
A Study of Adrenal Incidentaloma-Related Hormonal Assays After First Integration of the Diagnosis Within Primary Healthcare

 , ,
, ,  ,
,  and
and 
Abstract
1. Introduction
Objective
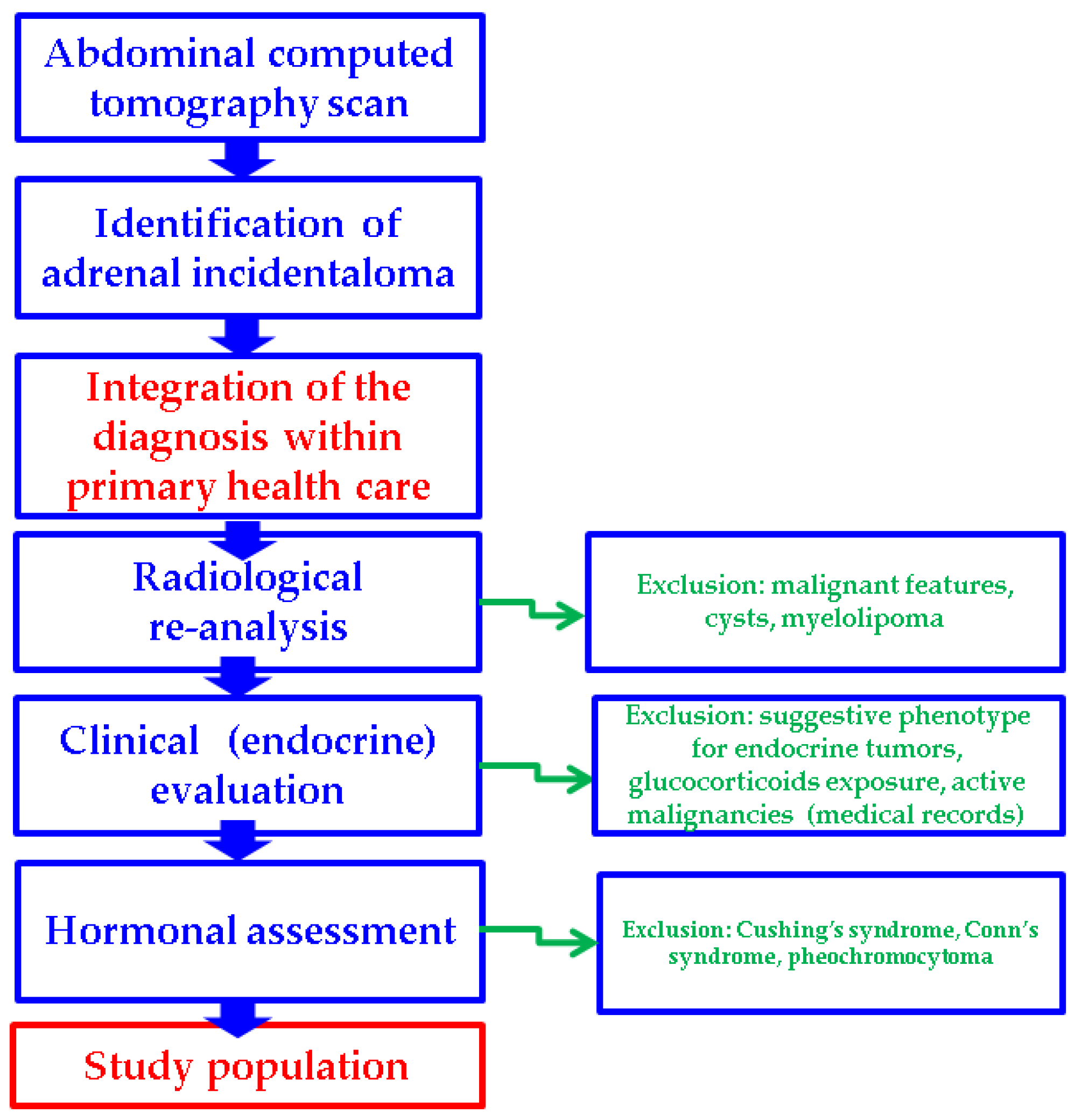
2. Patients and Methods
- clinical aspects and medical records (active malignancies or malignancies under surveillance protocols; subjects under exogenous glucocorticoids exposure (current or during the previous year); suggestive endocrine phenotype for any hormonal ailment)
- radiological appearance (subjects with distinct imaging features at CT scan such as suspected/confirmed primary or secondary adrenal malignancy, adrenal cysts, or myelolipomas)
- endocrine assays consistent with a diagnosis of pheochromocytoma, Conn’s syndrome, or Cushing’s syndrome
3. Results
3.1. Baseline Clinical and Hormonal Features
3.2. Age-Decade Analysis
3.3. Correlations Between the Adrenal Incidentaloma Features
3.4. Gender Analysis
3.5. Unilateral Versus Bilateral Incidentalomas
3.6. MACS-Positive Versus MACS-Negative Profile in Adrenal Tumors
4. Discussion
4.1. Demographic Features and Clinical Picture in Subjects with Adrenal Incidentalomas
4.2. Adrenal Tumor Imaging Assessment Amid CT Scan
4.3. Hormonal Profile in Adrenal Incidentalomas: Focus on MACS
4.4. From Disease Burden to Healthcare System Integration of Patients with Adrenal Incidentalomas
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACTH | adrenocorticotropic hormone |
| BMI | body mass index |
| CT | computed tomography |
| CI | confidence interval |
| C-B | baseline morning plasma cortisol |
| C-6 pm | plasma cortisol at 6 p.m. |
| C-1 mg-DST | second-day plasm cortisol after 1 mg dexamethasone test |
| HBP | high blood pressure |
| M | median |
| N | number of patients |
| NFAs | nonfunctioning adrenal adenomas |
| Q | quartile |
| SD | standard deviation |
| T2DM | type 2 diabetes mellitus |
| vs. | versus |
| UFC | 24-h urinary free cortisol |
Appendix A
References
- Zhang, X.; Si, Y.; Shi, X.; Zhang, Y.; Yang, L.; Yang, J.; Zhang, Y.; Leng, J.; Hu, P.; Liu, H.; et al. Differentiation of multiple adrenal adenoma subtypes based on a radiomics and clinico-radiological model: A dual-center study. BMC Med. Imaging 2025, 25, 45. [Google Scholar] [CrossRef] [PubMed]
- Montalvão, P.V.G.; Mangueira, I.M.; Alves, G.D.M.; Cordeiro, J.V.F.; Costa, M.H.S.; Ravanini, G.D.A.G. Evaluation of adrenal tumors and analysis of the metabolic profile of patients with incidentaloma. Rev. Col. Bras. Cir. 2025, 51, e20243685. [Google Scholar] [CrossRef] [PubMed]
- Janiak, K.; Józwik-Plebanek, K.; Kamiński, G. Recent guidelines for diagnostic and therapeutic management of accidentally detected adrenal tumours (incidentaloma) in adults. Endokrynol. Pol. 2024, 75, 385–394. [Google Scholar] [CrossRef] [PubMed]
- Puglisi, S.; Nekić, A.B.; Morelli, V.; Alessi, Y.; Fosci, M.; Pani, A.; Tomsic, K.Z.; Palmieri, S.; Ferraù, F.; Pia, A.; et al. Are comorbidities of patients with adrenal incidentaloma tied to sex? Front. Endocrinol. 2024, 15, 1385808. [Google Scholar] [CrossRef]
- Rowe, N.E.; Kumar, R.; Schieda, N.; Siddiqi, F.; McGregor, T.; McAlpine, K.; Violette, P.; Bathini, V.; Eng, M.; Izard, J. Diagnosis, Management, and Follow-Up of the Incidentally Discovered Adrenal Mass: CUA Guideline Endorsed by the AUA. J. Urol. 2023, 210, 590–599. [Google Scholar] [CrossRef]
