
Saving Resources: SARS-CoV-2 Diagnostics by Real-Time RT-PCR Using Reduced Reaction Volumes


Abstract
:1. Introduction
2. Materials and Methods
2.1. RNA Standard, Virus and Diagnostic Samples
2.2. Real-Time RT-PCRs
3. Results
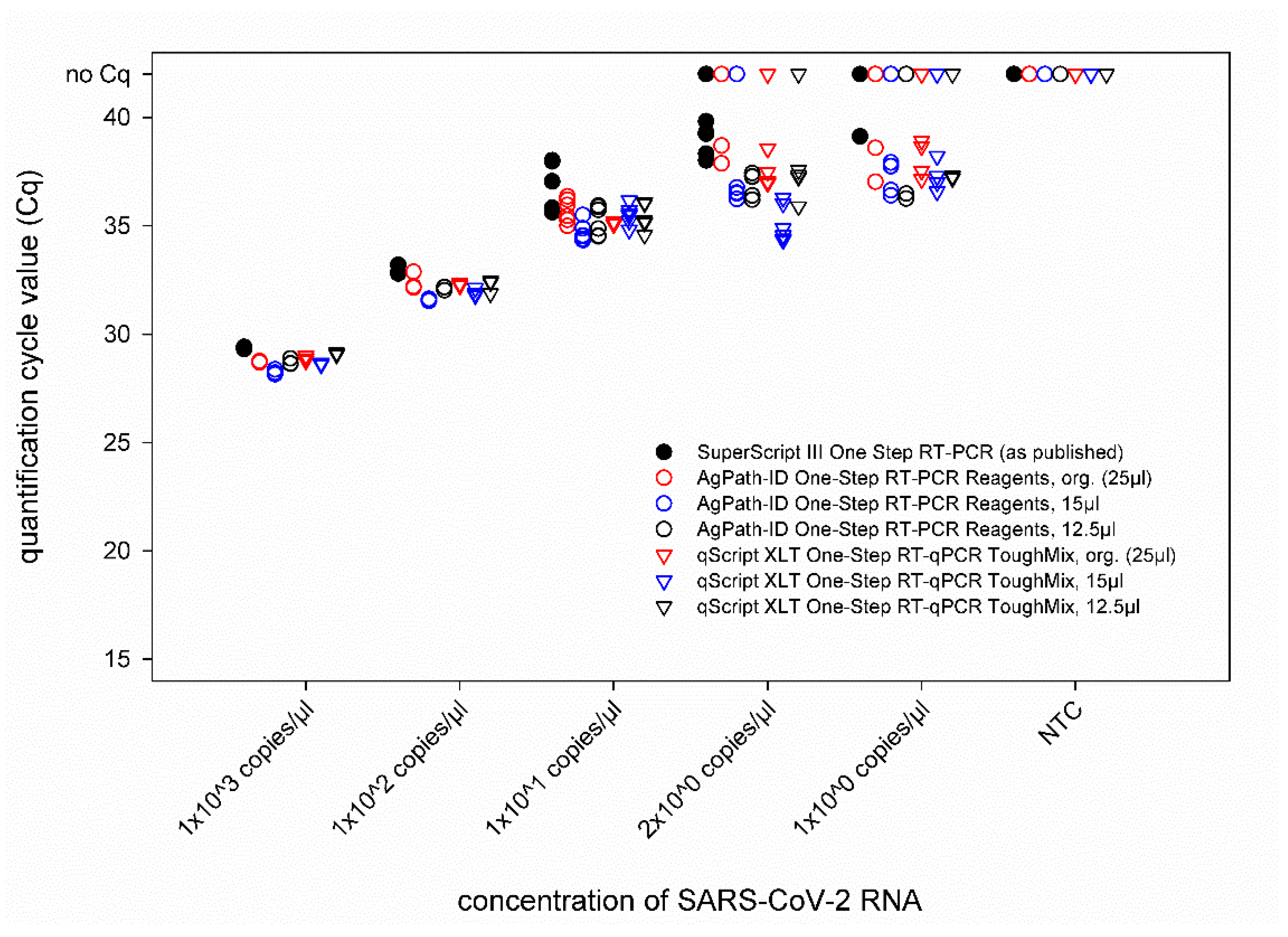
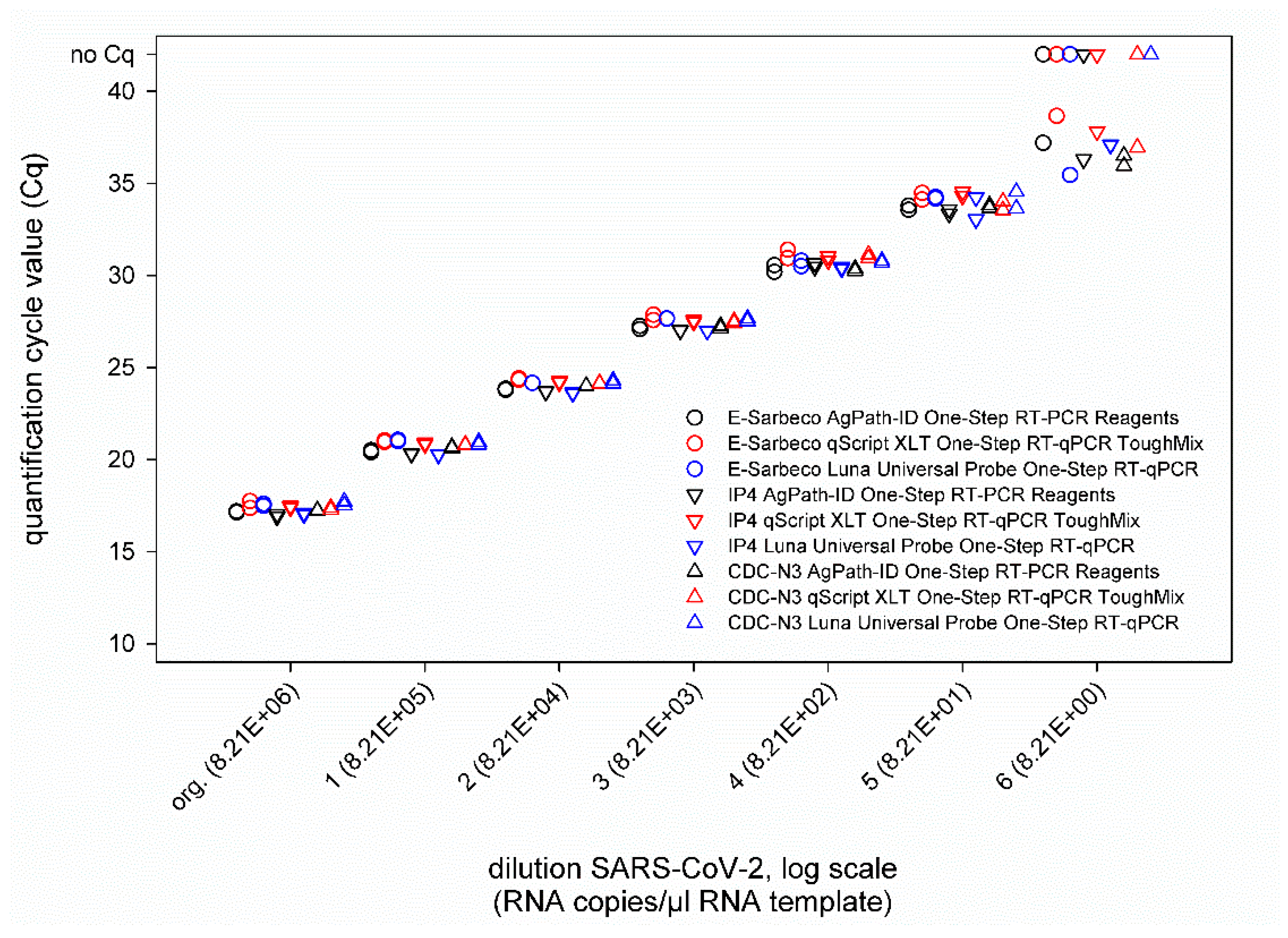
