
Mucoadhesive Vaginal Tablets Containing Metronidazole: Screening of Optimal Natural Polymer in the Composition

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Tablets Formulation
2.2. Quality Assessment of Prepared Tablets
2.2.1. Uniformity of Mass
2.2.2. Resistance to Crushing
2.2.3. Friability
2.2.4. Mucoadhesive Strength
2.2.5. Swelling Capacity
2.2.6. In Vitro Drug Release
2.2.7. In Vitro Drug Release Kinetics
2.2.8. Characterization of Morphological Changes in Swollen Tablets by SEM
2.2.9. Statistical Analysis
3. Results
3.1. Uniformity of Mass
3.2. Resistance to Crushing
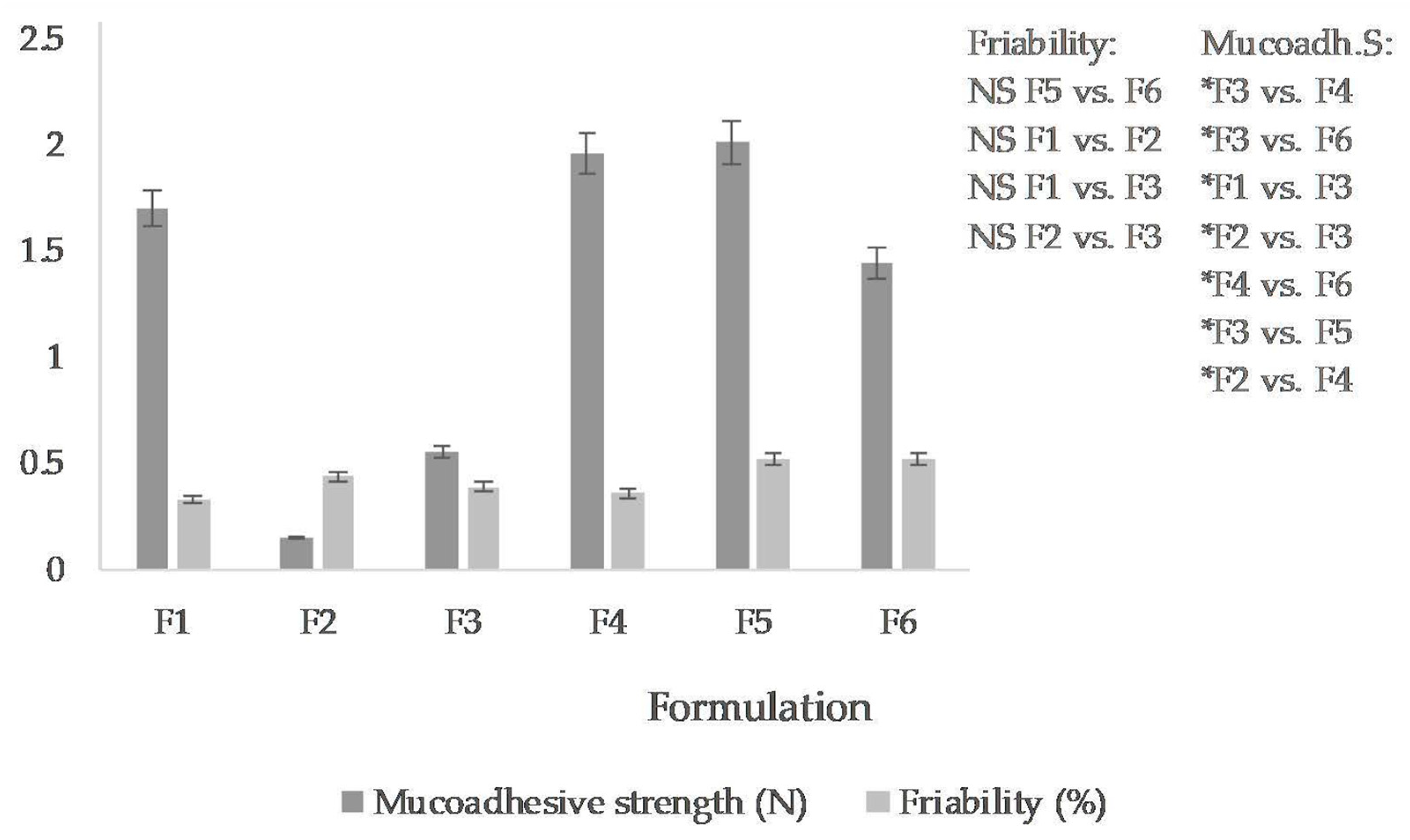
3.3. Friability
3.4. Mucoadhesive Strength
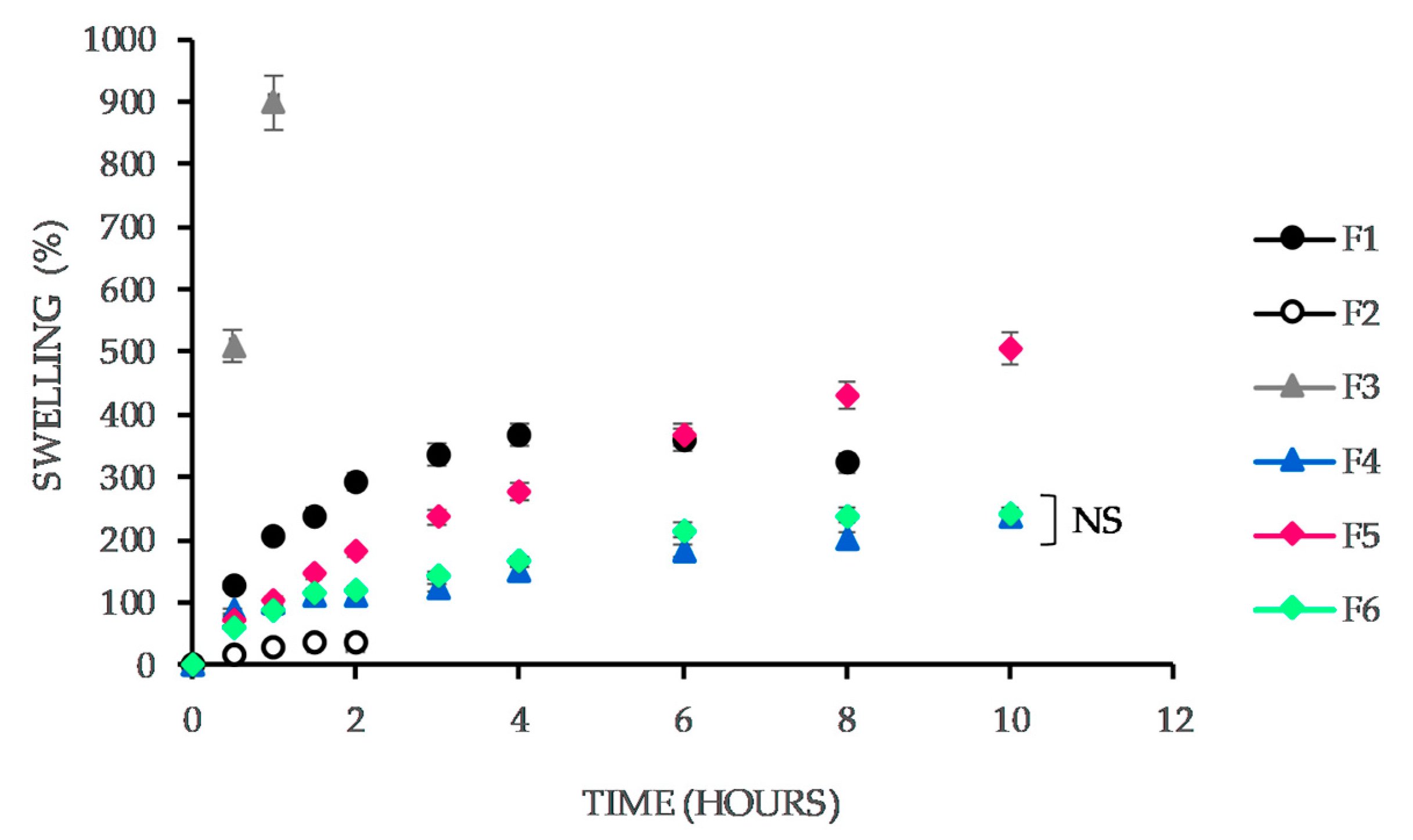
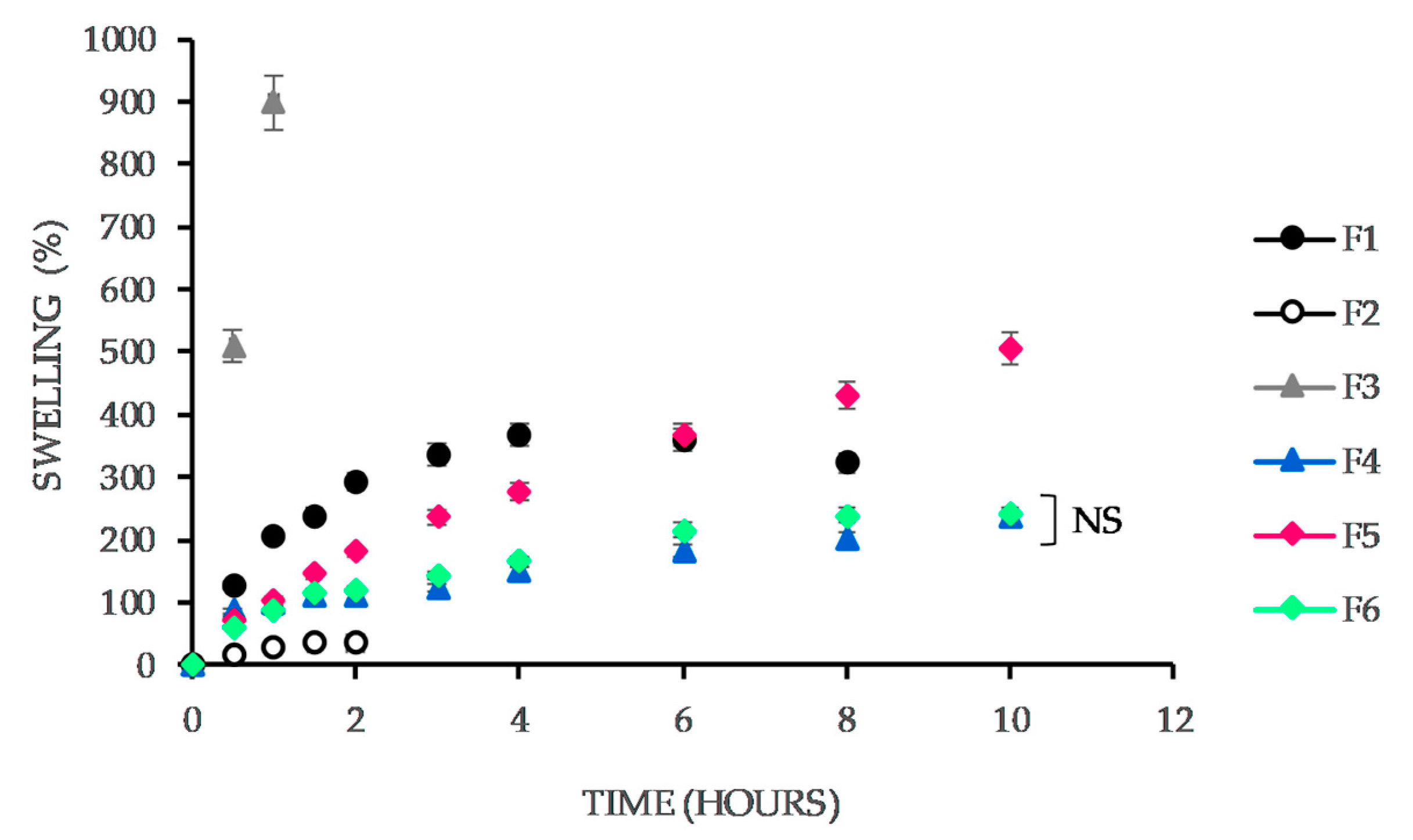
3.5. Swelling Capacity
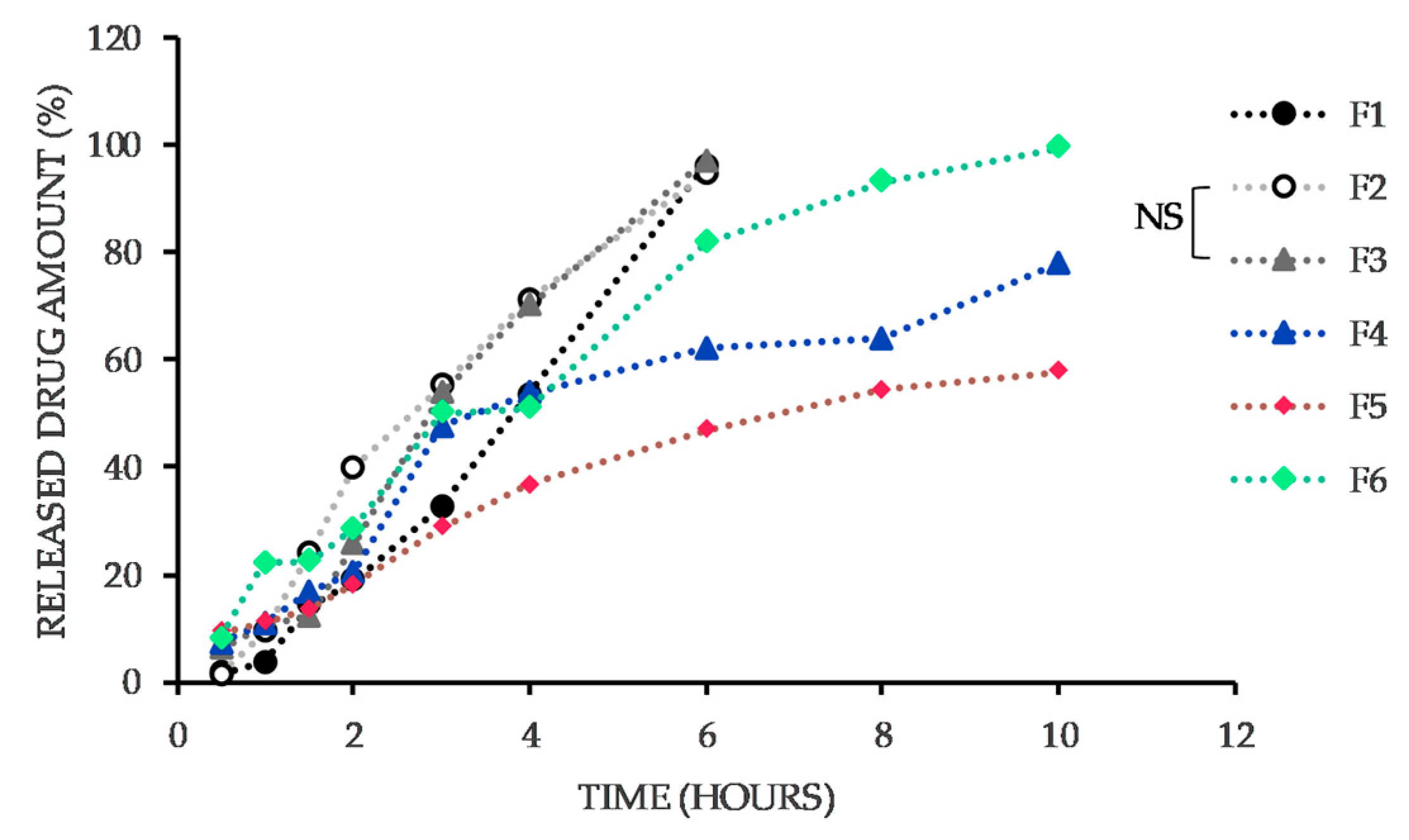
3.6. In Vitro Drug Release
3.7. In Vitro Drug Release Kinetics
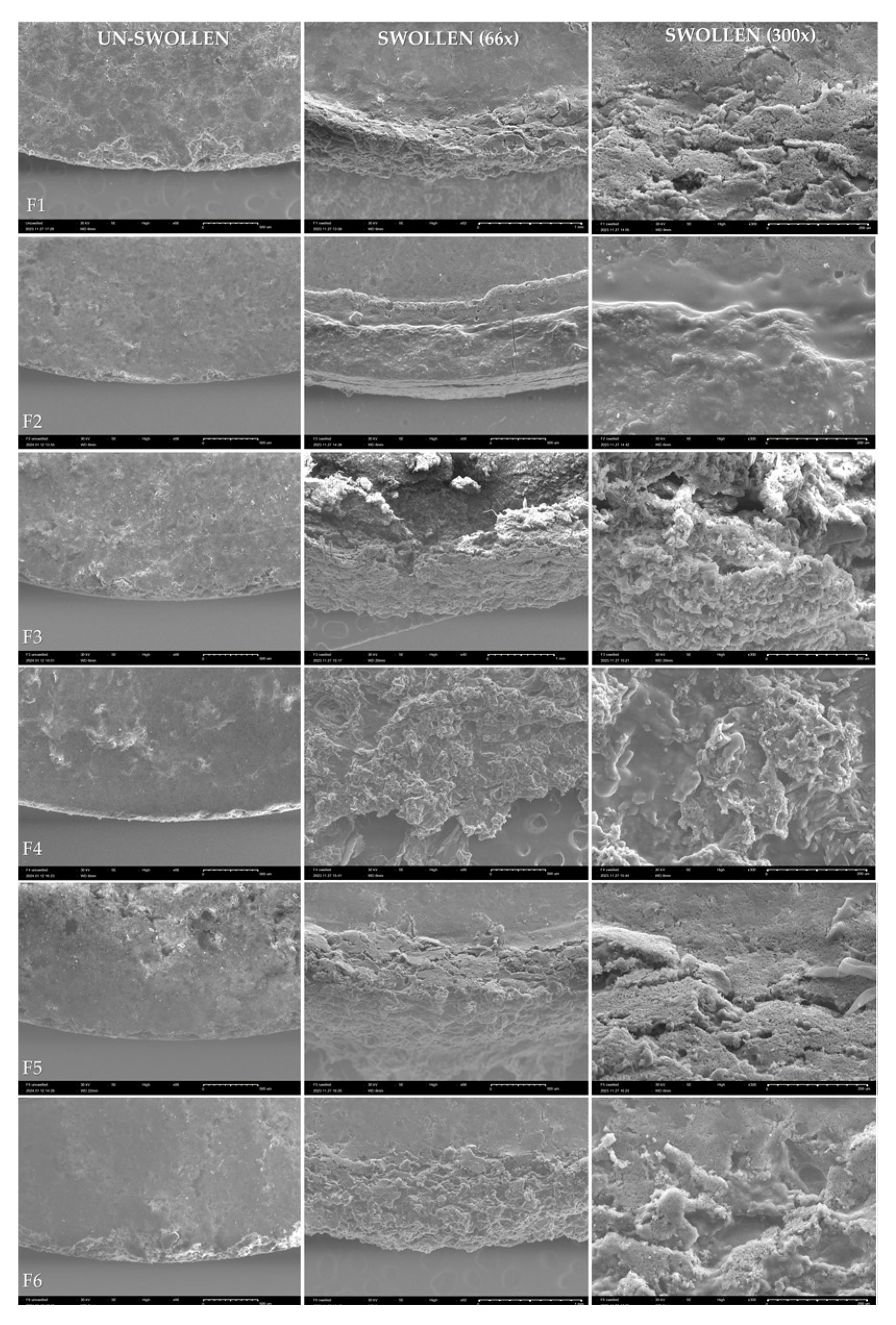
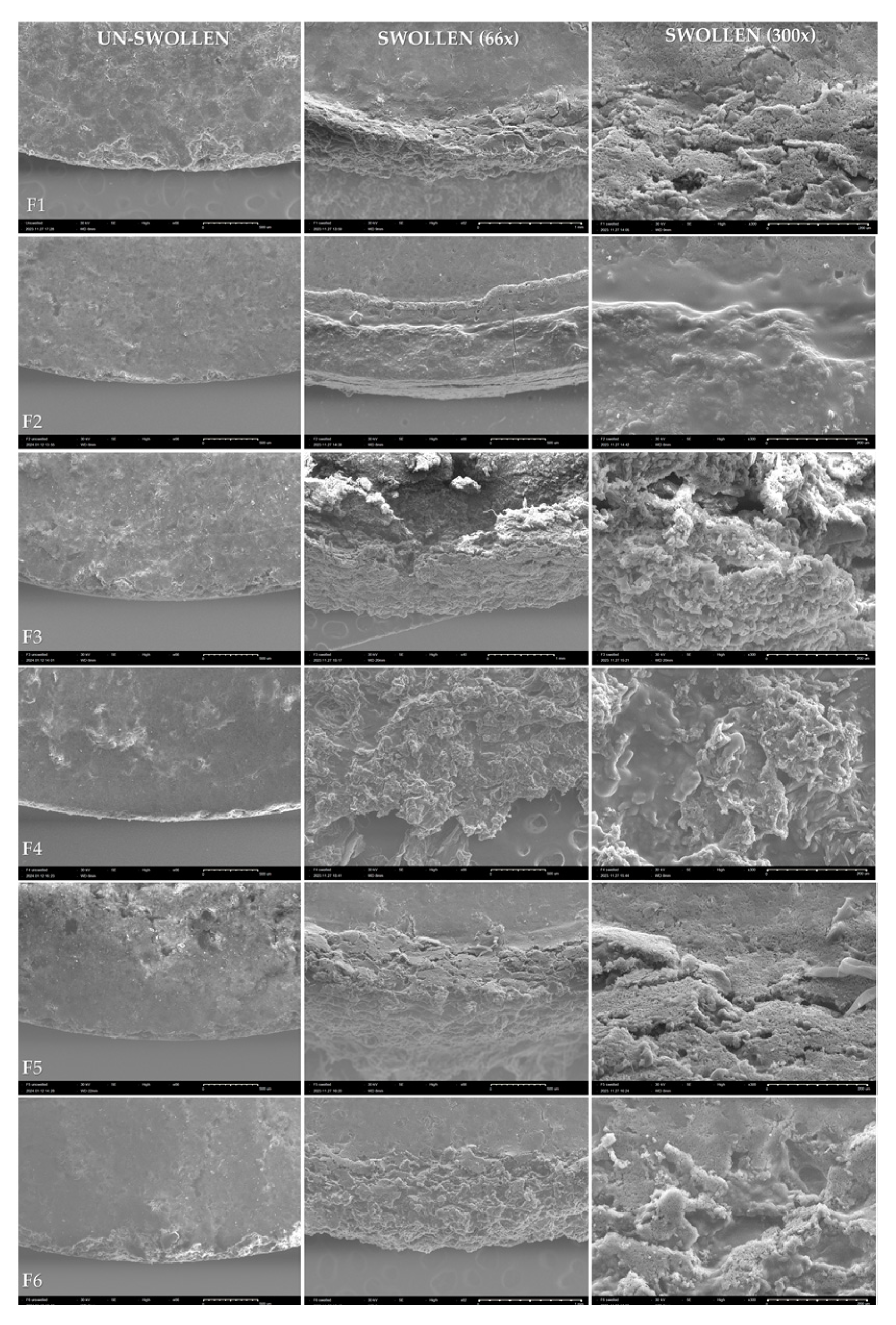
3.8. Characterization of Morphological Changes in Swollen Tablets by SEM
4. Discussion
4.1. Physical Parameters of Tablets and Their Mechanical Resistance
4.2. Mucoadhesive Strength
4.3. Swelling Capacity
4.4. In Vitro Drug Release
