
Lipid Profiles of Human Serum Fractions Enhanced with CD9 Antibody-Immobilized Magnetic Beads

 , ,
, , 
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Reagents
4.2. Serum Samples
4.3. Preparation of CD9 Antibody- and IgG-Immobilized Magnetic Beads
4.4. Serum Enrichment with CD9 Antibody and IgG-Immobilized Magnetic Beads
4.5. Liquid Chromatography/Mass Spectrometry Measurements
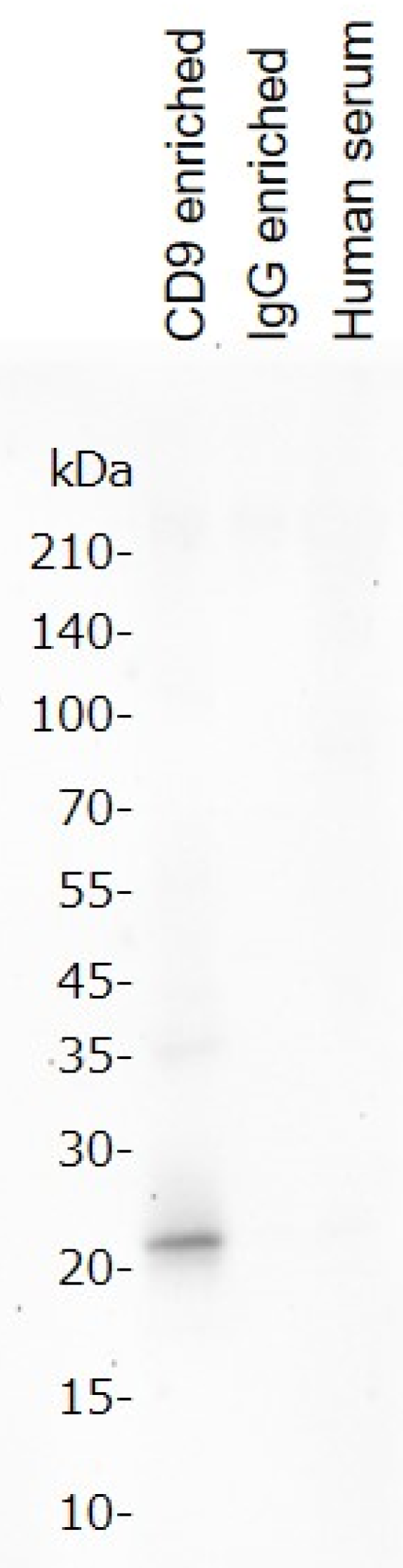
4.6. Western Blot
4.7. LDL/HDL Assay
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Han, X. Lipidomics for studying metabolism. Nat. Rev. Endocrinol. 2016, 12, 668–679. [Google Scholar] [CrossRef] [PubMed]
- Yang, K.; Han, X. Lipidomics: Techniques, Applications, and Outcomes Related to Biomedical Sciences. Trends Biochem. Sci. 2016, 41, 954–969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avela, H.F.; Sirén, H. Advances in lipidomics. Clin. Chim. Acta 2020, 510, 123–141. [Google Scholar] [CrossRef] [PubMed]
- Mayeux, R. Biomarkers: Potential Uses and Limitations. NeuroRx 2004, 1, 182–188. [Google Scholar] [CrossRef]
- Ishikawa, M.; Maekawa, K.; Saito, K.; Senoo, Y.; Urata, M.; Murayama, M.; Tajima, Y.; Kumagai, Y.; Saito, Y. Plasma and serum lipidomics of healthy white adults shows characteristic profiles by subjects’ gender and age. PLoS ONE 2014, 9, e91806. [Google Scholar] [CrossRef] [Green Version]
- Guerra, I.M.S.; Ferreira, H.B.; Neves, B.; Melo, T.; Diogo, L.M.; Domingues, M.R.; Moreira, A.S.P. Lipids and phenylketonuria: Current evidences pointed the need for lipidomics studies. Arch. Biochem. Biophys. 2020, 688, 108431. [Google Scholar] [CrossRef]
- Lanzon, B.; Martin-Taboada, M.; Castro-Alves, V.; Vila-Bedmar, R.; González de Pablos, I.; Duberg, D.; Gomez, P.; Rodriguez, E.; Orešič, M.; Hyötyläinen, T.; et al. Lipidomic and Metabolomic Signature of Progression of Chronic Kidney Disease in Patients with Severe Obesity. Metabolites 2021, 11, 836. [Google Scholar] [CrossRef]
- Schmelter, F.; Föh, B.; Mallagaray, A.; Rahmöller, J.; Ehlers, M.; Lehrian, S.; von Kopylow, V.; Künsting, I.; Lixenfeld, A.S.; Martin, E.; et al. Metabolic and Lipidomic Markers Differentiate COVID-19 From Non-Hospitalized and Other Intensive Care Patients. Front. Mol. Biosci. 2021, 8, 1091. [Google Scholar] [CrossRef]
- Minamoto, T.; Parambeth, J.C.; Walzem, R.L.; Payne, H.R.; Lidbury, J.A.; Suchodolski, J.S.; Steiner, J.M. Evaluation of density gradient ultracentrifugation serum lipoprotein profiles in healthy dogs and dogs with exocrine pancreatic insufficiency. J. Vet. Diagn. Investig. 2018, 30, 878–886. [Google Scholar] [CrossRef]
