Metallomics Analysis for Assessment of Toxic Metal Burdens in Infants/Children and Their Mothers: Early Assessment and Intervention Are Essential



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Sampling and Metal Analysis
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Harada, M. Minamata Disease: Methylmercury Poisoning in Japan Caused by Environmental Pollution. Crit. Rev. Toxicol. 1995, 25, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Silbergeld, E.K. Preventing lead poisoning in children. Annu. Rev. Public Health 1997, 18, 187–210. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, H.; Yoshida, K.; Yasuda, Y.; Tsutsui, T. Two age-related accumulation profiles of toxic metals. Curr. Aging Sci. 2012, 5, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, H.; Yasuda, Y.; Tsutsui, T. Estimation of autistic children by metallomics analysis. Sci. Rep. 2013, 3, srep01199. [Google Scholar] [CrossRef]
- Yasuda, H.; Tsutsui, T. Assessment of Infantile Mineral Imbalances in Autism Spectrum Disorders (ASDs). Int. J. Environ. Res. Public Health 2013, 10, 6027–6043. [Google Scholar] [CrossRef]
- Arora, M.; Reichenberg, A.; Willfors, C.; Austin, C.; Gennings, C.; Berggren, S.; Lichtenstein, P.; Anckarsäter, H.; Tammimies, K.; Bölte, S. Fetal and postnatal metal dysregulation in autism. Nat. Commun. 2017, 8, 15493. [Google Scholar] [CrossRef]
- Curtin, P.; Austin, C.; Curtin, A.; Gennings, C.; Arora, M.; Tammimies, K.; Willfors, C.; Berggren, S.; Siper, P.; Rai, D.; et al. Dynamical features in fetal and postnatal zinc-copper metabolic cycles predict the emergence of autism spectrum disorder. Sci. Adv. 2018, 4, eaat1293. [Google Scholar] [CrossRef]
- Fiore, M.; Barone, R.; Copat, C.; Grasso, A.; Cristaldi, A.; Rizzo, R.; Ferrante, M. Metal and essential element levels in hair and association with autism severity. J. Trace Elements Med. Biol. 2020, 57, 126409. [Google Scholar] [CrossRef]
- Cicero, C.E.; Mostile, G.; Vasta, R.; Rapisarda, V.; Signorelli, S.S.; Ferrante, M.; Zappia, M.; Nicoletti, A. Metals and neurodegenerative diseases. A systematic review. Environ. Res. 2017, 159, 82–94. [Google Scholar] [CrossRef]
- McLachlan, D.R.C.; Bergeron, C.; Alexandrov, P.N.; Walsh, W.J.; Pogue, A.I.; Percy, M.E.; Kruck, T.P.A.; Fang, Z.; Sharfman, N.M.; Jaber, V.; et al. Retraction Note: Aluminum in Neurological and Neurodegenerative Disease. Mol. Neurobiol. 2020, 57, 1779. [Google Scholar] [CrossRef]
