Transmission Electron Microscopy of XDR Mycobacterium tuberculosis Isolates Grown on High Dose of Ofloxacin

Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Isolates
2.2. Culture Conditions
2.3. Inoculation
2.4. Transmission Electron Microscopy (TEM)
3. Results
3.1. Culture Results
3.2. TEM Examinations
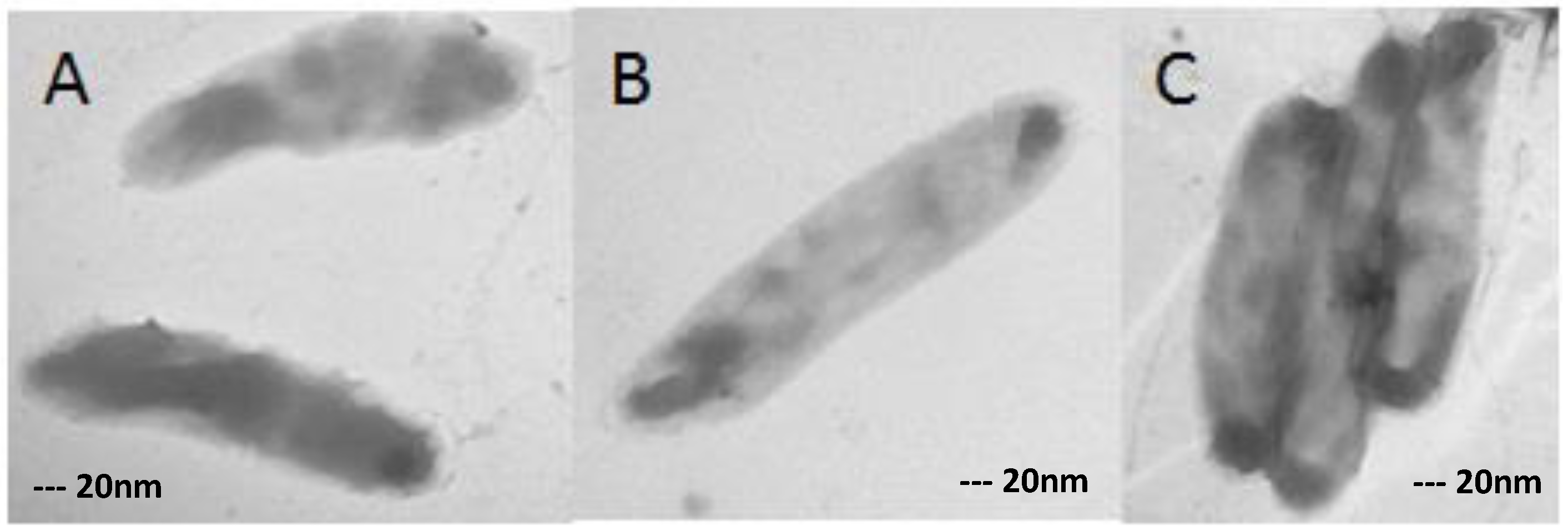
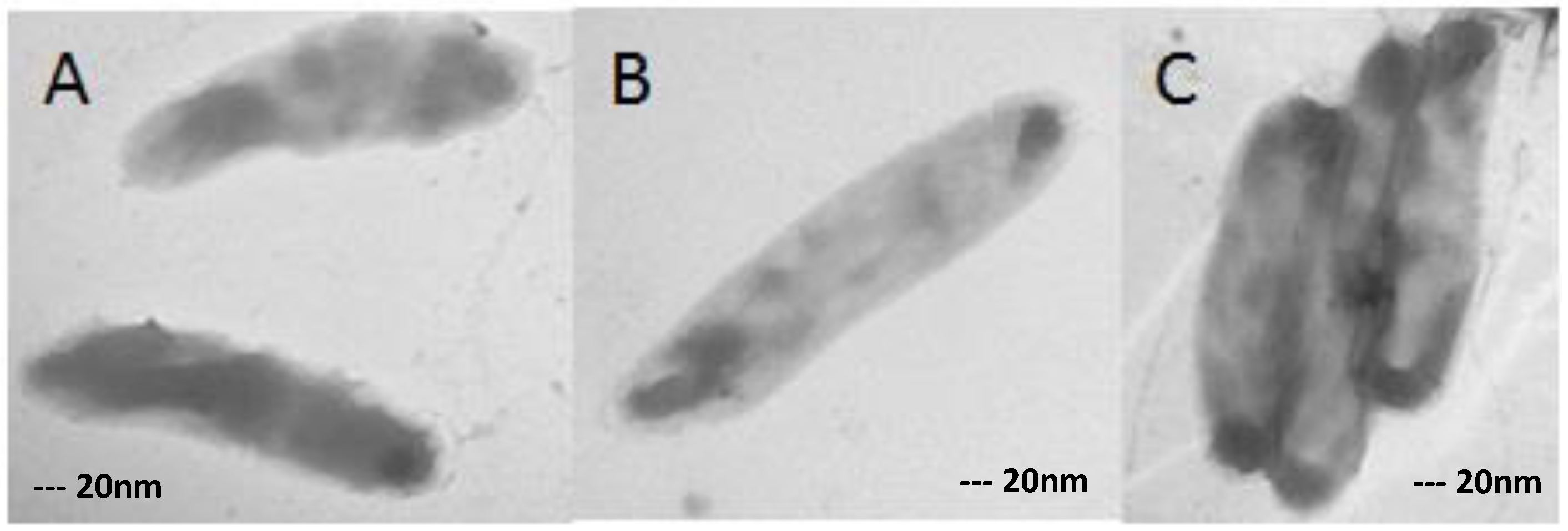
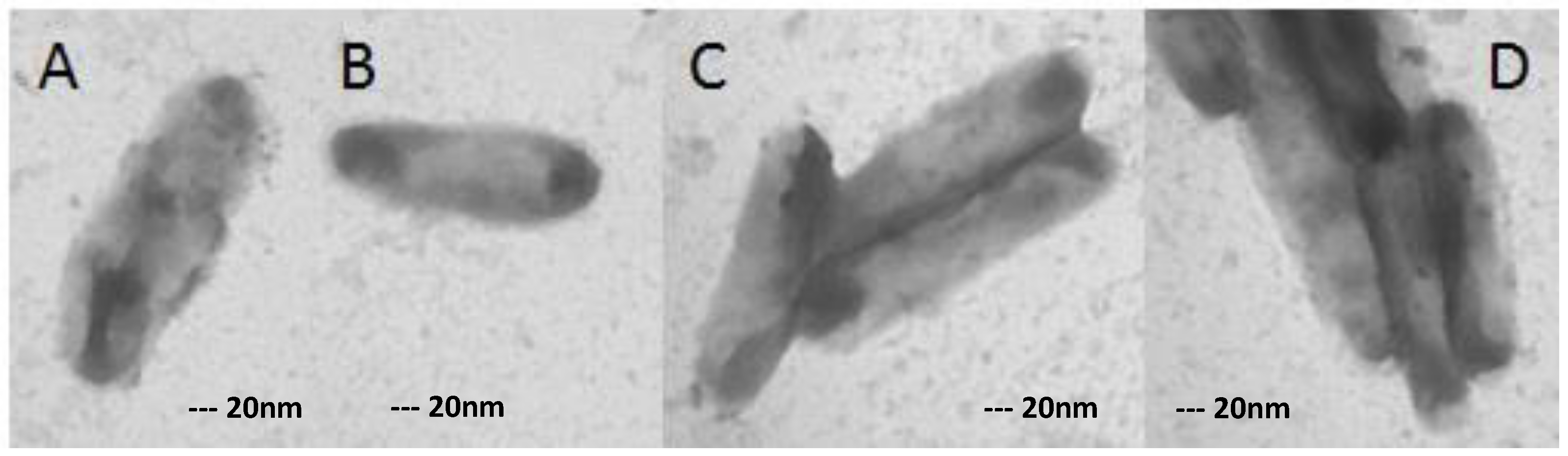
3.3. XDR MTB Grown on Drug-Free Medium
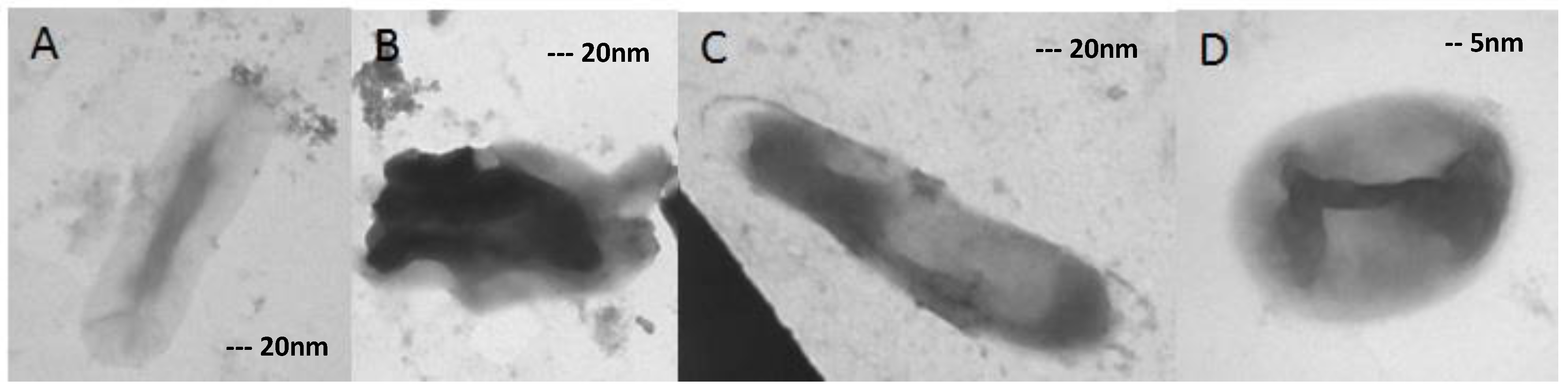
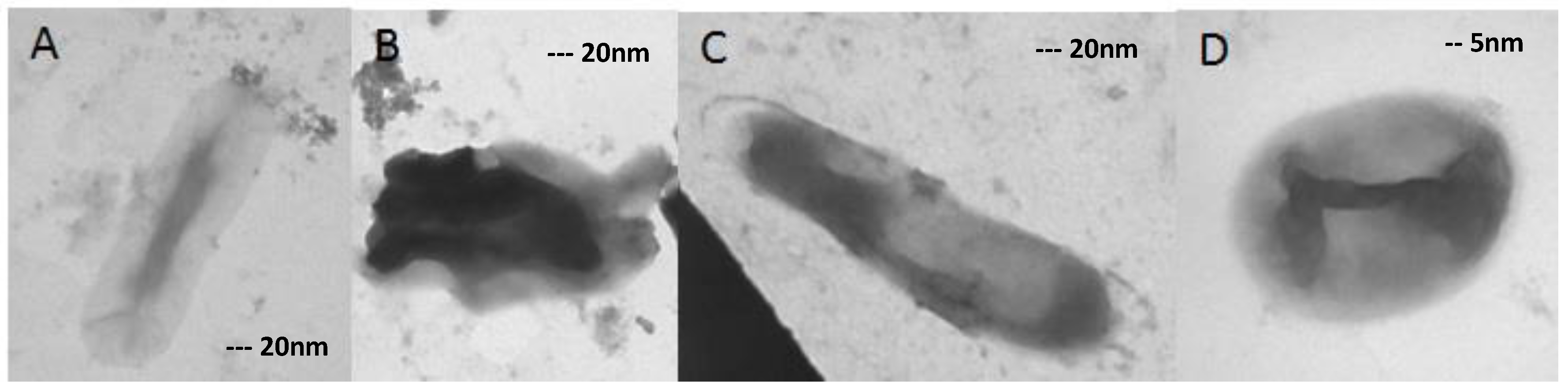
3.4. XDR MTB Grown on 8 mg/L Ofloxacin
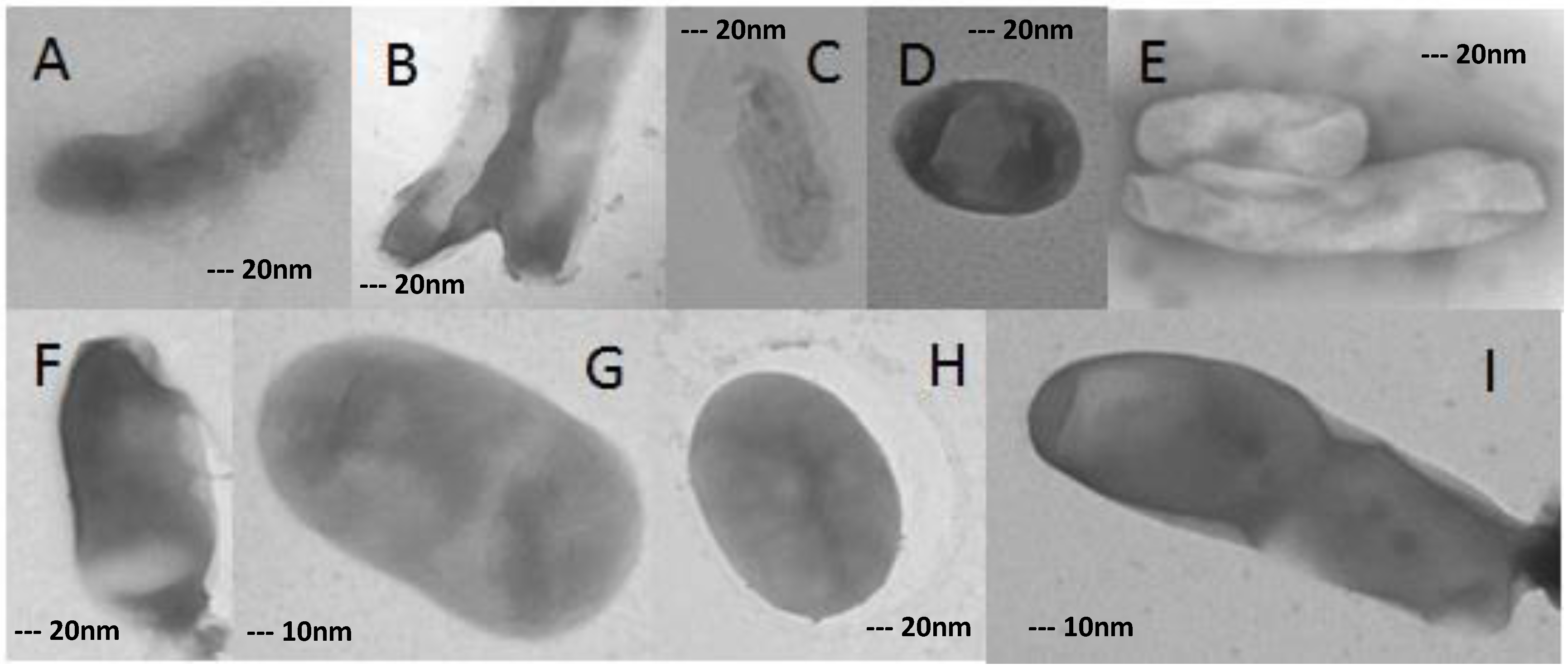
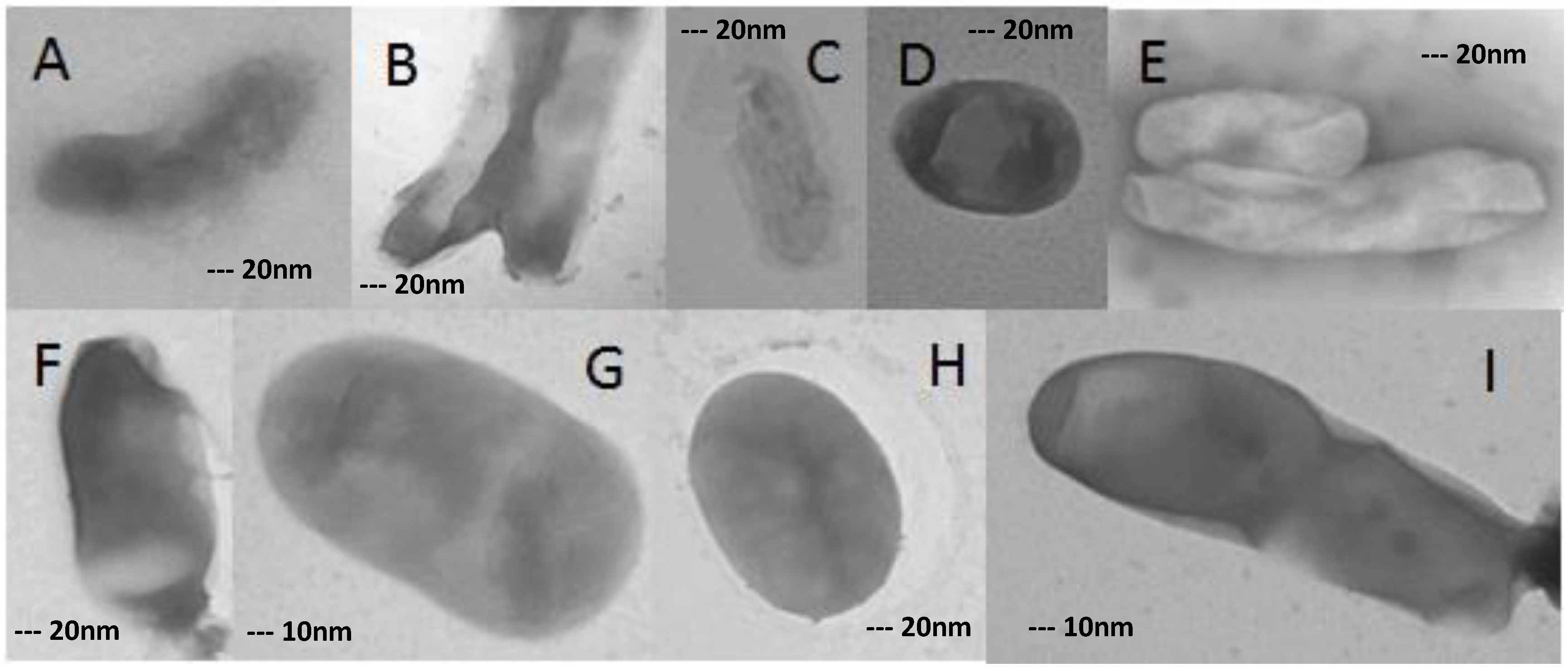
3.5. XDR MTB Grown on 16 mg/L Ofloxacin
3.6. XDR MTB Grown on 32 mg/L Ofloxacin
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Zager, E.M.; Mcnerney, R. Multidrug-resistant tuberculosis. BMC Infect. Dis. 2008, 8, 1–5. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Global Tuberculosis Control—Surveillance, Planning, Financing. 2008. Available online: http://www.who.int/tb/publications/global_report/2008/en/index.html (accessed on 6 March 2013).
