
Strength and Performance Tests for Screening Reduced Muscle Mass in Elderly Lebanese Males with Obesity in Community Dwellings




Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.3. Statistical Analysis
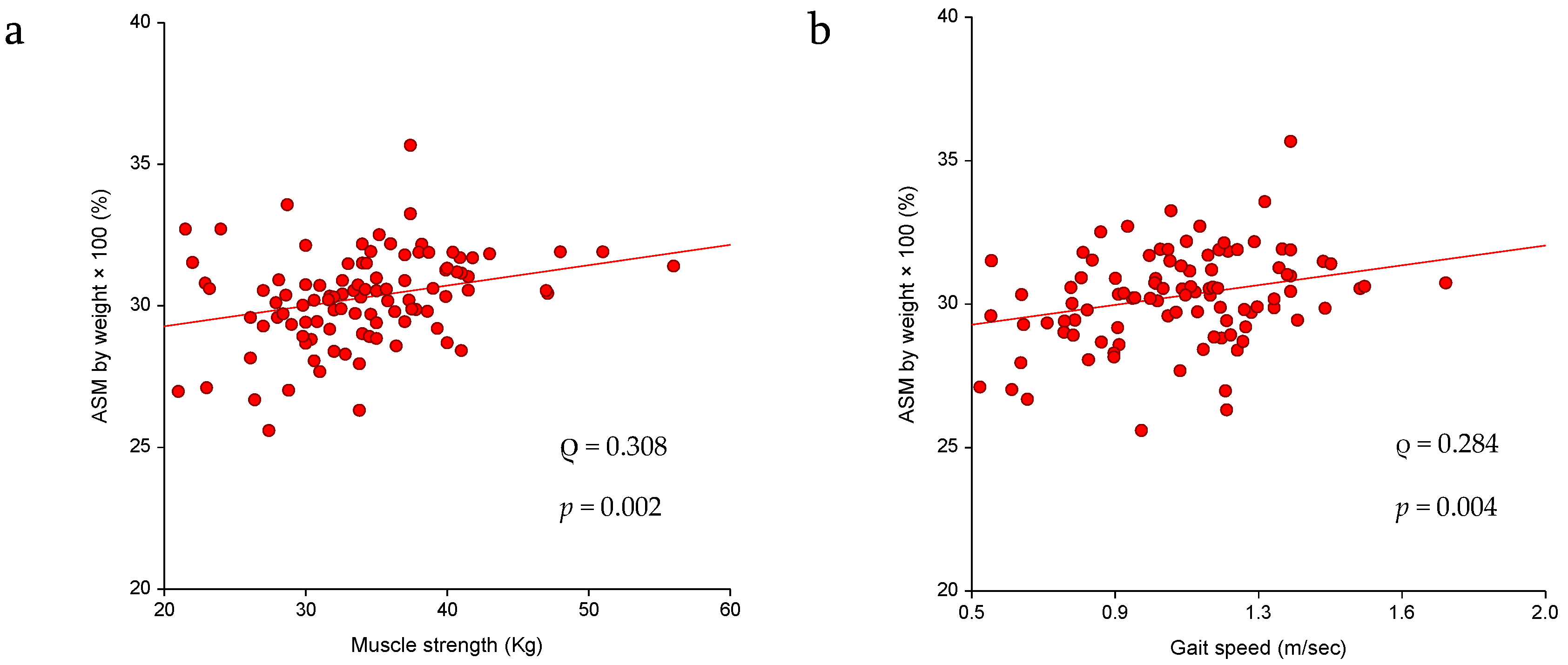
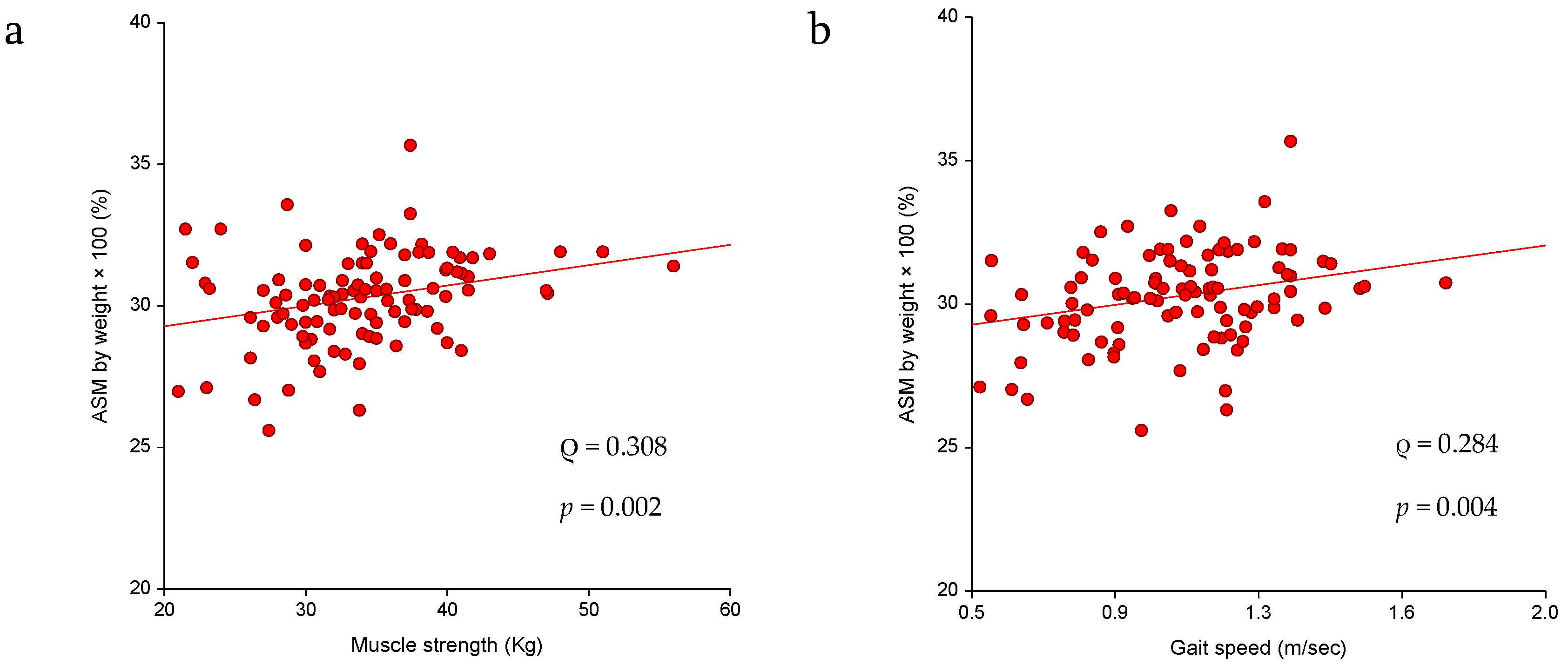
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Sample Availability
References
- Liang, X.; Chen, X.; Li, J.; Yan, M.; Yang, Y. Study on body composition and its correlation with obesity: A Cohort Study in 5121 Chinese Han participants. Medicine (Baltim.) 2018, 97, e10722. [Google Scholar] [CrossRef] [PubMed]
- Das, S.K. Body composition measurement in severe obesity. Curr. Opin. Clin. Nutr. Metab. Care 2005, 8, 602–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silver, H.J.; Welch, E.B.; Avison, M.J.; Niswender, K.D. Imaging body composition in obesity and weight loss: Challenges and opportunities. Diabetes Metab. Syndr. Obes. 2010, 3, 337–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Ghoch, M.; Rossi, A.P.; Calugi, S.; Rubele, S.; Soave, F.; Zamboni, M.; Chignola, E.; Mazzali, G.; Bazzani, P.V.; Dalle Grave, R. Physical performance measures in screening for reduced lean body mass in adult females with obesity. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 917–921. [Google Scholar] [CrossRef]
- Nezameddin, R.; Itani, L.; Kreidieh, D.; El Masri, D.; Hana Tannir, H.; El Ghoch, M. Understanding Sarcopenic Obesity in Terms of Definition and Health Consequences: A Clinical Review. Curr. Diabetes Rev. 2020, 16, 957–961. [Google Scholar] [CrossRef]
- Visser, M.; Deeg, D.J.; Lips, P. Longitudinal Aging Study A: Low vitamin D and high parathyroid hormone levels as determinants of loss of muscle strength and muscle mass (sarcopenia): The Longitudinal Aging Study Amsterdam. J. Clin. Endocrinol. Metab. 2003, 88, 5766–5772. [Google Scholar] [CrossRef]