4.5. In Vitro Drug Release Kinetics
4.6. Characterization of Morphological Changes in Swollen Tablets by SEM
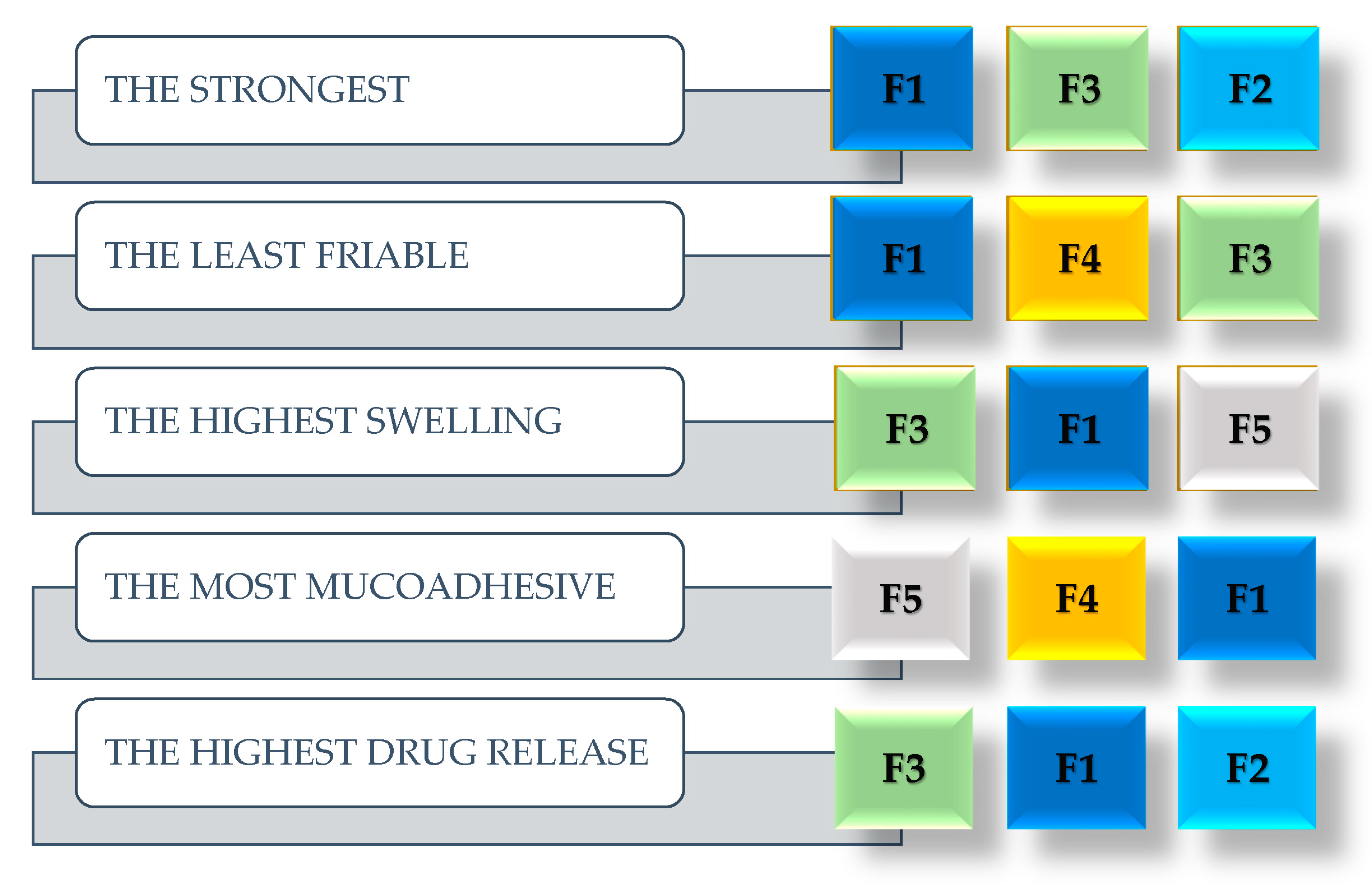
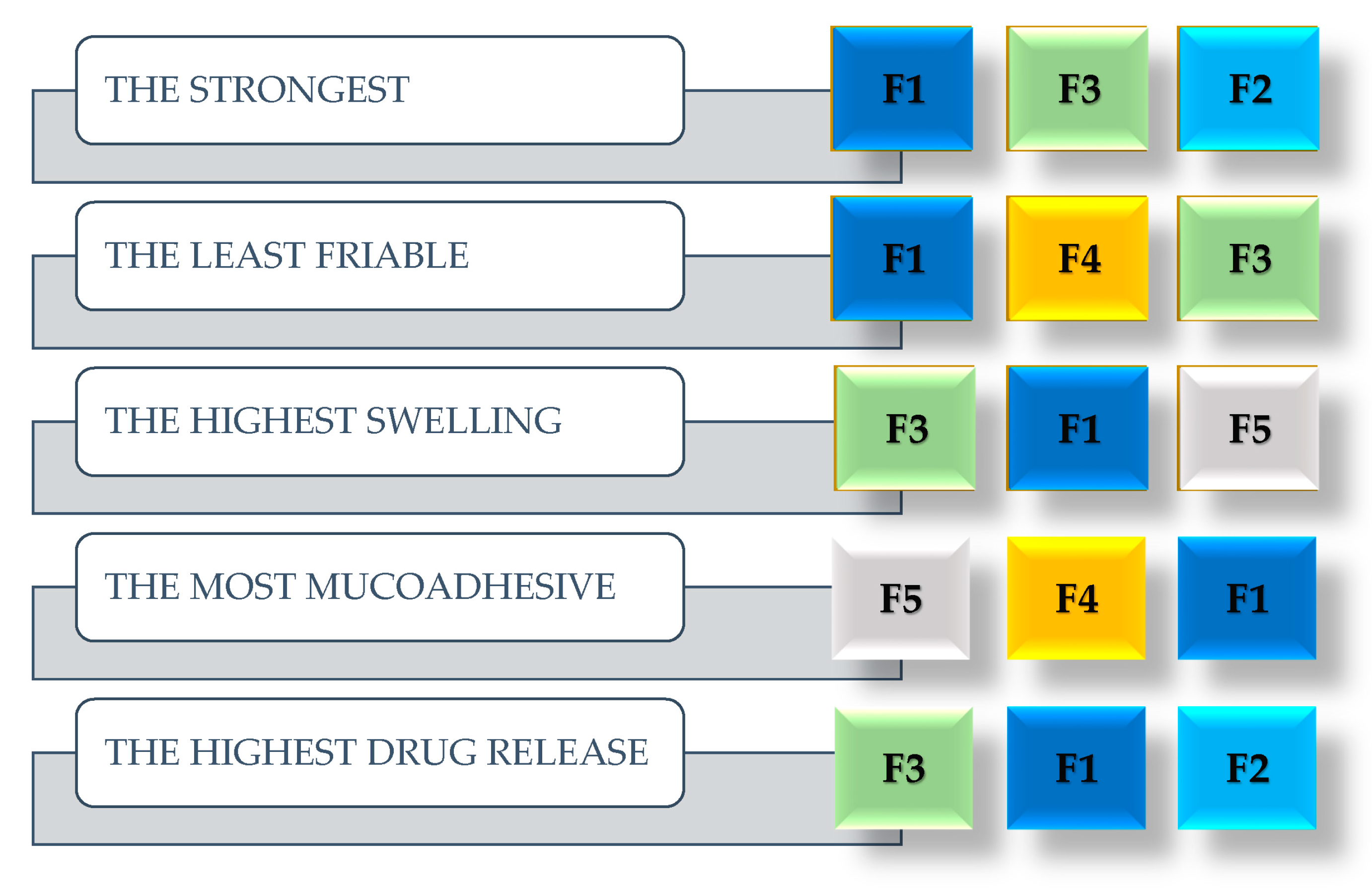
4.7. Summary
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Utomo, E.; Domínguez-Robles, J.; Anjani, Q.K.; Picco, C.J.; Korelidou, A.; Magee, E.; Donnelly, R.F.; Larrañeta, E. Development of 3D-Printed Vaginal Devices Containing Metronidazole for Alternative Bacterial Vaginosis Treatment. Int. J. Pharm. X 2023, 5, 100142. [Google Scholar] [CrossRef] [PubMed]
