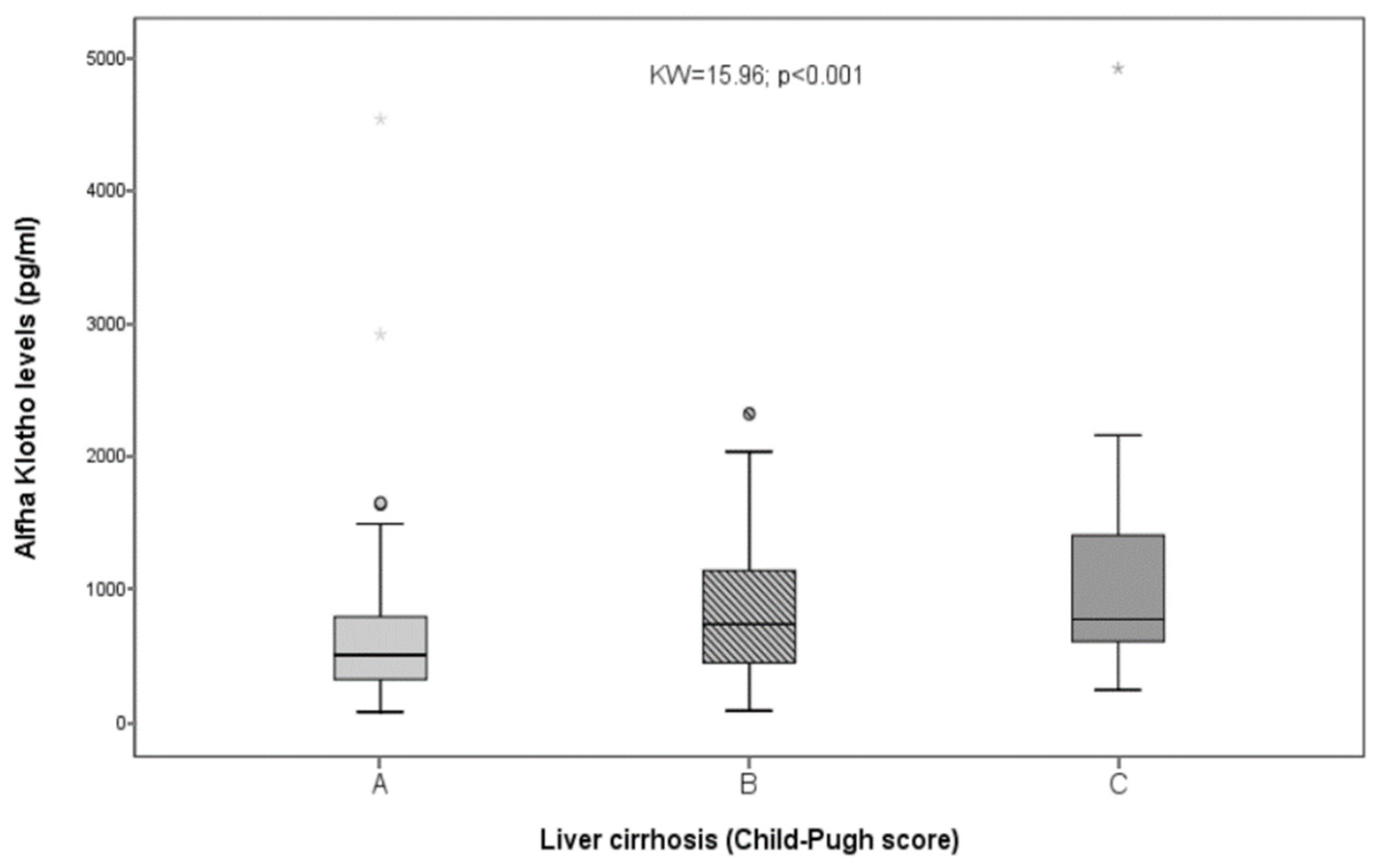
3.1. Liver Function
3.2. Klotho and Inflammation
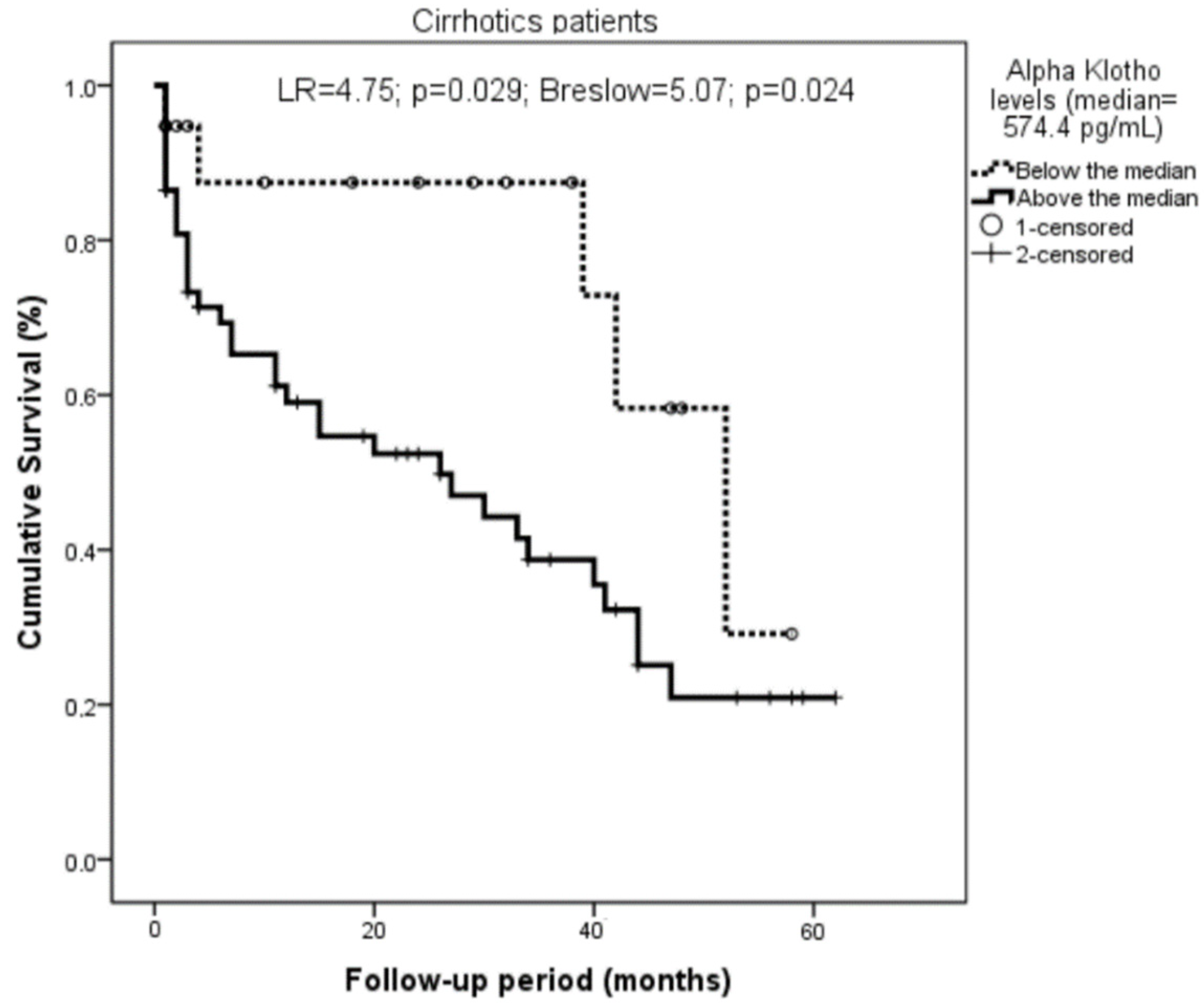
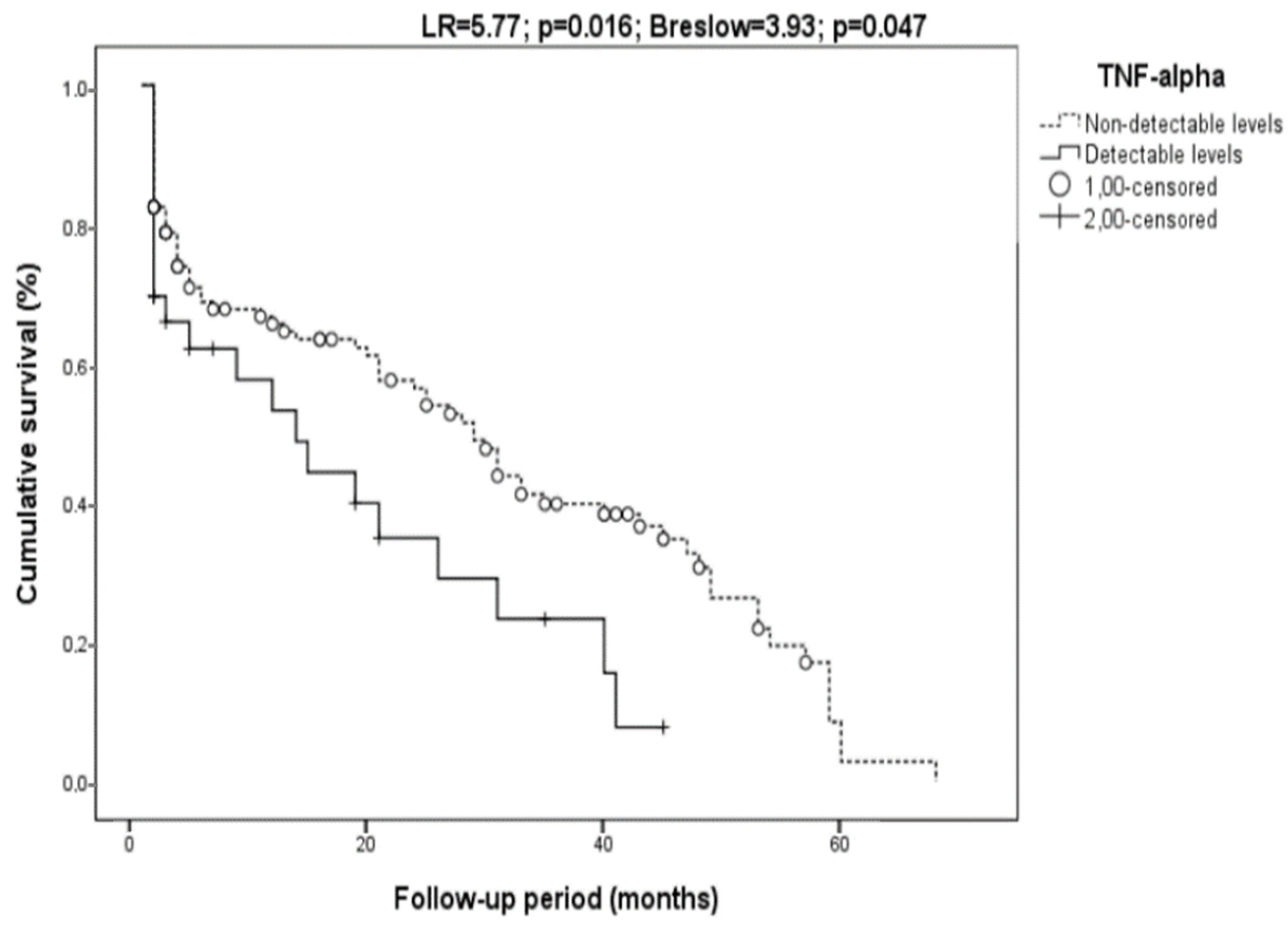
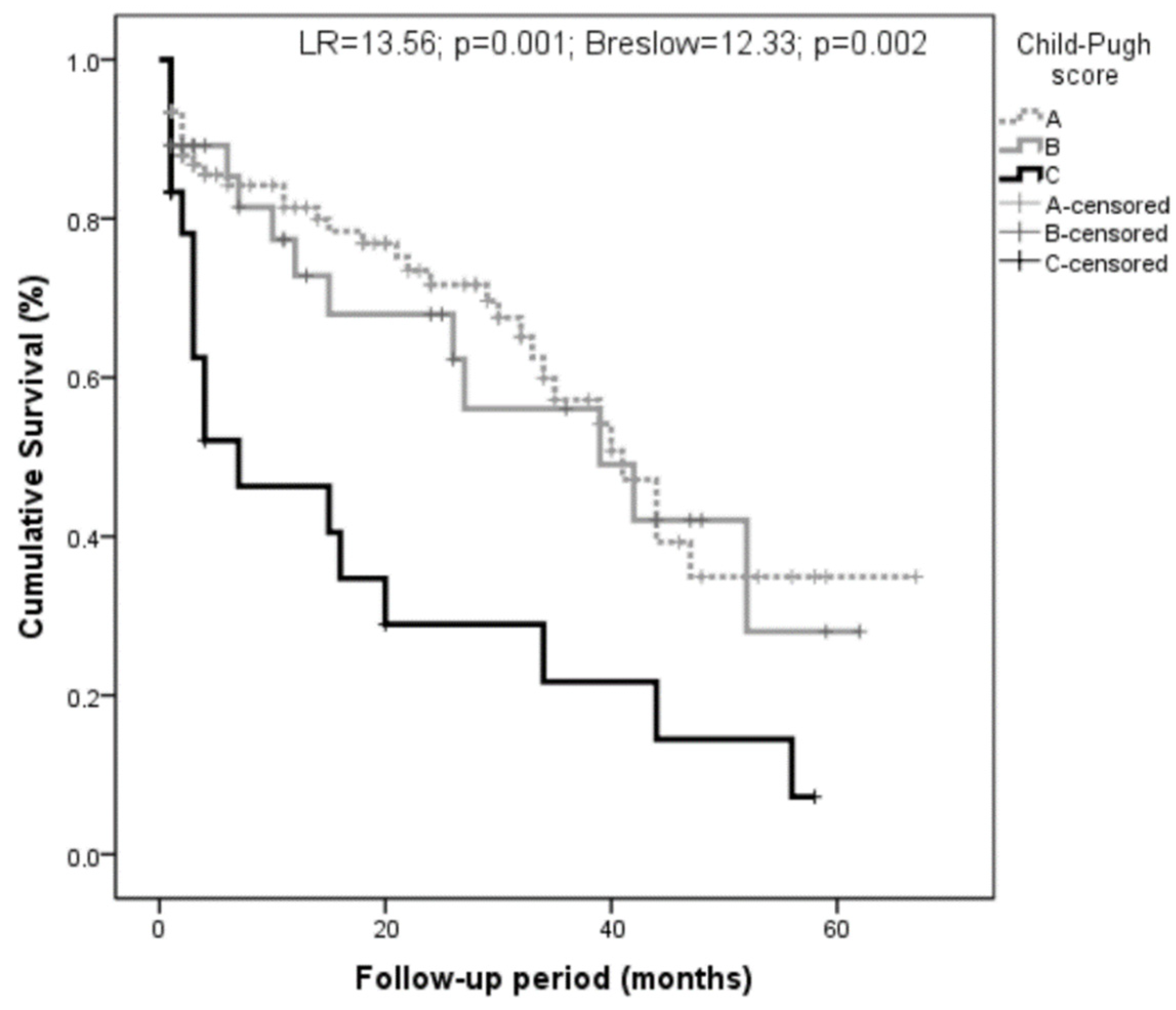
3.3. Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bjørkhaug, S.T.; Neupane, S.P.; Bramness, J.G.; Aanes, H.; Skar, V.; Medhus, A.W.; Valeur, J. Plasma Cytokine Levels in Patients with Chronic Alcohol Overconsumption: Relations to Gut Microbiota Markers and Clinical Correlates. Alcohol 2020, 85, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Buján, G.E.; Serra, H.A.; Molina, S.J.; Guelman, L.R. Oxidative Stress-Induced Brain Damage Triggered by Voluntary Ethanol Consumption during Adolescence: A Potential Target for Neuroprotection? Curr. Pharm. Des. 2019, 25, 4782–4790. [Google Scholar] [CrossRef] [PubMed]
- Ceni, E.; Mello, T.; Galli, A. Pathogenesis of Alcoholic Liver Disease: Role of Oxidative Metabolism. World J. Gastroenterol. 2014, 20, 17756–17772. [Google Scholar] [CrossRef]
- Bishehsari, F.; Magno, E.; Swanson, G.; Desai, V.; Voigt, R.M.; Forsyth, C.B.; Keshavarzian, A. Alcohol and Gut-Derived Inflammation. Alcohol Res. Curr. Rev. 2017, 38, e1–e9. [Google Scholar]
- Cavaillon, J.M. Exotoxins and Endotoxins: Inducers of Inflammatory Cytokines. Toxicon 2018, 149, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Crews, F.T.; Bechara, R.; Brown, L.A.; Guidot, D.M.; Mandrekar, P.; Oak, S.; Qin, L.; Szabo, G.; Wheeler, M.; Zou, J. Cytokines and Alcohol. Alcohol. Clin. Exp. Res. 2006, 30, 720–730. [Google Scholar] [CrossRef] [PubMed]
- Morgan, M.J.; Liu, Z.G. Crosstalk of Reactive Oxygen Species and NF-ΚB Signaling. Cell Res. 2011, 21, 103–115. [Google Scholar] [CrossRef]
