
Increase in Serum MMP-9 and TIMP-1 Concentrations during Alcohol Intoxication in Adolescents—A Preliminary Study

 ,
,
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Global Status Report on Alcohol and Health 2018; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Hyun, J.; Han, J.; Lee, C.; Yoon, M.; Jung, Y. Pathophysiological Aspects of Alcohol Metabolism in the Liver. Int. J. Mol. Sci. 2021, 22, 5717. [Google Scholar] [CrossRef] [PubMed]
- Pohl, K.; Moodley, P.; Dhanda, A.D. Alcohol’s Impact on the Gut and Liver. Nutrients 2021, 13, 3170. [Google Scholar] [CrossRef] [PubMed]
- Crabb, D.W.; Im, G.Y.; Szabo, G.; Mellinger, J.L.; Lucey, M.R. Diagnosis and Treatment of Alcohol-Associated Liver Diseases: 2019 Practice Guidance From the American Association for the Study of Liver Diseases. Hepatology 2020, 71, 306–333. [Google Scholar] [CrossRef] [PubMed]
- Le Daré, B.; Lagente, V.; Gicquel, T. Ethanol and its metabolites: Update on toxicity, benefits, and focus on immunomodulatory effects. Drug Metab. Rev. 2019, 51, 545–561. [Google Scholar] [CrossRef]
- Lackner, C.; Stauber, R.E.; Davies, S.; Denk, H.; Dienes, H.P.; Gnemmi, V.; Guido, M.; Miquel, R.; Paradis, V.; Schirmacher, P.; et al. Development and prognostic relevance of a histologic grading and staging system for alcohol-related liver disease. J. Hepatol. 2021, 75, 810–819. [Google Scholar] [CrossRef]
- Enomoto, H.; Bando, Y.; Nakamura, H.; Nishiguchi, S.; Koga, M. Liver fibrosis markers of nonalcoholic steatohepatitis. World J. Gastroenterol. 2015, 21, 7427–7435. [Google Scholar] [CrossRef]
- Charzewski, Ł.; Krzyśko, K.A.; Lesyng, B. Structural characterisation of inhibitory and non-inhibitory MMP-9-TIMP-1 complexes and implications for regulatory mechanisms of MMP-9. Sci. Rep. 2021, 11, 13376. [Google Scholar] [CrossRef]
- Jotwani, R.; Eswaran, S.V.; Moonga, S.; Cutler, C.W. MMP-9/TIMP-1 imbalance induced in human dendritic cells by Porphyromonas gingivalis. FEMS Immunol. Med. Microbiol. 2010, 58, 314–321. [Google Scholar] [CrossRef]
