
Cross-National Variations in COVID-19 Mortality: The Role of Diet, Obesity and Depression


Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources
- The crude mortality rate, defined as the number of deaths per 100,000 population. This indicator provides a broad index of the impact of COVID-19 on the general population as a whole in terms of mortality. It has been widely used in prior ecological research on factors associated with COVID-19 mortality [4,13]; however, it is significantly affected by the total population size (the denominator), as well as local practices in attributing deaths to COVID-19 [48];
- The case-fatality ratio, defined as the ratio of deaths to infections and expressed as a percentage. This indicator provides an estimate of what proportion of patients with COVID-19 will have a fatal outcome. This index has also been used extensively in ecological studies of the COVID-19 pandemic [6,7] and has the advantage of not being directly affected by population size. However, it is significantly affected by the number of tests carried out in the general populations; low-income countries may have artificially high case-fatality ratios because they lack the resources to test asymptomatic or mild cases [13,48].
2.2. Measurement of Potential Confounders
- National life expectancy, in view of the robust association between advanced age and COVID-19 mortality. Data on this variable was obtained from the official statistics of the World Bank [53];
- Estimated prevalence of diabetes mellitus, as this condition is independently associated with COVID-19 mortality and is often comorbid with both depression and obesity [54]. Data on this variable was obtained from the aggregates of the International Diabetes Federation and Diabetes Atlas data, available at the World Bank website [55];
2.3. Data Analyses
3. Results
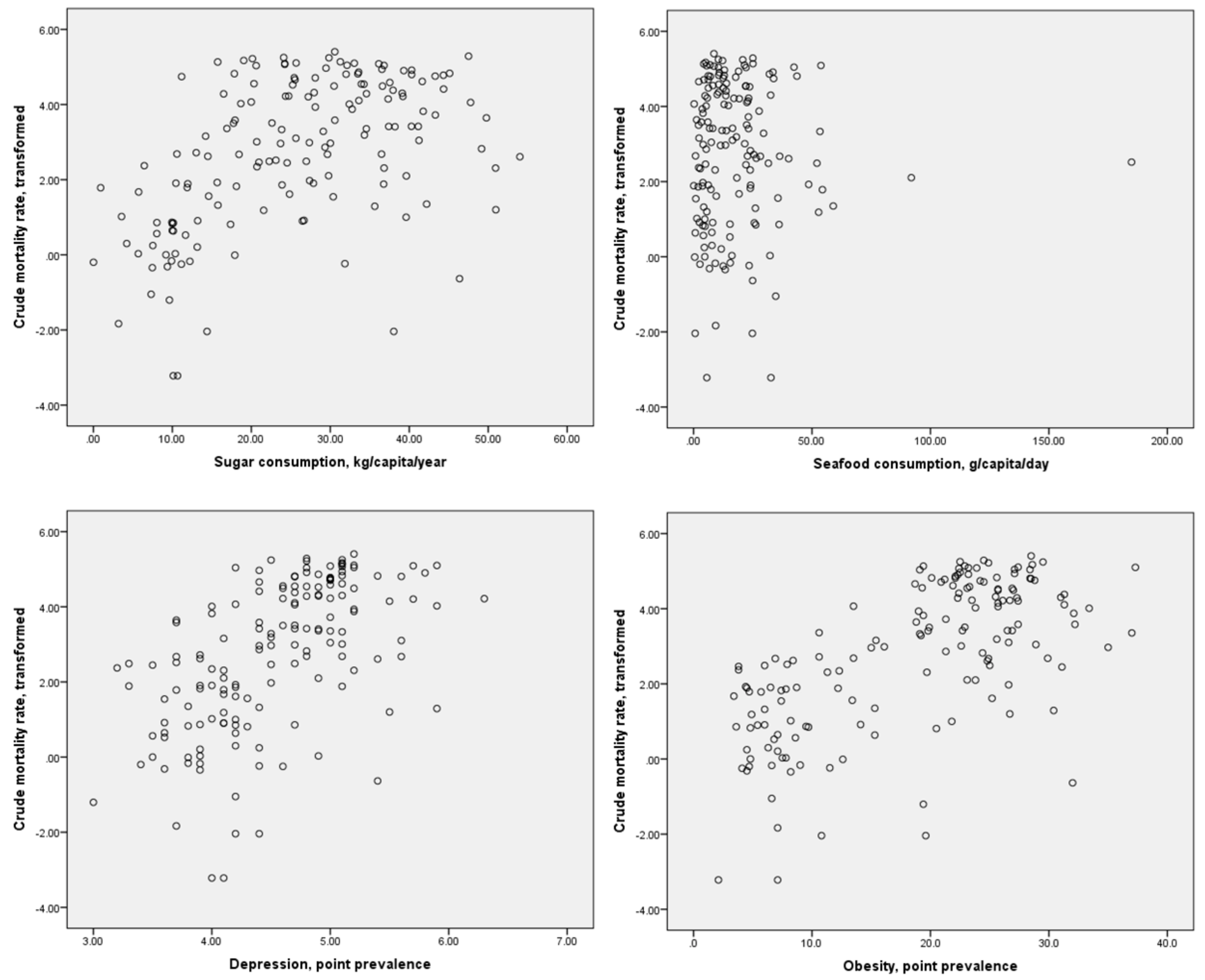
3.1. Bivariate Analyses
3.2. Analyses of Potential Confounders
3.3. Multivariate Analysis
3.4. Exploration of the Effect of Outliers, and of Possible Non-Linear Relationships
4. Discussion
4.1. Mechanisms Linking Depression and Obesity with COVID-19 Mortality
4.2. Diet as an Indirect Mediator of Mortality in COVID-19
4.3. Implications for Preventive and Mitigation Strategies
4.4. Methodological Issues and Limitations
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Flook, M.; Jackson, C.; Vasileiou, E.; Simpson, C.R.; Muckian, M.D.; Agrawal, U.; McCowan, C.; Jia, Y.; Murray, J.L.K.; Ritchie, L.D.; et al. Informing the public health response to COVID-19: A systematic review of risk factors for disease, severity, and mortality. BMC Infect. Dis. 2021, 21, 342. [Google Scholar] [CrossRef] [PubMed]
- Rajgor, D.D.; Lee, M.H.; Archuleta, S.; Bagdasarian, N.; Quek, S.C. The many estimates of the COVID-19 case fatality rate. Lancet Infect. Dis. 2020, 20, 776–777. [Google Scholar] [CrossRef]
- Patel, U.; Malik, P.; Mehta, D.; Shah, D.; Kelkar, R.; Pinto, C.; Suprun, M.; Dhamoon, M.; Hennig, N.; Sacks, H. Early epidemiological indicators, outcomes, and interventions of COVID-19 pandemic: A systematic review. J. Glob. Health 2020, 10, 020506. [Google Scholar] [CrossRef]
- Al-Tawfiq, J.A.; Leonardi, R.; Fasoli, G.; Rigamonti, D. Prevalence and fatality rates of COVID-19: What are the reasons for the wide variations worldwide? Travel Med. Infect. Dis. 2020, 35, 101711. [Google Scholar] [CrossRef]