- Hirschfeld, H.P.; Kinsella, R.; Duque, G. Osteosarcopenia: Where bone, muscle, and fat collide. Osteoporos. Int. 2017, 28, 2781–2790. [Google Scholar] [CrossRef]
- Wolfe, R.R. The underappreciated role of muscle in health and disease. Am. J. Clin. Nutr. 2006, 84, 475–482. [Google Scholar] [CrossRef]
- Pichard, C.; Kyle, U.G.; Morabia, A.; Perrier, A.; Vermeulen, B.; Unger, P. Nutritional assessment: Lean body mass depletion at hospital admission is associated with an increased length of stay. Am. J. Clin. Nutr. 2004, 79, 613–618. [Google Scholar] [CrossRef] [Green Version]
- Szulc, P.; Munoz, F.; Marchand, F.; Chapurlat, R.; Delmas, P.D. Rapid loss of appendicular skeletal muscle mass is associated with higher all-cause mortality in older men: The prospective MINOS study. Am. J. Clin. Nutr. 2010, 91, 1227–1236. [Google Scholar] [CrossRef] [Green Version]
- Bachettini, N.P.; Bielemann, R.M.; Barbosa-Silva, T.G.; Menezes, A.M.B.; Tomasi, E.; Gonzalez, M.C. Sarcopenia as a mortality predictor in community-dwelling older adults: A comparison of the diagnostic criteria of the European Working Group on Sarcopenia in Older People. Eur. J. Clin. Nutr. 2020, 74, 573–580. [Google Scholar] [CrossRef]
- El Ghoch, M.; Fakhoury, R. Challenges and New Directions in Obesity Management: Lifestyle Modification Programmes, Pharmacotherapy and Bariatric Surgery. J. Popul. Ther. Clin. Pharmacol. 2019, 26, e1–e4. [Google Scholar] [CrossRef] [Green Version]
- Khadra, D.; Itani, L.; Tannir, H.; Kreidieh, D.; El Masri, D.; El Ghoch, M. Association between sarcopenic obesity and higher risk of type 2 diabetes in adults: A systematic review and meta-analysis. World J. Diabetes 2019, 15, 311–323. [Google Scholar] [CrossRef] [PubMed]