- Pérez-Hernández, O.; González-Reimers, E.; Quintero-Platt, G.; Abreu-González, P.; de la Vega-Prieto, M.J.; Sánchez-Pérez, M.J.; Martín-González, C.; Martínez-Riera, A.; Santolaria-Fernández, F. Malondialdehyde as a Prognostic Factor in Alcoholic Hepatitis. Alcohol Alcohol. 2017, 52, 305–310. [Google Scholar] [CrossRef][Green Version]
- Kim, S.J.; Cheresh, P.; Eren, M.; Jablonski, R.P.; Yeldandi, A.; Ridge, K.M.; Scott Budinger, G.R.; Kim, D.H.; Wolf, M.; Vaughan, D.E.; et al. Klotho, an Antiaging Molecule, Attenuates Oxidant-Induced Alveolar Epithelial Cell MtDNA Damage and Apoptosis. Am. J. Physiol.—Lung Cell. Mol. Physiol. 2017, 313, L16–L26. [Google Scholar] [CrossRef]
- Zhou, H.J.; Li, H.; Shi, M.Q.; Mao, X.N.; Liu, D.L.; Chang, Y.R.; Gan, Y.M.; Kuang, X.; Du, J.R. Protective Effect of Klotho against Ischemic Brain Injury Is Associated with Inhibition of RIG-I/NF-ΚB Signaling. Front. Pharmacol. 2018, 8, 950. [Google Scholar] [CrossRef]
- Kuro-o, M.; Matsumura, Y.; Aizawa, H.; Kawaguchi, H.; Suga, T.; Utsugi, T.; Ohyama, Y.; Kurabayashi, M.; Kaname, T.; Kume, E.; et al. Mutation of the Mouse Klotho Gene Leads to a Syndrome Resembling Ageing. Nature 1997, 390, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Kurosu, H.; Yamamoto, M.; Clark, J.D.; Pastor, J.V.; Nandi, A.; Gurnani, P.; McGuinness, O.P.; Chikuda, H.; Yamaguchi, M.; Kawaguchi, H.; et al. Physiology: Suppression of Aging in Mice by the Hormone Klotho. Science 2005, 309, 1829–1833. [Google Scholar] [CrossRef] [PubMed]
- Maekawa, Y.; Ishikawa, K.; Yasuda, O.; Oguro, R.; Hanasaki, H.; Kida, I.; Takemura, Y.; Ohishi, M.; Katsuya, T.; Rakugi, H. Klotho Suppresses TNF-α-Induced Expression of Adhesion Molecules in the Endothelium and Attenuates NF-ΚB Activation. Endocrine 2009, 35, 341–346. [Google Scholar] [CrossRef] [PubMed]
