Cutaneous Carotenoid Level Measured by Multiple Spatially Resolved Reflection Spectroscopy Sensors Correlates with Vegetable Intake and Is Increased by Continual Intake of Vegetable Juice


Abstract
1. Introduction
2. Materials and Methods
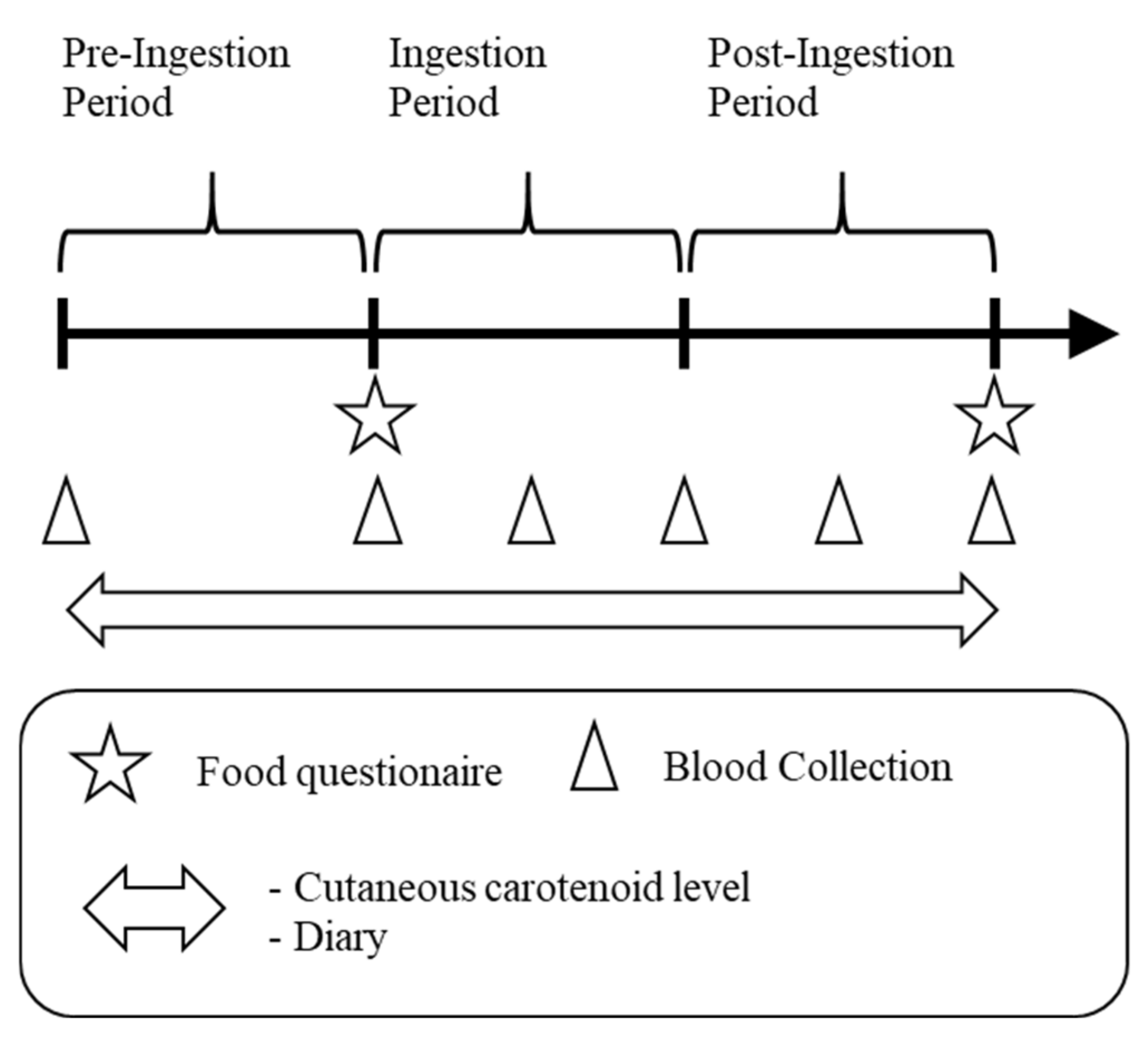
2.1. Study Design
2.2. Subjects
2.3. Test Food
2.4. Blood Carotenoid Levels
2.5. CCL Measurement
2.6. Food Questionnaire
2.7. Statistical Analysis
3. Results
3.1. Subjects
3.2. Blood Carotenoid Levels
3.3. Cutaneous Carotenoid Level (CCL)
3.4. Correlation between Blood Carotenoid Levels and CCLs (Cross-Sectional Study)
3.5. Correlation between Blood Carotenoid Concentrations and CCLs (Intervention Study)
3.6. Vegetable Intake
4. Discussion
4.1. Cross-Sectional Correlation
4.2. Effect of Vegetable Juice Ingestion on Blood Carotenoid Levels
4.3. Effect of Vegetable Juice Ingestion on CCLs
4.4. Correlation between Increased CCLs and Individual Blood Carotenoid Levels after Vegetable Juice Ingestion
4.5. Comparison with Similar Intervention Studies
4.6. Advantages of Measuring CCLs
4.7. Limitation of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD. Diet Collaborators, Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar]
- Widmer, R.J.; Flammer, A.J.; Lerman, L.O.; Lerman, A. The Mediterranean diet, its components, and cardiovascular disease. Am. J. Med. 2015, 128, 229–238. [Google Scholar] [PubMed]
- Saneei, P.; Salehi-Abargouei, A.; Esmaillzadeh, A.; Azadbakht, L. Influence of dietary approaches to stop hypertension (DASH) diet on blood pressure: A systematic review and meta-analysis on randomized controlled trials. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 1253–1261. [Google Scholar]
- Nishi, N.; Okuda, N. National Health and Nutrition Survey in target setting of Health Japan 21, 2nd ed. J. Natl. Inst. Public Health 2012, 61, 399–408. [Google Scholar]
- Wagner, M.G.; Rhee, Y.; Honrath, K.; Blodgett Salafia, E.H.; Terbizan, D. Nutrition education effective in increasing fruit and vegetable consumption among overweight and obese adults. Appetite 2016, 100, 94–101. [Google Scholar] [PubMed]
- Watanabe, D.; Nanri, H.; Sagayama, H.; Yoshida, T.; Itoi, A.; Yamaguchi, M.; Yokoyama, K.; Watanabe, Y.; Goto, C.; Ebine, N.; et al. Estimation of energy intake by a food frequency questionnaire: Calibration and validation with the doubly labeled water method in Japanese older people. Nutrients 2019, 11, 1546. [Google Scholar]
- Kaplan, L.A.; Lau, J.M.; Stein, E.A. Carotenoid composition, concentrations, and relationships in various human organs. Clin. Physiol. Biochem. 1990, 8, 1–10. [Google Scholar] [PubMed]
- Milani, A.; Basirnejad, M.; Shahbazi, S.; Bolhassani, A. Carotenoids: Biochemistry, pharmacology and treatment. Br. J. Pharmacol. 2017, 174, 1290–1324. [Google Scholar]