- Khazem, S.; Itani, L.; Kreidieh, D.; El Masri, D.; Tannir, H.; Citarella, R.; El Ghoch, M. Reduced Lean Body Mass and Cardiometabolic Diseases in Adult Males with Overweight and Obesity: A Pilot Study. Int. J. Environ. Res. Public Health 2018, 15, 2754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, S.C.; Khow, K.S.; Jadczak, A.D.; Visvanathan, R. Clinical Screening Tools for Sarcopenia and Its Management. Curr. Gerontol. Geriatr. Res. 2016, 2016, 5978523. [Google Scholar] [CrossRef] [Green Version]
- Petroni, M.L.; Caletti, M.T.; Dalle Grave, R.; Bazzocchi, A.; Aparisi Gómez, M.P.; Marchesini, G. Prevention and Treatment of Sarcopenic Obesity in Women. Nutrients 2019, 11, 1302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, L.F.; Lim, Z.Y.; Choe, R.; Seetharaman, S.; Merchant, R. Screening for Frailty and Sarcopenia Among Older Persons in Medical Outpatient Clinics and its Associations with Healthcare Burden. J. Am. Med. Dir. Assoc. 2017, 18, 583–587. [Google Scholar] [CrossRef]
- Johnson Stoklossa, C.A.; Sharma, A.M.; Forhan, M.; Siervo, M.; Padwal, R.S.; Prado, C.M. Prevalence of Sarcopenic Obesity in Adults with Class, II/III Obesity Using Different Diagnostic Criteria. J. Nutr. Metab. 2017, 2017, 7307618. [Google Scholar] [CrossRef]
- Oh, C.; Jho, S.; No, J.K.; Kim, H.S. Body composition changes were related to nutrient intakes in elderly men but elderly women had a higher prevalence of sarcopenic obesity in a population of Korean adults. Nutr. Res. 2015, 35, 1–6. [Google Scholar] [CrossRef]
- Taing, K.Y.; Farkouh, M.E.; Moineddin, R.; Tu, J.V.; Jha, P. Comparative associations between anthropometric and bioelectric impedance analysis derived adiposity measures with blood pressure and hypertension in India: A cross-sectional analysis. BMC Obes. 2017, 1, 37. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, A.; Balnave, R.; Adams, R. Grip strength testing reliability. J. Hand Ther. 1994, 7, 163–170. [Google Scholar] [CrossRef]