- Schuppan, D.; Surabattula, R.; Wang, X.Y. Determinants of fibrosis progression and regression in NASH. J. Hepatol. 2018, 68, 238–250. [Google Scholar] [CrossRef]
- Cicoira, M.; Rossi, A.; Bonapace, S.; Zanolla, L.; Golia, G.; Franceschini, L.; Caruso, B.; Marino, P.N.; Zardini, P. Independent and additional prognostic value of aminoterminal propeptide of type III procollagen circulating levels in patients with chronic heart failure. J. Card. Fail. 2004, 10, 403–411. [Google Scholar] [CrossRef]
- Lachowski, D.; Cortes, E.; Rice, A.; Pinato, D.; Rombouts, K.; Del Rio Hernandez, A. Matrix stiffness modulates the activity of MMP-9 and TIMP-1 in hepatic stellate cells to perpetuate fibrosis. Sci. Rep. 2019, 9, 7299. [Google Scholar] [CrossRef] [PubMed]
- Mukamal, K.J. A safe level of alcohol consumption: The right answer demands the right question. J. Intern. Med. 2020, 288, 550–559. [Google Scholar] [CrossRef] [PubMed]
- Torp, N.; Israelsen, M.; Nielsen, M.J.; Åstrand, C.P.; Juhl, P.; Johansen, S.; Hansen, C.D.; Madsen, B.; Villesen, I.F.; Leeming, D.J.; et al. Binge drinking induces an acute burst of markers of hepatic fibrogenesis (PRO-C3). Liver Int. 2022, 42, 92–101. [Google Scholar] [CrossRef] [PubMed]
- Zdanowicz, K.; Olanski, W.; Kowalczuk-Kryston, M.; Bobrus-Chociej, A.; Werpachowska, I.; Lebensztejn, D.M. Total Keratin-18 (M65) as a Potential, Early, Non-Invasive Biomarker of Hepatocyte Injury in Alcohol Intoxicated Adolescents-A Preliminary Study. Biomolecules 2021, 11, 911. [Google Scholar] [CrossRef]
- Cordell, R.L.; Pandya, H.; Hubbard, M.; Turner, M.A.; Monks, P.S. GC-MS analysis of ethanol and other volatile compounds in micro-volume blood samples--quantifying neonatal exposure. Anal. Bioanal. Chem. 2013, 405, 4139–4147. [Google Scholar] [CrossRef]
- Liangpunsakul, S.; Qi, R.; Crabb, D.W.; Witzmann, F. Relationship between alcohol drinking and aspartate aminotransferase:alanine aminotransferase (AST:ALT) ratio, mean corpuscular volume (MCV), gamma-glutamyl transpeptidase (GGT), and apolipoprotein A1 and B in the U.S. population. J. Stud. Alcohol. Drugs 2010, 71, 249–252. [Google Scholar] [CrossRef]
