
Salivary Tryptophan as a Metabolic Marker of HER2-Negative Molecular Subtypes of Breast Cancer



Abstract
1. Introduction
2. Materials and Methods
2.1. Description of the Study Group
2.2. Collection of Saliva Samples
2.3. Determination of Tryptophan in Saliva by Capillary Electrophoresis
2.4. Determination of the Expression of the Receptors for Estrogen, Progesterone, HER2 and Ki-67
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Youlden, D.R.; Cramb, S.M.; Dunn, N.A.M.; Muller, J.M.; Pyke, C.M.; Baade, P.D. The descriptive epidemiology of female breast cancer: An international comparison of screening, incidence, survival and mortality. Cancer Epidemiol. 2012, 36, 237–248. [Google Scholar] [CrossRef] [PubMed]
- Bel’skaya, L.V.; Sarf, E.A. «Salivaomics» of Different Molecular Biological Subtypes of Breast Cancer. Curr. Issues Mol. Biol. 2022, 44, 3053–3074. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Wang, H.; Luo, Y.; Tuo, B.; Liu, X.; Li, T. Effect of metabolism on the immune microenvironment of breast cancer. Biochim. Biophys. Acta Rev. Cancer 2023, 1878, 188861. [Google Scholar] [CrossRef]
- Lieu, E.L.; Nguyen, T.; Rhyne, S.; Kim, J. Amino acids in cancer. Exp. Mol. Med. 2020, 52, 15–30. [Google Scholar] [CrossRef]
- Lukey, M.J.; Katt, W.P.; Cerione, R.A. Targeting amino acid metabolism for cancer therapy. Drug Discov. Today 2017, 22, 796–804. [Google Scholar] [CrossRef]
- Zarate, L.V.; Miret, N.V.; Nicola Candia, A.J.; Zappia, C.D.; Pontillo, C.A.; Chiappini, F.A.; Monczor, F.; Candolfi, M.; Randi, A.S. Breast cancer progression and kynurenine pathway enzymes are induced by hexachlorobenzene exposure in a Her2-positive model. Food Chem. Toxicol. 2023, 177, 113822. [Google Scholar] [CrossRef]
- Xue, L.; Wang, C.; Qian, Y.; Zhu, W.; Liu, L.; Yang, X.; Zhang, S.; Luo, D. Tryptophan metabolism regulates inflammatory macrophage polarization as a predictive factor for breast cancer immunotherapy. Int. Immunopharmacol. 2023, 125, 111196. [Google Scholar] [CrossRef] [PubMed]
- Limón Pacheco, J.H.; Elizondo, G. Interplay between Estrogen, Kynurenine, and AHR Pathways: An immunosuppressive axis with therapeutic potential for breast cancer treatment. Biochem. Pharmacol. 2023, 217, 115804. [Google Scholar]
- Zhao, Y.; Pu, C.; Liu, Z. Essential amino acids deprivation is a potential strategy for breast cancer treatment. Breast 2022, 62, 152–161. [Google Scholar] [CrossRef]