- Gardner, R.M.; Kippler, M.; Tofail, F.; Bottai, M.; Hamadani, J.D.; Grandér, M.; Nermell, B.; Palm, B.; Rasmussen, K.M.; Vahter, M. Environmental Exposure to Metals and Children’s Growth to Age 5 Years: A Prospective Cohort Study. Am. J. Epidemiology 2013, 177, 1356–1367. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.; Chang, J.Y.; Hong, J.; Shin, S.; Park, J.S.; Oh, S. Low-Level Toxic Metal Exposure in Healthy Weaning-Age Infants: Association with Growth, Dietary Intake, and Iron Deficiency. Int. J. Environ. Res. Public Health 2017, 14, 388. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, H.; Yoshida, K.; Yasuda, Y.; Tsutsui, T. Infantile zinc deficiency: Association with autism spectrum disorders. Sci. Rep. 2011, 1, 129. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, H. Early assessment and intervention of mineral imbalances for autistic children. In Autism Spectrum Disorders; Valdez, A., Ed.; Nova Science Publishers: New York, NY, USA, 2013; pp. 27–49. [Google Scholar]
- Cusick, S.E.; Georgieff, M.K. The Role of Nutrition in Brain Development: The Golden Opportunity of the “First 1000 Days”. J. Pediatr. 2016, 175, 16–21. [Google Scholar] [CrossRef]
- Austin, C.; Curtin, P.; Curtin, A.; Gennings, C.; Arora, M.; Tammimies, K.; Isaksson, J.; Willfors, C.; Bölte, S. Dynamical properties of elemental metabolism distinguish attention deficit hyperactivity disorder from autism spectrum disorder. Transl. Psychiatry 2019, 9, 1–9. [Google Scholar] [CrossRef]
- Pfaender, S.; Sauer, A.K.; Hagmeyer, S.; Mangus, K.; Linta, L.; Liebau, S.; Bockmann, J.; Huguet, G.; Bourgeron, T.; Boeckers, T.M.; et al. Zinc deficiency and low enterocyte zinc transporter expression in human patients with autism related mutations in SHANK3. Sci. Rep. 2017, 7, 45190. [Google Scholar] [CrossRef]
- Ha, H.T.T.; Leal-Ortiz, S.; Lalwani, K.; Kiyonaka, S.; Hamachi, I.; Mysore, S.P.; Montgomery, J.M.; Garner, C.C.; Huguenard, J.R.; Kim, S.A. Shank and Zinc Mediate an AMPA Receptor Subunit Switch in Developing Neurons. Front. Mol. Neurosci. 2018, 11, 405. [Google Scholar] [CrossRef]
- Hagmeyer, S.; Sauer, A.K.; Grabrucker, A.M. Prospects of Zinc Supplementation in Autism Spectrum Disorders and Shankopathies Such as Phelan McDermid Syndrome. Front. Synaptic Neurosci. 2018, 10, 11. [Google Scholar] [CrossRef]
- Yasuda, H.; Tsutsui, T. Infants and elderlies are susceptible to zinc deficiency. Sci. Rep. 2016, 6, 21850. [Google Scholar] [CrossRef]