- Ohashi, K.; Pimienta, M.; Seki, E. Alcoholic liver disease: A current molecular and clinical perspective. Liver Res. 2018, 2, 161–172. [Google Scholar] [CrossRef]
- Cabral-Pacheco, G.A.; Garza-Veloz, I.; Castruita-De la Rosa, C.; Ramirez-Acuña, J.M.; Perez-Romero, B.A.; Guerrero-Rodriguez, J.F.; Martinez-Avila, N.; Martinez-Fierro, M.L. The Roles of Matrix Metalloproteinases and Their Inhibitors in Human Diseases. Int. J. Mol. Sci. 2020, 21, 9739. [Google Scholar] [CrossRef]
- Aiken, A.; Clare, P.J.; Wadolowski, M.; Hutchinson, D.; Najman, J.M.; Slade, T.; Bruno, R.; McBride, N.; Kypri, K.; Mattick, R.P. Age of Alcohol Initiation and Progression to Binge Drinking in Adolescence: A Prospective Cohort Study. Alcohol. Clin. Exp. Res. 2018, 42, 100–110. [Google Scholar] [CrossRef]
- Center for Behaviora Health, Statistics. 2016 National Survey on Drug Use and Health Public Use File Codebook. Substance. Abuse and Mental Health Services Administration 2017. Available online: http://www.samhsa.gov/ (accessed on 1 February 2022).
- Lees, B.; Meredith, L.R.; Kirkland, A.E.; Bryant, B.E.; Squeglia, L.M. Effect of alcohol use on the adolescent brain and behavior. Pharmacol. Biochem. Behav. 2020, 192, 172906. [Google Scholar] [CrossRef]
- Hagström, H.; Hemmingsson, T.; Discacciati, A.; Andreasson, A. Alcohol consumption in late adolescence is associated with an increased risk of severe liver disease later in life. J. Hepatol. 2018, 68, 505–510. [Google Scholar] [CrossRef] [PubMed]
- Hagström, H.; Hemmingsson, T.; Discacciati, A.; Andreasson, A. Risk Behaviors Associated with Alcohol Consumption Predict Future Severe Liver Disease. Dig. Dis. Sci. 2019, 64, 2014–2023. [Google Scholar] [CrossRef] [PubMed]
- Roderfeld, M. Matrix metalloproteinase functions in hepatic injury and fibrosis. Matrix Biol. 2018, 68–69, 452–462. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Liu, X.; Zhang, J.; Lu, L.; Feng, M.; Wang, J. Dynamic features of liver fibrogenesis and fibrosis resolution in the absence of matrix metalloproteinase-9. Mol. Med. Rep. 2019, 20, 5239–5248. [Google Scholar] [CrossRef]