- Fassnacht, M.; Tsagarakis, S.; Terzolo, M.; Tabarin, A.; Sahdev, A.; Newell-Price, J.; Pelsma, I.; Marina, L.; Lorenz, K.; Bancos, I.; et al. European Society of Endocrinology clinical practice guidelines on the management of adrenal incidentalomas, in collaboration with the European Network for the Study of Adrenal Tumors. Eur. J. Endocrinol. 2023, 189, G1–G42. [Google Scholar] [CrossRef]
- Grazzini, G.; Pradella, S.; De Litteris, F.; Galluzzo, A.; Anichini, M.; Treballi, F.; Bicci, E.; Miele, V. Adrenal Mass Evaluation: Suspicious Radiological Signs of Malignancy. Cancers 2025, 17, 849. [Google Scholar] [CrossRef]
- Sobolewska, J.; Respondek, W.; Witek, P. A rare manifestation of adrenocortical carcinoma as a mimic of pheochromocytoma: A case report and literature review. Front. Endocrinol. 2025, 16, 1533711. [Google Scholar] [CrossRef]
- Carsote, M.; Valea, A.; Dumitru, N.; Terzea, D.; Petrova, E.; Albu, S.; Buruiana, A.; Ghemigian, A. Metastases in daily endocrine practice. Arch. Balk. Med. Union 2016, 51, 476–480. [Google Scholar]
- Ngo, B.; Liu, T.; Lau, E. Imaging of Adrenal Incidentalomas: What Actually Happens in Everyday Clinical Practice? J. Med. Imaging Radiat. Oncol. 2025. [Google Scholar] [CrossRef]
- Huang, C.; Chang, L.-Y.; Sheu, J.-Y.; Huang, Y.-T.; Chen, J.-Y.; Lai, C.-F.; Wu, V.-C. Exploring the high prevalence, comorbidities, and indicators of mild autonomous cortisol secretion in primary aldosteronism: A cohort study and systematic review. Hypertens. Res. 2025, 48, 1716–1729. [Google Scholar] [CrossRef] [PubMed]
- Suntornlohanakul, O.; Mandal, S.; Saha, P.; Saygili, E.S.; Asia, M.; Arlt, W.; Elhassan, Y.S.; Prete, A.; Ronchi, C.L. Presentation and management of patients with adrenal masses: A large tertiary centre experience. Eur. J. Endocrinol. 2024, 191, 481–490. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, N.; Sinha, A.; Chakraborty, P.P.; Bhattacharjee, R.; Awasthi, A.; Maiti, A. A Cross-Sectional Study on Comparison of Serum Cortisol Concentration Measured by Chemiluminescent Immunoassay in Four Different Automated Analyzers in a Variety of Adrenal Disorders. Indian. J. Endocrinol. Metab. 2025, 29, 83–88. [Google Scholar] [CrossRef]
- Kjellbom, A.; Löndahl, M.; Danielsson, M.; Olsen, H.; Lindgren, O. Urine-normetanephrine, a predictor of mortality risk in patients with adrenal adenomas. Sci. Rep. 2025, 15, 11145. [Google Scholar] [CrossRef]
- Han, M.-M.; Cao, X.-M.; Liu, Z.-A.; Zhang, Y.; Liu, Y.-F. Continuum of glucose and bone metabolism impairment across autonomous cortisol secretion: A cross-sectional study. World J. Diabetes 2025, 16, 100580. [Google Scholar] [CrossRef]
- Savoie, P.-H.; Murez, T.; Rocher, L.; Neuville, P.; Escoffier, A.; Fléchon, A.; Branger, N.; Camparo, P.; Rouprêt, M. French AFU Cancer Committee Guidelines-Update 2024–2026: Assessment of an adrenal incidentaloma and oncological management. Fr. J. Urol. 2024, 34, 102748. [Google Scholar] [CrossRef]
- Jung, J.; Kim, B.-C.; Kwon, D.; Kim, W.W.; Lee, Y.-M.; Park, K.J.; Lee, S.H.; Chung, K.-W.; Sung, T.-Y. Predictors of malignancy for treatment direction in patients with nonfunctioning adrenal incidentaloma. Surg. Oncol. 2024, 56, 102122. [Google Scholar] [CrossRef]