- Kranjac, A.W.; Kranjac, D. Decomposing differences in coronavirus disease 2019-related case-fatality rates across seventeen nations. Pathog. Glob. Health 2021, 115, 100–107. [Google Scholar] [CrossRef]
- Pan, J.; St Pierre, J.M.; Pickering, T.A.; Demirjian, N.L.; Fields, B.K.K.; Desai, B.; Gholamrezanezhad, A. Coronavirus disease 2019 (COVID-19): A modeling study of factors driving variation in case fatality rate by country. Int. J. Environ. Res. Public Health 2020, 17, 8189. [Google Scholar] [CrossRef] [PubMed]
- Okonji, E.F.; Okonji, O.C.; Mukumbang, F.C.; VanWyk, B. Understanding varying COVID-19 mortality rates reported in Africa compared to Europe, United States of America and Asia. Trop. Med. Int. Health 2021. [Google Scholar] [CrossRef]
- Challen, R.; Brooks-Pollock, E.; Read, J.M.; Dyson, L.; Tsaneva-Atanasova, K.; Danon, L. Risk of mortality in patients infected with SARS-CoV-2 variant of concern 202012.1: Matched cohort study. BMJ 2021, 372, n579. [Google Scholar] [CrossRef]
- Pati, A.; Padhi, S.; Panda, D.; Suvankar, S.; Panda, A.K. A cluster of differentiation (CD14) polymorphism (C159-T rs2569190) is associated with SARS-CoV-2 infection and mortality in the European population. J. Infect. Dis. 2021. [Google Scholar] [CrossRef]
- Lehrer, S.; Rheinstein, P.H. Homozygosity for rs17775810 minor allele associated with reduced mortality of COVID-19 in the UK Biobank Cohort. In Vivo 2021, 35, 965–968. [Google Scholar] [CrossRef] [PubMed]
- Booth, A.; Reed, A.B.; Ponzo, S.; Yassaee, A.; Aral, M.; Plans, D.; Labrique, A.; Mohan, D. Population risk factors for severe disease and mortality in COVID-19: A global systematic review and meta-analysis. PLoS ONE 2021, 16, e0247461. [Google Scholar] [CrossRef] [PubMed]
- Hashim, M.J.; Alsuwaidi, A.R.; Khan, G. Population risk factors for COVID-19 mortality in 93 countries. J. Epidemiol. Glob. Health 2020, 10, 204–208. [Google Scholar] [CrossRef] [PubMed]
- Xiang, G.; Xie, L.; Chen, Z.; Hao, S.; Fu, C.; Wu, Q.; Liu, X.; Li, S. Clinical risk factors for mortality of hospitalized patients with COVID-19: Systematic review and meta-analysis. Ann. Palliat. Med. 2021, 10, 2723–2735. [Google Scholar] [CrossRef]
- Lembo, R.; Landoni, G.; Cianfanelli, L.; Frontera, A. Air pollutants and SARS-CoV-2 in 33 European countries. Acta Biomed. 2021, 92, e2021166. [Google Scholar] [CrossRef]
- Gelfand, M.J.; Jackson, J.C.; Pan, X.; Nau, D.; Pieper, D.; Denison, E.; Dagher, M.; Van Lange, P.A.M.; Chiu, C.-Y.; Wang, M. The relationship between cultural tightness-looseness and COVID-19 cases and deaths: A global analysis. Lancet Planet. Health 2021, 5, e135–e144. [Google Scholar] [CrossRef]
- Castro, V.M.; Gunning, F.M.; McCoy, T.H.; Perlis, R.H. Mood disorders and outcomes of COVID-19 hospitalizations. Am. J. Psychiatry 2021. [Google Scholar] [CrossRef]
- Wang, Q.; Xu, R.; Volkow, N.D. Increased risk of COVID-19 infection and mortality in people with mental disorders: Analysis from electronic health records in the United States. World Psychiatry 2021, 20, 124–130. [Google Scholar] [CrossRef]
- Atkins, J.L.; Masoli, J.A.H.; Delgado, J.; Pilling, L.C.; Kuo, C.-L.; Kuchel, G.A.; Melzer, D. Preexisting comorbidities predicting COVID-19 and mortality in the UK Biobank cohort. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 11, 2224–2230. [Google Scholar] [CrossRef]
- Capoccia, K.; Odegard, P.S.; Letassy, N. Medication adherence with diabetes medication: A systematic review of the literature. Diabetes Educ. 2016, 42, 34–71. [Google Scholar] [CrossRef]