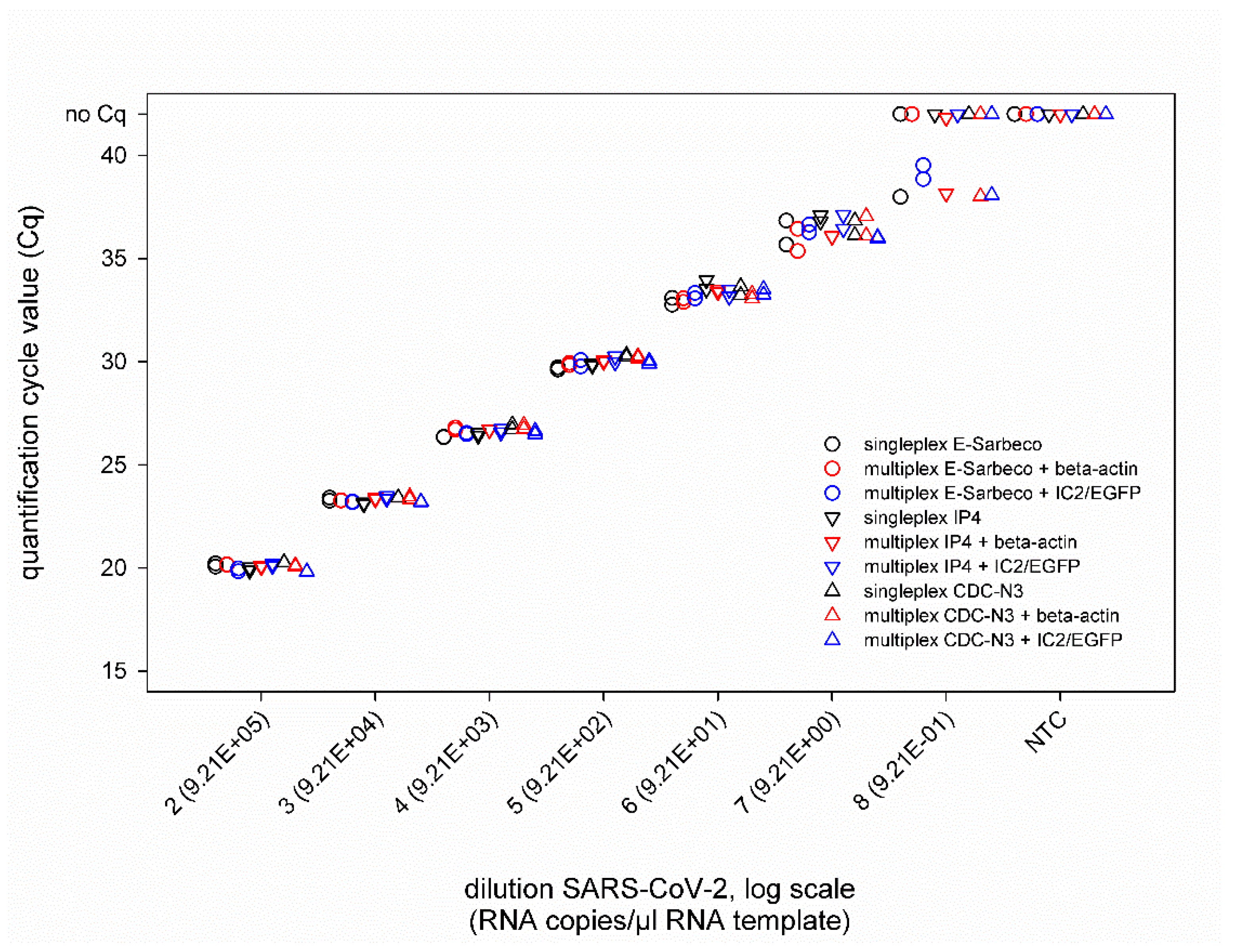
3.1. Volume Reduction of Reagents to 12.5 µL and Type of Used PCR Chemistry Did Not Influence the PCR Sensitivity
3.2. Diagnostic Performance of the Optimized Real-Time PCR Protocols with Clinical Samples
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Pneumonia of Unknown Cause—China. 2020. Available online: https://www.who.int/csr/don/05-january-2020-pneumonia-of-unkown-cause-china (accessed on 16 May 2020).
- WHO. Covid-19 Strategy Update—14 April 2020. Available online: https://www.who.int/publications-detail/covid-19-strategy-update---14-april-2020 (accessed on 16 May 2020).