- Huang, Z.; Yang, X.; Huang, Y.; Tang, Z.; Chen, Y.; Liu, H.; Huang, M.; Qing, L.; Li, L.; Wang, Q.; et al. Saliva—A new opportunity for fluid biopsy. Clin. Chem. Lab. Med. 2023, 61, 4–32. [Google Scholar] [CrossRef] [PubMed]
- Song, M.; Bai, H.; Zhang, P.; Zhou, X.; Ying, B. Promising applications of human-derived saliva biomarker testing in clinical diagnostics. Int. J. Oral Sci. 2023, 15, 2. [Google Scholar] [CrossRef] [PubMed]
- Khurshid, Z.; Warsi, I.; Moin, S.F.; Slowey, P.D.; Latif, M.; Zohaib, S.; Zafar, M.S. Biochemical analysis of oral fluids for disease detection. Adv. Clin. Chem. 2021, 100, 205–253. [Google Scholar] [PubMed]
- Meghnani, V.; Mohammed, N.; Giauque, C.; Nahire, R.; David, T. Performance characterization and validation of saliva as an alternative specimen source for detecting hereditary breast cancer mutations by next generation sequencing. Int. J. Genom. 2016, 2016, 2059041. [Google Scholar] [CrossRef] [PubMed]
- Nijakowski, K.; Zdrojewski, J.; Nowak, M.; Gruszczyński, D.; Knoll, F.; Surdacka, A. Salivary Metabolomics for Systemic Cancer Diagnosis: A Systematic Review. Metabolites 2023, 13, 28. [Google Scholar] [CrossRef] [PubMed]
- Kaczor-Urbanowicz, K.E.; Wei, F.; Rao, S.L.; Kim, J.; Shin, H.; Cheng, J.; Tu, M.; Wong, D.T.W.; Kim, Y. Clinical validity of saliva and novel technology for cancer detection. BBA Rev. Cancer 2019, 1872, 49–59. [Google Scholar] [CrossRef]
- Eftekhari, A.; Dizaj, S.M.; Sharifi, S.; Salatin, S.; Khalilov, R.; Samiei, M.; Vahed, S.Z.; Ahmadian, E. Salivary biomarkers in cancer. Adv. Clin. Chem. 2022, 110, 171–192. [Google Scholar] [PubMed]
- Bel’skaya, L.V.; Sarf, E.A.; Loginova, A.I. Diagnostic Value of Salivary Amino Acid Levels in Cancer. Metabolites 2023, 13, 950. [Google Scholar] [CrossRef]
- Bel’skaya, L.V.; Gundyrev, I.A.; Solomatin, D.V. The Role of Amino Acids in the Diagnosis, Risk Assessment, and Treatment of Breast Cancer: A Review. Curr. Issues Mol. Biol. 2023, 45, 7513–7537. [Google Scholar] [CrossRef]
- Sugimoto, M.; Wong, D.T.; Hirayama, A.; Soga, T.; Tomita, M. Capillary electrophoresis mass spectrometry-based saliva metabolomics identified oral, breast and pancreatic cancer-specific profiles. Metabolomics 2010, 6, 78–95. [Google Scholar] [CrossRef]
- Cheng, F.; Wang, Z.; Huang, Y.; Duan, Y.; Wang, X. Investigation of salivary free amino acid profile for early diagnosis of breast cancer with ultra-performance liquid chromatography-mass spectrometry. Clin. Chim. Acta 2015, 447, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Zhong, L.; Cheng, F.; Lu, X.; Duan, Y.; Wang, X. Untargeted saliva metabonomics study of breast cancer based on ultra-performance liquid chromatography coupled to mass spectrometry with HILIC and RPLC separations. Talanta 2016, 158, 351–360. [Google Scholar] [CrossRef]
