Fosfomycin, Applying Known Methods and Remedies to A New Era


 , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Bacterial Isolates
2.2. Susceptibility Testing
2.3. Molecular Detection of Carbapenem Resistance
2.4. Statistical Analysis
3. Results
3.1. Fosfomycin Revealed Great In Vitro Efficacy Against Carbapenem-Resistant Enterobacteriaceae
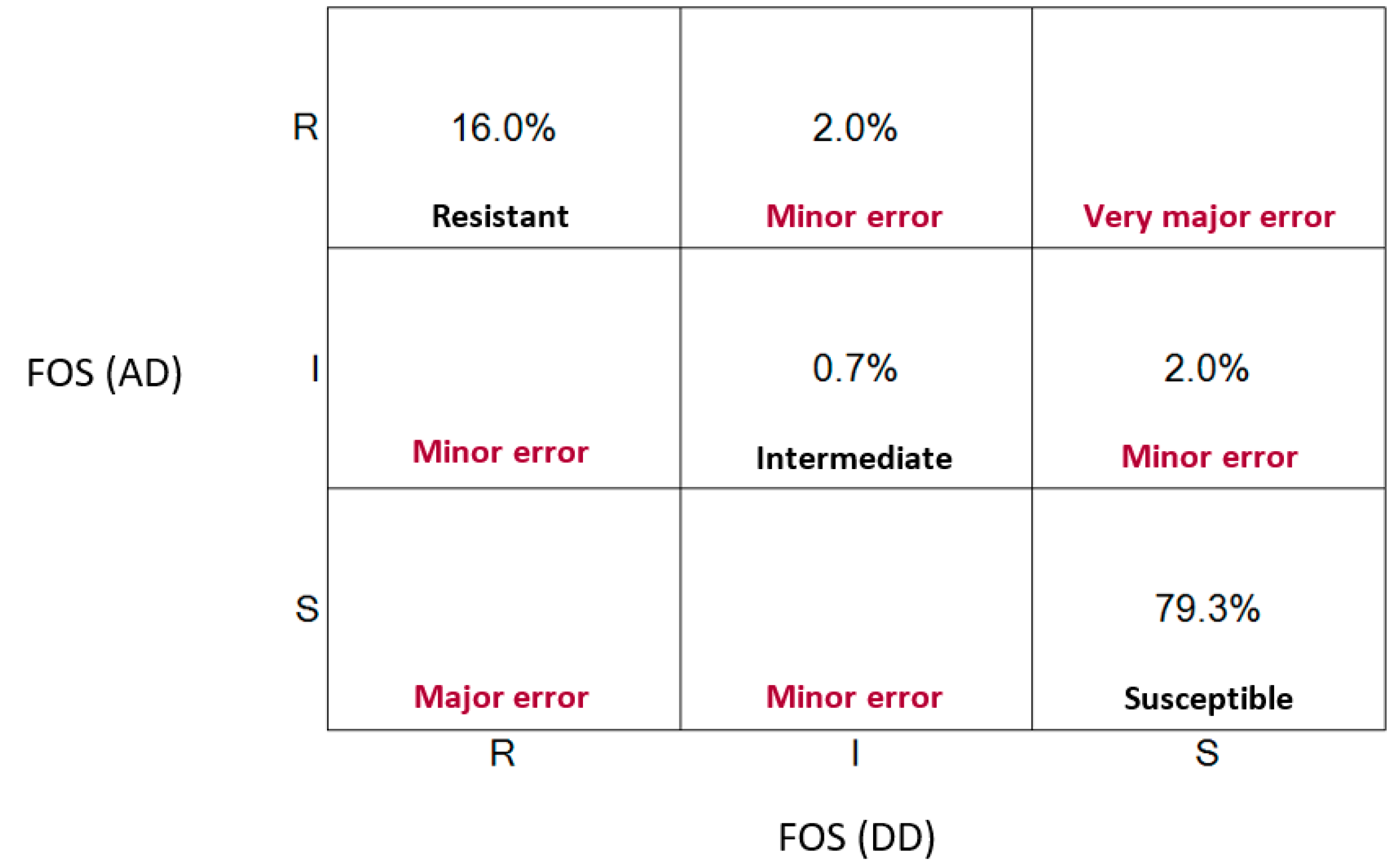
3.2. Disk Diffusion is A Reliable Test to Evaluate Fosfomycin Resistance Similar to the Agar Dilution Technique
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Ethical Approval
References
- Logan, L.K.; Weinstein, R.A. The Epidemiology of Carbapenem-Resistant Enterobacteriaceae: The Impact and Evolution of a Global Menace. J. Infect. Dis. 2017, 215 (suppl. 1), S28–S36. [Google Scholar] [CrossRef] [PubMed]
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [PubMed]
- Raz, R. Fosfomycin: An old—New antibiotic. Clin. Microbiol. Infect. 2012, 18, 4–7. [Google Scholar] [CrossRef] [PubMed]
- Borisova, M.; Gisin, J.; Mayer, C. Blocking peptidoglycan recycling in Pseudomonas aeruginosa attenuates intrinsic resistance to fosfomycin. Microb. Drug Resist. 2014, 20, 231–237. [Google Scholar] [CrossRef]
- Hashemian, S.M.R.; Farhadi, Z.; Farhadi, T. Fosfomycin: The characteristics, activity, and use in critical care. Ther. Clin. Risk Manag. 2019, 15, 525–530. [Google Scholar] [CrossRef]
- Gobernado, M. Revisión Fosfomicina. Marzo Prous Sci. 2003, 16, 15–40. [Google Scholar]
- Gardiner, B.J.; Mahony, A.A.; Ellis, A.G.; Lawrentschuk, N.; Bolton, D.M.; Zeglinski, P.T.; Frauman, A.G.; Grayson, M.L. Is Fosfomycin a Potential Treatment Alternative for Multidrug-Resistant Gram-Negative Prostatitis? Clin. Infect. Dis. 2014, 58, e101–e105. [Google Scholar] [CrossRef]
- Florent, A.; Chichmanian, R.M.; Cua, E.; Pulcini, C. Adverse events associated with intravenous fosfomycin. Int. Antimicrob. Agents 2011, 37, 82–83. [Google Scholar] [CrossRef]
- Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing, 28th ed.; CLSI supplement M100; CLSI: Wayne, PA, USA, 2018. [Google Scholar]