- Toniolo, A.; Agostini, E.; Ceccato, F.; Tizianel, I.; Cabrelle, G.; Lupi, A.; Pepe, A.; Campi, C.; Quaia, E.; Crimì, F.; et al. Radiomic Analysis of Benign Adrenal Incidentalomas Suggest the Need for Further Endocrinological Evaluation? Curr. Oncol. 2024, 31, 4917–4926. [Google Scholar] [CrossRef]
- Hu, J.; Kassu, R.; Titanji, B.; Kebebew, E. Evaluation of Adrenal Incidentaloma. Surg. Clin. N. Am. 2024, 104, 837–849. [Google Scholar] [CrossRef]
- Boyraz, A.; Candemir, B.; Akın, Ş.; Candemir, M.; Gülçelik, N.E. Increased cardiovascular risk despite unchanged body composition in nonfunctional adrenal incidentaloma. Ann. Endocrinol. 2025, 86, 101687. [Google Scholar] [CrossRef]
- Kastelan, D.; Dusek, T. Do adrenal incidentalomas have an impact on mental health? A comprehensive review. Eur. J. Endocrinol. 2025, 192, R1–R6. [Google Scholar] [CrossRef] [PubMed]
- Erdogan, B.T.; Ogmen, B.E.; Sacikara, M.; Aydin, C.; Topaloglu, O.; Ersoy, R.; Cakir, B. The relationship between mild autonomous cortisol secretion and metabolic diseases in cases with adrenal incidentaloma. Endokrynol. Pol. 2025, 76, 172–181. [Google Scholar] [CrossRef] [PubMed]
- Parasiliti-Caprino, M.; Roux, A.; Campioni, L.; Procopio, M.; Arata, S.; Giannelli, J.; Bollati, M.; Bima, C.; Lopez, C.; Bioletto, F.; et al. Increased cardiometabolic risk and prevalence of ascending aorta dilation in patients with nonfunctioning adrenal incidentaloma: A retrospective propensity score-matched study. Hypertens. Res. 2024, 47, 2874–2883. [Google Scholar] [CrossRef]
- Petramala, L.; Circosta, F.; Marino, L.; Palombi, E.; Costanzo, M.L.; Servello, A.; Galardo, G.; Letizia, C. Clinical Evaluation of Adrenal Incidentaloma: The Experience of a Referral Center. Biomedicines 2024, 12, 1910. [Google Scholar] [CrossRef]
- Meric, C.; Tasci, I.; Akin, S.; Candemir, B.; Guzel Esen, S.; Dag, Z.; Demir, O.; Ersoz Gulcelik, N. Triglyceride-glucose index in patients with non-functioning adrenal incidentaloma, cortisol-secreting adrenal incidentaloma and healthy controls. Am. J. Transl. Res. 2024, 16, 6679–6688. [Google Scholar] [CrossRef]
- Alkan, S.; Guney, S.C.; Akcura, C.; Ozdemir, N.; Hekimsoy, Z. Should adrenal incidentaloma patients be evaluated for muscle mass, function, and quality? A cross-sectional study. Endocrine 2025, 88, 616–626. [Google Scholar] [CrossRef]
- Martino, M.C.D.; Canu, L.; Bonaventura, I.; Vitiello, C.; Sparano, C.; Cozzolino, A. Hypertension and Cushing’s syndrome: Hunt for the red flag. J. Endocrinol. Investig. 2025. [Google Scholar] [CrossRef]
- Jiménez Cassinello, J.M.; Vega-Beyhart, A.; Iriarte, M.B.; Donato, S.; Herrera-Martínez, A.D.; Marazuela, M.; Araujo-Castro, M. Mild autonomous cortisol secretion: Impact on bone health and quality of life. A review. Endocrine 2025. [Google Scholar] [CrossRef]
- Łebek-Szatańska, A.; Januszewicz, A.; Kołodziejczyk-Kruk, S.; Kabat, M.; Śpiewak, M.; Januszewicz, M. How to manage adrenal incidentaloma in a hypertensive patient? Pol. Arch. Intern. Med. 2025, 135, 16949. [Google Scholar] [CrossRef]
- Manea, M.M.; Dragos, D.; Ghenu, M.I.; Enache, I.I.; Stoican, I.C.; Ciulavu, C.; Vasiliu, O.; Sirbu, C.A.; Tuta, S. The Neurocardiogenic Impact of Ischemic Stroke: Intricacies of Cardiac Enzymes and the Vegetative System. Rom. J. Mil. Med. 2025, 128, 36–42. [Google Scholar] [CrossRef]