- Murata, T.; Yanagisawa, T.; Kurihara, T.; Kaneko, M.; Ota, S.; Enomoto, A.; Tomita, M.; Sugimoto, M.; Sunamura, M.; Hayashida, T.; et al. Salivary metabolomics with alternative decision tree-based machine learning methods for breast cancer discrimination. Breast Cancer Res. Treat. 2019, 177, 591–601. [Google Scholar] [CrossRef] [PubMed]
- Bel’skaya, L.V.; Sarf, E.A. Application of the capillary electrophoresis method for the quantitative determination of tryptophan in the saliva of breast cancer patients. Klin. Lab. Diagn. Russ. Clin. Lab. Diagn. 2024, 69, 117–122. [Google Scholar]
- Ilić, I.R.; Stojanović, N.M.; Radulović, N.S.; Živković, V.V.; Randjelović, P.J.; Petrović, A.S.; Božić, M.; Ilić, R.S. The Quantitative ER Immunohistochemical Analysis in Breast Cancer: Detecting the 3 + 0, 4 + 0, and 5 + 0 Allred Score Cases. Medicina 2019, 55, 461. [Google Scholar] [CrossRef] [PubMed]
- Wolff, A.C.; Hammond, M.E.H.; Allison, K.H.; Harvey, B.E.; Mangu, P.B.; Bartlett, J.M.S.; Bilous, M.; Ellis, I.O.; Fitzgibbons, P.; Hanna, W.; et al. Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Focused Update. J. Clin. Oncol. 2018, 36, 2105–2122. [Google Scholar] [CrossRef] [PubMed]
- Stålhammar, G.; Robertson, S.; Wedlund, L.; Lippert, M.; Rantalainen, M.; Bergh, J.; Hartman, J. Digital image analysis of Ki67 in hot spots is superior to both manual Ki67 and mitotic counts in breast cancer. Histopathology 2018, 72, 974–989. [Google Scholar] [CrossRef]
- Agus, A.; Planchais, J.; Sokol, H. Gut microbiota regulation of tryptophan metabolism in health and disease. Cell Host Microbe 2018, 23, 716–724. [Google Scholar] [CrossRef]
- Zlatnik, E.Y.; Sagakyants, A.B.; Novikova, I.A.; Maksimov, A.Y.; Shatova, O.P.; Appolonova, S.A.; Moskaleva, N.E.; Rumyantsev, S.A.; Shestopalov, A.V. Metabolism of tryptophan in non-small lung cancer patients with different effect of PD-1/PD-L1 inhibitors immunotherapy. Uspekhi Mol. Onkol. Adv. Mol. Oncol. 2022, 9, 89–96. [Google Scholar] [CrossRef]
- Liu, X.-H.; Zhai, X.-Y. Role of tryptophan metabolism in cancers and therapeutic implications. Biochimie 2021, 182, 131–139. [Google Scholar] [CrossRef]
- Sarangi, P. Role of indoleamine 2, 3-dioxygenase 1 in immunosuppression of breast cancer. Cancer Pathogenesis and Therapy. 2023. [Google Scholar] [CrossRef]