- Dingsdag, S.A.; Hunter, N. Metronidazole: An Update on Metabolism, Structure-Cytotoxicity and Resistance Mechanisms. J. Antimicrob. Chemother. 2018, 73, 265–279. [Google Scholar] [CrossRef] [PubMed]
- Ceruelos, A.H.; Romero-Quezada, L.C.; Ledezma, J.C.R.; Contreras, L.L. Therapeutic Uses of Metronidazole and Its Side Effects: An Update. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 397–401. [Google Scholar] [CrossRef]
- PubChem Metronidazole. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/4173 (accessed on 5 February 2023).
- Leitsch, D. A Review on Metronidazole: An Old Warhorse in Antimicrobial Chemotherapy. Parasitology 2019, 146, 1167–1178. [Google Scholar] [CrossRef]
- Weir, C.B.; Le, J.K. Metronidazole; StatPearls Publishing: Tampa, FL, USA, 2022. [Google Scholar]
- Żyro, D.; Radko, L.; Śliwińska, A.; Chęcińska, L.; Kusz, J.; Korona-Głowniak, I.; Przekora, A.; Wójcik, M.; Posyniak, A.; Ochocki, J. Multifunctional Silver(I) Complexes with Metronidazole Drug Reveal Antimicrobial Properties and Antitumor Activity against Human Hepatoma and Colorectal Adenocarcinoma Cells. Cancers 2022, 14, 900. [Google Scholar] [CrossRef]
- Metronidazole. Available online: https://go.drugbank.com/drugs/db00916 (accessed on 17 February 2023).