- Arac, Y.; Yaylali, G.F.; Topsakal, S.; Onder, C. Clinical and Metabolic Characteristics and Follow-Up Results of Adrenal Incidentalomas: A 10-Year Experience. Cureus 2024, 16, e72221. [Google Scholar] [CrossRef] [PubMed]
- Popa, F.L.; Stanciu, M.; Bighea, A.; Berteanu, M.; Totoianu, I.G.; Rotaru, M. Decreased serum levels of sex steroids associated with osteoporosis in a group of Romanian male patients. Rev. Romana Med. Laborator 2016, 24, 75–82. [Google Scholar] [CrossRef]
- Anghel, D.; Ciobica, L.M.; Negru, M.M.; Jurcut, C.; Otlocan, L.; Coca, A. Bone mineral density and vitamin D levels in patients with rheumatoid arthritis. Osteoporos. Int. 2017, 28, S435–S436. [Google Scholar]
- Favero, V.; Parazzoli, C.; Bernasconi, D.P.; Chiodini, I. Cardiometabolic comorbidities and cardiovascular events in “non-functioning” adrenal incidentalomas: A systematic review and meta-analysis. J. Endocrinol. Investig. 2024, 47, 2929–2942. [Google Scholar] [CrossRef]
- Dumitru, N.; Carsote, M.; Cocolos, A.; Petrova, E.; Olaru, M.; Dumitrache, C.; Ghemigian, A. The Link Between Bone Osteocalcin and Energy Metabolism in a Group of Postmenopausal Women. Curr. Health Sci. J. 2019, 45, 47–51. [Google Scholar] [CrossRef]
- Favero, V.; Cairoli, E.; Eller-Vainicher, C.; Morelli, V.; Salcuni, A.S.; Della Casa, S.; Muscogiuri, G.; Columbu, C.; Pugliese, F.; Corbetta, S.; et al. Fragility Fractures and Cortisol Secretion in Patients with Nonfunctioning Adrenal Incidentalomas. J. Endocr. Soc. 2024, 8, bvae144. [Google Scholar] [CrossRef]
- Siemińska, L.; Siemińska, K.; Marek, B.; Kos-Kudła, B.; Nowak, M.; Głogowska-Szeląg, J.; Kajdaniuk, D. Adrenal tumours and subclinical adrenal hyperfunction. Endokrynol. Pol. 2024, 75, 630–642. [Google Scholar] [CrossRef]
- Czapla-Iskrzycka, A.; Świątkowska-Stodulska, R.; Sworczak, K. Comorbidities in Mild Autonomous Cortisol Secretion-A Clinical Review of Literature. Exp. Clin. Endocrinol. Diabetes 2022, 130, 567–576. [Google Scholar] [CrossRef]
- Yozamp, N.; Vaidya, A. Assessment of mild autonomous cortisol secretion among incidentally discovered adrenal masses. Best Pract. Res. Clin. Endocrinol. Metab. 2021, 35, 101491. [Google Scholar] [CrossRef]
- Ivović, M.; Marina, L.V.; Šojat, A.S.; Tančić-Gajić, M.; Arizanović, Z.; Kendereški, A.; Vujović, S. Approach to the Patient with Subclinical Cushing’s Syndrome. Curr. Pharm. Des. 2020, 26, 5584–5590. [Google Scholar] [CrossRef]
- Ren, X.; Nan, M.; Zhang, X. Evaluating the efficacy of surgical and conservative approaches in mild autonomous cortisol secretion: A meta-analysis. Front. Endocrinol. 2024, 15, 1399311. [Google Scholar] [CrossRef] [PubMed]
- Allahwasaya, A.; Akhund, R.; Balachandra, S.; McLeod, C.; Lindeman, B.; Fazendin, J.; Gillis, A.; Zmijewski, P.; Chen, H. Adrenal Referral Pattern: Management of Patients with an Adrenal Incidentaloma. J. Surg. Res. 2024, 302, 144–149. [Google Scholar] [CrossRef] [PubMed]
- AnCeschi, U.; Tufano, A.; Flammia, R.S.; Mormando, M.; Fiori, C.; Zappalà, O.; De Concilio, B.; Carrara, A.; Consiglia, F.M.; Tuderti, G.; et al. Clinical cure vs a novel trifecta system for evaluating long-term outcomes of minimally-invasive partial or total adrenalectomy for unilateral primary aldosteronism: Results of a multicentric series. Cent. Eur. J. Urol. 2022, 75, 345–351. [Google Scholar] [CrossRef]