- Maggio, M.; Ceda, G.P.; Ticinesi, A.; De Vita, F.; Gelmini, G.; Costantino, C.; Meschi, T.; Kressig, R.W.; Cesari, M.; Fabi, M.; et al. Instrumental and non-instrumental evaluation of 4-m walking speed in older individuals. PLoS ONE 2016, 11, e0153583. [Google Scholar] [CrossRef]
- Rashed, A.M.; Abdel-Wahab, N.; Moussa, E.M.M.; Hammam, N. Association of hand grip strength with disease activity, disability and quality of life in children and adolescents with Juvenile Idiopathic Arthritis. Adv. Rheumatol. 2018, 58, 11. [Google Scholar] [CrossRef] [Green Version]
- Tyrovolas, S.; Panagiotakos, D.; Georgousopoulou, E.; Chrysohoou, C.; Tousoulis, D.; Haro, J.M.; Pitsavos, C. Skeletal muscle mass in relation to 10 year cardiovascular disease incidence among middle aged and older adults: The ATTICA study. J. Epidemiol. Community Health 2020, 74, 26–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shou, J.; Chen, P.J.; Xiao, W.H. Mechanism of increased risk of insulin resistance in aging skeletal muscle. Diabetol. Metab. Syndr. 2020, 12, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuttle, C.S.L.; Thang, L.A.N.; Maier, A.B. Markers of inflammation and their association with muscle strength and mass: A systematic review and meta-analysis. Ageing Res. Rev. 2020, 64, 101185. [Google Scholar] [CrossRef] [PubMed]
- Liao, Y.S.; Li, H.C.; Lu, H.K.; Lai, C.L.; Wang, Y.S.; Hsieh, K.C. Comparison of Bioelectrical Impedance Analysis and Dual Energy X-ray Absorptiometry for Total and Segmental Bone Mineral Content with a Three-Compartment Model. Int. J. Environ. Res. Public Health 2020, 17, 2595. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.; Kim, C.H.; Kim, D.W.; Park, M.; Park, H.S.; Min, S.S.; Han, S.H.; Yee, J.Y.; Chung, S.; Kim, C. External cross-validation of bioelectrical impedance analysis for the assessment of body composition in Korean adults. Nutr. Res. Pract. 2011, 5, 246–252. [Google Scholar] [CrossRef]
