
Effect of Sucrose on Amino Acid Absorption of Whey: A Randomized Crossover Trial


 ,
,
Abstract
:1. Introduction
2. Results
2.1. Plasma Total Amino Acid (TAA) Concentrations
2.2. Blood Glucose Levels
2.3. Plasma Insulin Levels
3. Discussion
4. Materials and Methods
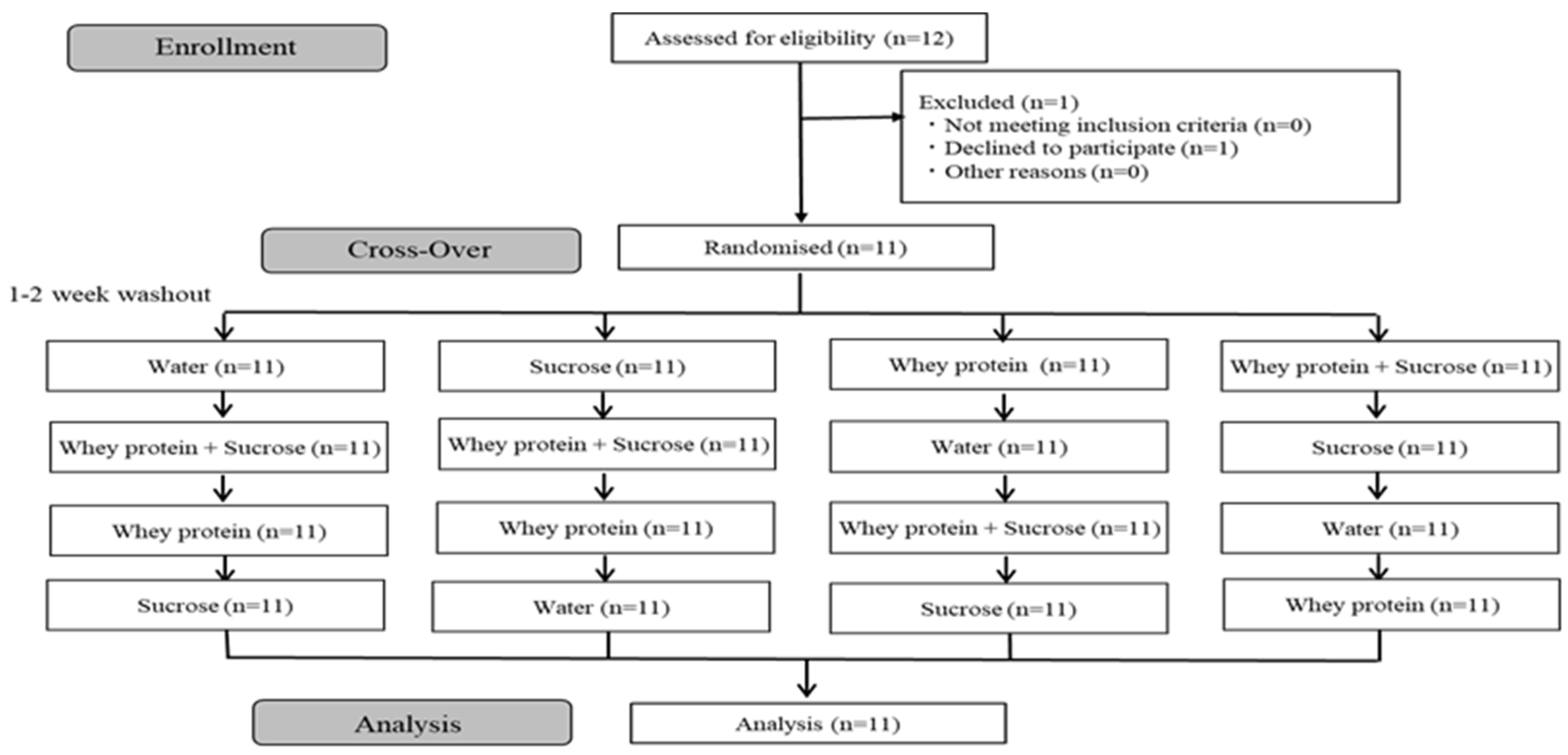
4.1. Study Design and Participants
- (1)
- Individuals for whom sucrose ingestion and/or whey protein solutions may adversely affect their health.