- World Health Organization. Global Tuberculosis Report 2012. 2012. Available online: http://apps.who.int/iris/bitstream/10665/75938/1/9789241564502_eng.pdf (accessed on 6 March 2013).
- Surkova, L.; Horevich, H.L.; Titov, L.P.; Sahalchyk, E.; Arjomandzadegan, M.; Alinejad, S.; Sadrnia, M. A study on demographic characteristics of drug resistant Mycobacterium tuberculosis isolates in Belarus. Int. J. Mycobacteriol. 2012, 1, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Ojha, A.K.; Hatfull, G.F. Biofilms of Mycobacterium tuberculosis: New perspectives of an old pathogen. In Understanding Tuberculosis—Deciphering the Secret Life of the Bacilli; Cardona, P., Ed.; Intech Open Access Publisher: Reijek, Croatia, 2012; pp. 181–192. [Google Scholar]
- Espinal, M.A. The global situation of MDR-TB. Tuberculosis 2003, 83, 44–51. [Google Scholar] [CrossRef]
- Spigelman, M.; Ma, Z. Mycobacterium tuberculosis: New tricks for an old bug. Expert Rev. Anti-Infect. Ther. 2004, 2, 467–469. [Google Scholar] [CrossRef] [PubMed]
- Arjomandzadegan, M.; Titov, L.P.; Surkova, L.K.; Farnia, P.; Sheikholeslami, F.; Owlia, P.; Eshghinejad, A.; Farazi, A.A. Determination of principal genotypic groups among susceptible, MDR and XDR clinical isolates of Mycobacterium tuberculosis in Belarus and Iran. Tuberk Toraks 2012, 60, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Arjomandzadegan, M.; Nazari, R.; Zolfaghari, M.R.; Taherahmadi, M.; Sadrnia, M.; Titov, L.P.; Ahmadi, A.; Shojapoor, M. Performance Assessment of the Polymerase Chain Reaction-Restriction Fragment Length Polymorphism Method for Rapid Detection of Susceptibility to Ethambutol and Molecular Prediction of Extensively Drug-resistant Tuberculosis in Clinical Isolates of Mycobacterium tuberculosis. West Indian Med. J. 2015, 64, 325–332. [Google Scholar] [PubMed]
- Hall, C.E.; Keegan, H.; Rogstad, K.E. Psychiatric side effects of ofloxacin used in the treatment of pelvic inflammatory disease. Int. J. STD AIDS 2003, 14, 636–637. [Google Scholar] [CrossRef] [PubMed]