- Stangl-Kremser, J.; Muto, G.; Grosso, A.A.; Briganti, A.; Comperat, E.; Di Maida, F.; Montironi, R.; Remzi, M.; Pradere, B.; Soria, F.; et al. European Association of Urology-Young Academic Urologists (EAU-YAU): Urothelial carcinoma working group. The impact of lymphovascular invasion in patients treated with radical nephroureterectomy for upper tract urothelial carcinoma: An extensive updated systematic review and meta-analysis. Urol. Oncol. 2022, 40, 243–261. [Google Scholar] [CrossRef]
- Flammia, R.S.; Anceschi, U.; Tuderti, G.; Di Maida, F.; Grosso, A.A.; Lambertini, L.; Mari, A.; Mastroianni, R.; Bove, A.; Capitanio, U.; et al. Development and internal validation of a nomogram predicting 3-year chronic kidney disease upstaging following robot-assisted partial nephrectomy. Int. Urol. Nephrol. 2024, 56, 913–921. [Google Scholar] [CrossRef]
- Candemir, B.; Kisip, K.; Akın, Ş.; Sanal, H.T.; Taşar, M.; Candemir, M.; Gülçelik, N.E. Prevalence and Predictive Features of CT-Derived Nonalcoholic Fatty Liver Disease in Metabolically Healthy MACS. Clin. Endocrinol. 2025, 102, 380–388. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Descriptive Statistics | Value |
|---|---|---|
| Female | N (%) | 47 (78.33) |
| HBP | N (%) | 40 (66.67) |
| T2D | N (%) | 17 (28.37) |
| Age (years) | Mean ± SD | 60.72 ± 10.62 |
| Median (Q1, Q3) | 63.00 (54.00, 67.00) | |
| Minimum, maximum | 40.00, 82.00 | |
| BMI (kg/sqm) | Mean ± SD | 30.37 ± 5.03 |
| Median (Q1, Q3) | 29.85 (26.94, 32.91) | |
| Minimum, maximum | 20.00, 43.63 |
| Parameter | Descriptive Statistics | Value |
|---|---|---|
| MACS-positive | N (%) | 14 (23.33) |
| Unilateral tumor | N (%) | 44 (73.33) |
| Right tumor | N (%) | 18 (30.00) |
| Left tumor | N (%) | 26 (43.33) |
| Bilateral tumors | N (%) | 16 (26.67) |
| Largest tumor diameter (mm) | Mean ± SD | 26.08 ± 8.78 |
| Median (Q1, Q3) | 25.50 (19.00, 32.00) | |
| Minimum, maximum | 10.00, 51.00 | |
| ACTH (pg/mL) (7.20–63.30) | Mean ± SD | 19.19 ± 12.44 |
| Median (Q1, Q3) | 14.50 (11.44, 21.00) | |
| Minimum, maximum | 8.00, 62.44 | |
| C-B (μg/dL) (6.24–18.00) | Mean ± SD | 14.55 ± 5.07 |
| Median (Q1, Q3) | 13.90 (10.68, 18.00) | |
| Minimum, maximum | 5.73, 34.20 | |
| C-6 pm (μg/dL) (2.69–10.40) | Mean ± SD | 5.09 ± 2.34 |
| Median (Q1, Q3) | 4.83 (3.20, 6.62) | |
| Minimum, maximum | 1.30, 11.50 | |
| C-1 mg-DST (μg/dL) (<1.8) | Mean ± SD | 1.94 ± 2.16 |
| Median (Q1, Q3) | 1.32 (0.10, 1.79) | |
| Minimum, maximum | 0.67, 14.50 | |
| UFC (μg/24 h) (11.50–102.00) | Mean ± SD | 38.53 ± 27.51 |
| Median (Q1, Q3) | 34.70 (21.60, 45.85) | |
| Minimum, maximum | 9.50, 148.80 |
| Age Group (Years) | N (%) | Largest Tumor Diameter (mm) Mean ± SD | 95% CI | p-Value |
|---|---|---|---|---|
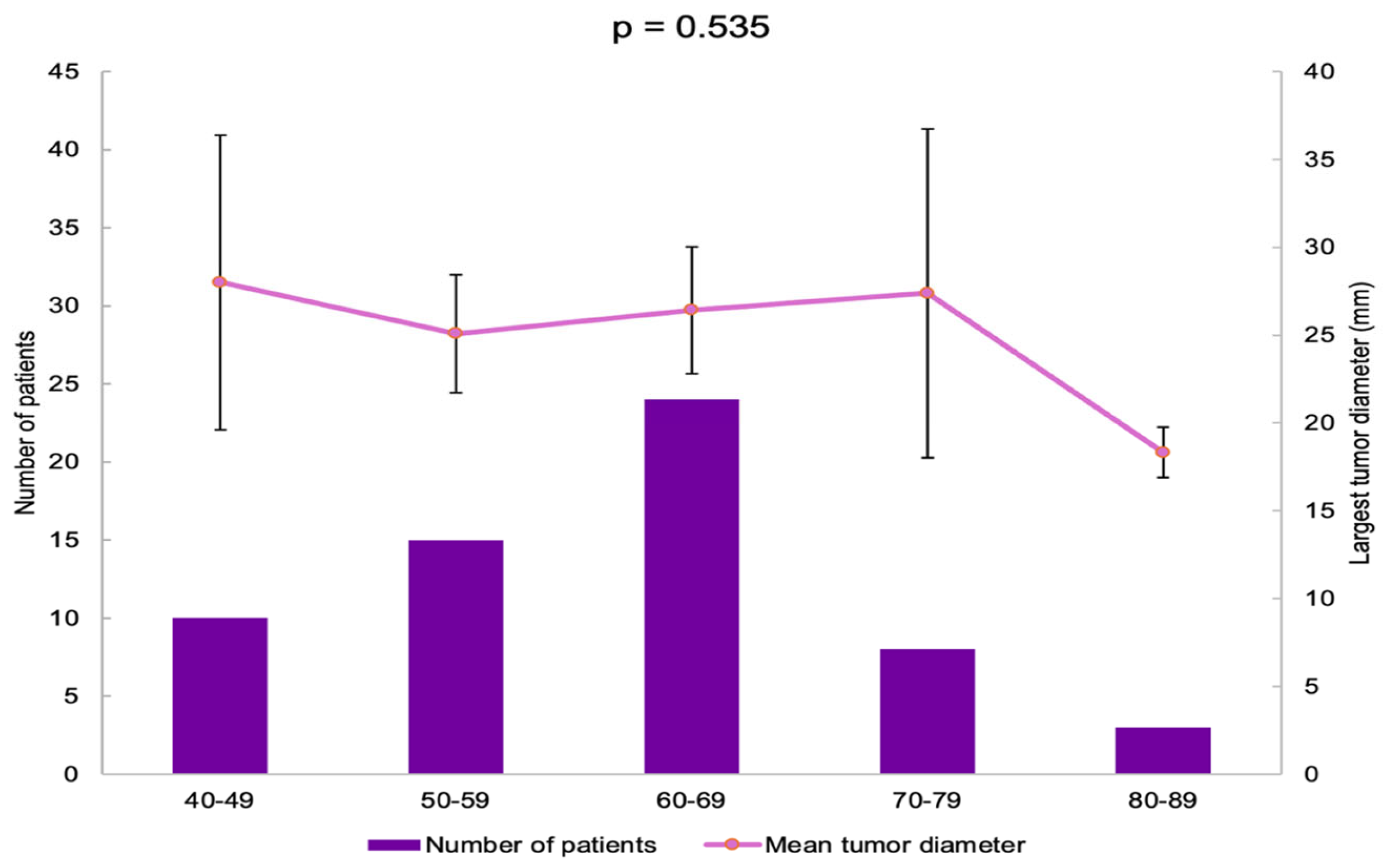
| 40–49 | 10 (16.66) | 28.00 ± 11.72 | 19.62–36.38 | 0.535 |
| 50–59 | 15 (25.00) | 25.09 ± 6.05 | 21.75–28.44 | |
| 60–69 | 24 (40.00) | 26.43 ± 8.54 | 22.83–30.04 | |
| 70–79 | 8 (13.33) | 27.38 ± 11.19 | 18.02–36.73 | |
| 80–89 | 3 (5.00) | 18.33 ± 0.58 | 16.90–19.77 |
| Age Group (Years) | Bilateral Tumors N (%) | Right Adrenal Tumor N (%) | Left Adrenal Tumor N (%) | p-Value |
|---|---|---|---|---|
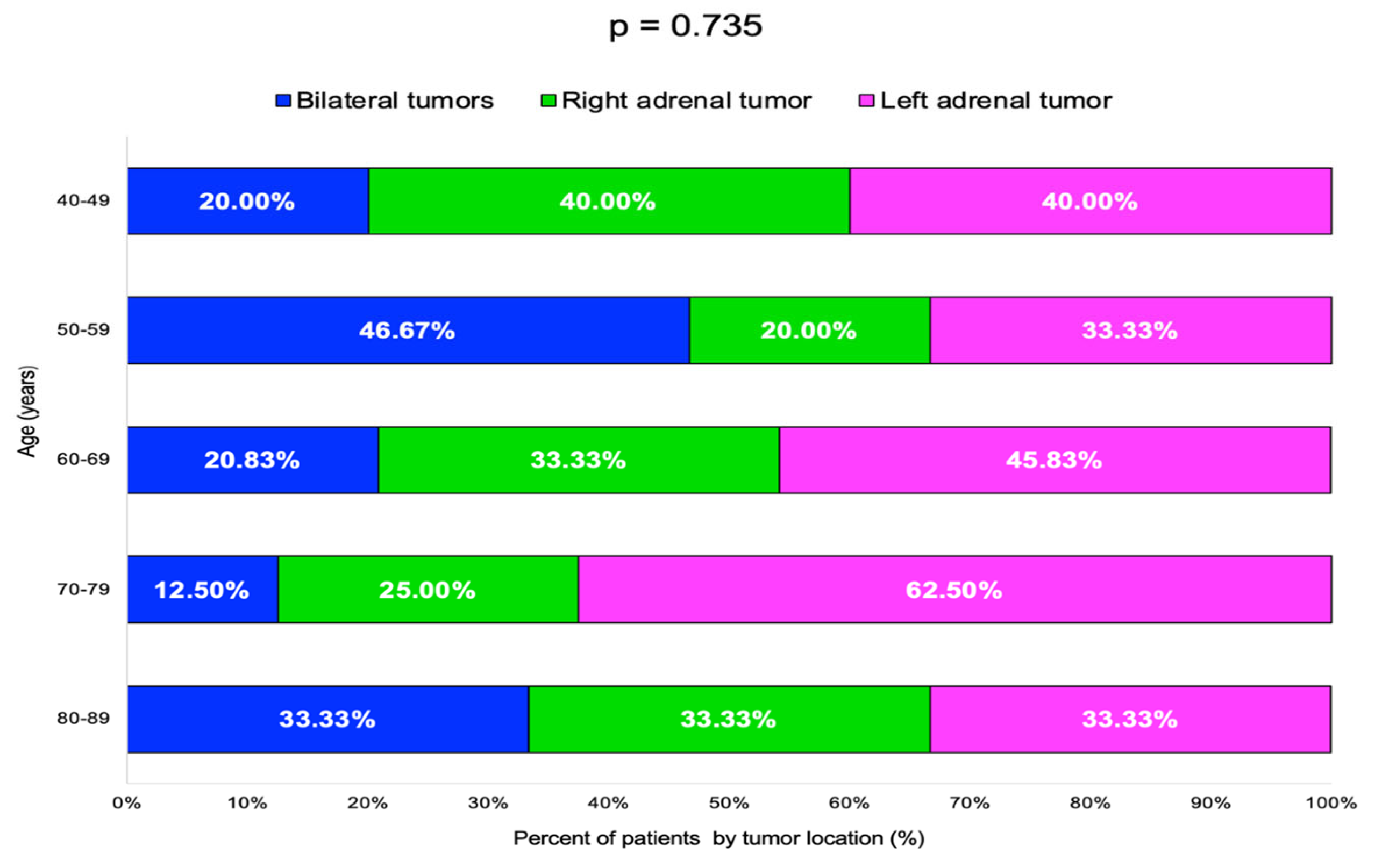
| 40–49 | 2 (20.00) | 4 (40.00) | 4 (40.00) | 0.735 |