- Lin, C.-Y.; Hammash, M.; Miller, J.L.; Schrader, M.; Mudd-Martin, G.; Biddle, M.J.; Moser, D.K. Delay in seeking medical care for worsening heart failure symptoms: Predictors and association with cardiac events. Eur. J. Cardiovasc. Nurs. 2021. [Google Scholar] [CrossRef]
- Briggs, R.; Ward, M.; Kenny, R.A. The “wish to die” in later life: Prevalence, longitudinal course and mortality. Data from TILDA. Age Ageing 2021, 1–8. [Google Scholar] [CrossRef]
- Valkanova, V.; Ebmeier, K.P.; Allan, C.L. CRP, IL-6 and depression: A systematic review and meta-analysis of longitudinal studies. J. Affect. Disord. 2013, 150, 736–744. [Google Scholar] [CrossRef]
- Kohler, C.A.; Freitas, T.H.; Maes, M.; de Andrade, N.Q.; Liu, C.S.; Fernandes, B.S.; Stubbs, B.; Solmi, M.; Veronese, N.; Herrmann, N.; et al. Peripheral cytokine and chemokine alterations in depression: A meta-analysis of 82 studies. Acta Psychiatr. Scand. 2017, 135, 373–387. [Google Scholar] [CrossRef]
- Liu, T.; Zhong, S.; Liao, X.; Chen, J.; He, T.; Lai, S.; Jia, Y. A meta-analysis of oxidative stress markers in depression. PLoS ONE 2015, 10, e0138904. [Google Scholar] [CrossRef]
- Raison, C.L.; Miller, A.H. The evolutionary significance of depression in Pathogen Host Defense (PATHOS-D). Mol. Psychiatry 2013, 18, 15–37. [Google Scholar] [CrossRef]
- Ji, P.; Zhu, J.; Zhong, Z.; Li, H.; Pang, J.; Li, B.; Zhang, J. Association of elevated inflammatory markers and severe COVID-19: A meta-analysis. Medicine 2020, 99, e23315. [Google Scholar] [CrossRef]
- Hoong, C.W.S.; Hussain, I.; Aravamudan, V.M.; Phyu, E.E.; Lin, J.H.X.; Koh, H. Obesity is associated with poor COVID-19 outcomes: A systematic review and meta-analysis. Horm. Metab. Res. 2021, 53, 85–93. [Google Scholar] [CrossRef]
- Yang, J.; Ma, Z.; Lei, Y. A meta-analysis of the association between obesity and COVID-19. Epidemiol. Infect. 2020, 149, e11. [Google Scholar] [CrossRef]
- Du, Y.; Lv, Y.; Zha, W.; Zhou, N.; Hong, X. Association of body mass index (BMI) with critical COVID-19 and in-hospital mortality: A dose-response meta-analysis. Metabolism 2021, 117, 154373. [Google Scholar] [CrossRef]
- Sharma, J.R.; Yadav, U.C.S. COVID-19 severity in obese patients: Potential mechanisms and molecular targets for clinical intervention. Obes. Res. Clin. Pract. 2021, 15, 163–171. [Google Scholar] [CrossRef]
- Krams, I.A.; Joers, P.; Luoto, S.; Trakimas, G.; Lietuvietis, V.; Krams, R.; Kaminska, I.; Rantala, M.J.; Krama, T. The obesity paradox predicts the second wave of COVID-19 to be severe in Western countries. Int. J. Environ. Res. Public Health 2021, 18, 1029. [Google Scholar] [CrossRef]
- Gharipour, M.; Barekatain, M.; Sung, J.; Emami, N.; Sadeghian, L.; Dianatkhah, M.; Sarrafzadegan, N.; Jahanfar, S. The epigenetic overlap between obesity and mood disorders: A systematic review. Int. J. Mol. Sci. 2020, 21, 6758. [Google Scholar] [CrossRef]
- Britto, F.A.; Dumas, K.; Giorgetti-Peraldi, S.; Ollendorff, V.; Favier, F.B. Is REDD1 a metabolic double agent? Lessons from physiology and pathology. Am. J. Physiol. Cell. Physiol. 2020, 319, C807–C824. [Google Scholar] [CrossRef]
- Milano, W.; Ambrosio, P.; Carizzone, F.; De Biaiso, V.; Di Munzio, W.; Foia, M.G.; Capasso, A. Depression and obesity: Analysis of common biomarkers. Diseases 2020, 14, 23. [Google Scholar] [CrossRef]