- Khrustalev, V.V.; Arjomandzadegan, M.; Barkovsky, E.V.; Titov, L.P. Low rates of synonymous mutations in sequences of Mycobacterium tuberculosis GyrA and KatG genes. Tuberculosis 2012, 92, 333–344. [Google Scholar] [CrossRef] [PubMed]
- Hosseini, H.; Fooladi, A.A.I.; Arjomandzadegan, M.; Emami, N.; Bornasi, H. Genetics study and transmission electron microscopy of pili in susceptible and resistant clinical isolates of Mycobacterium tuberculosis. Asian Pac. J. Trop. Med. 2014, 7 (Suppl. S1), S199–S203. [Google Scholar] [CrossRef]
- Drlica, K.; Zhao, X. DNA gyrase, topoisomerase IV, and the 4-quinolones. Microbiol. Mol. Biol. Rev. 1997, 61, 377–392. [Google Scholar] [PubMed]
- Nelson, J.M.; Chiller, T.M.; Powers, J.H.; Angulo, F.J. Fluoroquinolone-resistant Campylobacter species and the withdrawal of fluoroquinolones from use in poultry: A public health success story. Clin. Infect. Dis. 2007, 44, 977–980. [Google Scholar] [CrossRef] [PubMed]
- Sieniawska, E.; Swatko-Ossor, M.; Sawicki, R.; Ginalska, G. Morphological Changes in the Overall Mycobacterium tuberculosis H37Ra Cell Shape and Cytoplasm Homogeneity due to Mutellina purpurea L. Essential Oil and Its Main Constituents. Med. Princ. Pract. 2015, 24, 527–532. [Google Scholar] [CrossRef] [PubMed]