- Boneva-Asiova, Z.; Boyanov, M.A. Body composition analysis by leg-to-leg bioelectrical impedance and dual-energy X-ray absorptiometry in non-obese and obese individuals. Diabetes Obes. Metab. 2008, 10, 1012–1018. [Google Scholar] [CrossRef]
- Pateyjohns, I.R.; Brinkworth, G.D.; Buckley, J.D.; Noakes, M.; Clifton, P.M. Comparison of three bioelectrical impedance methods with DXA in overweight and obese men. Obesity (Silver Spring) 2006, 14, 2064–2070. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Demographics | Total N = 102 | Normal SMM N = 70 | Reduced SMM N = 32 | Significance |
|---|---|---|---|---|
| Age (Years) | 67.64 (6.96) | 66.13 (5.93) | 70.94 (7.96) | p = 0.004 |
| Marital status | X2 = 3.075; p = 0.079 | |||
| Not married | 11 (10.8) | 5 (7.1) | 6 (18.8) | |
| Married | 91 (89.2) | 65 (92.9) | 26 (81.3) | |
| Level of education | X2 = 1.155; p = 0.283 | |||
| Lower education | 83 (81.4) | 55 (78.6) | 28 (87.5) | |
| Higher education | 19 (18.6) | 15 (21.4) | 4 (12.5) | |
| Employment | X2 = 0.073; p = 0.787 | |||
| Not employed | 65 (63.7) | 44 (62.9) | 21 (65.6) | |
| Employed | 37 (36.3) | 26 (37.1) | 11 (34.4) | |
| Salary | X2 = 5.038; p = 0.025 | |||
| <LL 1 million | 60 (58.8) | 36 (51.4) | 24 (75.0) | |
| >LL 1 million | 42 (41.2) | 34 (48.6) | 8 (25.0) | |
| Smoking | X2 = 0.415; p = 0.520 | |||
| Non smoker | 59 (57.8) | 39 (55.7) | 20 (62.5) | |
| Smoker | 43 (42.2) | 31 (44.3) | 12 (37.5) | |
| Place of residence | X2 = 0.164; p = 0.686 | |||
| Outside Beirut | 8 (7.8) | 6 (8.6) | 2 (6.3) | |
| Inside Beirut | 94 (92.2) | 64 (91.4) | 30 (93.8) | |
| Weight (kg) § | 83.75 (76.78–92.02) | 82.70 (75.73–88.25) | 89.10 (78.88–106.10) | p = 0.014 |
| Body Fat (BF) § | 22.25 (18.18–26.42) | 20.40 (17.18–27.51) | 27.45 (21.78–35.10) | p < 0.0001 |
| Body fat percentage (BF%) | 26.68 (5.05) | 24.78 (4.13) | 30.82 (4.40) | p < 0.0001 |