- (2)
- Individuals who had been hospitalized or were on medications.
- (3)
- Individuals with a history of serious hepatopathy, renal damage, cardiac disease, pulmonary disease, or blood disease.
- (4)
- Individuals who contracted or had a history of serious gastrointestinal disease.
- (5)
- Individuals with an addiction to alcohol or who were mentally unfit to provide informed consent.
- (6)
- Individuals who had used a therapeutic pharmaceutical drug within the preceding month.
- (7)
- Individuals exhibiting symptoms of probable seasonal allergy during the recruitment period. Specifically, this included allergies to Betulaceae (alder, oba alnus firma, shirakaba), Taxodiaceae (Cryptomeria spp., hinoki cypress), Asteraceae (ragweed, Artemisia vulgaris var. indica), and Gramineae (Dactylis glomerata, Phleum pratense).
- (8)
- Individuals with known severe food and drug allergies, for whom the possibility of a severe allergic reaction to sucrose and/or whey protein ingestion could not be excluded.
- (9)
- Individuals unable to consume milk or dairy products.
- (10)
- Individuals with severe anemia.
- (11)
- Individuals with high fasting blood glucose (>126 mg/dL).
- (12)
- Individuals who are smokers.
- (13)
- Females who are pregnant or lactating.
- (14)
- Individuals expecting a significant lifestyle change during the study period. (Long-term travel, late-night work, etc.)
- (15)
- Individuals who habitually ingested healthy foods and/or supplements within the preceding three months or expecting to do so during the study period.
- (16)
- Individuals who were hospitalized and had received medical treatment within the preceding six months.
- (17)
- Individuals who had participated in other clinical studies within the preceding month or expected to do so during the study period.
- (18)
- Individuals who are not healthy. (Including BMI > = 30 kg/m2 considering criteria of Japan Society for the Study of Obesity).
- (19)
- Individuals judged to be inappropriate for study inclusion by the principal investigator.
4.2. Experimental Protocols: Nutrient Supplementation and Blood Analysis
4.3. Preparation of Test Solutions
4.4. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Murakami, K.; Livingstone, M.B.E.; Sasaki, S. Meal-specific dietary patterns and their contribution to overall dietary patterns in the Japanese context: Findings from the 2012 National Health and Nutrition Survey, Japan. Nutrition 2019, 59, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Bohé, J.; Low, A.; Wolfe, R.R.; Rennie, M.J. Human muscle protein synthesis is modulated by extracellular, not intramuscular amino acid availability: A dose-response study. J. Physiol. 2003, 552, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Pitkanen, H.T.; Nykanen, T.; Knuutinen, J.; Lahti, K.; Keinanen, O.; Alen, M.; Komi, P.V.; Mero, A.A. Free amino acid pool and muscle protein balance after resistance exercise. Med. Sci. Sports Exerc. 2003, 35, 784–792. [Google Scholar] [CrossRef] [PubMed]
- Hulmi, J.J.; Lockwood, C.M.; Stout, J.R. Effect of protein/essential amino acids and resistance training on skeletal muscle hypertrophy: A case for whey protein. Nutr. Metab. 2010, 7, 51. [Google Scholar] [CrossRef] [Green Version]
- Pennings, B.; Groen, B.; de Lange, A.; Gijsen, A.P.; Zorenc, A.H.; Senden, J.M.; van Loon, L.J. Amino acid absorption and subsequent muscle protein accretion following graded intakes of whey protein in elderly men. Am. J. Physiol. Endocrinol. Metab. 2012, 302, E992–E999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buckley, J.D.; Thomson, R.L.; Coates, A.M.; Howe, P.R.; DeNichilo, M.O.; Rowney, M.K. Supplementation with a whey protein hydrolysate enhances recovery of muscle force-generating capacity following eccentric exercise. J. Sci. Med. Sport 2010, 13, 178–181. [Google Scholar] [CrossRef] [PubMed]