- Dahl, J.L. Electron microscopy analysis of Mycobacterium tuberculosis cell division. FEMS Microbiol. Lett. 2004, 240, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Dahl, J.L. Scanning electron microscopy analysis of aged Mycobacterium tuberculosis cells. Can. J. Microbiol. 2005, 51, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Velayati, A.A.; Farnia, P. Differences in cell wall thickness between resistant and nonresistant strains of Mycobacterium tuberculosis: Using transmission electron microscopy. Chemotherapy 2009, 55, 303–307. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dose (mg/mL) | Destruction | Spherical | Oval | Without Changes |
|---|---|---|---|---|
| 8 | 0% | 0% | 43% | 57% |
| 16 | 29.40% | 29.40% | 17.60% | 23.50% |
| 32 | 32.20% | 20.80% | 28% | 19% |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arjomandzadegan, M.; Sadrnia, M.; Titov, L.; Surkova, L.; Sarmadian, H.; Ghasemikhah, R.; Hosseiny, H. Transmission Electron Microscopy of XDR Mycobacterium tuberculosis Isolates Grown on High Dose of Ofloxacin. Sci. Pharm. 2017, 85, 3. https://doi.org/10.3390/scipharm85010003
Arjomandzadegan M, Sadrnia M, Titov L, Surkova L, Sarmadian H, Ghasemikhah R, Hosseiny H. Transmission Electron Microscopy of XDR Mycobacterium tuberculosis Isolates Grown on High Dose of Ofloxacin. Scientia Pharmaceutica. 2017; 85(1):3. https://doi.org/10.3390/scipharm85010003
Chicago/Turabian StyleArjomandzadegan, Mohammad, Maryam Sadrnia, Leonid Titov, Larissa Surkova, Hossein Sarmadian, Reza Ghasemikhah, and Hossein Hosseiny. 2017. "Transmission Electron Microscopy of XDR Mycobacterium tuberculosis Isolates Grown on High Dose of Ofloxacin" Scientia Pharmaceutica 85, no. 1: 3. https://doi.org/10.3390/scipharm85010003
APA StyleArjomandzadegan, M., Sadrnia, M., Titov, L., Surkova, L., Sarmadian, H., Ghasemikhah, R., & Hosseiny, H. (2017). Transmission Electron Microscopy of XDR Mycobacterium tuberculosis Isolates Grown on High Dose of Ofloxacin. Scientia Pharmaceutica, 85(1), 3. https://doi.org/10.3390/scipharm85010003