- Brennan, K.; Martin, K.; FitzGerald, S.P.; O’Sullivan, J.; Wu, Y.; Blanco, A.; Richardson, C.; Mc Gee, M.M. A comparison of methods for the isolation and separation of extracellular vesicles from protein and lipid particles in human serum. Sci. Rep. 2020, 10, 1039. [Google Scholar] [CrossRef] [Green Version]
- Fredolini, C.; Byström, S.; Sanchez-Rivera, L.; Ioannou, M.; Tamburro, D.; Pontén, F.; Branca, R.M.; Nilsson, P.; Lehtiö, J.; Schwenk, J.M. Systematic assessment of antibody selectivity in plasma based on a resource of enrichment profiles. Sci. Rep. 2019, 9, 8324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sivertsson, Å.; Lindström, E.; Oksvold, P.; Katona, B.; Hikmet, F.; Vuu, J.; Gustavsson, J.; Sjöstedt, E.; Von Feilitzen, K.; Kampf, C.; et al. Enhanced Validation of Antibodies Enables the Discovery of Missing Proteins. J. Proteome Res. 2020, 19, 4766–4781. [Google Scholar] [CrossRef] [PubMed]
- Iglesias, M.J.; Kruse, L.D.; Sanchez-Rivera, L.; Enge, L.; Dusart, P.; Hong, M.G.; Uhlén, M.; Renné, T.; Schwenk, J.M.; Bergstrom, G.; et al. Identification of Endothelial Proteins in Plasma Associated With Cardiovascular Risk Factors. Arterioscler. Thromb. Vasc. Biol. 2021, 41, 2990–3004. [Google Scholar] [CrossRef] [PubMed]
- Brzozowski, J.S.; Bond, D.R.; Jankowski, H.; Goldie, B.J.; Burchell, R.; Naudin, C.; Smith, N.D.; Scarlett, C.J.; Larsen, M.R.; Dun, M.D.; et al. Extracellular vesicles with altered tetraspanin CD9 and CD151 levels confer increased prostate cell motility and invasion. Sci. Rep. 2018, 8, 8822. [Google Scholar] [CrossRef] [Green Version]
- Higashihara, M.; Takahata, K.; Yatomi, Y.; Nakahara, K.; Kurokawa, K. Purification and partial characterization of CD9 antigen of human platelets. FEBS Lett. 1990, 264, 270–274. [Google Scholar] [CrossRef] [Green Version]
- Jennings, L.K.; Crossno, J.T.; Fox, C.F.; White, M.M.; Green, C.A. Platelet p24/CD9, a Member of the Tetraspanin Family of Proteins. Ann. N. Y. Acad. Sci. 1994, 714, 175–184. [Google Scholar] [CrossRef]
- Ozaki, Y.; Satoh, K.; Kuroda, K.; Qi, R.; Yatomi, Y.; Yanagi, S.; Sada, K.; Yamamura, H.; Yanabu, M.; Nomura, S.; et al. Anti-CD9 monoclonal antibody activates p72syk in human platelets. J. Biol. Chem. 1995, 270, 15119–15124. [Google Scholar] [CrossRef] [Green Version]
- Reyes, R.; Cardeñes, B.; Machado-Pineda, Y.; Cabañas, C. Tetraspanin CD9: A key regulator of cell adhesion in the immune system. Front. Immunol. 2018, 9, 863. [Google Scholar] [CrossRef]
- Brosseau, C.; Colas, L.; Magnan, A.; Brouard, S. CD9 tetraspanin: A new pathway for the regulation of inflammation? Front. Immunol. 2018, 9, 2316. [Google Scholar] [CrossRef] [Green Version]