| 50–59 | 7 (46.67) | 3 (20.00) | 5 (33.33) | |
| 60–69 | 5 (20.83) | 8 (33.33) | 11 (45.83) | |
| 70–79 | 1 (12.50) | 2 (25.00) | 5 (62.50) | |
| 80–89 | 1 (33.33) | 1 (33.33) | 1 (33.33) |
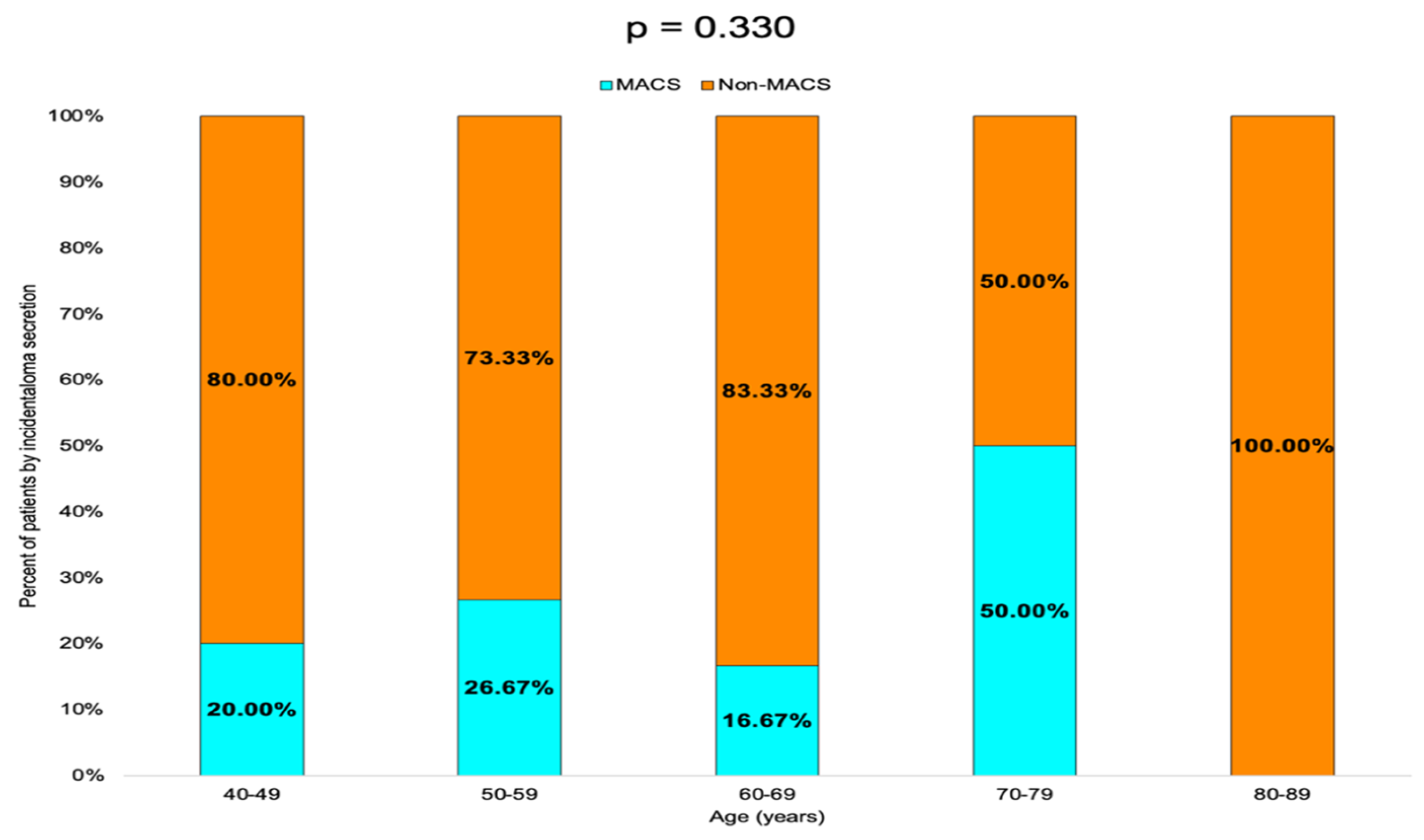
| Age Group (Years) | N (%) | MACS N (%) | Non-MACS N (%) | p-Value |
|---|---|---|---|---|
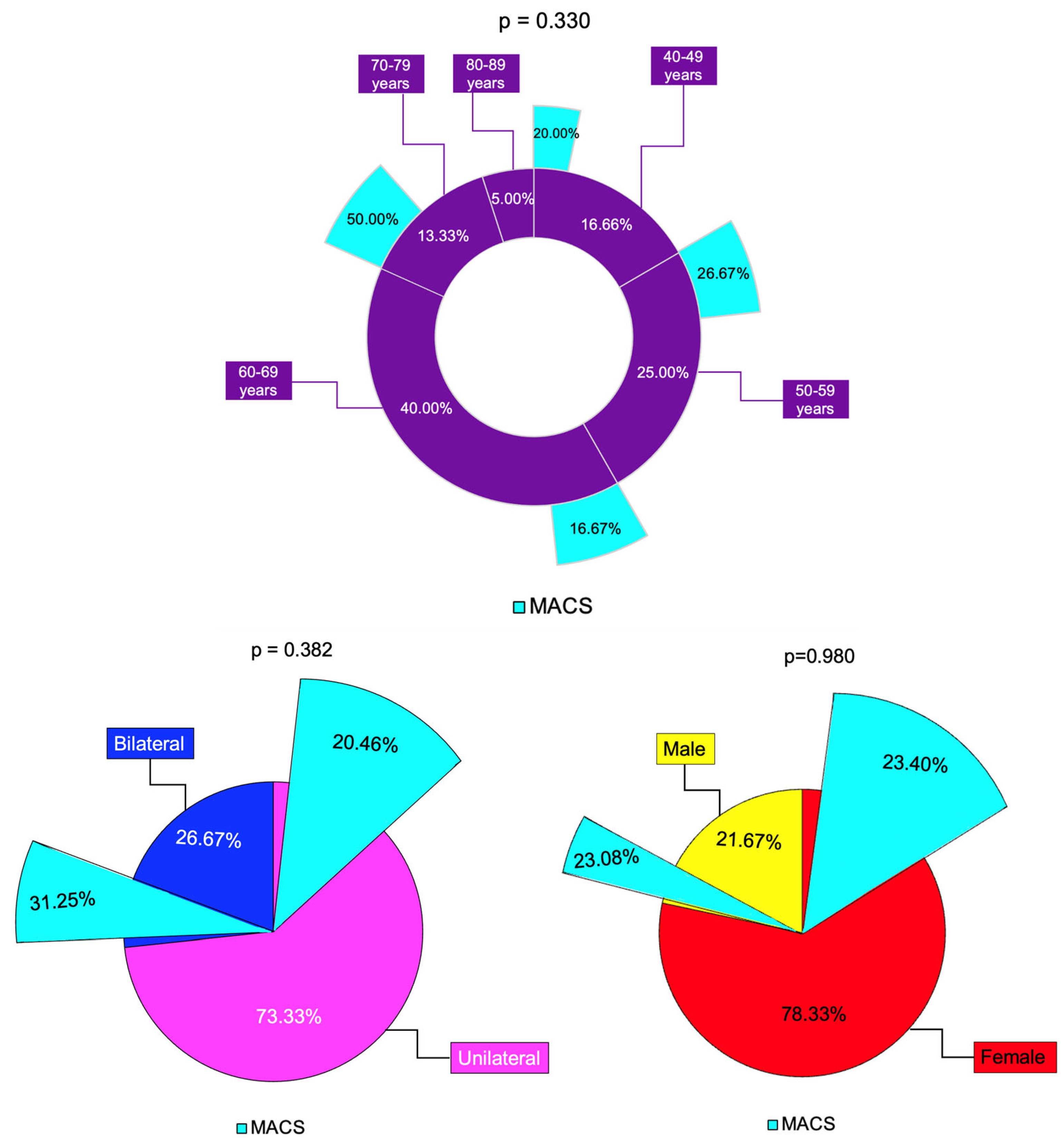
| 40–49 | 10 (16.66) | 2 (20.00) | 8 (80.00) | 0.330 |
| 50–59 | 15 (25.00) | 4 (26.67) | 11 (73.33) | |
| 60–69 | 24 (40.00) | 4 (16.67) | 20 (83.33) | |
| 70–79 | 8 (13.33) | 4 (50.00) | 4 (50.00) | |
| 80–89 | 3 (5.00) | 0 (0.00) | 3 (100.00) |
| Largest Tumor Diameter (mm) | ACTH (pg/mL) | C-B (μg/dL) | C-6 pm (μg/dL) | C-1 mg-DST (μg/dL) | UFC (μg/24 h) | |
|---|---|---|---|---|---|---|
| Age (years) | p = 0.677 r = −0.038 | p = 0.365 r = 0.019 | p = 0.107 r = −0.145 | p = 0.275 r = −0.098 | p = 0.759 r = 0.028 | p = 0.341 r = 0.086 |
| BMI (kg/sqm) | p = 0.583 r = 0.049 | p = 0.481 r = 0.147 | p = 0.030 r = −0.193 | p = 0.515 r = −0.058 | p = 0.198 r = −0.114 | p = 0.038 r = −0.185 |
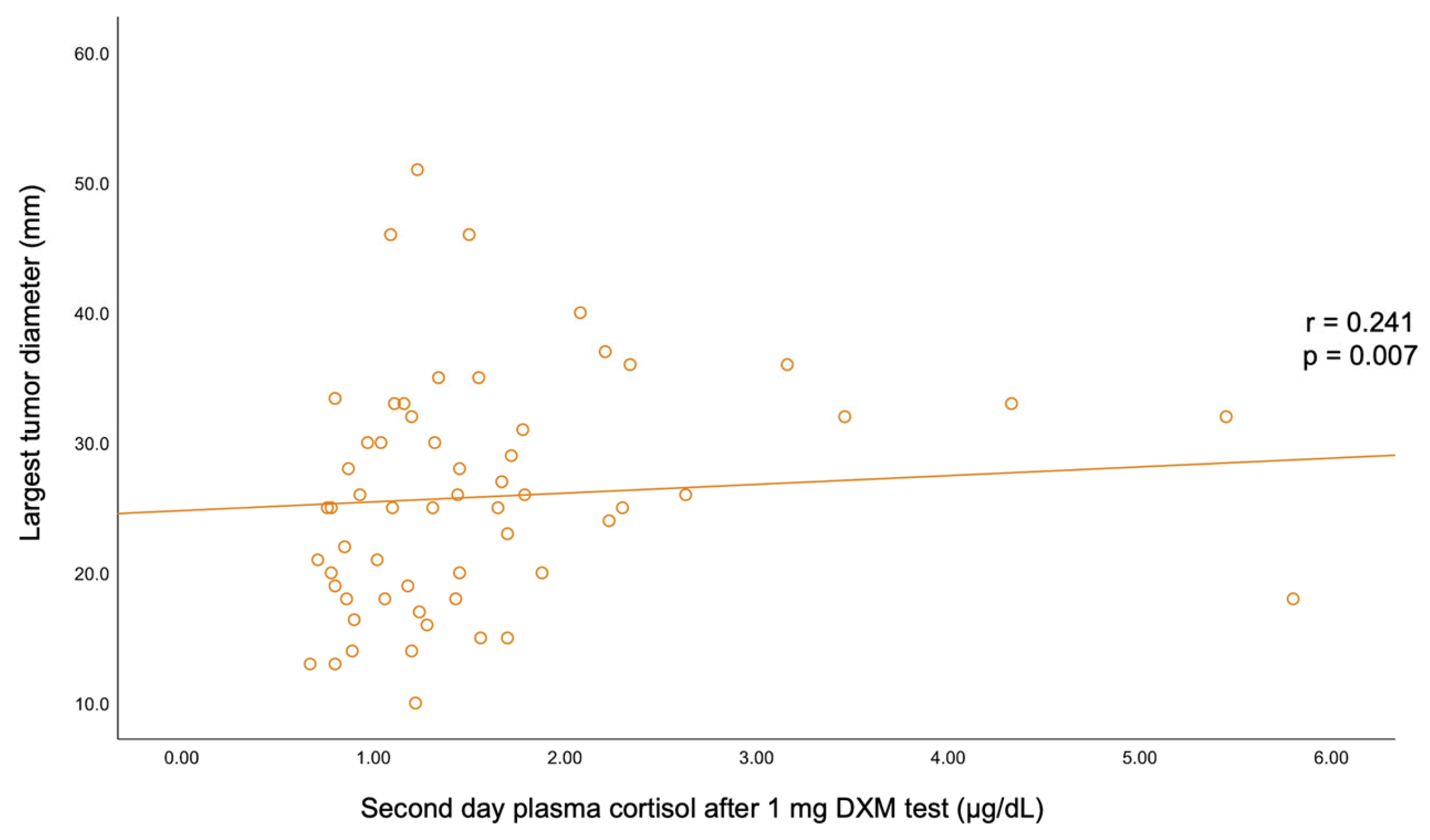
| Largest tumor diameter (mm) | p = 0.415 r = 0.183 | p = 0.627 r = 0.044 | p = 0.325 r = 0.088 | p = 0.007 r = 0.241 | p = 0.999 r = 0.000 | |
| ACTH (pg/mL) | p = 0.415 r = 0.183 | p = 0.255 r = 0.069 | p = 0.194 r = −0.043 | p = 0.135 r = −0.030 | p = 0.520 r = −0.171 | |
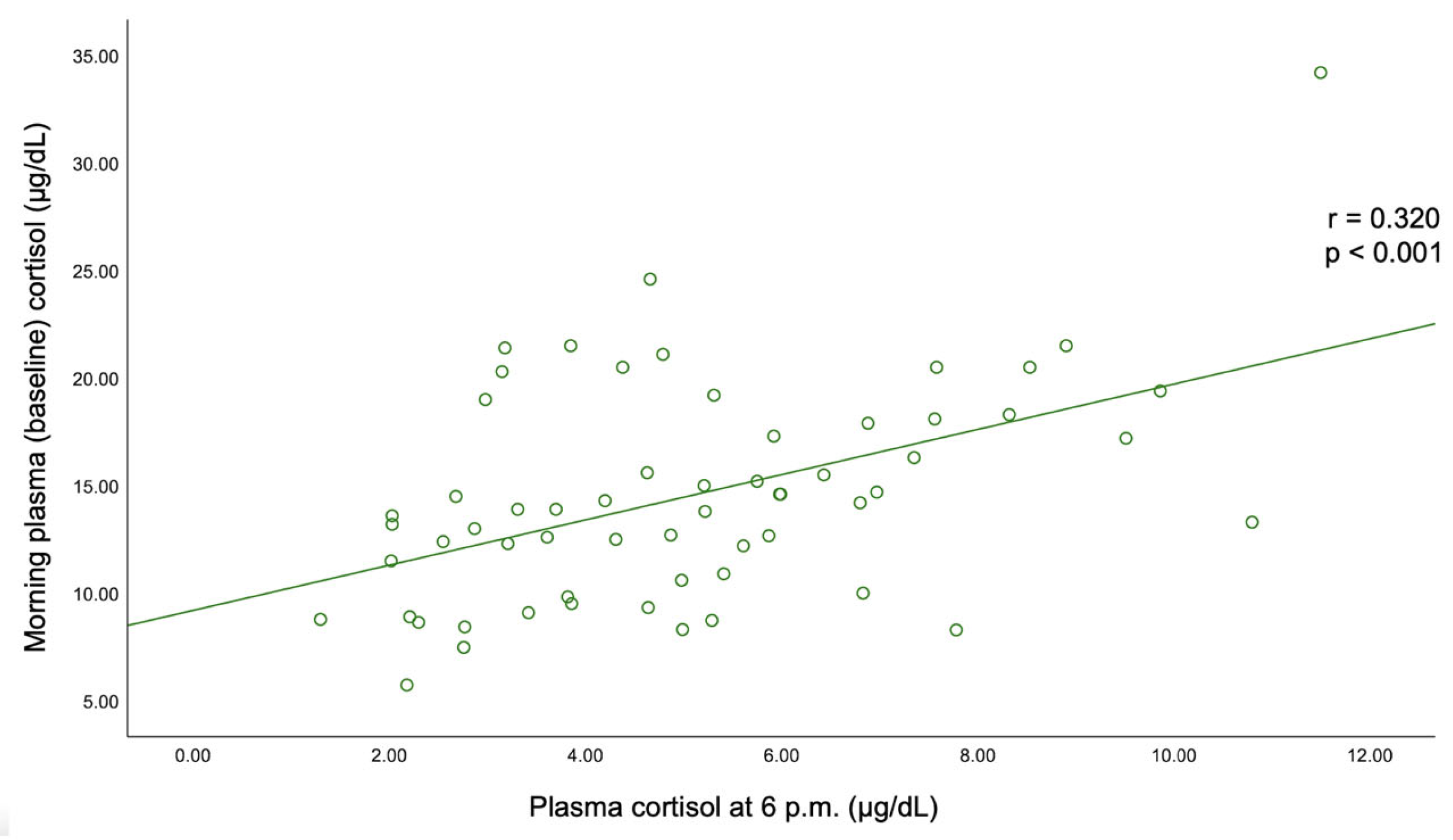
| C-B (μg/dL) | p = 0.627 r = 0.044 | p = 0.255 r = 0.069 | p < 0.001 r = 0.320 | p = 0.623 r = −0.043 | p = 0.011 r = 0.226 | |
| C-6 pm (μg/dL) | p = 0.325 r = 0.088 | p = 0.194 r = −0.043 | p < 0.001 r = 0.320 | p = 0.010 r = 0.229 | p = 0.108 r = 0.143 | |
| C-1 mg-DST (μg/dL) | p = 0.007 r = 0.241 | p = 0.135 r = −0.030 | p = 0.632 r = −0.043 | p = 0.010 r = 0.229 | p = 0.326 r = 0.087 | |
| UFC (μg/24 h) | p = 0.999 r = 0.000 | p = 0.520 r = −0.171 | p = 0.011 r = 0.226 | p = 0.108 r = 0.143 | p = 0.326 r = 0.087 |
| Parameter | Descriptive Statistics | Female (N = 47, 78.33%) | Male (N = 13, 21.67%) | p-Value |
|---|---|---|---|---|
| HBP | N (%) | 30 (63.82) | 10 (76.92) | 0.902 |
| T2D | N (%) | 13 (27.66) | 4 (30.77) | 0.826 |
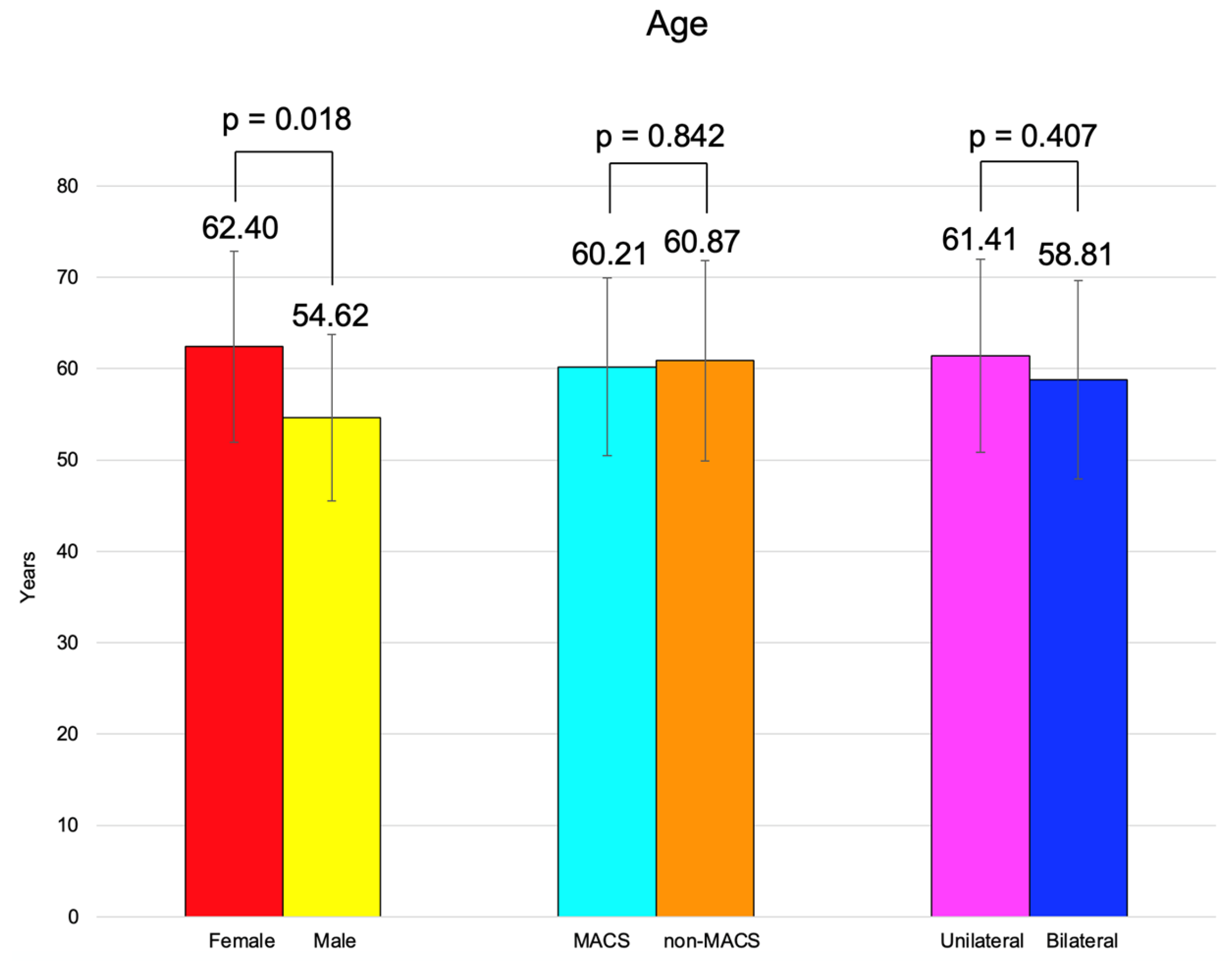
| Age (years) | Mean ± SD | 62.40 ± 10.47 | 54.62 ± 9.11 | 0.018 |
| Median (Q1, Q3) | 65.00 (55.00, 69.00) | 58.00(50.00, 61.00) | ||
| Minimum, maximum | 44.00, 82.00 | 40.00, 66.00 | ||
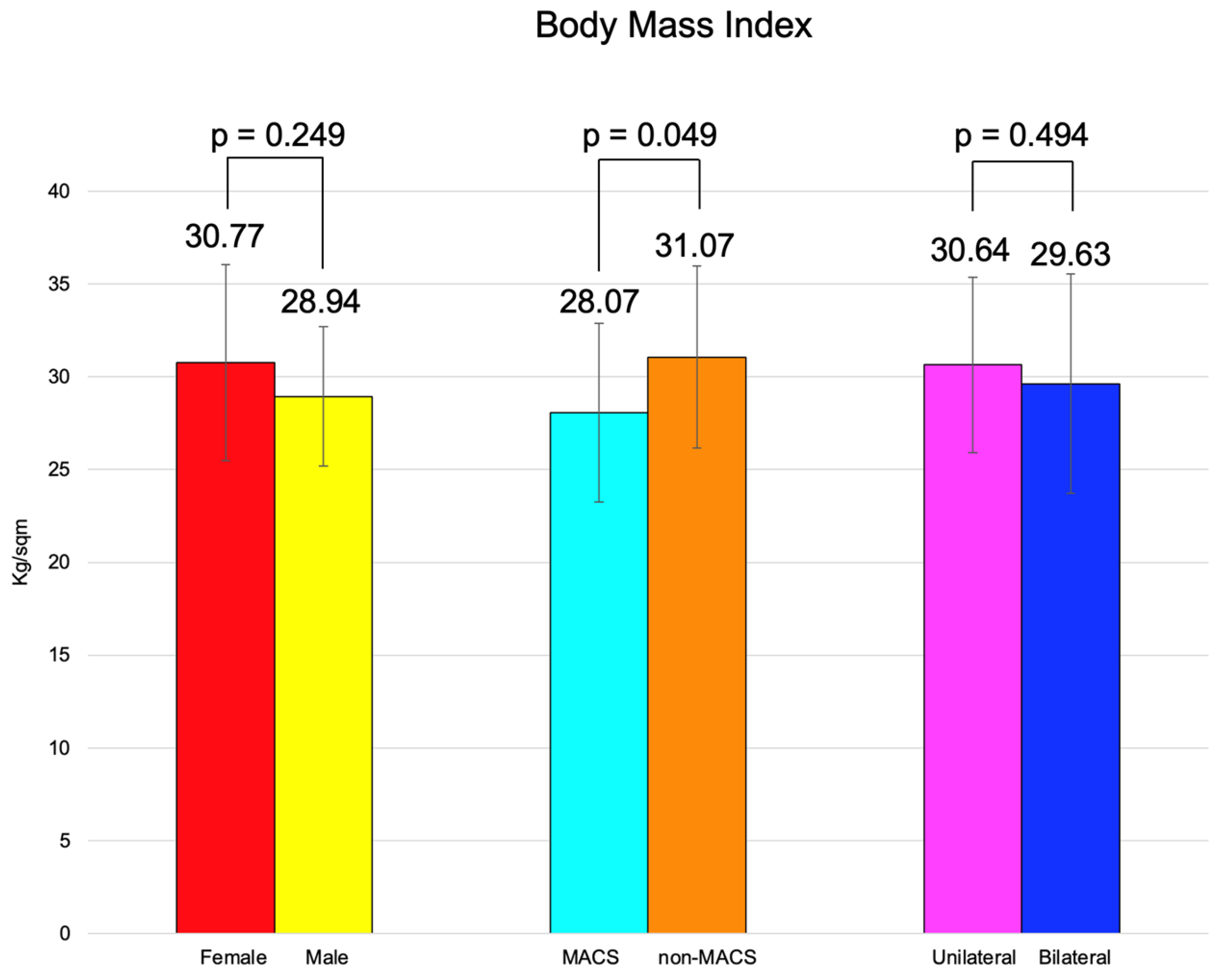
| BMI (kg/sqm) | Mean ± SD | 30.77 ± 5.29 | 28.94 ± 3.76 | 0.249 |
| Median (Q1, Q3) | 30.00 (27.80, 34.36) | 28.08 (25.60, 32.50) | ||
| Minimum, maximum | 20.00, 43.63 | 22.85, 34.60 |
| Parameter | Descriptive Statistics | Female (N = 47, 78.33%) | Male (N = 13, 21.67%) | p-Value |
|---|---|---|---|---|
| MACS-positive | N (%) | 11 (23.40) | 3 (23.08) | 0.980 |
| Unilateral tumor | N (%) | 34 (72.34) | 10 (76.92) | 0.741 |
| Right tumor | N (%) | 13 (27.66) | 5 (38.46) | |
| Left tumor | N (%) | 21 (44.68) | 5 (38.46) | |
| Bilateral tumors | N (%) | 13 (27.66) | 3 (23.08) | |
| Largest tumor diameter (mm) | Mean ± SD | 26.63 ± 9.16 | 24.08 ± 7.23 | 0.357 |
| Median (Q1, Q3) | 26.00 (19.00, 32.50) | 25.00 (20.00, 28.00) | ||
| Minimum, maximum | 13.00, 51.00 | 10.00, 35.00 | ||
| ACTH (pg/mL) (7.20–63.30) | Mean ± SD | 20.47 ± 10.53 | 18.92 ± 11.28 | 0.444 |