- Platten, M.; Wick, W.; Van de Eynde, B.J. Tryptophan Catabolism in Cancer: Beyond IDO and Tryptophan Depletion. Cancer Res. 2012, 72, 5435–5440. [Google Scholar] [CrossRef] [PubMed]
- Ohshima, M.; Sugahara, K.; Kasahara, K.; Katakura, A. Metabolomic analysis of the saliva of Japanese patients with oral squamous cell carcinoma. Oncol. Rep. 2017, 37, 2727–2734. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Wen, X.; Li, Y.; Zhang, J.; Li, X.; Qian, C.; Tian, Y.; Ling, R.; Duan, Y. Diagnostic approach to thyroid cancer based on amino acid metabolomics in saliva by ultra-performance liquid chromatography with high resolution mass spectrometry. Talanta 2021, 235, 122729. [Google Scholar] [CrossRef] [PubMed]
- Ala, M. The footprint of the kynurenine pathway in every cancer: A new target for chemotherapy. Eur. J. Pharmacol. 2021, 896, 173921. [Google Scholar] [CrossRef] [PubMed]
- Arenas, M.; Fargas-Saladié, M.; Moreno-Solé, M.; Moyano-Femenia, L.; Jiménez-Franc, A.; Canela-Capdevila, M.; Castañé, H.; Martínez-Navidad, C.; Camps, J.; Joven, J. Metabolomics and triple-negative breast cancer: A systematic review. Heliyon 2023, 10, e23628. [Google Scholar] [CrossRef]
- Gong, S.; Wang, Q.; Huang, J.; Huang, R.; Chen, S.; Cheng, X.; Liu, L.; Dai, X.; Zhong, Y.; Fan, C.; et al. LC-MS/MS platform-based serum untargeted screening reveals the diagnostic biomarker panel and molecular mechanism of breast cancer. Methods 2024, 222, 100–111. [Google Scholar] [CrossRef]
- Li, Y.; Wang, M.; Zhao, L.; Liang, C.; Li, W. KYNU-related transcriptome profile and clinical outcome from 2994 breast tumors. Heliyon 2023, 9, e17216. [Google Scholar] [CrossRef]
- Heldring, N.; Pike, A.; Andersson, S.; Matthews, J.; Cheng, G.; Hartman, J.; Tujague, M.; Ström, A.; Treuter, E.; Warner, M.; et al. Estrogen receptors: How do they signal and what are their targets. Physiol. Rev. 2007, 87, 905–931. [Google Scholar] [CrossRef]
- Duffy, M.J.; Harbeck, N.; Nap, M.; Molina, R.; Nicolini, A.; Senkus, E.; Cardoso, F. Clinical use of biomarkers in breast cancer: Updated guidelines from the European Group on Tumor Markers (EGTM). Eur. J. Cancer 2017, 75, 284–298. [Google Scholar] [CrossRef]
- Meireson, A.; Devos, M.; Brochez, L. IDO Expression in Cancer: Different Compartment, Different Functionality? Front. Immunol. 2020, 11, 531491. [Google Scholar] [CrossRef] [PubMed]