- Li, Y.; Liu, H.; Xu, L. Expression of MMP-9 in different degrees of chronic hepatitis B and its correlation with inflammation. Exp. Ther. Med. 2018, 16, 4136–4140. [Google Scholar] [CrossRef]
- D’Amico, F.; Consolo, M.; Amoroso, A.; Skarmoutsou, E.; Mauceri, B.; Stivala, F.; Stivala, F.; Malaponte, G.; Bertino, G.; Neri, S.; et al. Liver immunolocalization and plasma levels of MMP-9 in non-alcoholic steatohepatitis (NASH) and hepatitis C infection. Acta Histochem. 2010, 112, 474–481. [Google Scholar] [CrossRef]
- Lebensztejn, D.M.; Sobaniec-Lotowska, M.E.; Kaczmarski, M.; Voelker, M.; Schuppan, D. Matrix-derived serum markers in monitoring liver fibrosis in children with chronic hepatitis B treated with interferon alpha. World J. Gastroenterol. 2006, 12, 3338–3343. [Google Scholar] [CrossRef]
- Wei, L.; Shao, C.; Luo, L.; He, H.; Xv, S.; Shi, L.; Qiu, S.; Gu, H.; Zhu, C.; Chen, J.; et al. Predictive Value of the Serum Matrix Metalloproteinase-9 Level on Hepatic Encephalopathy in Patients with Chronic Liver Disease. Ann. Clin. Lab. Sci. 2021, 51, 713–720. [Google Scholar]
- Daniluk, U.; Daniluk, J.; Guzinska-Ustymowicz, K.; Pryczynicz, A.; Lebensztejn, D. Usefulness of metalloproteinase-9 and tissue inhibitor of metalloproteinase-1 in clinical characterisation of children with newly diagnosed Crohn’s disease. J. Paediatr. Child. Health 2020, 56, 1233–1241. [Google Scholar] [CrossRef]
- Prystupa, A.; Boguszewska-Czubara, A.; Bojarska-Junak, A.; Toruń-Jurkowska, A.; Roliński, J.; Załuska, W. Activity of MMP-2, MMP-8 and MMP-9 in serum as a marker of progression of alcoholic liver disease in people from Lublin Region, eastern Poland. Ann. Agric. Environ. Med. 2015, 22, 325–328. [Google Scholar] [CrossRef]
- Roeb, E. Matrix metalloproteinases and liver fibrosis (translational aspects). Matrix Biol. 2018, 68–69, 463–473. [Google Scholar] [CrossRef] [PubMed]