- Sarafian, M.H.; Gaudin, M.; Lewis, M.R.; Martin, F.P.; Holmes, E.; Nicholson, J.K.; Dumas, M.E. Objective set of criteria for optimization of sample preparation procedures for ultra-high throughput untargeted blood plasma lipid profiling by ultra performance liquid chromatography-mass spectrometry. Anal. Chem. 2014, 86, 5766–5774. [Google Scholar] [CrossRef]
- Satomi, Y.; Hirayama, M.; Kobayashi, H. One-step lipid extraction for plasma lipidomics analysis by liquid chromatography mass spectrometry. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2017, 1063, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Umeda, R.; Satouh, Y.; Takemoto, M.; Nakada-Nakura, Y.; Liu, K.; Yokoyama, T.; Shirouzu, M.; Iwata, S.; Nomura, N.; Sato, K.; et al. Structural insights into tetraspanin CD9 function. Nat. Commun. 2020, 11, 1606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suárez, H.; Andreu, Z.; Mazzeo, C.; Toribio, V.; Pérez-Rivera, A.E.; López-Martín, S.; García-Silva, S.; Hurtado, B.; Morato, E.; Peláez, L.; et al. CD9 inhibition reveals a functional connection of extracellular vesicle secretion with mitophagy in melanoma cells. J. Extracell. Vesicles 2021, 10, e12082. [Google Scholar] [CrossRef] [PubMed]
- Wood, P.L.; Cebak, J.E. Lipidomics biomarker studies: Errors, limitations, and the future. Biochem. Biophys. Res. Commun. 2018, 504, 569–575. [Google Scholar] [CrossRef] [PubMed]
- Izumi, Y.; Matsuda, F.; Hirayama, A.; Ikeda, K.; Kita, Y.; Horie, K.; Saigusa, D.; Saito, K.; Sawada, Y.; Nakanishi, H.; et al. Inter-laboratory comparison of metabolite measurements for metabolomics data integration. Metabolites 2019, 9, 257. [Google Scholar] [CrossRef] [Green Version]
- Züllig, T.; Trötzmüller, M.; Köfeler, H.C. Lipidomics from sample preparation to data analysis: A primer. Anal. Bioanal. Chem. 2020, 412, 2191–2209. [Google Scholar] [CrossRef] [Green Version]
- Bowden, J.A.; Heckert, A.; Ulmer, C.Z.; Jones, C.M.; Koelmel, J.P.; Abdullah, L.; Ahonen, L.; Alnouti, Y.; Armando, A.M.; Asara, J.M.; et al. Harmonizing lipidomics: NIST interlaboratory comparison exercise for lipidomics using SRM 1950–Metabolites in Frozen Human Plasma. J. Lipid Res. 2017, 58, 2275–2288. [Google Scholar] [CrossRef] [Green Version]
- Li, S.; Park, Y.; Duraisingham, S.; Strobel, F.H.; Khan, N.; Soltow, Q.A.; Jones, D.P.; Pulendran, B. Predicting Network Activity from High Throughput Metabolomics. PLoS Comput. Biol. 2013, 9, e1003123. [Google Scholar] [CrossRef] [Green Version]