| Body mass index (BMI) § | 29.89 (28.00–33.07) | 28.81 (27.51–31.60) | 33.20 (29.58–38.71) | p < 0.0001 |
| Gait speed | 1.02 (0.25) | 1.08 (0.24) | 0.91 (0.24) | p = 0.002 |
| Handgrip strength | 33.64 (6.94) | 35.05 (6.75) | 30.56 (6.42) | p = 0.002 |
| Cardiometabolic disease | X2 = 0.012; p = 0.913 | |||
| No | 55 (53.9) | 38 (54.3) | 17 (53.1) | |
| Yes | 47 (46.1) | 32 (45.7) | 15 (46.9) |
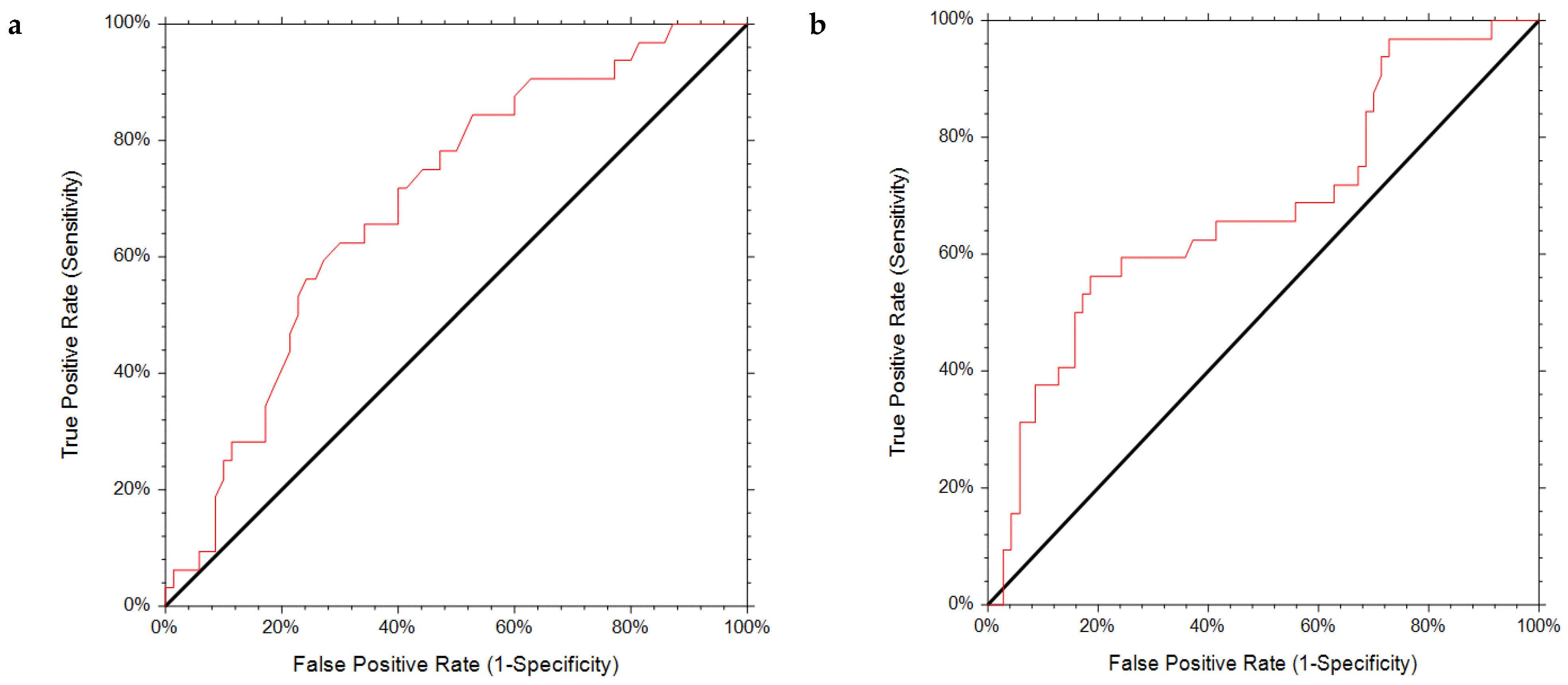
| AUC | 95%CI | p Value | Sensitivity | Specificity | Cut Off | Specificity at 90% Sensitivity | Cut-Off at 90% Sensitivity | |
|---|---|---|---|---|---|---|---|---|
| Muscle strength (kg) | 0.696 | 0.573–0.788 | 0.0002 | 0.625 | 0.700 | 32.00 | 0.377 | 36.88 |
| Gait speed (m/s) | 0.679 | 0.543–0.779 | 0.0014 | 0.625 | 0.629 | 1.01 | 0.289 | 1.19 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saadeddine, D.; Itani, L.; Rossi, A.P.; Pellegrini, M.; El Ghoch, M. Strength and Performance Tests for Screening Reduced Muscle Mass in Elderly Lebanese Males with Obesity in Community Dwellings. Diseases 2021, 9, 23. https://doi.org/10.3390/diseases9010023
Saadeddine D, Itani L, Rossi AP, Pellegrini M, El Ghoch M. Strength and Performance Tests for Screening Reduced Muscle Mass in Elderly Lebanese Males with Obesity in Community Dwellings. Diseases. 2021; 9(1):23. https://doi.org/10.3390/diseases9010023
Chicago/Turabian StyleSaadeddine, Dana, Leila Itani, Andrea P. Rossi, Massimo Pellegrini, and Marwan El Ghoch. 2021. "Strength and Performance Tests for Screening Reduced Muscle Mass in Elderly Lebanese Males with Obesity in Community Dwellings" Diseases 9, no. 1: 23. https://doi.org/10.3390/diseases9010023
APA StyleSaadeddine, D., Itani, L., Rossi, A. P., Pellegrini, M., & El Ghoch, M. (2021). Strength and Performance Tests for Screening Reduced Muscle Mass in Elderly Lebanese Males with Obesity in Community Dwellings. Diseases, 9(1), 23. https://doi.org/10.3390/diseases9010023