- Latronico, T.; Mascia, C.; Pati, I.; Zuccala, P.; Mengoni, F.; Marocco, R.; Tieghi, T.; Belvisi, V.; Lichtner, M.; Vullo, V.; et al. Liver Fibrosis in HCV Monoinfected and HIV/HCV Coinfected Patients: Dysregulation of Matrix Metalloproteinases (MMPs) and Their Tissue Inhibitors TIMPs and Effect of HCV Protease Inhibitors. Int. J. Mol. Sci. 2016, 17, 455. [Google Scholar] [CrossRef] [PubMed]
- Karsdal, M.A.; Daniels, S.J.; Holm Nielsen, S.; Bager, C.; Rasmussen, D.G.K.; Loomba, R.; Surabattula, R.; Villesen, I.F.; Luo, Y.; Shevell, D.; et al. Collagen biology and non-invasive biomarkers of liver fibrosis. Liver Int. 2020, 40, 736–750. [Google Scholar] [CrossRef] [PubMed]
- Israelsen, M.; Kim, M.; Suvitaival, T.; Madsen, B.S.; Hansen, C.D.; Torp, N.; Trost, K.; Thiele, M.; Hansen, T.; Legido-Quigley, C.; et al. Comprehensive lipidomics reveals phenotypic differences in hepatic lipid turnover in ALD and NAFLD during alcohol intoxication. JHEP Rep. 2021, 3, 100325. [Google Scholar] [CrossRef]
- Sørensen, M.D.; Thiele, M.; Krag, A.; Daniels, S.J.; Leeming, D.J.; Karsdal, M.; Detlefsen, S. Stage-dependent expression of fibrogenic markers in alcohol-related liver disease. Pathol. Res. Pract. 2022, 231, 153798. [Google Scholar] [CrossRef]
- Mak, A.L.; Lee, J.; van Dijk, A.M.; Vali, Y.; Aithal, G.P.; Schattenberg, J.M.; Anstee, Q.M.; Brosnan, M.J.; Zafarmand, M.H.; Ramsoekh, D.; et al. Systematic Review with Meta-Analysis: Diagnostic Accuracy of Pro-C3 for Hepatic Fibrosis in Patients with Non-Alcoholic Fatty Liver Disease. Biomedicines 2021, 9, 1920. [Google Scholar] [CrossRef]
- Madsen, B.S.; Thiele, M.; Detlefsen, S.; Kjaergaard, M.; Møller, L.S.; Trebicka, J.; Nielsen, M.J.; Gudmann, N.S.; Leeming, D.J.; Karsdal, M.A.; et al. PRO-C3 and ADAPT algorithm accurately identify patients with advanced fibrosis due to alcohol-related liver disease. Aliment. Pharmacol. Ther. 2021, 54, 699–708. [Google Scholar] [CrossRef]
- Sorva, R.; Anttila, R.; Siimes, M.A.; Sorva, A.; Tähtelä, R.; Turpeinen, M. Serum markers of collagen metabolism and serum osteocalcin in relation to pubertal development in 57 boys at 14 years of age. Pediatr. Res. 1997, 42, 528–532. [Google Scholar] [CrossRef][Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Study Group (n = 57) | Control Group (n = 24) | p |