- Xia, W.; Zhang, A.; Jia, Z.; Gu, J.; Chen, H. Klotho Contributes to Pravastatin Effect on Suppressing Il-6 Production in Endothelial Cells. Mediat. Inflamm. 2016, 2016, 2193210. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Fan, J.; Wang, S.; Sun, Z. Secreted Klotho Attenuates Inflammation-Associated Aortic Valve Fibrosis in Senescence-Accelerated Mice P1. Hypertension 2018, 71, 877–885. [Google Scholar] [CrossRef] [PubMed]
- Pathare, G.; Raju, S.; Mashru, M.; Shah, V.; Shalia, K. α-Klotho and Catalase Expression in Essential Hypertension. Integr. Mol. Med. 2020, 7, 1–6. [Google Scholar] [CrossRef]
- Yamamoto, M.; Clark, J.D.; Pastor, J.V.; Gurnani, P.; Nandi, A.; Kurosu, H.; Miyoshi, M.; Ogawa, Y.; Castrillon, D.H.; Rosenblatt, K.P.; et al. Regulation of Oxidative Stress by the Anti-Aging Hormone Klotho. J. Biol. Chem. 2005, 280, 38029–38034. [Google Scholar] [CrossRef]
- Wang, Y.; Kuro-O, M.; Sun, Z. Klotho Gene Delivery Suppresses Nox2 Expression and Attenuates Oxidative Stress in Rat Aortic Smooth Muscle Cells via the CAMP-PKA Pathway. Aging Cell 2012, 11, 410–417. [Google Scholar] [CrossRef]
- Marçais, C.; Maucort-Boulch, D.; Drai, J.; Dantony, E.; Carlier, M.C.; Blond, E.; Genet, L.; Kuentz, F.; Lataillade, D.; Legrand, E.; et al. Circulating Klotho Associates with Cardiovascular Morbidity and Mortality during Hemodialysis. J. Clin. Endocrinol. Metab. 2017, 102, 3154–3161. [Google Scholar] [CrossRef]
- Kresovich, J.K.; Bulka, C.M. Low Serum Klotho Associated With All-Cause Mortality Among a Nationally Representative Sample of American Adults. J. Gerontol. Ser. A 2022, 77, 452–456. [Google Scholar] [CrossRef]