- Betts, J.A.; Stokes, K.A.; Toone, R.J.; Williams, C. Growth-hormone responses to consecutive exercise bouts with ingestion of carbohydrate plus protein. Int. J. Sport Nutr. Exerc. Metab. 2013, 23, 259–270. [Google Scholar] [CrossRef]
- Rustad, P.I.; Sailer, M.; Cumming, K.T.; Jeppesen, P.B.; Kolnes, K.J.; Sollie, O.; Franch, J.; Ivy, J.L.; Daniel, H.; Jensen, J. Intake of Protein Plus Carbohydrate during the First Two Hours after Exhaustive Cycling Improves Performance the following Day. PLoS ONE 2016, 11, e0153229. [Google Scholar] [CrossRef] [Green Version]
- Tagawa, R.; Watanabe, D.; Ito, K.; Ueda, K.; Nakayama, K.; Sanbongi, C.; Miyachi, M. Dose-response relationship between protein intake and muscle mass increase: A systematic review and meta-analysis of randomized controlled trials. Nutr. Rev. 2020, 79, 66–75. [Google Scholar] [CrossRef]
- Rantanen, T.; Guralnik, J.M.; Foley, D.; Masaki, K.; Leveille, S.; Curb, J.D.; White, L. Midlife hand grip strength as a predictor of old age disability. JAMA 1999, 281, 558–560. [Google Scholar] [CrossRef] [Green Version]
- Allerton, D.M.; Campbell, M.D.; Gonzalez, J.T.; Rumbold, P.L.; West, D.J.; Stevenson, E.J. Co-Ingestion of Whey Protein with a Carbohydrate-Rich Breakfast Does Not Affect Glycemia, Insulinemia or Subjective Appetite Following a Subsequent Meal in Healthy Males. Nutrients 2016, 8, 116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karamanlis, A.; Chaikomin, R.; Doran, S.; Bellon, M.; Bartholomeusz, F.D.; Wishart, J.M.; Jones, K.L.; Horowitz, M.; Rayner, C.K. Effects of protein on glycemic and incretin responses and gastric emptying after oral glucose in healthy subjects. Am. J. Clin. Nutr. 2007, 86, 1364–1368. [Google Scholar] [CrossRef] [PubMed]
- Kawai, K.; Murayama, Y.; Okuda, Y.; Yamashita, K. Postprandial glucose, insulin and glucagon responses to meals with different nutrient compositions in non-insulin-dependent diabetes mellitus. Endocrinol. Jpn. 1987, 34, 745–753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujita, S.; Rasmussen, B.B.; Cadenas, J.G.; Grady, J.J.; Volpi, E. Effect of insulin on human skeletal muscle protein synthesis is modulated by insulin-induced changes in muscle blood flow and amino acid availability. Am. J. Physiol. Endocrinol. Metab. 2006, 291, E745–E754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boden, G.; Rezvani, I.; Owen, O.E. Effects of glucagon on plasma amino acids. J. Clin. Investig. 1984, 73, 785–793. [Google Scholar] [CrossRef] [Green Version]
- Hayashi, Y.; Seino, Y. Regulation of amino acid metabolism and α-cell proliferation by glucagon. J. Diabetes Investig. 2018, 9, 464–472. [Google Scholar] [CrossRef]
- Adeva-Andany, M.M.; Funcasta-Calderón, R.; Fernández-Fernández, C.; Castro-Quintela, E.; Carneiro-Freire, N. Metabolic effects of glucagon in humans. J. Clin. Transl. Endocrinol. 2019, 15, 45–53. [Google Scholar] [CrossRef]
- Gunnerud, U.J.; Ostman, E.M.; Björck, I.M. Effects of whey proteins on glycaemia and insulinaemia to an oral glucose load in healthy adults; a dose-response study. Eur. J. Clin. Nutr. 2013, 67, 749–753. [Google Scholar] [CrossRef]
- King, D.G.; Walker, M.; Campbell, M.D.; Breen, L.; Stevenson, E.J.; West, D.J. A small dose of whey protein co-ingested with mixed-macronutrient breakfast and lunch meals improves postprandial glycemia and suppresses appetite in men with type 2 diabetes: A randomized controlled trial. Am. J. Clin. Nutr. 2018, 107, 550–557. [Google Scholar] [CrossRef]