- de Araújo Pereira, R.R.; Bruschi, M.L. Vaginal Mucoadhesive Drug Delivery Systems. Drug Dev. Ind. Pharm. 2012, 38, 643–652. [Google Scholar] [CrossRef] [PubMed]
- Alzainy, A.; Boateng, J. Novel Mucoadhesive Wafers for Treating Local Vaginal Infections. Biomedicines 2022, 10, 3036. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, L.M.; Rohan, L.C. The Importance of the Vaginal Delivery Route for Antiretrovirals in HIV Prevention. Ther. Deliv. 2011, 2, 1535–1550. [Google Scholar] [CrossRef]
- da Silva, P.B.; dos Santos Ramos, M.A.; Bonifácio, B.V.; Negri, K.M.S.; Sato, M.R.; Bauab, T.M.; Chorilli, M. Nanotechnological Strategies for Vaginal Administration of Drugs—A Review. J. Biomed. Nanotechnol. 2014, 10, 2218–2243. [Google Scholar] [CrossRef]
- Dedeloudi, A.; Siamidi, A.; Pavlou, P.; Vlachou, M. Recent Advances in the Excipients Used in Modified Release Vaginal Formulations. Materials 2022, 15, 327. [Google Scholar] [CrossRef]
- Marques, M.R.C.; Loebenberg, R.; Almukainzi, M. Simulated Biological Fluids with Possible Application in Dissolution Testing. Dissolution Technol. 2011, 18, 15–28. [Google Scholar] [CrossRef]
- Deshkar, S.S.; Mahore, J.G. Chapter 5—Herbal Bioactive–Based Vaginal and Rectal Drug Delivery Systems. In Herbal Bioactive-Based Drug Delivery Systems; Bakshi, I.S., Bala, R., Madaan, R., Sindhu, R.K., Eds.; Academic Press: Cambridge, MA, USA, 2022; pp. 111–168. ISBN 978-0-12-824385-5. [Google Scholar]
- Shaikh, R.; Raj Singh, T.R.; Garland, M.J.; Woolfson, A.D.; Donnelly, R.F. Mucoadhesive Drug Delivery Systems. J. Pharm. Bioallied Sci. 2011, 3, 89–100. [Google Scholar] [CrossRef]
- Osmałek, T.; Froelich, A.; Jadach, B.; Tatarek, A.; Gadziński, P.; Falana, A.; Gralińska, K.; Ekert, M.; Puri, V.; Wrotyńska-Barczyńska, J.; et al. Recent Advances in Polymer-Based Vaginal Drug Delivery Systems. Pharmaceutics 2021, 13, 884. [Google Scholar] [CrossRef]
- Žigrayová, D.; Mikušová, V.; Mikuš, P. Advances in Antiviral Delivery Systems and Chitosan-Based Polymeric and Nanoparticulate Antivirals and Antiviral Carriers. Viruses 2023, 15, 647. [Google Scholar] [CrossRef]
- Reddy, P.C.; Chaitanya, K.S.C.; Rao, Y.M. A Review on Bioadhesive Buccal Drug Delivery Systems: Current Status of Formulation and Evaluation Methods. DARU J. Pharm. Sci. 2011, 19, 385. [Google Scholar]
- das Neves, J.; Amaral, M.H.; Bahia, M.F. Vaginal Drug Delivery. In Pharmaceutical Manufacturing Handbook; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2008; pp. 809–878. ISBN 978-0-470-25981-8. [Google Scholar]
- Machado, R.M.; Palmeira-de-Oliveira, A.; Martinez-de-Oliveira, J.; Palmeira-de-Oliveira, R. Vaginal Semisolid Products: Technological Performance Considering Physiologic Parameters. Eur. J. Pharm. Sci. 2017, 109, 556–568. [Google Scholar] [CrossRef]
- Abidin, I.Z.; Rezoagli, E.; Simonassi-Paiva, B.; Fehrenbach, G.W.; Masterson, K.; Pogue, R.; Cao, Z.; Rowan, N.; Murphy, E.J.; Major, I. A Bilayer Vaginal Tablet for the Localized Delivery of Disulfiram and 5-Fluorouracil to the Cervix. Pharmaceutics 2020, 12, 1185. [Google Scholar] [CrossRef]
- Hani, U.; Shivakumar, H.G.; Osmani, R.A.M.; Srivastava, A.; Kumar Varma, N.S. Development of a Curcumin Bioadhesive Monolithic Tablet for Treatment of Vaginal Candidiasis. Iran. J. Pharm. Res. IJPR 2016, 15, 23–34. [Google Scholar] [PubMed]
- Pacheco-Quito, E.-M.; Ruiz-Caro, R.; Rubio, J.; Tamayo, A.; Veiga, M.-D. Carrageenan-Based Acyclovir Mucoadhesive Vaginal Tablets for Prevention of Genital Herpes. Mar. Drugs 2020, 18, 249. [Google Scholar] [CrossRef] [PubMed]
- Abruzzo, A.; Bigucci, F.; Cerchiara, T.; Saladini, B.; Gallucci, M.C.; Cruciani, F.; Vitali, B.; Luppi, B. Chitosan/Alginate Complexes for Vaginal Delivery of Chlorhexidine Digluconate. Carbohydr. Polym. 2013, 91, 651–658. [Google Scholar] [CrossRef] [PubMed]
- Cirri, M.; Maestrelli, F.; Scuota, S.; Bazzucchi, V.; Mura, P. Development and Microbiological Evaluation of Chitosan and Chitosan-Alginate Microspheres for Vaginal Administration of Metronidazole. Int. J. Pharm. 2021, 598, 120375. [Google Scholar] [CrossRef] [PubMed]
- Sánchez, M.T.; Ruiz, M.A.; Castán, H.; Morales, M.E. A Novel Double-Layer Mucoadhesive Tablet Containing Probiotic Strain for Vaginal Administration: Design, Development and Technological Evaluation. Eur. J. Pharm. Sci. Off. J. Eur. Fed. Pharm. Sci. 2018, 112, 63–70. [Google Scholar] [CrossRef]
- Rao, D.M.; Zope, A. Formulation and Evaluation of Mucoadhesive Clotrimazole Vaginal Tablet Using Liquisolid Technology. J. Drug Deliv. Ther. 2019, 9, 477–485. [Google Scholar] [CrossRef]
- Council of Europe. European Pharmacopoeia, 11th ed.; EDQM: Strasbourg, France, 2023. [Google Scholar]
- Perioli, L.; Ambrogi, V.; Pagano, C.; Scuota, S.; Rossi, C. FG90 Chitosan as a New Polymer for Metronidazole Mucoadhesive Tablets for Vaginal Administration. Int. J. Pharm. 2009, 377, 120–127. [Google Scholar] [CrossRef]