|---|---|---|---|
| Alcohol (g/L) | 1.78 (0.48–3.26) | - | NA |
| Age (years) | 15 (12–17) | 16 (12–17) | NS |
| ALT (IU/L) | 13 (7–48) | 13 (11–15) | NS |
| AST (IU/L) | 22 (14–45) | 20 (14–29) | NS |
| PIIINP (ng/mL) | 25.66 (14.34–48.42) | 24.67 (12.96–40.82) | NS |
| Collagen IV (ng/mL) | 68.11 (40.72–121.1) | 70.79 (43.16–108.1) | NS |
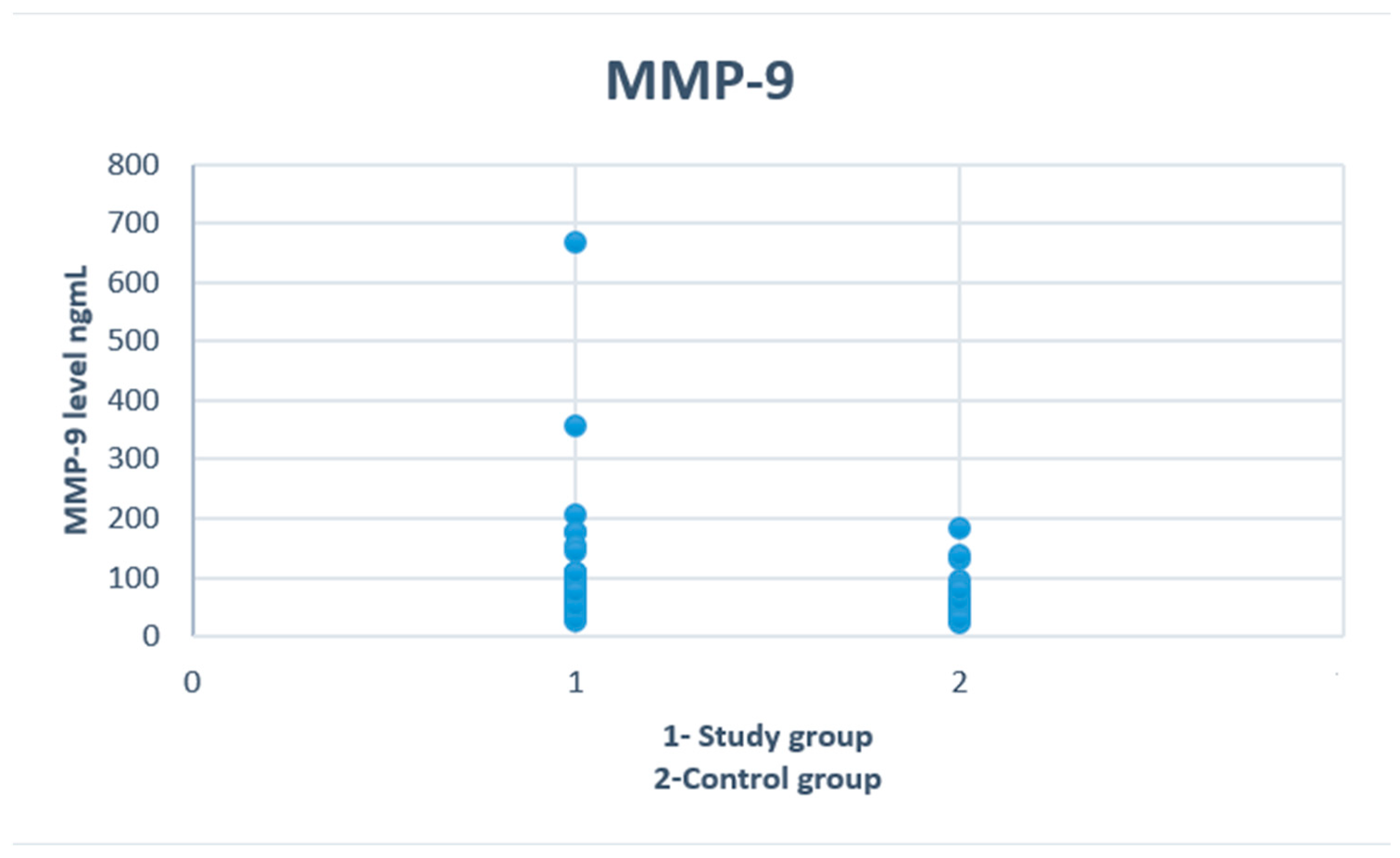
| MMP-9 (ng/mL) | 72.4 (26.4–667.4) | 58 (22.8–183.0) | 0.02 * |
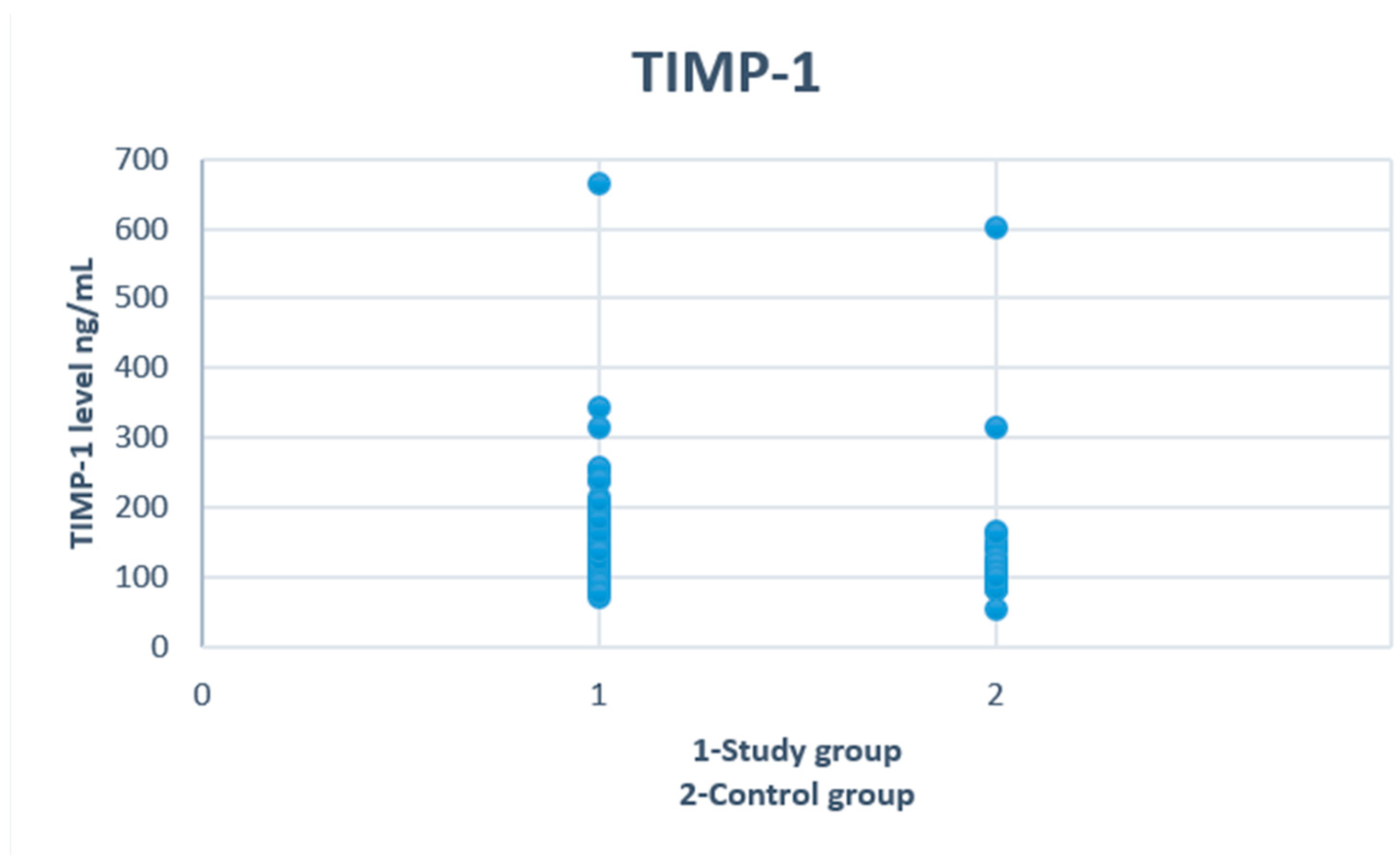
| TIMP-1 (ng/mL) | 153.4 (71.1–665.0) | 110.3 (54.0–601.0) | 0.007 * |
| MMP-9/TIMP-1 ratio | 0.5 (0.21–1.04) | 0.52 (0.22–1.15) | NS |
| Parameter | 12–15 Years (n = 30) | 16–17 Years (n = 27) | p |
|---|---|---|---|
| Alcohol (g/L) | 1.64 (0.48–3.26) | 2.06 (0.51–3.06) | 0.02 * |
| ALT (IU/L) | 13 (9–48) | 13 (7–38) | NS |
| AST (IU/L) | 21 (14–45) | 22 (15–35) | NS |
| Bilirubin (mg/dL) | 0.35 (0.15–1.49) | 0.32 (0.15–1.57) | NS |
| CK (IU/L) | 218 (88–923) | 193 (79–624) | NS |
| CK-MB (IU/L) | 21 (13–32) | 19 (11–55) | NS |
| Urea (mg/dL) | 23 (12–35) | 21 (10–36) | NS |
| PIIINP (ng/mL) | 27.74 (14,34–45.9) | 24.81 (19–48.42) | NS |
| Collagen IV (ng/mL) | 73.59 (40.72–121.1) | 67.59 (50.94–120.29) | NS |
| MMP-9 (ng/mL) | 69.2 (26.4–667.4) | 74.6 (39.8–355.4) | NS |
| TIMP-1 (ng/mL) | 134.55 (71.1–665) | 176.1 (96.6–342.8) | 0.03 * |
| MMP-9/TIMP-1 ratio | 0.57 (0.21–1) | 0.43 (0.21–1.04) | NS |
| Parameter | BAC < 1.78 (n = 28) | BAC ≥ 1.78 (n = 29) | p |
|---|---|---|---|
| Age (year) | 15 (12–17) | 16 (12–17) | NS |
| ALT (IU/L) | 13 (7–38) | 13 (8–48) | NS |
| AST (IU/L) | 22 (15–45) | 22 (14–42) | NS |
| Bilirubin (mg/dL) | 0.31 (0.15–1.49) | 0.33 (0.15–1.57) | NS |
| CK (IU/L) | 218 (88–923) | 202 (79–624) | NS |
| CK-MB (IU/L) | 20 (11–43) | 20 (13–55) | NS |
| Urea (mg/dL) | 23 (12–35) | 21 (10–36) | NS |
| PIIINP (ng/mL) | 25.66 (14.34–40.18) | 26.05 (18.3–48.42) | NS |
| Collagen IV (ng/mL) | 67.45 (40.72–104.32) | 69.77 (46.34–121.1) | NS |
| MMP-9 (ng/mL) | 69.2 (26.4–667.4) | 74.6 (39.8–205.2) | NS |