- Terao, J.; Minami, Y.; Bando, N. Singlet molecular oxygen-quenching activity of carotenoids: Relevance to protection of the skin from photoaging. J. Clin. Biochem. Nutr. 2011, 48, 57–62. [Google Scholar]
- Mayne, S.T.; Cartmel, B.; Scarmo, S.; Lin, H.; Leffell, D.J.; Welch, E.; Ermakov, I.; Bhosale, P.; Bernstein, P.S.; Gellermann, W. Noninvasive assessment of dermal carotenoids as a biomarker of fruit and vegetable intake. Am. J. Clin. Nutr. 2010, 92, 794–800. [Google Scholar]
- Jahns, L.; Johnson, L.K.; Mayne, S.T.; Cartmel, B.; Picklo, M.J.; Ermakov, I.V.; Gellermann, W.; Whigham, L.D. Skin and plasma carotenoid response to a provided intervention diet high in vegetables and fruit: Uptake and depletion kinetics. Am. J. Clin. Nutr. 2014, 100, 930–937. [Google Scholar] [CrossRef] [PubMed]
- Darvin, M.E.; Sandhagen, C.; Koecher, W.; Sterry, W.; Lademann, J.; Meinke, M.C. Comparison of two methods for noninvasive determination of carotenoids in human and animal skin: Raman spectroscopy versus Reflection Spectroscopy. J. Biophotonics 2012, 5, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Darvin, M.E.; Meinke, M.C.; Sterry, W.; Lademann, J. Optical methods for noninvasive determination of carotenoids in human and animal skin. J. Biomed. Opt. 2013, 18, 61230. [Google Scholar] [CrossRef] [PubMed]
- Meinke, M.C.; Schanzer, S.; Lohan, S.B.; Shchatsinin, I.; Darvin, M.E.; Vollert, H.; Magnussen, B.; Köcher, W.; Helfmann, J.; Lademann, J. Comparison of different cutaneous carotenoid sensors and influence of age, skin type, and kinetic changes subsequent to intake of a vegetable extract. J. Biomed. Opt. 2016, 21, 107002. [Google Scholar] [CrossRef] [PubMed]
- Meinke, M.C.; Lohan, S.B.; Köcher, W.; Magnussen, B.; Darvin, M.E.; Lademann, J. Multiple spatially resolved reflection spectroscopy to monitor cutaneous carotenoids during supplementation of fruit and vegetable extracts in vivo. Skin Res. Technol. 2017, 23, 459–462. [Google Scholar] [CrossRef] [PubMed]
- Aguilar, S.S.; Wengreen, H.J.; Dew, J. Skin Carotenoid response to a high-carotenoid juice in children: A randomized clinical trial. J. Acad. Nutr. Diet. 2015, 115, 1771–1778. [Google Scholar] [CrossRef]
- Gärtner, C.; Stahl, W.; Sies, H. Lycopene is more bioavailable from tomato paste than from fresh tomatoes. Am. J. Clin. Nutr. 1997, 66, 116–122. [Google Scholar] [CrossRef]
- Livny, O.; Reifen, R.; Levy, I.; Madar, Z.; Faulks, R.; Southon, S.; Schwartz, B. Beta-carotene bioavailability from differently processed carrot meals in human ileostomy volunteers. Eur. J. Nutr. 2003, 42, 338–345. [Google Scholar] [CrossRef]