- Seiler, S.; Rogacev, K.S.; Roth, H.J.; Shafein, P.; Emrich, I.; Neuhaus, S.; Floege, J.; Fliser, D.; Heine, G.H. Associations of FGF-23 and Sklotho with Cardiovascular Outcomes among Patients with CKD Stages 2–4. Clin. J. Am. Soc. Nephrol. 2014, 9, 1049–1058. [Google Scholar] [CrossRef] [PubMed]
- Abdelmalik, P.A.; Stevens, R.D.; Singh, S.; Skinner, J.; Carhuaopoma, J.R.; Noel, S.; Johns, R.; Fuchs, R.J. Anti-Aging Factor, Serum Alpha-Klotho, as a Marker of Acute Physiological Stress, and a Predictor of ICU Mortality, in Patients with Septic Shock. J. Crit. Care 2018, 44, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Quintero-Platt, G.; González-Reimers, E.; Rodríguez-Gaspar, M.; Martín-González, C.; Pérez-Hernández, O.; Romero-Acevedo, L.; Espelosín-Ortega, E.; de la Vega-Prieto, M.J.; Santolaria-Fernández, F. Alpha Klotho and Fibroblast Growth Factor-23 among Alcoholics. Alcohol Alcohol. 2017, 52, 542–549. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Cienfuegos, A.; Cantero-Nieto, L.; Garcia-Gomez, J.A.; Robledo, G.; González-Gay, M.A.; Ortego-Centeno, N. FGF23-Klotho Axis in Patients with Rheumatoid Arthritis. Clin. Exp. Rheumatol. 2020, 38, 50–57. [Google Scholar]
- Martín-González, C.; Gómez-Bernal, F.; Quevedo-Abeledo, J.C.; Ferrer-Moure, C.; Espelosín-Ortega, E.; González-Gay, M.Á.; Ferraz-Amaro, I. Alpha-Klotho Protein in Systemic Lupus Erythematosus. Clin. Exp. Rheumatol. 2022. Epub ahead of print. [Google Scholar] [CrossRef]
- Infante-Rivard, C.; Esnaola, S.; Villeneuve, J.P. Clinical and Statistical Validity of Conventional Prognostic Factors in Predicting Short-Term Survival among Cirrhotics. Hepatology 1987, 7, 660–664. [Google Scholar] [CrossRef]