- Dufner-Beattie, J.; Wang, F.; Kuo, Y.-M.; Gitschier, J.; Eide, D.; Andrews, G.K. The Acrodermatitis Enteropathica GeneZIP4Encodes a Tissue-specific, Zinc-regulated Zinc Transporter in Mice. J. Biol. Chem. 2003, 278, 33474–33481. [Google Scholar] [CrossRef]
- Dufner-Beattie, J.; Kuo, Y.-M.; Gitschier, J.; Andrews, G.K. The Adaptive Response to Dietary Zinc in Mice Involves the Differential Cellular Localization and Zinc Regulation of the Zinc Transporters ZIP4 and ZIP5. J. Biol. Chem. 2004, 279, 49082–49090. [Google Scholar] [CrossRef] [PubMed]
- Cousins, R.J.; Liuzzi, J.P.; Lichten, L.A. Mammalian Zinc Transport, Trafficking, and Signals. J. Biol. Chem. 2006, 281, 24085–24089. [Google Scholar] [CrossRef]
- Lichten, L.A.; Cousins, R.J. Mammalian Zinc Transporters: Nutritional and Physiologic Regulation. Annu. Rev. Nutr. 2009, 29, 153–176. [Google Scholar] [CrossRef] [PubMed]
- Goyer, R.A. Toxic and essential metal interactions. Annu. Rev. Nutr. 1997, 17, 37–50. [Google Scholar] [CrossRef] [PubMed]
- Razagui, I.B.-A.; Ghribi, I. Maternal and Neonatal Scalp Hair Concentrations of Zinc, Copper, Cadmium, and Lead: Relationship to Some Lifestyle Factors. Biol. Trace Element Res. 2005, 106, 001–028. [Google Scholar] [CrossRef]
- Symanski, E.; Hertz-Picciotto, I. Blood Lead Levels in Relation to Menopause, Smoking, and Pregnancy History. Am. J. Epidemiol. 1995, 141, 1047–1058. [Google Scholar] [CrossRef]
- Gulson, B.; Jameson, C.; Mahaffey, K.; Mizon, K.; Korsch, M.; Vimpani, G. Pregnancy increases mobilization of lead from maternal skeleton. J. Lab. Clin. Med. 1997, 130, 51–62. [Google Scholar] [CrossRef]
- Exley, C.; Begum, A.; Woolley, M.P.; Bloor, R.N. Aluminum in Tobacco and Cannabis and Smoking-Related Disease. Am. J. Med. 2006, 119, 276.e9–276.e11. [Google Scholar] [CrossRef]
- Mutti, A.; Corradi, M.; Goldoni, M.; Vettori, M.V.; Bernard, A.; Apostoli, P. Exhaled Metallic Elements and Serum Pneumoproteins in Asymptomatic Smokers and Patients with COPD or Asthma. Chest 2006, 129, 1288–1297. [Google Scholar] [CrossRef]
- Serdar, M.; Akin, B.S.; Razi, C.; Akin, O.; Tokgoz, S.; Kenar, L.; Aykut, O. The Correlation between Smoking Status of Family Members and Concentrations of Toxic Trace Elements in the Hair of Children. Biol. Trace Element Res. 2012, 148, 11–17. [Google Scholar] [CrossRef]