- Mannan, M.; Mamun, A.; Doi, S.; Clavarino, A. Is there a bi-directional relationship between depression and obesity in adult men and women? Systematic review and bias-adjusted meta analysis. Asian J. Psychiatr. 2016, 21, 51–66. [Google Scholar] [CrossRef] [PubMed]
- Luoto, S.; Karlsson, H.; Krams, I.; Rantala, M.J. Depression subtyping based on evolutionary psychiatry: From reactive short-term mood change to depression. Brain. Behav. Immun. 2018, 69, 630. [Google Scholar] [CrossRef] [PubMed]
- Rantala, M.J.; Luoto, S.; Borraz-Leon, J.I.; Krams, I. Bipolar disorder: An evolutionary psychoneuroimmunological approach. Neurosci. Biobehav. Rev. 2021, 122, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Molendijk, M.; Molero, P.; Sanchez-Pedreno, F.O.; Van der Does, W.; Martinez-Gonzalez, M.A. Diet quality and depression risk: A systematic review and dose-response meta-analysis of prospective studies. J. Affect. Disord. 2018, 226, 346–354. [Google Scholar] [CrossRef]
- Heras-Gonzalez, L.; Latorre, J.A.; Martinez-Bebia, M.; Gimenez-Blasi, N.; Olea-Serrano, F.; Mariscal-Arcas, M. Sugar consumption in schoolchildren from southern Spain and influence on the prevalence of obesity. PLoS ONE 2020, 15, e0242602. [Google Scholar] [CrossRef]
- Bentley, R.A.; Ruck, D.J.; Fouts, H.N. U.S. obesity as delayed effect of excess sugar. Econ. Hum. Biol. 2020, 36, 100818. [Google Scholar] [CrossRef]
- Peet, M. International variations in the outcome of schizophrenia and the prevalence of depression in relation to national dietary practices: An ecological analysis. Br. J. Psychiatry 2004, 184, 404–408. [Google Scholar] [CrossRef]
- Westover, A.N.; Marangell, L.B. A cross-national relationship between sugar consumption and major depression? Depress. Anxiety 2002, 16, 118–120. [Google Scholar] [CrossRef]
- Yang, Y.; Kim, Y.; Je, Y. Fish consumption and risk of depression: Epidemiological evidence from prospective studies. Asia Pac. Psychiatry 2018, 10, e12335. [Google Scholar] [CrossRef]
- Ramel, A.; Martinez, J.A.; Kiely, M.; Bandarra, N.M.; Thorsdottir, I. Effects of weight loss and seafood consumption on inflammation parameters in young, overweight and obese European men and women during 8 weeks of energy restriction. Eur. J. Clin. Nutr. 2010, 64, 987–993. [Google Scholar] [CrossRef]
- Abdulah, D.M.; Hassan, A.B. Relation of dietary factors with infection and mortality rates of COVID-19 across the world. J. Nutr. Health Aging 2020, 24, 1011–1018. [Google Scholar] [CrossRef]
- Moscatelli, F.; Sessa, F.; Valenzano, A.; Polito, R.; Monda, V.; Cibelli, G.; Villano, I.; Pisanelli, D.; Perrella, M.; Daniele, A.; et al. COVID-19: Role of nutrition and supplementation. Nutrients 2021, 13, 976. [Google Scholar] [CrossRef]
- Corrao, G.; Rea, F.; Blangiardo, G.C. Lessons from COVID-19 mortality data across countries. J. Hypertens. 2021, 39, 856–860. [Google Scholar] [CrossRef]
- World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Bromet, E.; Andrade, L.H.; Hwang, I.; Sampson, N.A.; Alonso, J.; de Girolamo, G.; de Graaf, R.; Demyttenaere, K.; Hu, C.; Iwata, N.; et al. Cross-national epidemiology of DSM-IV major depressive episode. BMC Med. 2011, 9, 90. [Google Scholar] [CrossRef]
- World Health Organization. Prevalence of Obesity among Adults, BMI >=30 (Crude Estimate) (%). Available online: https://who.int/data/gho/indicators/indicator-details/GHO/prevalence-of-obesity-among-adults-bmi-=-30-(crude-estimate)-(-) (accessed on 21 April 2021).