- Kikugawa, K.; Kojima, T.; Yamaki, S.; Kosugi, H. Interpretation of the Thiobarbituric Acid Reactivity of Rat Liver and Brain Homogenates in the Presence of Ferric Ion and Ethylenediaminetetraacetic Acid. Anal. Biochem. 1992, 202, 249–255. [Google Scholar] [CrossRef]
- Hodges, D.M.; DeLong, J.M.; Forney, C.F.; Prange, R.K. Improving the Thiobarbituric Acid-Reactive-Substances Assay for Estimating Lipid Peroxidation in Plant Tissues Containing Anthocyanin and Other Interfering Compounds. Planta 1999, 207, 604–611. [Google Scholar] [CrossRef]
- Valenzuela, A. The Biological Significance of Malondialdehyde Determination in the Assessment of Tissue Oxidative Stress. Life Sci. 1991, 48, 301–309. [Google Scholar] [CrossRef]
- Prystupa, A.; Dąbrowska, A.; Sak, J.J.; Tarach, J.; Toruń-Jurkowska, A.; Lachowska-Kotowska, P.; Dzida, G. Concentrations of Fetuin-A, Osteoprotegerin and α-Klotho in Patients with Alcoholic Liver Cirrhosis. Exp. Ther. Med. 2016, 12, 3464–3470. [Google Scholar] [CrossRef][Green Version]
- Rao, Z.; Landry, T.; Li, P.; Bunner, W.; Laing, B.T.; Yuan, Y.; Huang, H. Administration of Alpha Klotho Reduces Liver and Adipose Lipid Accumulation in Obese Mice. Heliyon 2019, 5, e01494. [Google Scholar] [CrossRef]
- Huang, S.; Wang, W.; Cheng, Y.; Lin, J.; Wang, M. Clinicopathological and Prognostic Significance of Klotho and Estrogen Receptors Expression in Human Hepatocellular Carcinoma. Turkish J. Gastroenterol. Off. J. Turkish Soc. Gastroenterol. 2021, 32, 828–836. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.-Y.; Zhang, X.; Li, G.; Tang, L.-J.; Zhu, P.-W.; Rios, R.S.; Zheng, K.I.; Ma, H.-L.; Wang, X.-D.; Pan, Q.; et al. Protective Association of Klotho Rs495392 Gene Polymorphism against Hepatic Steatosis in Non-Alcoholic Fatty Liver Disease Patients. Clin. Mol. Hepatol. 2022, 28, 183–195. [Google Scholar] [CrossRef] [PubMed]