- Wachowska, M.; Stachura, J.; Tonecka, K.; Fidyt, K.; Braniewska, A.; Sas, Z.; Kotula, I.; Rygiel, T.P.; Boon, L.; Golab, J.; et al. Inhibition of IDO leads to IL-6-dependent systemic inflammation in mice when combined with photodynamic therapy. Cancer Immunol. Immunother. 2020, 69, 1101–1112. [Google Scholar] [CrossRef] [PubMed]
- Safdarian, A.R.; Farhangnia, P.; Rezaei, N. Indoleamine 2,3-Dioxygenase (IDO) and Cancerous Cells. In Handbook of Cancer and Immunology; Rezaei, N., Ed.; Springer: Cham, Switzerland, 2023; pp. 1–23. [Google Scholar]
- Jovanovic, F.; Jovanovic, V.; Knezevic, N.N. Glucocorticoid Hormones as Modulators of the Kynurenine Pathway in Chronic Pain Conditions. Cells 2023, 12, 1178. [Google Scholar] [CrossRef] [PubMed]
- Nagy, B.; Szekeres-Barthó, J.; Kovács, G.L.; Sulyok, E.; Farkas, B.; Várnagy, Á.; Vértes, V.; Kovács, K.; Bódis, J. Key to Life: Physiological Role and Clinical Implications of Progesterone. Int. J. Mol. Sci. 2021, 22, 11039. [Google Scholar] [CrossRef] [PubMed]
- De Bie, J.; Lim, C.K.; Guillemin, G.J. Progesterone Alters Kynurenine Pathway Activation in IFN-Gamma-Activated Macrophages—Relevance for Neuroinflammatory Diseases. Int. J. Tryptophan. Res. 2016, 9, 89–93. [Google Scholar] [CrossRef] [PubMed]
- Songtachalert, T.; Roomruangwong, C.; Carvalho, A.F.; Bourin, M.; Maes, M. Anxiety Disorders: Sex Differences in Serotonin and Tryptophan Metabolism. Curr. Top. Med. Chem. 2018, 18, 1704–1715. [Google Scholar] [CrossRef]
- Badawy, A.A. Tryptophan metabolism, disposition and utilization in pregnancy. Biosci. Rep. 2015, 35, e00261. [Google Scholar] [CrossRef]
- Badawy, A.A.; Dougherty, D.M. Assessment of the Human Kynurenine Pathway: Comparisons and Clinical Implications of Ethnic and Gender Differences in Plasma Tryptophan, Kynurenine Metabolites, and Enzyme Expressions at Baseline and After Acute Tryptophan Loading and Depletion. Int. J. Tryptophan Res. 2016, 9, 31–49. [Google Scholar] [CrossRef] [PubMed]
- Barth, C.; Villringer, A.; Sacher, J. Sex hormones affect neurotransmitters and shape the adult female brain during hormonal transition periods. Front Neurosci. 2015, 9, 37. [Google Scholar] [CrossRef]
- Schenkels, L.C.P.M.; Veerman, E.C.I.; Nieuw Amerongen, A.V. Biochemical Composition of Human Saliva in Relation to Other Mucosal Fluids. Crit. Rev. Oral Biol. Med. 1995, 6, 161–175. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Feature | Breast Cancer, n = 103 | Trp, µg/L | p-Value | |
|---|---|---|---|---|
| Clinical Stage | ||||
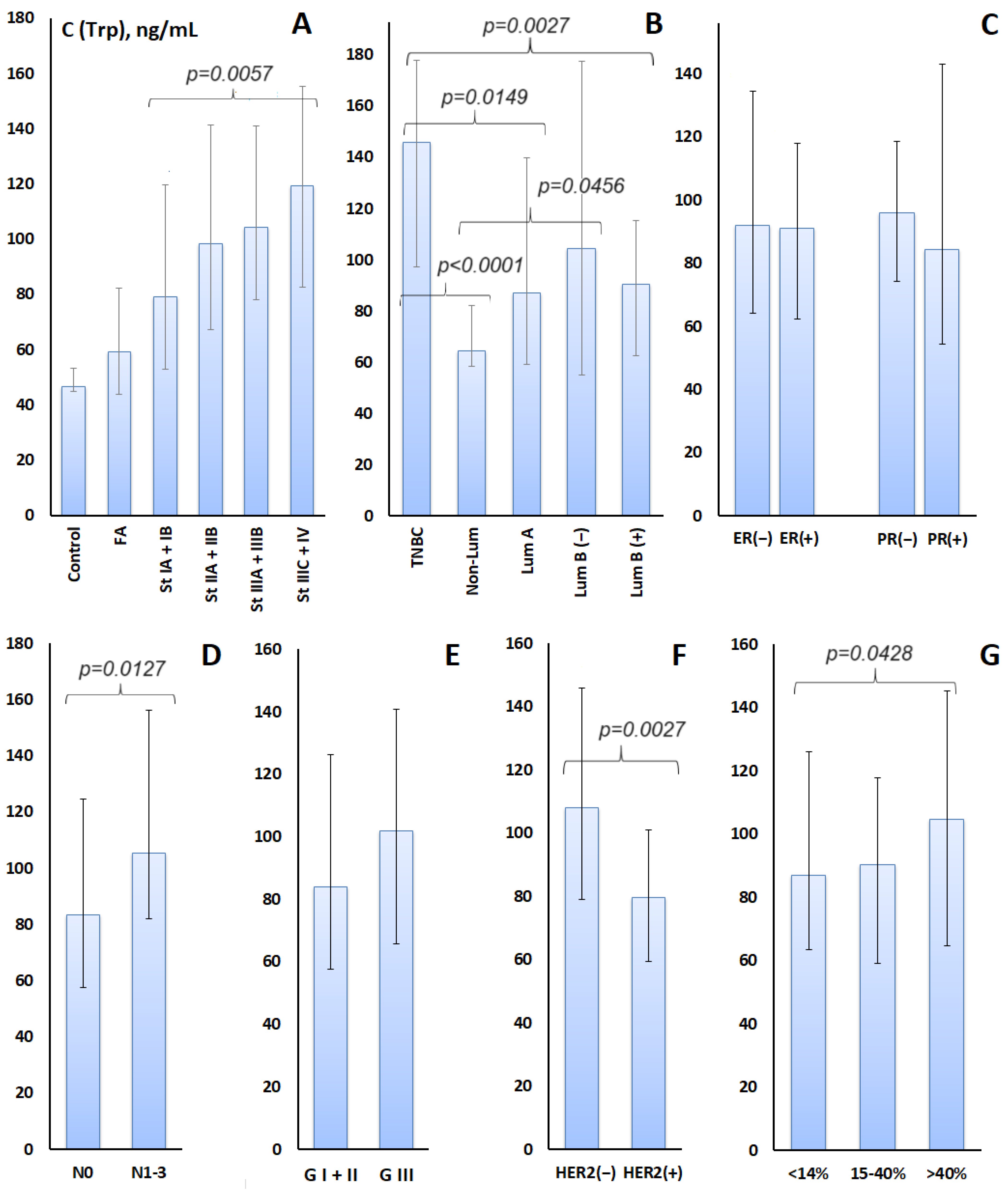