- Oshima, S.; Sakamoto, H.; Ishiguro, Y.; Terao, J. Accumulation and clearance of capsanthin in blood plasma after the ingestion of paprika juice in men. J. Nutr. 1997, 127, 1475–1479. [Google Scholar] [CrossRef]
- Aizawa, K.; Inakuma, T. Quantitation of carotenoids in commonly consumed vegetables in Japan. Food Sci. Technol. Res. 2007, 13, 247–252. [Google Scholar] [CrossRef][Green Version]
- Richelle, M.; Sanchez, B.; Tavazzi, I.; Lambelet, P.; Bortlik, K.; Williamson, G. Lycopene isomerisation takes place within enterocytes during absorption in human subjects. Br. J. Nutr. 2010, 103, 1800–1807. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, K.; Yoshimura, Y.; Kaimoto, T.; Kunii, D.; Komatsu, T.; Yamamoto, S. Validation of a food frequency questionnaire based on food groups for estimating individual nutrient intake. Jpn. J. Nutr. Diet. 2001, 59, 221–232. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software “EZR” for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Rock, C.L.; Flatt, S.W.; Wright, F.A.; Faerber, S.; Newman, V.; Kealey, S.; Pierce, J.P. Responsiveness of carotenoids to a high vegetable diet intervention designed to prevent breast cancer recurrence. Cancer Epidemiol. Biomark. Prev. 1997, 6, 617–623. [Google Scholar]
- Moran, N.E.; Cichon, M.J.; Riedl, K.M.; Grainger, E.M.; Schwartz, S.J.; Novotny, J.A.; Erdman, J.W.; Clinton, S.K. Compartmental and noncompartmental modeling of ¹³C-lycopene absorption, isomerization, and distribution kinetics in healthy adults. Am. J. Clin. Nutr. 2015, 102, 1436–1449. [Google Scholar] [CrossRef]
- Lademann, J.; Caspers, P.J.; van der Pol, A.; Richter, H.; Patzelt, A.; Zastrow, L.; Darvin, M.; Sterry, W.; Fluhr, J.W. In vivo Raman spectroscopy detects increased epidermal antioxidative potential with topically applied carotenoids. Laser Phys. Lett. 2009, 6, 76–79. [Google Scholar] [CrossRef]
- Blume-Peytavi, U.; Rolland, A.; Darvin, M.E.; Constable, A.; Pineau, I.; Voit, C.; Zappel, K.; Schäfer-Hesterberg, G.; Meinke, M.; Clavez, R.L.; et al. Cutaneous lycopene and beta-carotene levels measured by resonance Raman spectroscopy: High reliability and sensitivity to oral lactolycopene deprivation and supplementation. Eur. J. Pharm. Biopharm. 2009, 73, 187–194. [Google Scholar] [CrossRef]
- Meinke, M.C.; Darvin, M.E.; Vollert, H.; Lademann, J. Bioavailability of natural carotenoids in human skin compared to blood. Eur. J. Pharm. Biopharm. 2010, 76, 269–274. [Google Scholar] [CrossRef]
- Jung, S.; Darvin, M.E.; Chung, H.S.; Jung, B.; Lee, S.H.; Lenz, K.; Chung, W.S.; Yu, R.X.; Patzelt, A.; Lee, B.N.; et al. Antioxidants in Asian-Korean and Caucasian skin: The influence of nutrition and stress. Skin Pharmacol. Physiol. 2014, 27, 293–302. [Google Scholar] [CrossRef]