- McClain, C.J.; Song, Z.; Barve, S.S.; Hill, D.B.; Deaciuc, I. Recent Advances in Alcoholic Liver Disease. IV. Dysregulated Cytokine Metabolism in Alcoholic Liver Disease. Am. J. Physiol. Gastrointest. Liver Physiol. 2004, 287, G497–G502. [Google Scholar] [CrossRef] [PubMed]
- Ohyama, Y.; Kurabayashi, M.; Masuda, H.; Nakamura, T.; Aihara, Y.; Kaname, T.; Suga, T.; Arai, M.; Aizawa, H.; Matsumura, Y.; et al. Molecular Cloning of Rat Klotho CDNA: Markedly Decreased Expression of Klotho by Acute Inflammatory Stress. Biochem. Biophys. Res. Commun. 1998, 251, 920–925. [Google Scholar] [CrossRef]
- Chen, C.D.; Podvin, S.; Gillespie, E.; Leeman, S.E.; Abraham, C.R. Insulin Stimulates the Cleavage and Release of the Extracellular Domain of Klotho by ADAM10 and ADAM17. Proc. Natl. Acad. Sci. USA 2007, 104, 19796–19801. [Google Scholar] [CrossRef]
- Xie, H.; Zhou, F.; Liu, L.; Zhu, G.; Li, Q.; Li, C.; Gao, T. Vitiligo: How Do Oxidative Stress-Induced Autoantigens Trigger Autoimmunity? J. Dermatol. Sci. 2016, 81, 3–9. [Google Scholar] [CrossRef]
- Krick, S.; Baumlin, N.; Aller, S.P.; Aguiar, C.; Grabner, A.; Sailland, J.; Mendes, E.; Schmid, A.; Qi, L.; David, N.V.; et al. Klotho Inhibits Interleukin-8 Secretion from Cystic Fibrosis Airway Epithelia. Sci. Rep. 2017, 7, 14388. [Google Scholar] [CrossRef]
- Hsieh, C.C.; Kuro-o, M.; Rosenblatt, K.P.; Brobey, R.; Papaconstantinou, J. The ASK1-Signalosome Regulates P38 MAPK Activity in Response to Levels of Endogenous Oxidative Stress in the Klotho Mouse Models of Aging. Aging 2010, 2, 597–611. [Google Scholar] [CrossRef]