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track covid-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Lau, E.H.Y.; Wu, P.; Deng, X.; Wang, J.; Hao, X.; Lau, Y.C.; Wong, J.Y.; Guan, Y.; Tan, X.; et al. Temporal dynamics in viral shedding and transmissibility of covid-19. Nat. Med. 2020, 26, 672–675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaur, S.; Bherwani, H.; Gulia, S.; Vijay, R.; Kumar, R. Understanding covid-19 transmission, health impacts and mitigation: Timely social distancing is the key. Environ. Dev. Sustain. 2020, 23, 6681–6697. [Google Scholar] [CrossRef] [PubMed]
- Islam, N.; Sharp, S.J.; Chowell, G.; Shabnam, S.; Kawachi, I.; Lacey, B.; Massaro, J.M.; D’Agostino, R.B., Sr.; White, M. Physical distancing interventions and incidence of coronavirus disease 2019: Natural experiment in 149 countries. BMJ 2020, 370, m2743. [Google Scholar] [CrossRef]
- Li, Y.; Campbell, H.; Kulkarni, D.; Harpur, A.; Nundy, M.; Wang, X.; Nair, H. The temporal association of introducing and lifting non-pharmaceutical interventions with the time-varying reproduction number (r) of Sars-CoV-2: A modelling study across 131 countries. Lancet Infect. Dis. 2020, 21, 193–202. [Google Scholar] [CrossRef]
- Hasell, J.; Ortiz-Ospina, E.; Mathieu, E.; Ritchie, H.; Beltekian, D.; Macdonald, B.; Roser, M. Coronavirus (Covid-19) Testing. Our World in Data. 2020. Available online: https://ourworldindata.org/coronavirus-testing (accessed on 16 May 2020).
- Lorusso, A.; Calistri, P.; Mercante, M.T.; Monaco, F.; Portanti, O.; Marcacci, M.; Camma, C.; Rinaldi, A.; Mangone, I.; Di Pasquale, A.; et al. A “one-health” approach for diagnosis and molecular characterization of Sars-CoV-2 in Italy. One Health 2020, 10, 100135. [Google Scholar] [CrossRef]
- Bulterys, P.L.; Garamani, N.; Stevens, B.; Sahoo, M.K.; Huang, C.; Hogan, C.A.; Zehnder, J.; Pinsky, B.A. Comparison of a laboratory-developed test targeting the envelope gene with three nucleic acid amplification tests for detection of Sars-CoV-2. J. Clin. Virol. 2020, 129, 104427. [Google Scholar] [CrossRef]
- Park, M.; Won, J.; Choi, B.Y.; Lee, C.J. Optimization of primer sets and detection protocols for Sars-CoV-2 of coronavirus disease 2019 (Covid-19) using PCR and real-time PCR. Exp. Mol. Med. 2020, 52, 963–977. [Google Scholar] [CrossRef]
- WHO. Coronavirus Disease (Covid-19) Technical Guidance: Laboratory Testing for 2019-ncov in Humans. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/laboratory-guidance (accessed on 16 May 2020).
- Muenchhoff, M.; Mairhofer, H.; Nitschko, H.; Grzimek-Koschewa, N.; Hoffmann, D.; Berger, A.; Rabenau, H.; Widera, M.; Ackermann, N.; Konrad, R.; et al. Multicentre comparison of quantitative PCR-based assays to detect Sars-CoV-2, Germany, March 2020. Eurosurveillance 2020, 25, 2001057. [Google Scholar] [CrossRef]
- Iglói, Z.; Leven, M.; Abdel-Karem Abou-Nouar, Z.; Weller, B.; Matheeussen, V.; Coppens, J.; Koopmans, M.; Molenkamp, R. Comparison of commercial realtime reverse transcription PCR assays for the detection of Sars-CoV-2. J. Clin. Virol. 2020, 129, 104510. [Google Scholar] [CrossRef] [PubMed]