| Stage IA + IB | 33 (32.0%) | 79.09 [52.74; 139.7] | 0.1427 | |
| Stage IIA + 2B | 40 (38.8%) | 98.33 [67.10; 141.4] | 0.0055 * | |
| Stage IIIA + IIIB | 15 (14.6%) | 104.3 [78.06; 140.9] | 0.0284 | |
| Stage IIIC + IV | 15 (14.6%) | 119.1 [82.48; 175.3] | 0.0091 | |
| Lymph node status | ||||
| N0 | 58 (56.3%) | 83.50 [57.62; 124.7] | 0.0660 | |
| N1-3 | 45 (43.7%) | 105.2 [82.01; 176.3] | 0.0004 | |
| Subtype | ||||
| Luminal A-like | 22 (21.4%) | 87.01 [58.96; 139.7] | 0.0289 | |
| Luminal B-like (HER2+) | 21 (20.4%) | 90.58 [62.39; 115.3] | 0.1158 | |
| Luminal B-like (HER2−) | 24 (23.3%) | 104.3 [55.03; 177.3] | 0.0262 | |
| HER2-enriched (Non-Lum) | 16 (15.5%) | 64.57 [58.50; 81.97] | 0.6411 | |
| Triple-negative | 20 (19.4%) | 145.96 [97.18; 177.7] | 0.0001 | |
| HER2 status | ||||
| HER2-negative | 66 (64.1%) | 108.0 [78.98; 166.0] | 0.0005 | |
| HER2-positive | 37 (35.9%) | 79.43 [59.39; 101.9] | 0.2014 | |
| Estrogen (ER) status | ||||
| ER-negative | 38 (36.9%) | 91.86 [64.20; 154.6] | 0.0080 | |
| ER-positive | 65 (63.1%) | 90.98 [62.39; 137.9] | 0.0089 | |
| Progesterone (PR) status | ||||
| PR-negative | 68 (66.0%) | 95.93 [74.03; 138.6] | 0.0064 | |
| PR-positive | 35 (34.0%) | 84.08 [54.18; 162.8] | 0.0599 | |
| Degree of differentiation (G) | ||||
| G I + II | 51 (49.5%) | 83.92 [57.62; 146.1] | 0.0203 | |
| G III | 39 (37.8%) | 101.7 [65.50; 140.9] | 0.0083 | |
| Ki-67 | ||||
| <14% | 27 (26.2%) | 87.01 [63.46; 146.1] | 0.0127 | |
| 15–40% | 36 (35.0%) | 90.26 [59.17; 117.9] | 0.0627 | |
| >40% | 40 (38.8%) | 104.7 [64.57; 165.3] | 0.0037 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sarf, E.A.; Dyachenko, E.I.; Bel’skaya, L.V. Salivary Tryptophan as a Metabolic Marker of HER2-Negative Molecular Subtypes of Breast Cancer. Metabolites 2024, 14, 247. https://doi.org/10.3390/metabo14050247
Sarf EA, Dyachenko EI, Bel’skaya LV. Salivary Tryptophan as a Metabolic Marker of HER2-Negative Molecular Subtypes of Breast Cancer. Metabolites. 2024; 14(5):247. https://doi.org/10.3390/metabo14050247
Chicago/Turabian StyleSarf, Elena A., Elena I. Dyachenko, and Lyudmila V. Bel’skaya. 2024. "Salivary Tryptophan as a Metabolic Marker of HER2-Negative Molecular Subtypes of Breast Cancer" Metabolites 14, no. 5: 247. https://doi.org/10.3390/metabo14050247
APA StyleSarf, E. A., Dyachenko, E. I., & Bel’skaya, L. V. (2024). Salivary Tryptophan as a Metabolic Marker of HER2-Negative Molecular Subtypes of Breast Cancer. Metabolites, 14(5), 247. https://doi.org/10.3390/metabo14050247