- Li, K.L.; Castillo, A.L. Formulation and Evaluation of a Mucoadhesive Buccal Tablet of Mefenamic Acid. Braz. J. Pharm. Sci. 2020, 56, e18575. [Google Scholar] [CrossRef]
- Abd-Alrassol, K.S.; Al-Salman, H.N.K.; Jasim, E.; Hussein, H.H. Determination and Evaluation of Doses of Metronidazole in Different Quantities and Formulations with Multiple Spectroscopic Methods. Syst. Rev. Pharm. 2020, 11, 130–139. [Google Scholar] [CrossRef]
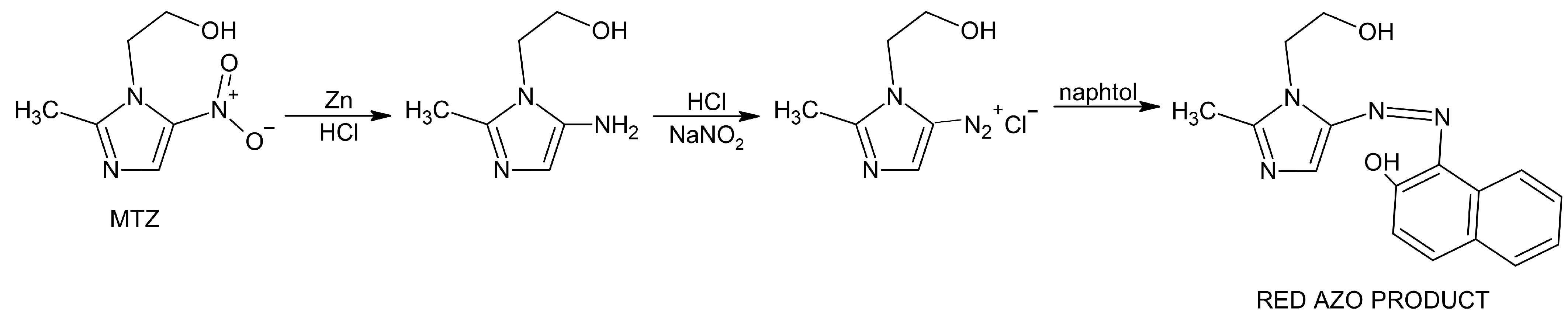
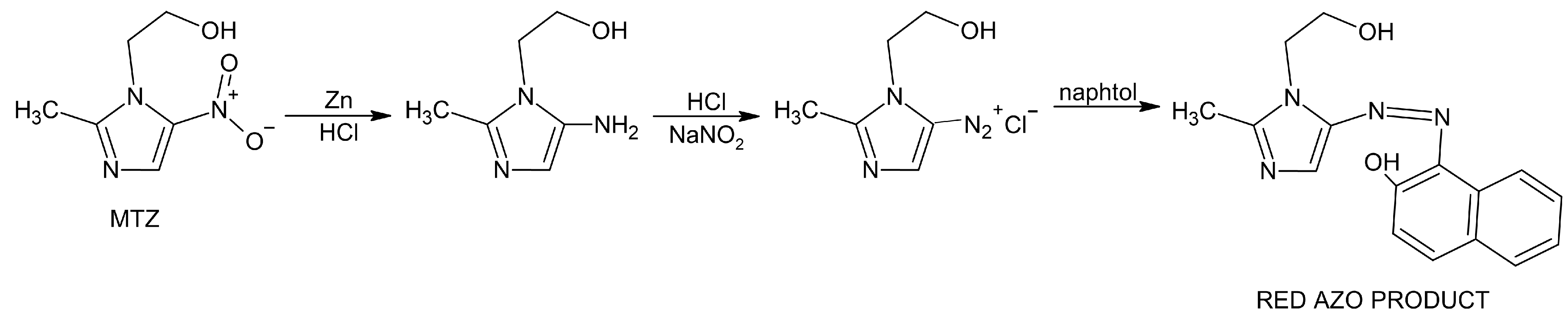
- Ibrahim, W.H.; Bashir, W.A. Spectrophotometric Determination of Metronidazole by Prior Reduction and Subsequent Diazotisation and Coupling with N-(1-Naphthyl)Ethylenediamine—Application to Pharmaceutical Preparations. Rafidain J. Sci. 2012, 23, 78–93. [Google Scholar] [CrossRef]
- Saffaj, T.; Charrouf, M.; Abourriche, A.; Aboud, Y.; Bennamara, A.; Berrada, M. Spectrophotometric Determination of Metronidazole and Secnidazole in Pharmaceutical Preparations Based on the Formation of Dyes. Dyes Pigment. 2006, 70, 259–262. [Google Scholar] [CrossRef]
- Dash, S.; Murthy, P.N.; Nath, L.; Chowdhury, P. Kinetic Modeling on Drug Release from Controlled Drug Delivery Systems. Acta Pol. Pharm. 2010, 67, 217–223. [Google Scholar]
- Fichorova, R.N.; Mendonca, K.; Yamamoto, H.S.; Murray, R.; Chandra, N.; Doncel, G.F. A Quantitative Multiplex Nuclease Protection Assay Reveals Immunotoxicity Gene Expression Profiles in the Rabbit Model for Vaginal Drug Safety Evaluation. Toxicol. Appl. Pharmacol. 2015, 285, 198–206. [Google Scholar] [CrossRef] [PubMed]
- McCracken, J.M.; Calderon, G.A.; Robinson, A.J.; Sullivan, C.N.; Cosgriff-Hernandez, E.; Hakim, J.C.E. Animal Models and Alternatives in Vaginal Research: A Comparative Review. Reprod. Sci. 2021, 28, 1759–1773. [Google Scholar] [CrossRef]
- Karmakar, K. Application of Natural Gum as a Binder in Modern Drug Delivery. J. Anal. Pharm. Res. 2016, 3, 09752366. [Google Scholar] [CrossRef]
- Bisht, T.; Poonam, R. A Comparative Study of Matrix Tablets Designed by Different Methods. Int. J. Pharm. Sci. Nanotechnol. IJPSN 2017, 10, 3645–3652. [Google Scholar] [CrossRef]
- Chavda, H.; Patel, M.S.; Patel, C.N. Preparation and in Vitro Evaluation of Guar Gum Based Triple-Layer Matrix Tablet of Diclofenac Sodium. Res. Pharm. Sci. 2012, 7, 57–64. [Google Scholar] [PubMed]
- Bruschi, M.L.; Borghi-Pangoni, F.B.; Junqueira, M.V.; de Souza Ferreira, S.B. Chapter 12—Nanostructured Therapeutic Systems with Bioadhesive and Thermoresponsive Properties. In Nanostructures for Novel Therapy; Ficai, D., Grumezescu, A.M., Eds.; Micro and Nano Technologies; Elsevier: Amsterdam, The Netherlands, 2017; pp. 313–342. ISBN 978-0-323-46142-9. [Google Scholar]
- Cook, S.L.; Bull, S.P.; Methven, L.; Parker, J.K.; Khutoryanskiy, V.V. Mucoadhesion: A Food Perspective. Food Hydrocoll. 2017, 72, 281–296. [Google Scholar] [CrossRef]
- Daneshmehr, M.; Adibpour, H.; Ataie, Z. Formulation and Evaluation of Hydrocortisone Sodium Succinate Mucoadhesive Buccal Tablet. Int. J. Pharm. Investig. 2020, 10, 300–304. [Google Scholar] [CrossRef]
- Munot, N.; Kandekar, U.; Rikame, C.; Patil, A.; Sengupta, P.; Urooj, S.; Bilal, A. Improved Mucoadhesion, Permeation and In Vitro Anticancer Potential of Synthesized Thiolated Acacia and Karaya Gum Combination: A Systematic Study. Molecules 2022, 27, 6829. [Google Scholar] [CrossRef] [PubMed]
- Martín-Illana, A.; Chinarro, E.; Cazorla-Luna, R.; Notario-Perez, F.; Veiga-Ochoa, M.D.; Rubio, J.; Tamayo, A. Optimized Hydration Dynamics in Mucoadhesive Xanthan-Based Trilayer Vaginal Films for the Controlled Release of Tenofovir. Carbohydr. Polym. 2022, 278, 118958. [Google Scholar] [CrossRef] [PubMed]
- Kotla, N.; Shivapooja, A.; Muthyala, J.; Pandya, P. Effect of Guar Gum and Xanthan Gum Compression Coating on Release Studies of Metronidazole in Human Fecal Media for Colon Targeted Drug Delivery Systems. Asian J. Pharm. Clin. Res. 2013, 6, 315–318. [Google Scholar]
- Baus, R.A.; Innerhofer, J.; Rohrer, J.; Lupo, N.; Bernkop-Schnürch, A. Anhydrous Thiomers: Strategy for Enhanced Mucoadhesion. Eur. J. Pharm. Biopharm. 2018, 129, 273–281. [Google Scholar] [CrossRef]
- Cevher, E.; Sensoy, D.; Taha, M.A.M.; Araman, A. Effect of Thiolated Polymers to Textural and Mucoadhesive Properties of Vaginal Gel Formulations Prepared with Polycarbophil and Chitosan. AAPS PharmSciTech 2008, 9, 953–965. [Google Scholar] [CrossRef]
- Ulery, B.D.; Nair, L.S.; Laurencin, C.T. Biomedical Applications of Biodegradable Polymers. J. Polym. Sci. Part B Polym. Phys. 2011, 49, 832–864. [Google Scholar] [CrossRef]
- Boddupalli, B.M.; Mohammed, Z.N.K.; Nath, R.A.; Banji, D. Mucoadhesive Drug Delivery System: An Overview. J. Adv. Pharm. Technol. Res. 2010, 1, 381–387. [Google Scholar] [CrossRef]