- FAOSTAT–Food and Agricultural Organization of the United Nations. Available online: https://fao.org/faostat/en (accessed on 18 April 2021).
- The World Bank Data. Life Expectancy at Birth, Total (Years). Available online: https://data.worldbank.org/indicator/SP.DYN.LE00.IN (accessed on 18 April 2021).
- Egede, L.E.; Ellis, C. Diabetes and depression: Global perspectives. Diabetes Res. Clin. Pract. 2010, 87, 302–312. [Google Scholar] [CrossRef]
- The World Bank Data. Diabetes Prevalence (% of Population Ages 20 to 79). International Diabetes Federation, Diabetes Atlas. Available online: https://data.worldbank.org/indicator/SH.STA.DIAB.ZS (accessed on 18 April 2021).
- United Nations Development Programme. Human Development Report 2020. The Next Frontier: Human Development and the Anthropocene; United Nations Development Programme: New York, NY, USA, 2020. [Google Scholar]
- Konishi, K. Associations between healthy Japanese dietary patterns and depression in Japanese women. Public Health Nutr. 2020, 1–13. [Google Scholar] [CrossRef]
- Noaghiul, S.; Hibbeln, J.R. Cross-national comparisons of seafood consumption and rates of bipolar disorders. Am. J. Psychiatry 2003, 160, 2222–2227. [Google Scholar] [CrossRef]
- Naghshi, S.; Sadeghi, O.; Willett, W.C.; Esmaillzadeh, A. Dietary intake of total, animal, and plant products and risk of all cause, cardiovascular, and cancer mortality: Systematic review and dose-response meta-analysis of prospective cohort studies. BMJ 2020, 370, m2412. [Google Scholar] [CrossRef]
- Bayrak, M.; Cadirci, K. The associations of life quality, depression, and cognitive impairment with mortality in older adults with COVID-19: A prospective, observational study. Acta Clin. Belg. 2021, 1–8. [Google Scholar] [CrossRef]
- Diez-Quevedo, C.; Iglesias-Gonzalez, M.; Giralt-Lopez, M.; Rangil, T.; Sanagustin, D.; Moreira, M.; Lopez-Ramentol, M.; Ibanez-Caparros, A.; Loran, M.-E.; Bustos-Cardona, T.; et al. Mental disorders, psychopharmacological treatments, and mortality in 2150 COVID-19 Spanish inpatients. Acta Psychiatr. Scand. 2021. [Google Scholar] [CrossRef]
- Rush, G.; O’Donovan, A.; Nagle, L.; Conway, C.; McCrohan, A.; O’Farrelly, C.; Lucey, J.V.; Malone, K.M. Alteration of immune markers in a group of melancholic depressed patients and their response to electroconvulsive therapy. J. Affect. Disord. 2016, 205, 60–68. [Google Scholar] [CrossRef]
- Smith, K.J.; Au, B.; Ollis, L.; Schmitz, N. The association between C-reactive protein, interleukin-6 and depression among older adults in the community: A systematic review and meta-analysis. Exp. Gerontol. 2018, 102, 109–132. [Google Scholar] [CrossRef]
- Martinez-Cengotitabengoa, M.; Carrascon, L.; O’Brien, J.T.; Diaz-Gutierrez, M.-J.; Bermudez-Ampudia, C.; Sanada, K.; Arrasate, M.; Gonzalez-Pinto, A. Peripheral inflammatory parameters in late-life depression: A systematic review. Int. J. Mol. Sci. 2016, 17, 2022. [Google Scholar] [CrossRef]
- Mazza, M.G.; Lucchi, S.; Tringali, A.G.M.; Rossetti, A.; Botti, E.R.; Clerici, M. Neutrophil/lymphocyte ratio and platelet/lymphocyte ratio in mood disorders: A meta-analysis. Prog. Neuropsychopharmacol. Biol. Psychiatry 2018, 84, 229–236. [Google Scholar] [CrossRef]
- Euteneuer, F.; Dannehl, K.; Del Ray, A.; Engler, H.; Schedlowski, M.; Rief, W. Peripheral immune alterations in major depression: The role of subtypes and pathogenetic characteristics. Front. Psychiatry 2017, 8, 250. [Google Scholar] [CrossRef]