- Vogels, C.B.F.; Brito, A.F.; Wyllie, A.L.; Fauver, J.R.; Ott, I.M.; Kalinich, C.C.; Petrone, M.E.; Casanovas-Massana, A.; Catherine Muenker, M.; Moore, A.J.; et al. Analytical sensitivity and efficiency comparisons of Sars-CoV-2 RT-qPCR primer-probe sets. Nat. Microbiol. 2020, 5, 1299–1305. [Google Scholar] [CrossRef] [PubMed]
- Mögling, R.; Meijer, A.; Berginc, N.; Bruisten, S.; Charrel, R.; Coutard, B.; Eckerle, I.; Enouf, V.; Hungnes, O.; Korukluoglu, G.; et al. Delayed laboratory response to covid-19 caused by molecular diagnostic contamination. Emerg. Infect. Dis. 2020, 26, 1944. [Google Scholar] [CrossRef] [PubMed]
- Wernike, K.; Keller, M.; Conraths, F.J.; Mettenleiter, T.C.; Groschup, M.H.; Beer, M. Pitfalls in Sars-CoV-2 PCR diagnostics. Transbound. Emerg. Dis. 2020, 68, 253–257. [Google Scholar] [CrossRef]
- Hoffmann, B.; Depner, K.; Schirrmeier, H.; Beer, M. A universal heterologous internal control system for duplex real-time RT-PCR assays used in a detection system for pestiviruses. J. Virol. Methods 2006, 136, 200–209. [Google Scholar] [CrossRef] [PubMed]
- Kralik, P.; Ricchi, M. A basic guide to real time PCR in microbial diagnostics: Definitions, parameters, and everything. Front. Microbiol. 2017, 8, 108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.K.W.; Bleicker, T.; Brunink, S.; Schneider, J.; Schmidt, M.L.; et al. Detection of 2019 novel coronavirus (2019-ncov) by real-time RT-PCR. Eurosurveillance 2020, 25, 2000045. [Google Scholar] [CrossRef] [Green Version]
- Wernike, K.; Hoffmann, B.; Kalthoff, D.; König, P.; Beer, M. Development and validation of a triplex real-time PCR assay for the rapid detection and differentiation of wild-type and glycoprotein E-deleted vaccine strains of bovine herpesvirus type 1. J. Virol. Methods 2011, 174, 77–84. [Google Scholar] [CrossRef]
- Griffin, S. Covid-19: Second wave death rate is doubling fortnightly but is lower and slower than in March. BMJ 2020, 371, m4092. [Google Scholar] [CrossRef]
- Grech, V.; Cuschieri, S. Covid-19: A global and continental overview of the second wave and its (relatively) attenuated case fatality ratio. Early Hum. Dev. 2020, 105211. [Google Scholar] [CrossRef]
- ProMED-Mail. Covid-19 Update (232): South Africa, USA Delta var., India, Israel, Who, Global. Archive Number: 20210706.8499538. 2021. Available online: Http://www.Promedmail.Org (accessed on 6 July 2021).
- Fereidouni, S.R.; Harder, T.C.; Gaidet, N.; Ziller, M.; Hoffmann, B.; Hammoumi, S.; Globig, A.; Starick, E. Saving resources: Avian influenza surveillance using pooled swab samples and reduced reaction volumes in real-time RT-PCR. J. Virol. Methods 2012, 186, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Batten, C.A.; Sanders, A.J.; Bachanek-Bankowska, K.; Bin-Tarif, A.; Oura, C.A. Bluetongue virus: European community proficiency test (2007) to evaluate ELISA and RT-PCR detection methods with special reference to pooling of samples. Vet. Microbiol. 2009, 135, 380–383. [Google Scholar] [CrossRef] [PubMed]
- Flannery, J.; Rajko-Nenow, P.; Hicks, H.; Hill, H.; Gubbins, S.; Batten, C. Evaluating the most appropriate pooling ratio for EDTA blood samples to detect bluetongue virus using real-time RT-PCR. Vet. Microbiol. 2018, 217, 58–63. [Google Scholar] [CrossRef]