- Shen, F.; Tang, X.; Cheng, W.; Wang, Y.; Wang, C.; Shi, X.; An, Y.; Zhang, Q.; Liu, M.; Liu, B.; et al. Fosfomycin enhances phagocyte-mediated killing of Staphylococcus aureus by extracellular traps and reactive oxygen species. Sci. Rep. 2016, 6, 19262. [Google Scholar] [CrossRef]
- An, Y.; Wang, Y.; Zhan, J.; Tang, X.; Shen, K.; Shen, F.; Wang, C.; Luan, W.; Wang, X.; Wang, X.; et al. Fosfomycin Protects Mice from Staphylococcus aureus Pneumonia Caused by α-Hemolysin in Extracellular Vesicles by Inhibiting MAPK-Regulated NLRP3 Inflammasomes. Front. Cell. Infect. Microbiol. 2019, 9, 253. [Google Scholar] [CrossRef]
- Krause, R.; Patruta, S.; Daxböck, F.; Fladerer, P.; Wenisch, C. The effect of fosfomycin on neutrophil function. J. Antimicrob. Chemother. 2001, 47, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Hamada, M.; Honda, J.; Yoshimuta, T.; Fumimori, T.; Okamoto, M.; Aizawa, H. Fosfomycin inhibits neutrophil function via a protein kinase C-dependent signaling pathway. Int. Immunopharmacol. 2002, 2, 511–518. [Google Scholar] [CrossRef]
- Morikawa, K.; Watabe, H.; Araake, M.; Morikawa, S. Modulatory effect of antibiotics on cytokine production by human monocytes in vitro. Antimicrob. Agents Chemother. 1996, 40, 1366–1370. [Google Scholar] [CrossRef] [PubMed]
- Morikawa, K.; Oseko, F.; Morikawa, S. Immunomodulatory effect of fosfomycin on human B-lymphocyte function. Antimicrob. Agents Chemother. 1993, 37, 270–275. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Marquès, C.; Collin, V.; Franceschi, C.; Charbonnel, N.; Chatellier, S.; Forestier, C. Fosfomycin and Staphylococcus aureus: Transcriptomic approach to assess effect on biofilm, and fate of unattached cells. J. Antibiot. 2020, 73, 91–100. [Google Scholar] [CrossRef]
- Fonnes, S.; Weisser, J.J.; Holzknecht, B.J.; Arpi, M.; Rosenberg, J. The plasma pharmacokinetics of fosfomycin and metronidazole after intraperitoneal administration in patients undergoing appendectomy for uncomplicated appendicitis. Fundam. Clin. Pharmacol. 2020, 34, 504–512. [Google Scholar] [CrossRef]