- Unkiewicz-Winiarczyk, A.; Gromysz-Kałkowska, K.; Szubartowska, E. Aluminium, Cadmium and Lead Concentration in the Hair of Tobacco Smokers. Biol. Trace Element Res. 2009, 132, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Eklund, G.; Oskarsson, A. Exposure of cadmium from infant formulas and weaning foods. Food Addit. Contam. 1999, 16, 509–519. [Google Scholar] [CrossRef]
- Freundlich, M.; Abitbol, C.; Zilleruelo, G.; Strauss, J.; Faugere, M.-C.; Malluche, H. Infant formula as a cause of Aluminium toxicity in neonatal URAEMIA. Lancet 1985, 326, 527–529. [Google Scholar] [CrossRef]
- Fernandez-Lorenzo, J.R.; Cocho, J.A.; Rey-Goldar, M.L.; Couce, M.; Fraga, J.M. Aluminum Contents of Human Milk, Cow’s Milk, and Infant Formulas. J. Pediatr. Gastroenterol. Nutr. 1999, 28, 270–275. [Google Scholar] [CrossRef] [PubMed]
- Lyons-Weiler, J.; Ricketson, R. Reconsideration of the immunotherapeutic pediatric safe dose levels of aluminum. J. Trace Elements Med. Biol. 2018, 48, 67–73. [Google Scholar] [CrossRef]
- Exley, C. An aluminium adjuvant in a vaccine is an acute exposure to aluminium. J. Trace Elements Med. Biol. 2020, 57, 57–59. [Google Scholar] [CrossRef]
- Kodama, H. Trace Element Deficiency in Infants and Children: Clinical Practice. Jpn. Med. Assoc. J. 2004, 47, 376–381. [Google Scholar]
- Bölte, S.; Girdler, S.; Marschik, P.B. The contribution of environmental exposure to the etiology of autism spectrum disorder. Cell. Mol. Life Sci. 2019, 76, 1275–1297. [Google Scholar] [CrossRef]
- Masini, E.; Loi, E.; Vega-Benedetti, A.F.; Carta, M.; Doneddu, G.; Fadda, R.; Zavattari, P. An Overview of the Main Genetic, Epigenetic and Environmental Factors Involved in Autism Spectrum Disorder Focusing on Synaptic Activity. Int. J. Mol. Sci. 2020, 21, 8290. [Google Scholar] [CrossRef]
- Arnold, L.E.; Bozzolo, H.; Hollway, J.; Cook, A.; DiSilvestro, R.A.; Bozzolo, D.R.; Crowl, L.; Ramadan, Y.; Williams, C. Serum Zinc Correlates with Parent- and Teacher-Rated Inattention in Children with Attention-Deficit/Hyperactivity Disorder. J. Child Adolesc. Psychopharmacol. 2005, 15, 628–636. [Google Scholar] [CrossRef]
- Yorbik, O.; Ozdag, M.F.; Olgun, A.; Senol, M.G.; Bek, S.; Akman, S. Potential effects of zinc on information processing in boys with attention deficit hyperactivity disorder. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2008, 32, 662–667. [Google Scholar] [CrossRef] [PubMed]