- Quell, J.D.; Römisch-Margl, W.; Colombo, M.; Krumsiek, J.; Evans, A.M.; Mohney, R.; Salomaa, V.; de Faire, U.; Groop, L.C.; Agakov, F.; et al. Automated pathway and reaction prediction facilitates in silico identification of unknown metabolites in human cohort studies. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2017, 1071, 58–67. [Google Scholar] [CrossRef] [Green Version]
- Cai, Q.; Alvarez, J.A.; Kang, J.; Yu, T. Network Marker Selection for Untargeted LC-MS Metabolomics Data. J. Proteome Res. 2017, 16, 1261–1269. [Google Scholar] [CrossRef] [Green Version]
- Basu, S.; Duren, W.; Evans, C.R.; Burant, C.F.; Michailidis, G.; Karnovsky, A. Sparse network modeling and metscape-based visualization methods for the analysis of large-scale metabolomics data. Bioinformatics 2017, 33, 1545–1553. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Disease | Group | Age | Female | Male |
|---|---|---|---|---|
| Alzheimer’s disease (Average age: 74.6) | Alzheimer’s 1 | 75.3 | 2 | 4 |
| Alzheimer’s 2 | 70.5 | 2 | 4 | |
| Alzheimer’s 3 | 76.8 | 5 | 1 | |
| Major depression (Average age: 74.6) | Depression 1 | 68.8 | 2 | 4 |
| Depression 2 | 76.7 | 3 | 3 | |
| Depression 3 | 78.3 | 5 | 1 | |
| Parkinson’s disease (Average age: 73.8) | Parkinson’s 1 | 74.3 | 4 | 2 |
| Parkinson’s 2 | 73.7 | 3 | 3 | |
| Parkinson’s 3 | 73.3 | 2 | 4 | |
| Schizophrenia (Average age: 72.2) | Schizophrenia 1 | 72.5 | 3 | 3 |
| Schizophrenia 2 | 73.3 | 3 | 3 | |
| Schizophrenia 3 | 70.7 | 2 | 4 | |
| Stroke (Average age: 74.7) | Stroke 1 | 75.5 | 4 | 2 |
| Stroke 2 | 72.2 | 1 | 5 | |
| Stroke 3 | 76.5 | 3 | 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tokuoka, S.M.; Kita, Y.; Sato, M.; Shimizu, T.; Yatomi, Y.; Oda, Y. Lipid Profiles of Human Serum Fractions Enhanced with CD9 Antibody-Immobilized Magnetic Beads. Metabolites 2022, 12, 230. https://doi.org/10.3390/metabo12030230
Tokuoka SM, Kita Y, Sato M, Shimizu T, Yatomi Y, Oda Y. Lipid Profiles of Human Serum Fractions Enhanced with CD9 Antibody-Immobilized Magnetic Beads. Metabolites. 2022; 12(3):230. https://doi.org/10.3390/metabo12030230
Chicago/Turabian StyleTokuoka, Suzumi M., Yoshihiro Kita, Masaya Sato, Takao Shimizu, Yutaka Yatomi, and Yoshiya Oda. 2022. "Lipid Profiles of Human Serum Fractions Enhanced with CD9 Antibody-Immobilized Magnetic Beads" Metabolites 12, no. 3: 230. https://doi.org/10.3390/metabo12030230
APA StyleTokuoka, S. M., Kita, Y., Sato, M., Shimizu, T., Yatomi, Y., & Oda, Y. (2022). Lipid Profiles of Human Serum Fractions Enhanced with CD9 Antibody-Immobilized Magnetic Beads. Metabolites, 12(3), 230. https://doi.org/10.3390/metabo12030230