- Abbott, I.J.; van Gorp, E.; Wijma, R.A.; Meletiadis, J.; Mouton, J.W.; Peleg, A.Y. Evaluation of pooled human urine and synthetic alternatives in a dynamic bladder infection in vitro model simulating oral fosfomycin therapy. J. Microbiol. Methods 2020, 171, 105861. [Google Scholar] [CrossRef]
- Ruiz Ramos, J.; Salavert Lletí, M. Fosfomycin in infections caused by multidrug-resistant Gram-negative pathogens. Rev. Esp. Quimioter. 2019, 32 (Suppl. 1), 45–54. [Google Scholar]
- Joukhadar, C.; Klein, N.; Dittrich, P.; Zeitlinger, M.; Geppert, A.; Skhirtladze, K.; Frossard, M.; Heinz, G.; Müller, M. Target site penetration of fosfomycin in critically ill patients. J. Antimicrob. Chemother. 2003, 51, 1247–1252. [Google Scholar] [CrossRef]
- European Committee on Antimicrobial Susceptibility Testing (EUCAST). Breakpoint Tables for Interpretation of MICs and Zone Diameters. Version 8.1. 2018. Available online: https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Breakpoint_tables/v_10.0_Breakpoint_Tables.pdf. (accessed on 20 June 2020).
- Mojica, M.F.; De La Cadena, E.; Hernández-Gómez, C.; Correa, A.; Appel, T.M.; Pallares, C.J.; Villegas, M.V. Performance of disk diffusion and broth microdilution for fosfomycin susceptibility testing of multidrug-resistant clinical isolates of Enterobacteriaceae and Pseudomonas aeruginosa. J. Glob. Antimicrob. Resist. 2020, 21, 391–395. [Google Scholar] [CrossRef]
- Mueller, J.H.; Hinton, J. A Protein-Free Medium for Primary Isolation of the Gonococcus and Meningococcus. Exp. Biol. Med. 1941, 48, 330–333. [Google Scholar] [CrossRef]
- Poirel, L.; Walsh, T.R.; Cuvillier, V.; Nordmann, P. Multiplex PCR for detection of acquired carbapenemase genes. Diagn. Microbiol. Infect. Dis. 2011, 70, 119–123. [Google Scholar] [CrossRef] [PubMed]
- RStudio Team. RStudio: Integrated Development for R. 2020. Available online: http://www.rstudio.com/ (accessed on 22 June 2020).
- World Health Organization. Antimicrobial Resistance: Global Report on Surveillance. 2014. Available online: https://apps.who.int/iris/handle/10665/112642 (accessed on 23 June 2020).