- Acar, E.; Demir, A.; Yildirim, B.; Kaya, M.G.; Gokcek, K. The role of hemogram parameters and CRP in predicting mortality in COVID-19 infection. Int. J. Clin. Pract. 2021, e14256. [Google Scholar] [CrossRef]
- Berenguer, J.; Borobia, A.M.; Ryan, P.; Rodriguez-Bano, J.; Bellon, J.M.; Jarrin, I.; Carratala, J.; Pachon, J.; Carcas, A.J.; Yllescas, M.; et al. Development and validation of a prediction model for 30-day mortality in hospitalized patients with COVID-19: The COVID-19 SEIMC score. Thorax 2021. [Google Scholar] [CrossRef] [PubMed]
- Schuch, F.; Vancampfort, D.; Firth, J.; Rosenbaum, S.; Ward, P.; Reichert, T.; Bagatini, N.C.; Bgeginski, R.; Stubbs, B. Physical activity and sedentary behavior in people with major depressive disorder: A systematic review and meta-analysis. J. Affect. Disord. 2017, 210, 139–150. [Google Scholar] [CrossRef] [PubMed]
- Quirk, S.E.; Williams, L.J.; O’Neil, A.; Pasco, J.A.; Jacka, F.N.; Housden, S.; Berk, M.; Brennan, S.L. The association between diet quality, dietary patterns and depression in adults: A systematic review. BMC Psychiatry 2013, 13, 175. [Google Scholar] [CrossRef]
- Hunt, G.E.; Malhi, G.S.; Lai, H.M.X.; Cleary, M. Prevalence of comorbid substance use in major depressive disorder in community and clinical settings, 1990-2019: Systematic review and meta-analysis. J. Affect. Disord. 2020, 266, 288–304. [Google Scholar] [CrossRef]
- Salgado-Aranda, R.; Perez-Castellano, N.; Nunez-Gil, I.; Orozco, A.J.; Torres-Esquivel, N.; Flores-Soler, J.; Chamaisse-Akari, A.; McInerney, A.; Vergara-Uzcategui, C.; Wang, L.; et al. Infleunce of baseline physical activity as a modifying factor on COVID-19 mortality: A single-center, retrospective study. Infect. Dis. Ther. 2021, 1–14. [Google Scholar] [CrossRef]
- Katon, W.J. Epidemiology and treatment of depression in patients with chronic medical illness. Dialogues Clin. Neurosci. 2011, 13, 7–23. [Google Scholar] [CrossRef]
- Mayston, R.; Lazarus, A.; Patel, V.; Abas, M.; Korgaonkar, P.; Paranjape, R.; Rodrigues, S.; Prince, M. Pathways to HIV testing and care in Goa, India: Exploring psychosocial barriers and facilitators using mixed methods. BMC Public Health 2016, 16, 765. [Google Scholar]
- Polacsek, M.; Boardman, G.H.; McCann, T.V. Help-seeking experiences of older adults with a diagnosis of moderate depression. Int. J. Ment. Health Nurs. 2019, 28, 278–287. [Google Scholar] [CrossRef]
- Arboleda-Florez, J.; Stuart, H. From sin to science: Fighting the stigmatization of mental illnesses. Can. J. Psychiatry 2012, 57, 457–463. [Google Scholar] [CrossRef]
- O’Rourke, R.W.; Lumeng, C.N. Pathways to severe COVID-19 for people with obesity. Obesity 2021, 29, 645–653. [Google Scholar] [CrossRef]
- Cheng, D.; Zhao, X.; Yang, S.; Cui, H.; Wang, G. Metabolomic signature between metabolically healthy overweight/obese and metabolically unhealthy overweight/obese: A systematic review. Diabetes Metab. Syndr. Obes. 2021, 14, 991–1010. [Google Scholar] [CrossRef]
- Hamjane, N.; Benyahya, F.; Nourouti, N.G.; Mechita, M.B.; Barakat, A. Cardiovascular diseases and metabolic abnormalities associated with obesity: What is the role of inflammatory responses? A systematic review. Microvasc. Res. 2020, 131, 104023. [Google Scholar] [CrossRef]
- Krams, I.A.; Luoto, S.; Rantala, M.J.; Joers, P.; Krama, T. COVID-19: Fat, obesity, inflammation, ethnicity, and sex differences. Pathogens 2020, 9, 887. [Google Scholar] [CrossRef]
- Ne, J.Y.A.; Cai, T.Y.; Celermajer, D.S.; Caterson, I.D.; Gill, T.; Lee, C.M.Y.; Skilton, M.R. Obesity, arterial function and arterial structure–A systematic review and meta-analysis. Obes. Sci. Pract. 2017, 3, 171–184. [Google Scholar] [CrossRef]