| Median (Q1, Q3) | 21.20 (13.50, 29.17) | 25.06 (15.10, 32.00) | ||
| Minimum, maximum | 11.36, 53.80 | 8.00, 50.37 | ||
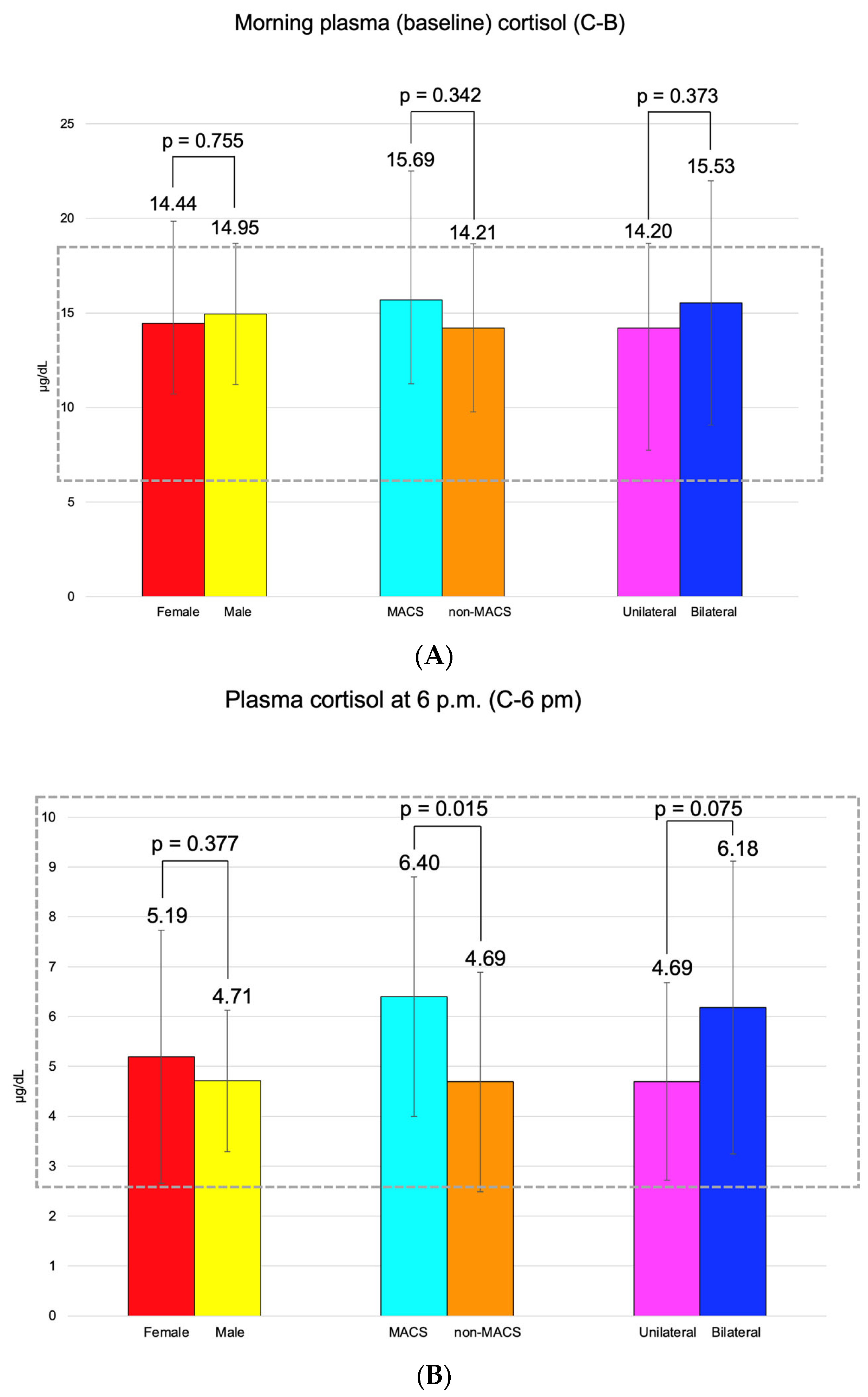
| C-B (μg/dL) (6.24–18.00) | Mean ± SD | 14.44 ± 5.41 | 14.95 ± 3.74 | 0.755 |
| Median (Q1, Q3) | 13.60 (10.30, 18.00) | 14.60 (13.00, 17.30) | ||
| Minimum, maximum | 5.73, 34.20 | 8.90, 20.50 | ||
| C-6 pm (μg/dL) (2.69–10.40) | Mean ± SD | 5.19 ± 2.54 | 4.71 ± 1.42 | 0.377 |
| Median (Q1, Q3) | 4.87 (3.17, 6.86) | 4.63 (4.20, 5.31) | ||
| Minimum, maximum | 1.30, 11.50 | 2.21, 7.58 | ||
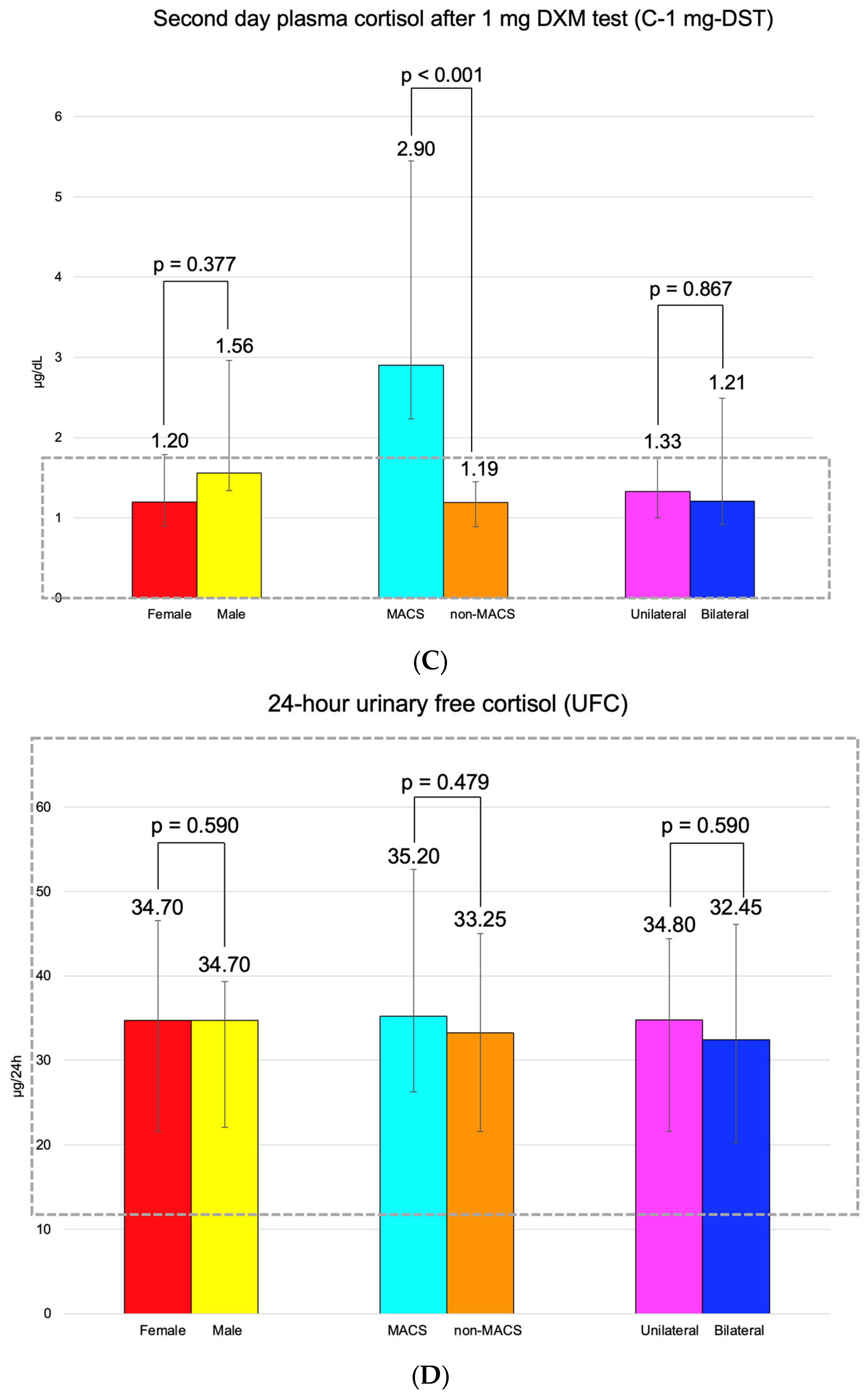
| C-1 mg-DST (μg/dL) (<1.8) | Mean ± SD | 1.99 ± 2.41 | 1.76 ± 0.84 | 0.093 |
| Median (Q1, Q3) | 1.20 (0.90, 1.79) | 1.56 (1.34, 1.70) | ||
| Minimum, maximum | 0.67, 14.50 | 1.04, 4.33 | ||
| UFC (μg/24 h) (11.50–102.00) | Mean ± SD | 40.40 ± 30.04 | 31.75 ± 14.04 | 0.590 |
| Median (Q1, Q3) | 34.70 (21.60, 46.55) | 34.70 (22.10, 39.30) | ||
| Minimum, maximum | 10.60, 148.80 | 9.50, 57.30 |
| Parameter | Descriptive Statistics | Unilateral (N = 44, 73.33%) | Bilateral (N = 16, 26.67%) | p-Value |
|---|---|---|---|---|
| Female | N (%) | 34 (77.27) | 13 (81.25) | 0.741 |
| HBP | N (%) | 28 (63.64) | 12 (75.00) | 0.409 |
| T2D | N (%) | 13 (29.55) | 4 (25.00) | 0.730 |
| Age (years) | Mean ± SD | 61.41 ± 10.57 | 58.81 ± 10.86 | 0.407 |
| Median (Q1, Q3) | 63.00 (53.00, 67.50) | 57.00 (54.50, 65.00) | ||
| Minimum, maximum | 44.00, 82.00 | 40.00, 80.00 | ||
| BMI (kg/sqm) | Mean ± SD | 30.64 ± 4.71 | 29.63 ± 5.92 | 0.494 |
| Median (Q1, Q3) | 30.05 (27.80, 33.30) | 28.92 (24.90, 32.91) | ||
| Minimum, maximum | 22.60, 42.50 | 20.00, 43.63 |
| Parameter | Descriptive Statistics | Unilateral (N = 44, 73.33%) | Bilateral (N = 16, 26.67%) | p-Value |
|---|---|---|---|---|
| MACS-positive | N (%) | 9 (20.46) | 5 (31.25) | 0.382 |
| Largest tumor diameter (mm) | Mean ± SD | 25.51 ± 9.25 | 27.65 ± 7.38 | 0.408 |
| Median (Q1, Q3) | 25.00 (18.00, 30.50) | 29.00 (23.00, 33.20) | ||
| Minimum, maximum | 13.00, 51.00 | 10.00, 36.00 | ||
| ACTH (pg/mL) (7.20–63.30) | Mean ± SD | 19.55 ± 10.96 | 22.67 ± 13.03 | 0.517 |
| Median (Q1, Q3) | 20.59 (12.06, 28.54) | 25.00 (11.32, 36.03) | ||
| Minimum, maximum | 13.85, 62.44 | 12.60, 50.53 | ||
| C-B (μg/dL) (6.24–18.00) | Mean ± SD | 14.20 ± 4.49 | 15.53 ± 6.46 | 0.373 |
| Median (Q1, Q3) | 13.85 (11.20, 17.60) | 14.60 (10.22, 18.20) | ||
| Minimum, maximum | 5.73, 24.60 | 8.29, 34.20 | ||
| C-6 pm (μg/dL) (2.69–10.40) | Mean ± SD | 4.69 ± 1.98 | 6.18 ± 2.94 | 0.075 |
| Median (Q1, Q3) | 4.65 (3.10, 5.90) | 6.00 (3.50, 8.05) | ||
| Minimum, maximum | 1.30, 9.86 | 2.21, 11.50 | ||
| C-1 mg-DST (μg/dL) (<1.8) | Mean ± SD | 1.65 ± 1.10 | 2.73 ± 3.74 | 0.867 |
| Median (Q1, Q3) | 1.33 (1.00, 1.75) | 1.21 (0.92, 2.49) | ||
| Minimum, maximum | 0.67, 5.80 | 0.71, 14.50 | ||
| UFC (μg/24 h) (11.50–102.00) | Mean ± SD | 37.79 ± 26.53 | 40.56 ± 30.86 | 0.953 |
| Median (Q1, Q3) | 34.80 (21.60, 44.40) | 32.45 (20.30, 46.10) | ||
| Minimum, maximum | 9.50, 148.80 | 11.40, 134.40 |
| Parameter | Descriptive Statistics | MACS (N = 14, 23.33%) | Non-MACS (N = 46, 76.67%) | p-Value |
|---|---|---|---|---|
| Female | N (%) | 11 (78.57) | 36 (78.36) | 0.980 |
| HBP | N (%) | 9 (64.29) | 31 (67.4) | 0.625 |
| T2D | N (%) | 1 (7.14) | 16 (34.78) | 0.044 |