- Matsumoto, M.; Suganuma, H.; Shimizu, S.; Hayashi, H.; Sawada, K.; Tokuda, I.; Ihara, K.; Nakaji, S. Skin carotenoid level as an alternative marker of serum total carotenoid concentration and vegetable intake correlates with biomarkers of circulatory diseases and metabolic syndrome. Nutrients 2020, 12, 1825. [Google Scholar] [CrossRef]


{kind=link}
| Lutein | Zeaxanthin | β-Cryptoxanthin | α-Carotene | β-Carotene | Lycopene | Total Carotenoid | |||
|---|---|---|---|---|---|---|---|---|---|
| Total | cis-Form | trans-Form | |||||||
| Day 1 of pre-ingestion Period | 0.197 ± 0.077 | 0.039 ± 0.015 | 0.086 ± 0.048 | 0.161 ± 0.091 | 0.462 ± 0.242 | 0.388 ± 0.131 | 0.253 ± 0.092 | 0.138 ± 0.045 | 1.333 ± 0.383 |
| Day 1 of ingestion period 1 | 0.189 ± 0.061 (0.992) | 0.034 ± 0.014 (0.618) | 0.088 ± 0.038 (1.000) | 0.147 ± 0.128 (0.990) | 0.405 ± 0.263 (0.939) | 0.371 ± 0.138 (0.991) | 0.237 ± 0.084 (0.966) | 0.137 ± 0.057 (1.000) | 1.232 ± 0.477 (0.919) |
| Week 3 of ingestion period 2 | 0.190 ± 0.064 (1.000) | 0.032 ± 0.015 (0.984) | 0.091 ± 0.042 (1.000) | 0.378 ± 0.161 *** (<0.001) | 0.820 ± 0.393 *** (<0.001) | 0.458 ± 0.156 (0.119) | 0.285 ± 0.094 (0.248) | 0.177 ± 0.068 * (0.045) | 1.968 ± 0.679 *** (<0.001) |
| Day 1 of post-ingestion period 2 | 0.207 ± 0.068 (0.746) | 0.038 ± 0.016 (0.757) | 0.096 ± 0.048 (0.993) | 0.480 ± 0.153 *** (<0.001) | 0.946 ± 0.396 *** (<0.001) | 0.487 ± 0.158 * (0.022) | 0.314 ± 0.105 * (0.021) | 0.176 ± 0.062 (0.051) | 2.253 ± 0.587 *** (<0.001) |
| Week 3 of post-ingestion period 2 | 0.197 ± 0.063 (0.978) | 0.034 ± 0.017 (0.999) | 0.092 ± 0.051 (0.999) | 0.306 ± 0.109 *** (<0.001) | 0.657 ± 0.322 * (0.016) | 0.452 ± 0.164 (0.168) | 0.311 ± 0.115 * (0.028) | 0.144 ± 0.054 (0.975) | 1.738 ± 0.507 ** (0.001) |
| Last day of post-ingestion period 2 | 0.199 ± 0.346 (0.942) | 0.036 ± 0.362 (0.924) | 0.147 ± 0.387 (0.079) | 0.236 ± 0.208 * (0.021) | 0.553 ± 0.333 (0.261) | 0.411 ± 0.227 (0.741) | 0.281 ± 0.243 (0.311) | 0.132 ± 0.308 (0.997) | 1.583 ± 0.384 * (0.042) |
| Period | Week | Cutaneous Carotenoid Level |
|---|---|---|
| Pre-ingestion | 1 | 6.55 ± 0.88 |
| 2 | 6.69 ± 0.98 | |
| 3 | 6.62 ± 0.89 | |
| 4 | 6.64 ± 0.96 | |
| Ingestion | 1 | 6.63 ± 1.02 |
| 2 | 6.71 ± 0.96 | |
| 3 | 6.91 ± 0.96 | |
| 4 | 7.16 ± 1.00 | |
| Post-ingestion | 1 | 7.34 ± 1.02 |
| 2 | 7.50 ± 0.93 * | |
| 3 | 7.46 ± 0.93 * | |
| 4 | 7.23 ± 0.91 |
| Correlation Coefficient | |
|---|---|
| Lutein | 0.206 |
| Zeaxanthin | 0.074 |
| β-Cryptoxanthin | 0.080 |
| α-Carotene | 0.748 ** |
| β-Carotene | 0.793 ** |
| Lycopene | 0.065 |
| Day 1 of Ingestion Period | Week 3 of Ingestion Period | Day 1 of Post-Ingestion Period | Week 3 of Post-Ingestion Period | Last Day of Post-Ingestion Period | |
|---|---|---|---|---|---|
| Lutein | 0 | 0.077 | −0.059 | −0.104 | −0.034 |