- Lim, K.; Halim, A.; Lu, T.S.; Ashworth, A.; Chong, I. Klotho: A Major Shareholder in Vascular Aging Enterprises. Int. J. Mol. Sci. 2019, 20, 4637. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cirrhotics (79) | Non-Cirrhotics (105) | T (Z); χ2 | |
|---|---|---|---|
| Sex (men/women) | 73/6 | 99/6 | χ2 = 0.04; p = 0.83 (NS) |
| Age (years) | 60.05 ± 9.87 | 58.10 ± 12.20 | T = 1.16; p = 0.25 (NS) |
| Daily ethanol (g) | 194 ± 101 200 (120–243) | 183 ± 146 147 (96–228) | Z = 1.67; p = 0.10 (NS) |
| Years of addiction | 32 ± 13 | 33 ± 14 | T = 0.37; p = 0.71 (NS) |
| MCV (fL) | 101.14 ± 10.22 100.60 (96.45–104.00) | 99.82 ± 6.17 100.60 (95.30–107.70) | Z = 0.76; p = 0.45 (NS) |
| GGT (U/L) | 348.53 ± 564.90 197.00 (71.00–390.00) | 209.29 ± 264.31 101.00 (54.00–243.50) | Z = 2.45; p = 0.014 |
| Klotho (pg/mL) | 967.98 ± 769.34 792.00 (580.60–1192.80) | 533.05 ± 410.11 439.40(289.35–660.64) | Z = 5.76; p < 0.001 |
| IL-6 (pg/mL) (*) | 14.68 ± 16.02 10.18 (4.08–18.23) | 15.21 ± 23.96 4.85 (0.92–19.64) | Z = 1.73; p = 0.08 (NS) |
| IL-8 (pg/mL) (**) | 99.30 ± 170.42 40.67 (22.65–100.00) | 49.10 ± 181.98 18.41 (11.36–30.97) | Z = 4.06; p < 0.001 |
| TNF-α (pg/mL) (***) | 5.27 ± 5.85 5.00 (1.59–5.00) | 7.72 ± 11.97 5.00 (2.75–5.00) | Z = 1.48; p = 0.14 (NS) |
| CRP (mg/L) (****) | 26.81 ± 38.12 14.40 (4.30–33.00) | 31.04 ± 56.24 11.90 (4.20–33.13) | Z = 0.22; p = 0.82 (NS) |
| MDA (µmol/L) (*****) | 4.32 ± 4.10 2.92 (1.93–5.30) | 2.75 ± 2.96 1.88 (1.26–2.84) | Z = 3.93; p < 0.001 |
| Prothrombin activity (%) | 66.37 ± 20.65 66.00 (53.00–83.00) | 87.30 ± 14.08 89.00 (79.00–100.00) | Z = 6.87; p < 0.001 |
| Albumin (g/dL) | 3.50 ± 0.80 3.50 (3.00–4.00) | 3.76 ± 0.60 3.80 (3.40–4.20) | T = 2.43; p = 0.016 |
| Bilirubin (mg/dL) | 3.41 ± 4.06 2.00 (1.00–4.20) | 1.33 ± 1.38 1.00 (1.00–2.00) | Z = 5.88; p < 0.001 |