- Kennedy, J.A.; Mortimer, R.G.; Powers, B. Reverse transcription-polymerase chain reaction on pooled samples to detect bovine viral diarrhea virus by using fresh ear-notch-sample supernatants. J. Vet. Diagn. Investig. 2006, 18, 89–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hogan, C.A.; Sahoo, M.K.; Pinsky, B.A. Sample pooling as a strategy to detect community transmission of Sars-CoV-2. JAMA 2020, 323, 1967–1969. [Google Scholar] [CrossRef] [Green Version]
- Aragón-Caqueo, D.; Fernández-Salinas, J.; Laroze, D. Optimization of group size in pool testing strategy for Sars-CoV-2: A simple mathematical model. J. Med. Virol. 2020, 92, 1988–1994. [Google Scholar] [CrossRef]
- Ben-Ami, R.; Klochendler, A.; Seidel, M.; Sido, T.; Gurel-Gurevich, O.; Yassour, M.; Meshorer, E.; Benedek, G.; Fogel, I.; Oiknine-Djian, E.; et al. Large-scale implementation of pooled RNA extraction and RT-PCR for Sars-CoV-2 detection. Clin. Microbiol. Infect. 2020, 26, 1248–1253. [Google Scholar] [CrossRef]
- Torres, I.; Albert, E.; Navarro, D. Pooling of nasopharyngeal swab specimens for Sars-CoV-2 detection by RT-PCR. J. Med. Virol. 2020. [Google Scholar] [CrossRef]
- Wacharapluesadee, S.; Kaewpom, T.; Ampoot, W.; Ghai, S.; Khamhang, W.; Worachotsueptrakun, K.; Wanthong, P.; Nopvichai, C.; Supharatpariyakorn, T.; Putcharoen, O.; et al. Evaluating the efficiency of specimen pooling for PCR-based detection of covid-19. J. Med. Virol. 2020, 92, 2193–2199. [Google Scholar] [CrossRef]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with covid-19-related death using opensafely. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef]
- Mallapaty, S. The coronavirus is most deadly if you are older and male—New data reveal the risks. Nature 2020, 585, 16–17. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Ruan, F.; Huang, M.; Liang, L.; Huang, H.; Hong, Z.; Yu, J.; Kang, M.; Song, Y.; Xia, J.; et al. Sars-CoV-2 viral load in upper respiratory specimens of infected patients. N. Engl. J. Med. 2020, 382, 1177–1179. [Google Scholar] [CrossRef] [PubMed]
- Weiss, A.; Jellingsø, M.; Sommer, M.O.A. Spatial and temporal dynamics of Sars-CoV-2 in covid-19 patients: A systematic review and meta-analysis. EBioMedicine 2020, 58, 102916. [Google Scholar] [CrossRef] [PubMed]
- Wölfel, R.; Corman, V.M.; Guggemos, W.; Seilmaier, M.; Zange, S.; Müller, M.A.; Niemeyer, D.; Jones, T.C.; Vollmar, P.; Rothe, C.; et al. Virological assessment of hospitalized patients with covid-2019. Nature 2020, 581, 465–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, C.G.; Lee, K.M.; Hsiao, M.J.; Yang, S.L.; Huang, P.N.; Gong, Y.N.; Hsieh, T.H.; Huang, P.W.; Lin, Y.J.; Liu, Y.C.; et al. Culture-based virus isolation to evaluate potential infectivity of clinical specimens tested for Covid-19. J. Clin. Microbiol. 2020, 58, e01068-20. [Google Scholar] [CrossRef]
- Cevik, M.; Kuppalli, K.; Kindrachuk, J.; Peiris, M. Virology, transmission, and pathogenesis of Sars-CoV-2. BMJ 2020, 371, m3862. [Google Scholar] [CrossRef]