| Zeaxanthin | 0 | −0.064 | −0.277 | −0.242 | −0.109 |
| β-Cryptoxanthin | 0 | 0.119 | −0.208 | 0.121 | 0.007 |
| α-Carotene | 0 | 0.420 * | 0.521 ** | 0.523 ** | 0.436 * |
| β-Carotene | 0 | 0.398 * | 0.46 * | 0.325 | 0.134 |
| Lycopene | 0 | 0.001 | −0.017 | −0.129 | −0.189 |
| cis-Lycopene | 0 | −0.192 | −0.157 | −0.170 | −0.196 |
| trans-Lycopene | 0 | 0.192 | 0.132 | −0.055 | −0.139 |
| Pre-Ingestion Period | Post-Ingestion Period | Difference | |
|---|---|---|---|
| Green and yellow vegetables (g) | 79.5 ± 53.2 | 80.6 ± 39.0 | 1.1 ± 30.2 |
| Other vegetables (g) | 139.6 ± 83.7 | 124.0 ± 55.0 | −15.6 ± 55.3 |
| Total vegetables (g) | 219.1 ± 132.2 | 204.6 ± 89.8 | −14.5 ± 73.5 |
| Meinke’s Study [28] | This Study | |||||
|---|---|---|---|---|---|---|
| Ingestion Period (Days) | ||||||
| 28 Days | 28 Days | |||||
| Amount of Carotenoids in Test Food (mg) | ||||||
| Lutein | 9 | - | ||||
| α-Carotene | - | 6 | ||||
| β-Carotene | 3 | 9.8 | ||||
| Lycopene | 0.78 | 16 | ||||
| Blood Carotenoids Concentration (Mean, µg/mL) | ||||||
| Pre | Post | Difference | Pre | Post | Difference | |
| β-Carotene | 0.172 | 0.278 | 0.106 | 0.462 | 0.946 | 0.484 |
| Total Carotenoids | 0.534 | 0.792 | 0.258 | 1.232 | 2.253 | 1.022 |
| cis-Lycopene | 0.0432 | 0.0553 | 0.0121 | 0.237 | 0.314 | 0.077 |
| Increased Blood Carotenoid Concentration per Ingested Carotenoids (Mean, µg/mL per mg Ingestion) | ||||||
| β-Carotene | 0.0353 | 0.0494 | ||||
| Lycopene | 0.0202 | 0.0321 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hayashi, H.; Sato, I.; Suganuma, H. Cutaneous Carotenoid Level Measured by Multiple Spatially Resolved Reflection Spectroscopy Sensors Correlates with Vegetable Intake and Is Increased by Continual Intake of Vegetable Juice. Diseases 2021, 9, 4. https://doi.org/10.3390/diseases9010004
Hayashi H, Sato I, Suganuma H. Cutaneous Carotenoid Level Measured by Multiple Spatially Resolved Reflection Spectroscopy Sensors Correlates with Vegetable Intake and Is Increased by Continual Intake of Vegetable Juice. Diseases. 2021; 9(1):4. https://doi.org/10.3390/diseases9010004
Chicago/Turabian StyleHayashi, Hiroki, Ikuo Sato, and Hiroyuki Suganuma. 2021. "Cutaneous Carotenoid Level Measured by Multiple Spatially Resolved Reflection Spectroscopy Sensors Correlates with Vegetable Intake and Is Increased by Continual Intake of Vegetable Juice" Diseases 9, no. 1: 4. https://doi.org/10.3390/diseases9010004
APA StyleHayashi, H., Sato, I., & Suganuma, H. (2021). Cutaneous Carotenoid Level Measured by Multiple Spatially Resolved Reflection Spectroscopy Sensors Correlates with Vegetable Intake and Is Increased by Continual Intake of Vegetable Juice. Diseases, 9(1), 4. https://doi.org/10.3390/diseases9010004