- Scoccia, A.; Gallone, G.; Cereda, A.; Palmisano, A.; Vignale, D.; Leone, R.; Nicoletti, V.; Gnasso, C.; Monello, A.; Khokhar, A.; et al. Impact of clinical and subclinical coronary artery disease as assessed by coronary artery calcium in COVID-19. Atherosclerosis 2021. [Google Scholar] [CrossRef]
- Wolf, M.; Alladina, J.; Navarrete-Welton, A.; Shoults, B.; Brait, K.; Ziehr, D.; Malhotra, A.; Hardin, C.C.; Hibbert, K.A. Obesity and critical illness in COVID-19: Respiratory pathophysiology. Obesity 2021. [Google Scholar] [CrossRef]
- Schavemaker, R.; Schultz, M.J.; Lagrand, W.K.; van Slobbe-Biljsma, E.R.; Neto, A.S.; Paulus, F. Associations of body mass index with ventilation management and clinical outcomes in invasively ventilated patients with ARDS related to COVID-19–Insights from the PRoVENT-COVID study. J. Clin. Med. 2021, 10, 1176. [Google Scholar] [CrossRef]
- Spooner, C.; Jayasinghe, U.W.; Faruqi, N.; Stocks, N.; Harris, M.F. Predictors of weight stigma experienced by middle-older aged, general-practice patients with obesity in disadvantaged areas of Australia: A cross-sectional study. BMC Public Health 2018, 18, 640. [Google Scholar] [CrossRef]
- Lasikiewicz, N.; Myrissa, K.; Hoyland, A.; Lawton, C.L. Psychological benefits of weight loss following behavioural and/or dietary weight loss interventions. A systematic research review. Appetite 2014, 72, 123–137. [Google Scholar] [CrossRef]
- da Silva Borges, D.; Fernandes, R.; Thives Mello, A.; da Silva Fontoura, E.; Soares Dos Santos, A.R.; Santos de Moraes Trinidade, E.B. Prebiotics may reduce serum concentrations of C-reactive protein and ghrelin in overweight and obese adults: A systematic review and meta-analysis. Nutr. Rev. 2020, 78, 235–248. [Google Scholar] [CrossRef] [PubMed]
- Kamyari, N.; Soltanian, A.R.; Mahjub, H.; Moghimbeigi, A. Diet, nutrition, obesity, and their implications for COVID-19 mortality: Development of a marginalized two-part model for semicontinuous data. JMIR Public Health Surveill. 2021, 26, e22717. [Google Scholar] [CrossRef] [PubMed]
- De Bandt, J.-P.; Monin, C. Obesity, nutrients and the immune system in the era of COVID-19. Nutrients 2021, 13, 610. [Google Scholar] [CrossRef] [PubMed]
- Grannell, A.; le Roux, C.W.; McGillicuddy, D. “I am terrified of something happening to me”. The lived experience of people with obesity during the COVID-19 pandemic. Clin. Obes. 2020, 10, e12406. [Google Scholar] [CrossRef]
- Al-Dmour, H.; Masa’deh, R.; Salman, A.; Abuhashesh, M.; Al-Dmour, R. Influence of social media platforms of public health protection against the COVID-19 pandemic via the mediating effects of public health awareness and behavioural changes: Integrated model. J. Med. Internet. Res. 2020, 22, e19996. [Google Scholar] [CrossRef]
- Joisten, C.; Kossow, A.; Book, J.; Broichhaus, L.; Daum, M.; Eisenburger, N.; Fabrice, A.; Feddern, S.; Gehlhar, A.; Graf, A.C.; et al. How to manage quarantine-adherence, psychosocial consequences, coping strategies and lifestyle of patients with COVID-19 and their confirmed contacts: Study protocol of the CoCo-Fakt surveillance study, Cologne, Germany. BMJ Open 2021, 11, e048001. [Google Scholar] [CrossRef]
- Hoertel, N.; Sanchez-Rico, M.; Vernet, R.; Beeker, N.; Jannot, A.-S.; Neuraz, A.; Salamanca, E.; Paris, N.; Daniel, C.; Gramfort, A.; et al. Association between antidepressant use and reduced risk of intubation or death in hospitalized patients with COVID-19: Results from an observational study. Mol. Psychiatry 2021. [Google Scholar] [CrossRef]