- Van Kampen, J.J.A.; van de Vijver, D.; Fraaij, P.L.A.; Haagmans, B.L.; Lamers, M.M.; Okba, N.; van den Akker, J.P.C.; Endeman, H.; Gommers, D.; Cornelissen, J.J.; et al. Duration and key determinants of infectious virus shedding in hospitalized patients with coronavirus disease-2019 (covid-19). Nat. Commun. 2021, 12, 267. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Reaction Step | SuperScript III One Step RT-PCR Kit | AgPath-ID One-Step RT-PCR Reagents Kit | qScript XLT One-Step RT-qPCR ToughMix Kit | Luna® Universal Probe One-Step RT-qPCR Kit |
|---|---|---|---|---|
| reverse transcription | 55 °C for 20 min | 45 °C for 10 min | 50 °C for 10 min | 55 °C for 10 min |
| PCR initial activation | 95 °C for 3 min | 95 °C for 10 min | 95 °C for 1 min | 95 °C for 1 min |
| three step cycling (42 cycles): | ||||
| denaturation | 95 °C for 15 s | 95 °C for 15 s | 95 °C for 15 s | 95 °C for 10 s |
| annealing | 58 °C for 30 s | 57 °C for 20 s | 57 °C for 20 s | 57 °C for 20 s |
| extension | (combined with annealing) | 72 °C for 20 s | 68 °C for 30 s | 68 °C for 30 s |
| Sample Material | E-Sarbeco | IP4 | CDC-N3 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SARS-CoV-2 | Beta-Actin | SARS-CoV-2 | IC2/EGFP | SARS-CoV-2 | Beta-Actin | SARS-CoV-2 | IC2/EGFP | SARS-CoV-2 | Beta-Actin | SARS-CoV-2 | IC2/EGFP | |
| human pharyngeal swab (n = 73) | neg. | 28.8 ± 3.0/ 31.3 ± 4.9 1 | neg. | 23.9 ± 0.1/ 24.6 ± 0.2 | neg. | 29.7 ± 3.1/ 30.5 ± 2.8 | neg. | 24.4 ± 0.2/ 24.8 ± 0.1 | neg. | 28.5 ± 3.1/ 29.9 ± 3.4 2 | neg. | 24.6 ± 0.2/ 23.8 ± 0.2 |
| human pharyngeal swab #74 | 23.6/23.8 | 28.3/29.4 | 24.3/24.0 | 25.6/26.2 | 23.9/24.1 | 28.9/31.4 | 24.4/24.2 | 26.0/27.1 | 24.4/23.5 | 28.1/29.4 | 24.2/23.5 | 25.3/24.3 |
| human pharyngeal swab #75 | 33.9/34.4 | 29.4/30.8 | 35.6/34.5 | 25.7/25.9 | 35.0/36.0 | 29.6/31.5 | 34.0/33.8 | 25.7/26.7 | 35.7/33.1 | 29.2/30.1 | 34.9/33.5 | 25.1/24.1 |
| human pharyngeal swab #76 | 27.5/28.1 | 27.2/28.9 | 28.4/28.1 | 25.7/26.1 | 27.8/28.0 | 27.5/29.5 | 28.2/28.0 | 25.5/26.6 | 28.5/27.3 | 27.1/28.2 | 28.4/27.6 | 24.8/24.1 |
| human pharyngeal swab #77 | 25.1/25.1 | 34.4/36.9 | 25.4/25.2 | 25.7/26.2 | 24.7/24.2 | 34.1/36.0 | 25.0/25.1 | 25.7/27.0 | 25.3/24.2 | 35.2/neg. | 25.1/24.4 | 24.8/24.1 |
| human pharyngeal swab #78 | 24.2/24.0 | 29.0/30.4 | 25.0/24.3 | 25.7/26.2 | 24.1/24.1 | 29.6/31.4 | 24.3/24.2 | 25.5/26.7 | 24.8/23.8 | 28.2/29.8 | 24.5/24.0 | 24.8/24.1 |
| human pharyngeal swab #79 | neg./neg. | 32.5/34.1 | neg./37.1 | 25.7/26.1 | neg./neg. | 32.5/35.1 | neg./neg. | 25.5/26.5 | neg./neg. | 31.5/35.4 | neg./neg. | 24.8/24.1 |
| human pharyngeal swab #80 | neg./37.3 | 32.0/34.4 | neg./neg. | 25.4/26.2 | neg./neg. | 32.6/34.9 | neg./37.4 | 25.4/26.5 | 36.6/neg. | 32.2/34.4 | neg./neg. | 25.0/23.9 |
| human pharyngeal swab #81 | 26.2/26.1 | 30.4/31.8 | 26.8/26.3 | 25.6/26.1 | 26.3/26.2 | 31.2/32.8 | 26.3/26.3 | 25.3/26.6 | 26.7/25.6 | 30.1/31.8 | 26.4/25.5 | 24.8/23.7 |
| human pharyngeal swab #82 | 28.2/28.7 | 33.4/35.6 | 28.2/28.8 | 25.3/26.1 | 28.9/28.9 | 34.4/35.6 | 28.6/28.8 | 25.5/26.6 | 28.5/27.6 | 33.3/neg. | 28.3/27.2 | 25.3/24.1 |