- DiGirolamo, A.M.; Ramirez-Zea, M.; Wang, M.; Flores-Ayala, R.; Martorell, R.; Neufeld, L.M.; Ramakrishnan, U.; Sellen, D.; Black, M.M.; Stein, A.D. Randomized trial of the effect of zinc supplementation on the mental health of school-age children in Guatemala. Am. J. Clin. Nutr. 2010, 92, 1241–1250. [Google Scholar] [CrossRef] [PubMed]
- Akhondzadeh, S.; Mohammadi, M.R.; Khademi, M. Zinc sulfate as an adjunct to methylphenidate for the treatment of attention deficit hyperactivity disorder in children: A double blind and randomized trial [ISRCTN64132371]. BMC Psychiatry 2004, 4, 9. [Google Scholar] [CrossRef] [PubMed]
- Miyake, K.; Kawaguchi, A.; Miura, R.; Kobayashi, S.; Tran, N.Q.V.; Kobayashi, S.; Miyashita, C.; Araki, A.; Kubota, T.; Yamagata, Z.; et al. Association between DNA methylation in cord blood and maternal smoking: The Hokkaido Study on Environment and Children’s Health. Sci. Rep. 2018, 8, 5654. [Google Scholar] [CrossRef]
- Kozielec, T.; Starobrat-Hermelin, B. Assessment of magnesium levels in children with attention deficit hyperactivity disorder (ADHD). Magnes. Res. 1997, 10, 143–148. [Google Scholar]
- Starobrat-Hermelin, B.; Kozielec, T. The effects of magnesium physiological supplementation on hyperactivity in children with attention deficit hyperactivity disorder (ADHD). Positive response to magnesium oral loading test. Magnes. Res. 1997, 10, 149–156. [Google Scholar]
- Mousain-Bosc, M.; Roche, M.; Rapin, J.; Bali, J.-P. Magnesium VitB6 Intake Reduces Central Nervous System Hyperexcitability in Children. J. Am. Coll. Nutr. 2004, 23, 545S–548S. [Google Scholar] [CrossRef]
- Mousain-Bosc, M.; Roche, M.; Polge, A.; Pradal-Prat, D.; Rapin, J.; Bali, J. Improvement of neurobehavioral disorders in children supplemented with magnesium-vitamin B6. II. Pervasive developmental disorder-autism. Magnes. Res. 2006, 19, 53–62. [Google Scholar]
- Botturi, A.; Ciappolino, V.; DelVecchio, G.; Boscutti, A.; Viscardi, B.; Brambilla, P. The Role and the Effect of Magnesium in Mental Disorders: A Systematic Review. Nutrients 2020, 12, 1661. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Geometric Mean (ng/g) | ||||||
|---|---|---|---|---|---|---|
| Toxic Metal | Mother | Infant/Child | Maximum | In Infant/Child | ||
| (N = 77) | (N = 77) | (ng/g) | Ratio | |||
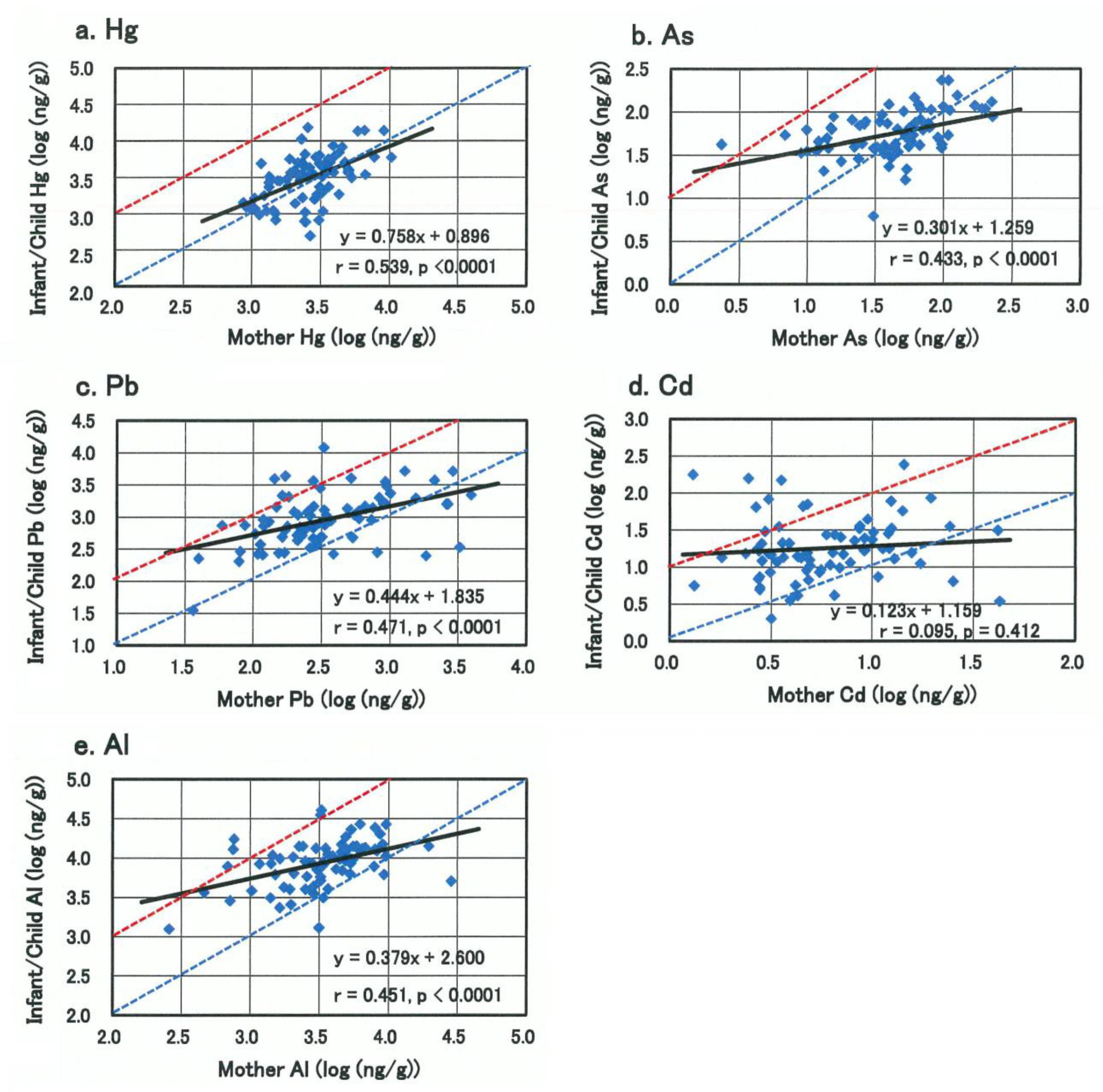
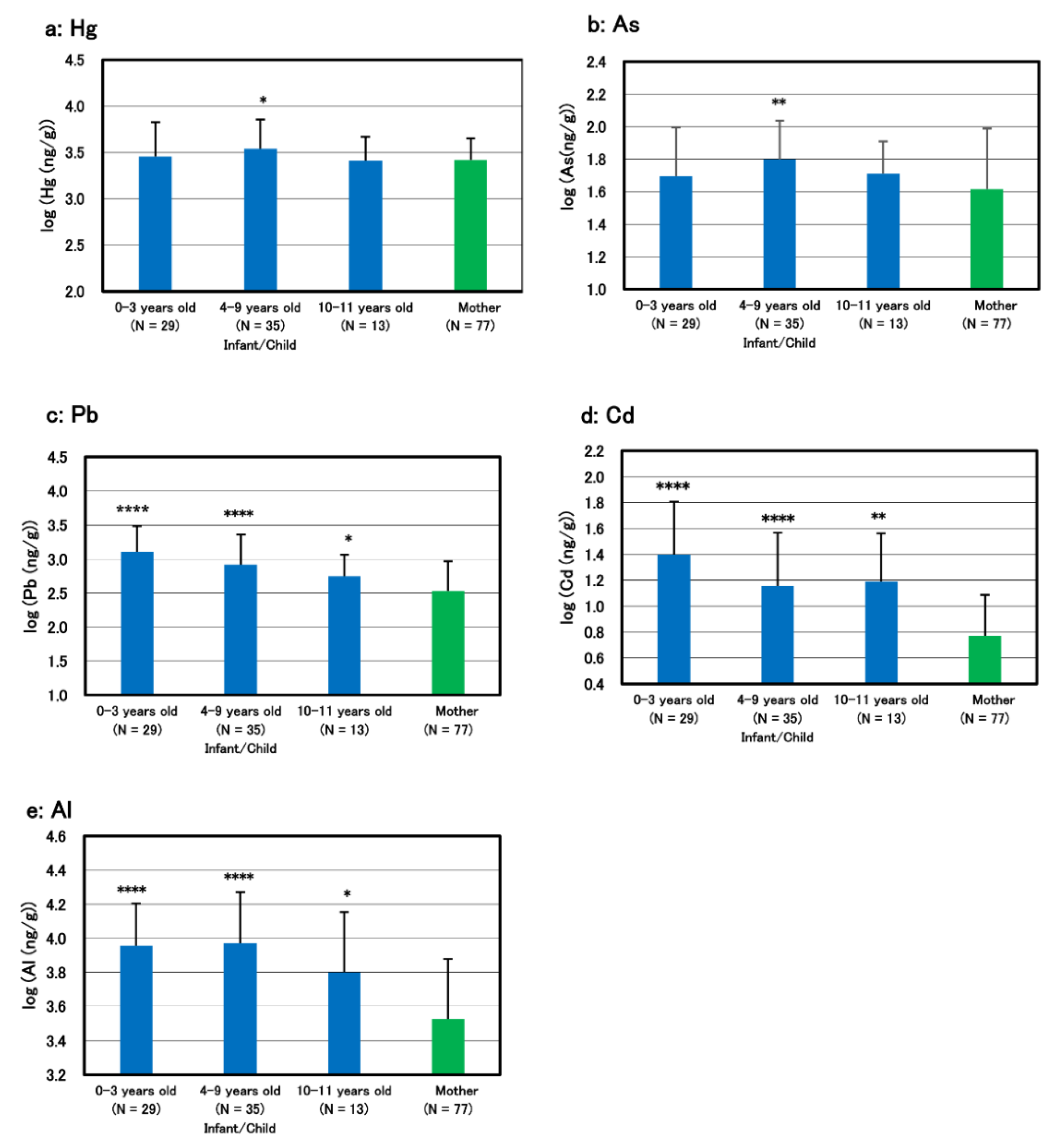
| Hg | 2621 | 3057 | 15,140 | 5.8 | (F 5) | |
| As | 41.2 | 55.5 | * | 233 | 5.7 | (M 4) |
| Pb | 338 | 907 | **** | 11,930 | 35.3 | (F 1) |