| TIMP-1 (ng/mL) | 148.8 (71.7–665) | 163.3 (83.6–253.8) | NS |
| MMP-9/TIMP-1 ratio | 0.59 (0.21–1) | 0.43 (0.21–1.04) | NS |
| PIIINP | Collagen IV | MMP-9 | TIMP-1 | MMP-9/TIMP-1 Ratio | |
|---|---|---|---|---|---|
| ALT | R = 0.28 p = 0.04 * | R = 0.34 p = 0.008 * | R = 0.38 p = 0.004 * | R = 0.47 p < 0.0001 * | R = 0.3; p = 0.02 * |
| AST | R = 0.42 p = 0.001 * | R = 0.42 p = 0.001 * | R = 0.23 p = 0.09 * | R = 0.29 p = 0.03 * | R = 0.3; p = 0.01 * |
| Total bilirubin | R = 0.44 p = 0.001 * | R = 0.44 p = 0.001 * | R = 0.39 p = 0.004 * | R = 0.32 p = 0.018 * | NS |
| CK | R = 0.3 p = 0.03 * | R = 0.3 p = 0.03 * | R = 0.24 p = 0.08 * | R = 0.28 p = 0.04 * | R = 0.38; p = 0.005 * |
| CK-MB | R = 0.33 p = 0.01 * | NS | NS | NS | R = 0.3; p = 0.03 * |
| Urea | R = 0.35 p = 0.008 * | R = 0.35 p = 0.008 * | NS | NS | R = 0.28; p = 0.04 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zdanowicz, K.; Kowalczuk-Kryston, M.; Olanski, W.; Werpachowska, I.; Mielech, W.; Lebensztejn, D.M. Increase in Serum MMP-9 and TIMP-1 Concentrations during Alcohol Intoxication in Adolescents—A Preliminary Study. Biomolecules 2022, 12, 710. https://doi.org/10.3390/biom12050710
Zdanowicz K, Kowalczuk-Kryston M, Olanski W, Werpachowska I, Mielech W, Lebensztejn DM. Increase in Serum MMP-9 and TIMP-1 Concentrations during Alcohol Intoxication in Adolescents—A Preliminary Study. Biomolecules. 2022; 12(5):710. https://doi.org/10.3390/biom12050710
Chicago/Turabian StyleZdanowicz, Katarzyna, Monika Kowalczuk-Kryston, Witold Olanski, Irena Werpachowska, Wlodzimierz Mielech, and Dariusz Marek Lebensztejn. 2022. "Increase in Serum MMP-9 and TIMP-1 Concentrations during Alcohol Intoxication in Adolescents—A Preliminary Study" Biomolecules 12, no. 5: 710. https://doi.org/10.3390/biom12050710
APA StyleZdanowicz, K., Kowalczuk-Kryston, M., Olanski, W., Werpachowska, I., Mielech, W., & Lebensztejn, D. M. (2022). Increase in Serum MMP-9 and TIMP-1 Concentrations during Alcohol Intoxication in Adolescents—A Preliminary Study. Biomolecules, 12(5), 710. https://doi.org/10.3390/biom12050710