- Morrill, H.J.; Pogue, J.M.; Kaye, K.S.; LaPlante, K.L. Treatment Options for Carbapenem-Resistant Enterobacteriaceae Infections. Open Forum Infect. Dis. 2015, 2, ofv050. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.-Y.; Wang, Y.; Walsh, T.R.; Yi, L.-X.; Zhang, R.; Spencer, J.; Doi, Y.; Tian, G.; Dong, B.; Huang, X.; et al. Emergence of plasmid-mediated colistin resistance mechanism MCR-1 in animals and human beings in China: A microbiological and molecular biological study. Lancet Infect. Dis. 2016, 16, 161–168. [Google Scholar] [CrossRef]
- Liu, Y.-Y.; Wang, Y.; Walsh, T.R.; Yi, L.-X.; Zhang, R.; Spencer, J.; Doi, Y.; Tian, G.; Dong, B.; Huang, X.; et al. Colistin Versus Ceftazidime-Avibactam in the Treatment of Infections Due to Carbapenem-Resistant Enterobacteriaceae. Clin. Infect Dis. 2018, 66, 163–171. [Google Scholar] [CrossRef]
- Simon, M.S.; Sfeir, M.M.; Calfee, D.P.; Satlin, M.J. Cost-effectiveness of ceftazidime-avibactam for treatment of carbapenem-resistant Enterobacteriaceae bacteremia and pneumonia. Antimicrob. Agents Chemother. 2019, 63, e00897-19. [Google Scholar] [CrossRef]
- Falagas, M.E.; Giannopoulou, K.P.; Kokolakis, G.N.; Rafailidis, P.I. Fosfomycin: Use beyond urinary tract and gastrointestinal infections. Clin. Infect. Dis. 2008, 46, 1069–1077. [Google Scholar] [CrossRef]
- Zurita, J. Resistencia Bacteriana en el Ecuador. In Quito, Ecuador, 1st ed.; Centro de Publicaciones Pontificia Universidad Católica del Ecuador: Quito, Ecuador, 2012. [Google Scholar]
- Vardakas, K.Z.; Legakis, N.J.; Triarides, N.; Falagas, M.E. Susceptibility of contemporary isolates to fosfomycin: A systematic review of the literature. Int. J. Antimicrob. Agents 2016, 47, 269–285. [Google Scholar] [CrossRef]
- CLSI. Development of In Vitro Susceptibility Testing Criteria and Quality Control Parameters, 3rd ed.; CLSI Document M23-A3; CLSI: Wayne, PA, USA, 2008. [Google Scholar]
- Endimiani, A.; Patel, G.; Hujer, K.M.; Swaminathan, M.; Perez, F.; Rice, L.B.; Jacobs, M.R.; Bonomo, R.A. In vitro activity of fosfomycin against blaKPC-containing Klebsiella pneumoniae isolates, including those nonsusceptible to tigecycline and/or colistin. Antimicrob. Agents Chemother. 2010, 54, 526–529. [Google Scholar] [CrossRef]
- Endimiani, A.; Patel, G.; Hujer, K.M.; Swaminathan, M.; Perez, F.; Rice, L.B.; Jacobs, M.R.; Bonomo, R.A. Antimicrobial susceptibilities of commonly encountered bacterial isolates to fosfomycin determined by agar dilution and disk diffusion methods. Antimicrob. Agents Chemother. 2011, 55, 4295–4301. [Google Scholar] [CrossRef]
- Kaase, M.; Szabados, F.; Anders, A.; Gatermann, S.G. Fosfomycin susceptibility in carbapenem-resistant Enterobacteriaceae from Germany. J. Clin. Microbiol. 2014, 52, 1893–1897. [Google Scholar] [CrossRef] [PubMed]