- Yermak, I.M.; Davydova, V.N.; Volod’ko, A.V. Mucoadhesive Marine Polysaccharides. Mar. Drugs 2022, 20, 522. [Google Scholar] [CrossRef]
- Aulton, M.E.; Taylor, K. Aulton’s Pharmaceutics: The Design and Manufacture of Medicines; Elsevier Health Sciences: Amsterdam, The Netherlands, 2013; ISBN 978-0-7020-4290-4. [Google Scholar]
- Acarturk, F. Mucoadhesive Vaginal Drug Delivery Systems. Recent Pat. Drug Deliv. Amp Formul. 2009, 3, 193. [Google Scholar] [CrossRef] [PubMed]
- Abidin, I.Z.; Murphy, E.J.; Fehrenbach, G.W.; Rezoagli, E.; Gately, N.; Major, I. A Systematic Review of Mucoadhesive Vaginal Tablet Testing. Drug Target Insights 2023, 17, 5–30. [Google Scholar] [CrossRef] [PubMed]
- Katz, D.F.; Yuan, A.; Gao, Y. Vaginal Drug Distribution Modeling. Adv. Drug Deliv. Rev. 2015, 92, 2–13. [Google Scholar] [CrossRef]
- Pourtalebi Jahromi, L.; Ghazali, M.; Ashrafi, H.; Azadi, A. A Comparison of Models for the Analysis of the Kinetics of Drug Release from PLGA-Based Nanoparticles. Heliyon 2020, 6, e03451. [Google Scholar] [CrossRef]
- Arora, G.; Malik, K.; Singh, I.; Arora, S.; Rana, V. Formulation and Evaluation of Controlled Release Matrix Mucoadhesive Tablets of Domperidone Using Salvia Plebeian Gum. J. Adv. Pharm. Technol. Res. 2011, 2, 163–169. [Google Scholar] [CrossRef]
- Jackson, T.C.; Agboke, A.A.; Udofa, E.J.; Ucheokoro, A.S.; Udo, B.E.; Ifekpolugo, N.L. Characterization and Release Kinetics of Metronidazole Loaded Silver Nanoparticles Prepared from Carica Papaya Leaf Extract. Adv. Nanopart. 2019, 08, 47–54. [Google Scholar] [CrossRef]
- Paul, D.R. Elaborations on the Higuchi Model for Drug Delivery. Int. J. Pharm. 2011, 418, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Rosu, M.-C.; Bratu, I. Promising Psyllium-Based Composite Containing TiO2 Nanoparticles as Aspirin-Carrier Matrix. Prog. Nat. Sci. Mater. Int. 2014, 24, 205–209. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Formulation | F1 | F2 | F3 | F4 | F5 | F6 |
|---|---|---|---|---|---|---|
| Metronidazole (g) | 0.05 | 0.05 | 0.05 | 0.05 | 0.05 | 0.05 |
| Vivapur® (g) | 0.127 | 0.127 | 0.127 | 0.127 | 0.127 | 0.127 |
| Magnesium stearate (g) | 0.003 | 0.003 | 0.003 | 0.003 | 0.003 | 0.003 |
| Sodium alginate (g) | 0.12 | - | - | - | - | - |
| Acacia gum (g) | - | 0.12 | - | - | - | - |
| Carrageenan (g) | - | - | 0.12 | - | - | - |
| Guar gum (g) | - | - | - | 0.12 | - | - |
| Xanthan gum (g) | - | - | - | - | 0.12 | - |
| Tragacanth (g) | - | - | - | - | - | 0.12 |
| Formulation | Average Mass (g) | Average Height (mm) | Hardness (N) | Average Hardness (N) | |
|---|---|---|---|---|---|
| Min. | Max. | ||||
| F1 | 0.302 ± 0.003 * | 2.96 ± 0.03 * | 69 | 116 | 95.30 ± 17.70 |
| F2 | 0.298 ± 0.003 * | 3.03 ± 0.02 * | 86 | 98 | 92.20 ± 4.29 |
| F3 | 0.298 ± 0.004 * | 2.94 ± 0.04 * | 85 | 112 | 93.10 ± 7.65 |
| F4 | 0.297 ± 0.003 * | 2.90 ± 0.03 * | 52 | 60 | 54.40 ± 2.59 |
| F5 | 0.297 ± 0.003 * | 3.02 ± 0.03 * | 69 | 82 | 74.80 ± 4.66 |
| F6 | 0.298 ± 0.003 * | 3.06 ± 0.04 * | 67 | 74 | 71.70 ± 2.26 |
| Zero | First | Higuchi | Hix.-Crowell | Kors.-Peppas | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| t | + Kft | |||||||||
| r2 | K0 | r2 | Kf | r2 | KH | r2 | KHC | r2 | KKP | |
| F1 | 0.9824 | 17.33 | 0.8102 | 0.23 | 0.9162 | 30.23 | 0.9562 | 0.57 | 0.9763 | 1.73 |
| F2 | 0.9687 | 17.24 | 0.9471 | 0.22 | 0.9923 | 31.51 | 0.9896 | 0.51 | 0.9635 | 1.66 |
| F3 | 0.9759 | 17.94 | 0.8897 | 0.26 | 0.9495 | 31.97 | 0.9562 | 0.57 | 0.9023 | 1.22 |
| F4 | 0.9545 | 9.45 | 0.9449 | 0.06 | 0.9406 | 17.20 | 0.9289 | 0.18 | 0.9568 | 0.86 |
| F5 | 0.9659 | 6.83 | 0.9795 | 0.04 | 0.9807 | 12.61 | 0.9717 | 0.12 | 0.9692 | 0.70 |
| F6 | 0.9518 | 11.99 | 0.8879 | 0.21 | 0.9789 | 22.29 | 0.9805 | 0.38 | 0.9441 | 0.82 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bartoníková, K.; Špaglová, M.; Papadakos, M.; Hanko, M.; Macho, O. Mucoadhesive Vaginal Tablets Containing Metronidazole: Screening of Optimal Natural Polymer in the Composition. Sci. Pharm. 2024, 92, 10. https://doi.org/10.3390/scipharm92010010
Bartoníková K, Špaglová M, Papadakos M, Hanko M, Macho O. Mucoadhesive Vaginal Tablets Containing Metronidazole: Screening of Optimal Natural Polymer in the Composition. Scientia Pharmaceutica. 2024; 92(1):10. https://doi.org/10.3390/scipharm92010010
Chicago/Turabian StyleBartoníková, Kamila, Miroslava Špaglová, Martina Papadakos, Michal Hanko, and Oliver Macho. 2024. "Mucoadhesive Vaginal Tablets Containing Metronidazole: Screening of Optimal Natural Polymer in the Composition" Scientia Pharmaceutica 92, no. 1: 10. https://doi.org/10.3390/scipharm92010010
APA StyleBartoníková, K., Špaglová, M., Papadakos, M., Hanko, M., & Macho, O. (2024). Mucoadhesive Vaginal Tablets Containing Metronidazole: Screening of Optimal Natural Polymer in the Composition. Scientia Pharmaceutica, 92(1), 10. https://doi.org/10.3390/scipharm92010010