| Cd | 5.9 | 17.9 | **** | 241 | 40.8 | (M 2) |
| Al | 3362 | 8645 | **** | 40,740 | 12.1 | (M 2) |
| Geometric Mean (ng/g) | Deficient Infant/Child | ||||
|---|---|---|---|---|---|
| Essential Mineral | Mother | Infant/Child | Significance | No. | Rate |
| (N = 77) | (N = 77) | (%) | |||
| Na | 16,804 | 13,307 | NS | ||
| K | 10,542 | 17,976 | ** | ||
| Mg | 76,513 | 27,929 | **** | 9 | 11.7 |
| Ca | 710,404 | 294,933 | **** | 8 | 10.4 |
| P | 117,833 | 102,574 | NS | ||
| Se | 587 | 577 | NS | 0 | 0 |
| I | 196 | 404 | *** | 0 | 0 |
| Cr | 34.9 | 74.1 | **** | 2 | 2.6 |
| Mo | 33.1 | 59.1 | **** | 0 | 0 |
| Mn | 108 | 174 | *** | 0 | 0 |
| Fe | 4514 | 7922 | **** | 1 | 1.3 |
| Cu | 22,967 | 19,175 | NS | 0 | 0 |
| Zn | 135,620 | 97,139 | **** | 29 | 37.7 |
| Infant/Child | Mother | |||||
|---|---|---|---|---|---|---|
| Metal-Metal | (N = 77) | (N = 77) | ||||
| Correlation | Coefficient | p-Value | Coefficient | p-Value | ||
| Cd-Pb | 0.616 | 0.000 | **** | 0.438 | 0.000 | **** |
| Al-Pb | 0.347 | 0.002 | ** | 0.273 | 0.016 | * |
| Al-Fe | 0.601 | 0.000 | **** | 0.426 | 0.001 | *** |
| Pb-Zn | −0.267 | 0.019 | * | 0.139 | 0.227 | |
| As-Mg | −0.514 | 0.000 | **** | −0.649 | 0.000 | **** |
| Zn-Mo | −0.331 | 0.003 | ** | −0.183 | 0.112 | |
| Ca-Mg | 0.871 | 0.000 | **** | 0.820 | 0.000 | **** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yasuda, H.; Tsutsui, T.; Suzuki, K. Metallomics Analysis for Assessment of Toxic Metal Burdens in Infants/Children and Their Mothers: Early Assessment and Intervention Are Essential. Biomolecules 2021, 11, 6. https://doi.org/10.3390/biom11010006
Yasuda H, Tsutsui T, Suzuki K. Metallomics Analysis for Assessment of Toxic Metal Burdens in Infants/Children and Their Mothers: Early Assessment and Intervention Are Essential. Biomolecules. 2021; 11(1):6. https://doi.org/10.3390/biom11010006
Chicago/Turabian StyleYasuda, Hiroshi, Toyoharu Tsutsui, and Katsuhiko Suzuki. 2021. "Metallomics Analysis for Assessment of Toxic Metal Burdens in Infants/Children and Their Mothers: Early Assessment and Intervention Are Essential" Biomolecules 11, no. 1: 6. https://doi.org/10.3390/biom11010006
APA StyleYasuda, H., Tsutsui, T., & Suzuki, K. (2021). Metallomics Analysis for Assessment of Toxic Metal Burdens in Infants/Children and Their Mothers: Early Assessment and Intervention Are Essential. Biomolecules, 11(1), 6. https://doi.org/10.3390/biom11010006