| Age (years) | Mean ± SD | 60.21 ± 9.76 | 60.87 ± 10.97 | 0.842 |
| Median (Q1, Q3) | 62.00 (51.00, 70.00) | 63.00 (54.00, 67.00) | ||
| Minimum, maximum | 44.00, 74.00 | 40.00, 82.00 | ||
| BMI (kg/sqm) | Mean ± SD | 28.07 ± 4.83 | 31.07 ± 4.92 | 0.049 |
| Median (Q1, Q3) | 27.64 (25.09, 30.21) | 30.05 (27.90, 33.80) | ||
| Minimum, maximum | 20.00, 36.41 | 22.85, 43.63 |
| Parameter | Descriptive Statistics | MACS (N = 14, 23.33%) | Non-MACS (N = 46, 76.67%) | p-Value |
|---|---|---|---|---|
| Unilateral tumor | N (%) | 9 (64.29) | 35 (76.09) | 0.382 |
| Right tumor | N (%) | 5 (35.71) | 13 (28.26) | |
| Left tumor | N (%) | 4 (28.57) | 22 (47.83) | |
| Bilateral tumors | N (%) | 5 (35.71) | 11 (23.91) | |
| Largest tumor diameter (mm) | Mean ± SD | 30.14 ± 6.81 | 24.84 ± 9.00 | 0.047 |
| Median (Q1, Q3) | 32.00 (24.75, 36.00) | 25.00 (18.00, 30.00) | ||
| Minimum, maximum | 18.00, 40.00 | 10.00, 51.00 | ||
| ACTH (pg/mL) (7.20–63.30) | Mean ± SD | 19.98 ± 9.12 | 21.30 ± 13.02 | 0.371 |
| Median (Q1, Q3) | 22.63 (17.03, 31.19) | 25.06 (17.90, 34.62) | ||
| Minimum, maximum | 13.59, 49.99 | 12.68, 50.94 | ||
| C-B (μg/dL) (6.24–18.00) | Mean ± SD | 15.69 ± 6.81 | 14.21 ± 4.44 | 0.342 |
| Median (Q1, Q3) | 13.95 (10.90, 18.10) | 13.90 (9.83, 17.90) | ||
| Minimum, maximum | 8.29, 34.20 | 5.73, 21.50 | ||
| C-6 pm (μg/dL) (2.69–10.40) | Mean ± SD | 6.40 ± 2.40 | 4.69 ± 2.20 | 0.015 |
| Median (Q1, Q3) | 5.81 (4.98, 7.56) | 4.26 (2.98, 5.98) | ||
| Minimum, maximum | 2.55, 11.50 | 1.30, 9.86 | ||
| C-1 mg-DST (μg/dL) (<1.8) | Mean ± SD | 4.38 ± 3.53 | 1.19 ± 0.33 | <0.001 |
| Median (Q1, Q3) | 2.90 (2.23, 5.45) | 1.19 (0.89, 1.45) | ||
| Minimum, maximum | 1.88, 14.50 | 0.67, 1.79 | ||
| UFC (μg/24 h) (11.50–102.00) | Mean ± SD | 43.41 ± 31.20 | 37.04 ± 26.48 | 0.479 |
| Median (Q1, Q3) | 35.20 (26.30, 52.60) | 33.25 (21.60, 45.00) | ||
| Minimum, maximum | 10.60, 128.40 | 9.50, 148.80 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sima, O.-C.; Costachescu, M.; Valea, A.; Stanciu, M.; Lebada, I.C.; Nistor, T.V.I.; Ciobica, M.-L.; Nistor, C.; Carsote, M. A Study of Adrenal Incidentaloma-Related Hormonal Assays After First Integration of the Diagnosis Within Primary Healthcare. Diseases 2025, 13, 169. https://doi.org/10.3390/diseases13060169
Sima O-C, Costachescu M, Valea A, Stanciu M, Lebada IC, Nistor TVI, Ciobica M-L, Nistor C, Carsote M. A Study of Adrenal Incidentaloma-Related Hormonal Assays After First Integration of the Diagnosis Within Primary Healthcare. Diseases. 2025; 13(6):169. https://doi.org/10.3390/diseases13060169
Chicago/Turabian StyleSima, Oana-Claudia, Mihai Costachescu, Ana Valea, Mihaela Stanciu, Ioana Codruta Lebada, Tiberiu Vasile Ioan Nistor, Mihai-Lucian Ciobica, Claudiu Nistor, and Mara Carsote. 2025. "A Study of Adrenal Incidentaloma-Related Hormonal Assays After First Integration of the Diagnosis Within Primary Healthcare" Diseases 13, no. 6: 169. https://doi.org/10.3390/diseases13060169
APA StyleSima, O.-C., Costachescu, M., Valea, A., Stanciu, M., Lebada, I. C., Nistor, T. V. I., Ciobica, M.-L., Nistor, C., & Carsote, M. (2025). A Study of Adrenal Incidentaloma-Related Hormonal Assays After First Integration of the Diagnosis Within Primary Healthcare. Diseases, 13(6), 169. https://doi.org/10.3390/diseases13060169