- Zimniak, M.; Kirschner, L.; Hilpert, H.; Geiger, N.; Danov, O.; Oberwinkler, H.; Steinke, M.; Sewald, K.; Seibel, J.; Bodem, J. The serotonin reuptake inhibitor fluoxetine inhibits SARS-CoV-2 in human lung tissue. Sci. Rep. 2021, 11, 5890. [Google Scholar] [CrossRef]
- Lenze, E.J.; Mattar, C.; Zorumski, C.F.; Stevens, A.; Schweiger, J.; Nicol, G.E.; Miller, J.P.; Yang, L.; Yingling, M.; Avidan, M.S.; et al. Fluvoxamine vs. placebo and clinical deterioration in outpatients with symptomatic COVID-19: A randomized clinical trial. JAMA 2020, 324, 2292–2300. [Google Scholar] [CrossRef]
- Nna, V.U.; McGrowder, D.; Nwokocha, C. Nutraceutical management of metabolic syndrome as a palliative and a therapeutic to coronavirus disease (COVID) crisis. Arch. Physiol. Biochem. 2021, 1–20. [Google Scholar] [CrossRef]
- Townsend, M.J.; Kyle, T.K.; Stanford, F.C. COVID-19 vaccination and obesity: Optimism and challenges. Obesity 2021, 29, 634–635. [Google Scholar] [CrossRef]
- Madison, A.A.; Shrout, M.R.; Renna, M.E.; Kiecolt-Glaser, J.K. Psychological and behavioural predictors of vaccine efficacy: Considerations for COVID-19. Perspect. Psychol. Sci. 2021, 16, 191–203. [Google Scholar] [CrossRef]
- Dalamaga, M.; Christodoulatos, C.S.; Karampela, I.; Vallianou, N.; Apovian, C.M. Understanding the co-epidemic of obesity and COVID-19: Current evidence, comparison with previous epidemics, mechanisms, and preventive and therapeutic perspectives. Curr. Obes. Rep. 2021, 1–30. [Google Scholar] [CrossRef]
- Diaz, A.; Baweja, R.; Bonatakis, J.K.; Baweja, R. Global health disparities in vulnerable populations of psychiatric patients during the COVID-19 pandemic. World J. Psychiatry 2021, 11, 94–108. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | COVID-19 Crude Mortality Rate | COVID-19 Case Fatality Ratio | Sugar Consumption, kg/Capita/Year | Seafood Consumption, g/Capita/Day | Depression, Point Prevalence (%) | Obesity, Point Prevalence (%) |
|---|---|---|---|---|---|---|
| COVID-19 crude mortality rate | * | 0.275 (0.018) ** | 0.51 (<0.001) ** | <0.01 (0.999) | 0.56 (<0.001) ** | 0.66 (<0.001) |
| COVID-19 case-fatality ratio | - | * | 0.01 (0.999) | −0.28 (0.015) ** | 0.01 (0.999) | −0.07 (0.999) |
| Sugar consumption | - | - | * | 0.07 (0.999) | 0.52 (<0.001) ** | 0.68 (<0.001) ** |
| Seafood consumption | - | - | - | * | 0.34 (0.999) | 0.07 (0.999) |
| Depression, point prevalence | - | - | - | - | * | 0.64 (<0.001) ** |
| Variable | Correlation Coefficient (β) | Significance Level | Part Correlation | Variance Inflation Factor |
|---|---|---|---|---|
| Sugar consumption | 0.03 | 0.739 | 0.02 | 2.04 |
| Depression, point prevalence | 0.19 | 0.017 | 0.14 | 1.83 |
| Obesity, point prevalence | 0.41 | <0.001 | 0.26 | 2.54 |
| Life expectancy | 0.17 | 0.041 | 0.12 | 1.96 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rajkumar, R.P. Cross-National Variations in COVID-19 Mortality: The Role of Diet, Obesity and Depression. Diseases 2021, 9, 36. https://doi.org/10.3390/diseases9020036
Rajkumar RP. Cross-National Variations in COVID-19 Mortality: The Role of Diet, Obesity and Depression. Diseases. 2021; 9(2):36. https://doi.org/10.3390/diseases9020036
Chicago/Turabian StyleRajkumar, Ravi Philip. 2021. "Cross-National Variations in COVID-19 Mortality: The Role of Diet, Obesity and Depression" Diseases 9, no. 2: 36. https://doi.org/10.3390/diseases9020036
APA StyleRajkumar, R. P. (2021). Cross-National Variations in COVID-19 Mortality: The Role of Diet, Obesity and Depression. Diseases, 9(2), 36. https://doi.org/10.3390/diseases9020036