| human pharyngeal swab #83 | 29.4/29.4 | 31.3/33.1 | 29.9/29.6 | 25.8/26.3 | 29.3/29.5 | 31.7/33.7 | 29.4/29.4 | 26.0/26.9 | 30.2/28.6 | 30.9/32.8 | 29.5/28.5 | 25.2/24.1 |
| human pharyngeal swab #84 | neg./36.2 | 32.9/35.3 | neg./neg. | 25.8/26.2 | 37.0/37.2 | 33.7/35.5 | neg./neg. | 25.9/26.5 | neg./neg. | 33.8/neg. | 36.59/neg. | 24.8/24.0 |
| human pharyngeal swab #85 | 31.5/31.1 | 31.7/34.4 | 31.8/31.9 | 25.8/26.1 | 31.4/31.5 | 32.5/34.3 | 31.4/31.5 | 25.6/26.7 | 31.8/30.7 | 31.5/33.0 | 31.4/30.4 | 24.8/24.1 |
| human pharyngeal swab #86 | 31.7/31.7 | 30.1/31.2 | 32.0/31.6 | 25.7/26.2 | 31.7/21.1 | 29.9/31.7 | 31.3/31.7 | 25.6/26.8 | 31.5/30.2 | 29.3/30.5 | 31.7/30.4 | 24.9/24.1 |
| human pharyngeal swab #87 | 36.8/36.1 | 32.7/34.6 | 34.7/35.5 | 25.6/26.0 | 35.0/35.1 | 33.4/35.1 | 35.7/35.0 | 25.6/26.3 | 38.1/35.8 | 32.6/34.5 | 35.0/neg. | 24.8/23.8 |
| human pharyngeal swab #88 | 29.3/29.3 | 30.3/31.7 | 29.6/29.6 | 25.5/25.9 | 29.4/29.3 | 31.0/32.9 | 29.4/29.3 | 25.5/26.5 | 30.1/28.3 | 30.2/31.3 | 29.8/28.3 | 24.8/23.7 |
| human pharyngeal swab #89 | 30.1/31.1 | 34.2/38.8 | 31.3/31.1 | 25.6/26.3 | 31.7/31.3 | 34.1/36.4 | 30.8/31.1 | 25.1/26.6 | 31.2/30.1 | 33.8/neg. | 30.7/29.5 | 24.8/23.8 |
| human pharyngeal swab #90 | 26.0/26.2 | 28.8/30.0 | 26.4/26.2 | 25.7/26.0 | 26.1/26.2 | 29.2/31.3 | 26.2/26.4 | 25.6/26.6 | 26.6/25.6 | 28.6/27.8 | 26.5/25.6 | 25.0/24.2 |
| human pharyngeal swab #91 | 30.1/30.3 | 28.0/29.3 | 30.5/30.1 | 26.0/26.2 | 30.2/30.3 | 28.0/30.1 | 30.1/30.1 | 25.6/26.8 | 30.0/28.7 | 27.3/28.4 | 29.7/28.5 | 24.8/24.2 |
| human pharyngeal swab #92 | 36.3/36.0 | 28.2/30.0 | neg./36.6 | 25.9/26.0 | 36.8/38.0 | 28.4/30.3 | neg./36.1 | 25.4/26.5 | 37.8/41.3 | 27.7/28.9 | neg./36.1 | 24.7/24.0 |
| human pharyngeal swab #93 | 27.5/27.4 | 32.1/34.1 | 27.9/27.5 | 25.7/26.1 | 27.2/27.3 | 32.9/34.8 | 27.3/27.3 | 25.4/26.5 | 28.0/27.0 | 32.0/34.6 | 27.5/27.0 | 24.9/24.0 |
| diagnostic specificity | 100.00%/ 100.00% | 100.00%/ 100.00% | 100.00%/ 100.00% | 100.00%/ 100.00% | 100.00%/ 100.00% | 100.00%/ 100.00% | ||||||
| diagnostic sensitivity | 85.00%/ 95.00% | 80.00%/ 90.00% | 90.00%/ 90.00% | 80.00%/ 90.00% | 90.00%/ 90.00% | 80.00%/ 95.00% | ||||||
| accuracy | 96.77%/ 98.92% | 95.70%/ 97.85% | 97.85%/ 97.85% | 95.70%/ 97.85 | 97.85%/ 97.85% | 95.70%/ 98.92% | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bock, S.; Hoffmann, B.; Beer, M.; Wernike, K. Saving Resources: SARS-CoV-2 Diagnostics by Real-Time RT-PCR Using Reduced Reaction Volumes. Diseases 2021, 9, 84. https://doi.org/10.3390/diseases9040084
Bock S, Hoffmann B, Beer M, Wernike K. Saving Resources: SARS-CoV-2 Diagnostics by Real-Time RT-PCR Using Reduced Reaction Volumes. Diseases. 2021; 9(4):84. https://doi.org/10.3390/diseases9040084
Chicago/Turabian StyleBock, Sabine, Bernd Hoffmann, Martin Beer, and Kerstin Wernike. 2021. "Saving Resources: SARS-CoV-2 Diagnostics by Real-Time RT-PCR Using Reduced Reaction Volumes" Diseases 9, no. 4: 84. https://doi.org/10.3390/diseases9040084
APA StyleBock, S., Hoffmann, B., Beer, M., & Wernike, K. (2021). Saving Resources: SARS-CoV-2 Diagnostics by Real-Time RT-PCR Using Reduced Reaction Volumes. Diseases, 9(4), 84. https://doi.org/10.3390/diseases9040084