- Ceriello, A.; Esposito, K.; Piconi, L.; Ihnat, M.A.; Thorpe, J.E.; Testa, R.; Boemi, M.; Giugliano, D. Oscillating glucose is more deleterious to endothelial function and oxidative stress than mean glucose in normal and type 2 diabetic patients. Diabetes 2008, 57, 1349–1354. [Google Scholar] [CrossRef] [Green Version]
- Monnier, L.; Mas, E.; Ginet, C.; Michel, F.; Villon, L.; Cristol, J.P.; Colette, C. Activation of oxidative stress by acute glucose fluctuations compared with sustained chronic hyperglycemia in patients with type 2 diabetes. JAMA 2006, 295, 1681–1687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindgren, O.; Pacini, G.; Tura, A.; Holst, J.J.; Deacon, C.F.; Ahrén, B. Incretin effect after oral amino acid ingestion in humans. J. Clin. Endocrinol. Metab. 2015, 100, 1172–1176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frid, A.H.; Nilsson, M.; Holst, J.J.; Björck, I.M. Effect of whey on blood glucose and insulin responses to composite breakfast and lunch meals in type 2 diabetic subjects. Am. J. Clin. Nutr. 2005, 82, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Vangsoe, M.T.; Thogersen, R.; Bertram, H.C.; Heckmann, L.L.; Hansen, M. Ingestion of Insect Protein Isolate Enhances Blood Amino Acid Concentrations Similar to Soy Protein in A Human Trial. Nutrients 2018, 10, 1357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WatersInc. Available online: https://www.waters.com/waters/library.htm?cid=511436&lid=134965704&locale=ja_JP (accessed on 9 November 2020).




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| W-Group | W-S-Group | p-Value | |
|---|---|---|---|
| Tmax (min) | 46.36 ± 7.42 | 43.64 ± 4.72 | 0.68 |
| AUC (µmol/L) | 78,619.74 ± 13,126.47 | 66,724.72 ± 18,564.73 | 0.66 |
| (a) | ||||
| Amino Acid | g/100 g | |||
| Arginine | 2.00 | |||
| Lysine | 6.13 | |||
| Histidine | 1.42 | |||
| Phenylalanine | 2.53 | |||
| Tyrosine | 2.51 | |||
| Leucine | 8.77 | |||
| Isoleucine | 5.28 | |||
| Methionine | 1.74 | |||
| Valine | 4.75 | |||
| Alanine | 4.47 | |||
| Glycine | 1.41 | |||
| Proline | 4.47 | |||
| Glutamic acid | 14.50 | |||
| Serine | 4.26 | |||
| Aspartic acid | 8.71 | |||
| Cysteine | 2.05 | |||
| Threonine | 5.84 | |||
| Tryptophan | 1.49 | |||
| (b) | ||||
| Per Test Solutions | P-Group | W-Group | S-Group | W-S-Group |
| Energy (kcal) | 0.00 | 46.80 | 40.00 | 86.80 |
| Protein (g) | 0.00 | 10.00 | 0.00 | 10.00 |
| Fat (g) | 0.00 | 0.75 | 0.00 | 0.75 |
| Carbohydrate (g) | 0.00 | 0.00 | 10.00 | 10.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wajiki, M.; Yamamoto, T.; Maruki-Uchida, H.; Nagashima, H.; Shimizu, T.; Morita, M. Effect of Sucrose on Amino Acid Absorption of Whey: A Randomized Crossover Trial. Metabolites 2022, 12, 282. https://doi.org/10.3390/metabo12040282
Wajiki M, Yamamoto T, Maruki-Uchida H, Nagashima H, Shimizu T, Morita M. Effect of Sucrose on Amino Acid Absorption of Whey: A Randomized Crossover Trial. Metabolites. 2022; 12(4):282. https://doi.org/10.3390/metabo12040282
Chicago/Turabian StyleWajiki, Mai, Takayuki Yamamoto, Hiroko Maruki-Uchida, Hirotaka Nagashima, Tetsu Shimizu, and Minoru Morita. 2022. "Effect of Sucrose on Amino Acid Absorption of Whey: A Randomized Crossover Trial" Metabolites 12, no. 4: 282. https://doi.org/10.3390/metabo12040282
APA StyleWajiki, M., Yamamoto, T., Maruki-Uchida, H., Nagashima, H., Shimizu, T., & Morita, M. (2022). Effect of Sucrose on Amino Acid Absorption of Whey: A Randomized Crossover Trial. Metabolites, 12(4), 282. https://doi.org/10.3390/metabo12040282