- Bijllaardt, W.V.D.; Schijffelen, M.J.; Bosboom, R.W.; Stuart, J.C.; Diederen, B.; Kampinga, G.; Le, T.-N.; Overdevest, I.; Stals, F.; Voorn, P.; et al. Susceptibility of ESBL Escherichia coli and Klebsiella pneumoniae to fosfomycin in the Netherlands and comparison of several testing methods including Etest, MIC test strip, Vitek2, Phoenix and disc diffusion. J. Antimicrob. Chemother. 2018, 73, 2380–2387. [Google Scholar] [CrossRef] [PubMed]
- Pasteran, F.G.; Lucero, C.; Rapoport, M.; Guerriero, L.; Barreiro, I.; Albornoz, E.; Veliz, O.; Corso, A. Tigecycline and intravenous fosfomycin zone breakpoints equivalent to the EUCAST MIC criteria for Enterobacteriaceae. J. Infect. Dev. Ctries. 2012, 6, 452–456. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Fosfomycin Agar Dilution | ||||||
|---|---|---|---|---|---|---|
| Strains | n | Susceptible (S) | Intermediate (I) | Resistant (R) | ||
| 16 µg/mL | 32 µg/mL | 64 µg/mL | 128 µg/mL | 256 µg/mL | ||
| Klebsiella pneumoniae | 125 | 46 | 37 | 15 | 3 | 24 |
| Klebsiella oxytoca | 4 | 4 | ||||
| Klebsiella ozaenae | 1 | 1 | ||||
| Escherichia coli | 4 | 4 | ||||
| Serratia marcescens | 2 | 2 | ||||
| Morganella morganii | 2 | 1 | 1 | |||
| Citrobacter freundii | 6 | 5 | 1 | |||
| Enterobacter cloacae | 3 | 2 | 1 | |||
| Enterobacter aerogenes | 2 | 1 | 1 | |||
| Citrobacter youngae | 1 | 1 | ||||
| TOTAL | 150 | 63 | 40 | 16 | 4 | 27 |
| Species | n | Agar Dilution | Disk Diffusion | ||||
|---|---|---|---|---|---|---|---|
| S | I | R | S | I | R | ||
| Klebsiella pneumoniae | 125 | 98 | 3 | 24 | 100 | 4 | 21 |
| Klebsiella oxytoca | 4 | 4 | 0 | 0 | 4 | 0 | 0 |
| Klebsiella ozaenae | 1 | 1 | 0 | 0 | 1 | 0 | 0 |
| Escherichia coli | 4 | 4 | 0 | 0 | 4 | 0 | 0 |
| Serratia marcescens | 2 | 2 | 0 | 0 | 2 | 0 | 0 |
| Morganella morganii | 2 | 0 | 1 | 1 | 1 | 0 | 1 |
| Citrobacter freundii | 6 | 5 | 0 | 1 | 5 | 0 | 1 |
| Enterobacter cloacae | 3 | 2 | 0 | 1 | 2 | 0 | 1 |
| Enterobacter aerogenes | 2 | 2 | 0 | 0 | 2 | 0 | 0 |
| Citrobacter youngae | 1 | 1 | 0 | 0 | 1 | 0 | 0 |
| Cohen’s kappa index: 0.88 * | |||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
M., V.A.; Mariño-Brito, E.; Villavicencio, F.; Satán, C.; Villacís, J.E.; Gestal, M.C. Fosfomycin, Applying Known Methods and Remedies to A New Era. Diseases 2020, 8, 31. https://doi.org/10.3390/diseases8030031
M. VA, Mariño-Brito E, Villavicencio F, Satán C, Villacís JE, Gestal MC. Fosfomycin, Applying Known Methods and Remedies to A New Era. Diseases. 2020; 8(3):31. https://doi.org/10.3390/diseases8030031
Chicago/Turabian StyleM., Viviana Albán, Estefanía Mariño-Brito, Fernando Villavicencio, Carolina Satán, José E. Villacís, and Mónica C. Gestal. 2020. "Fosfomycin, Applying Known Methods and Remedies to A New Era" Diseases 8, no. 3: 31. https://doi.org/10.3390/diseases8030031
APA StyleM., V. A., Mariño-Brito, E., Villavicencio, F., Satán, C., Villacís, J. E., & Gestal, M. C. (2020). Fosfomycin, Applying Known Methods and Remedies to A New Era. Diseases, 8(3), 31. https://doi.org/10.3390/diseases8030031