| Platelet count (/µL) | 136,784 ± 91,302 118,000 (68,000–167,000) | 234,298 ± 116,588 213,000 (149,500–292,500) | Z = 6.39; p < 0.001 |
| Serum creatinine (mg/dL) | 1.05 ± 0.78 0.80 (0.63–1.10) | 0.84 ± 0.40 0.76 (0.61–0.91) | Z = 1.32; p = 0.18 (NS) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martín-González, C.; Espelosín-Ortega, E.; Abreu-González, P.; Fernández-Rodríguez, C.; Vera-Delgado, V.E.; González-Navarrete, L.; García-Rodríguez, A.; Riera, A.M.; González-Reimers, E. Klotho Levels and Their Relationship with Inflammation and Survival among Alcoholic Patients. Biomolecules 2022, 12, 1151. https://doi.org/10.3390/biom12081151
Martín-González C, Espelosín-Ortega E, Abreu-González P, Fernández-Rodríguez C, Vera-Delgado VE, González-Navarrete L, García-Rodríguez A, Riera AM, González-Reimers E. Klotho Levels and Their Relationship with Inflammation and Survival among Alcoholic Patients. Biomolecules. 2022; 12(8):1151. https://doi.org/10.3390/biom12081151
Chicago/Turabian StyleMartín-González, Candelaria, Elisa Espelosín-Ortega, Pedro Abreu-González, Camino Fernández-Rodríguez, Víctor Eugenio Vera-Delgado, Lourdes González-Navarrete, Alen García-Rodríguez, Antonio Martínez Riera, and Emilio González-Reimers. 2022. "Klotho Levels and Their Relationship with Inflammation and Survival among Alcoholic Patients" Biomolecules 12, no. 8: 1151. https://doi.org/10.3390/biom12081151
APA StyleMartín-González, C., Espelosín-Ortega, E., Abreu-González, P., Fernández-Rodríguez, C., Vera-Delgado, V. E., González-Navarrete, L., García-Rodríguez, A., Riera, A. M., & González-Reimers, E. (2022). Klotho Levels and Their Relationship with Inflammation and Survival among Alcoholic Patients. Biomolecules, 12(8), 1151. https://doi.org/10.3390/biom12081151