
Seroprevalence and Serotypes of Dengue Virus Infection in Ghana: A Systematic Review and Meta-Analysis


{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Information Sources and Search Strategy
2.2. Study Selection and Data Extraction
- Author and year of publication;
- Study design (e.g., cross-sectional, case–control);
- Study setting and period;
- Time frame (e.g., outbreak, non-outbreak);
- Target population and inclusion/exclusion criteria;
- Sample size;
- Types of biological samples (e.g., blood, serum, plasma);
- Dengue diagnostic tests used (e.g., IgM ELISA, IgG ELISA, RT–PCR);
- Main outcome variables (e.g., IgG seroprevalence, IgM seroprevalence, and DENV RNA detection);
- DENV serotypes identified.
2.3. Inclusion Criteria
- Primary research studies conducted among humans of all age groups in Ghana;
- Studies employing serological and/or molecular techniques to detect DENV immunoglobulins (IgG and IgM) and/or RNA;
- No date restrictions were placed on the included studies;
- Studies providing key details on methodology, study characteristics (design, location, population), diagnostic methods used and main findings;
- Studies from all geographical regions and population groups across Ghana.
2.4. Exclusion Criteria
- Review articles, systematic reviews, meta-analyses, case reports, opinion pieces, letters, and conference abstracts—as these do not report primary research;
- Studies conducted outside Ghana or not among human populations;
- Studies detecting antibodies or antigens of pathogens other than dengue virus;
- Studies focusing only on vector surveillance or reporting vector indices without dengue virus detection;
- Studies with incomplete/insufficient methodological information to assess quality and extract relevant data;
- Studies published in languages other than English.
2.5. Quality Assessment
- Was the sample frame appropriate to address the target population?
- Were study participants sampled appropriately?
- Was the sample size adequate?
- Were the study subjects and setting described in detail?
- Was data analysis sufficiently comprehensive of the identified sample?
- Were valid methods used for condition identification?
- Was the condition measured reliably for all participants?
- Was statistical analysis appropriate?
- Was the response rate adequate, and if not, was this managed appropriately?
2.6. Statistical Analysis
3. Results
3.1. Search Results
- Study setting not specified (n = 1);
- Other pathogens/vectors studied (n = 7);
- Unable to access the full text (n = 2).
3.2. Study Characteristics
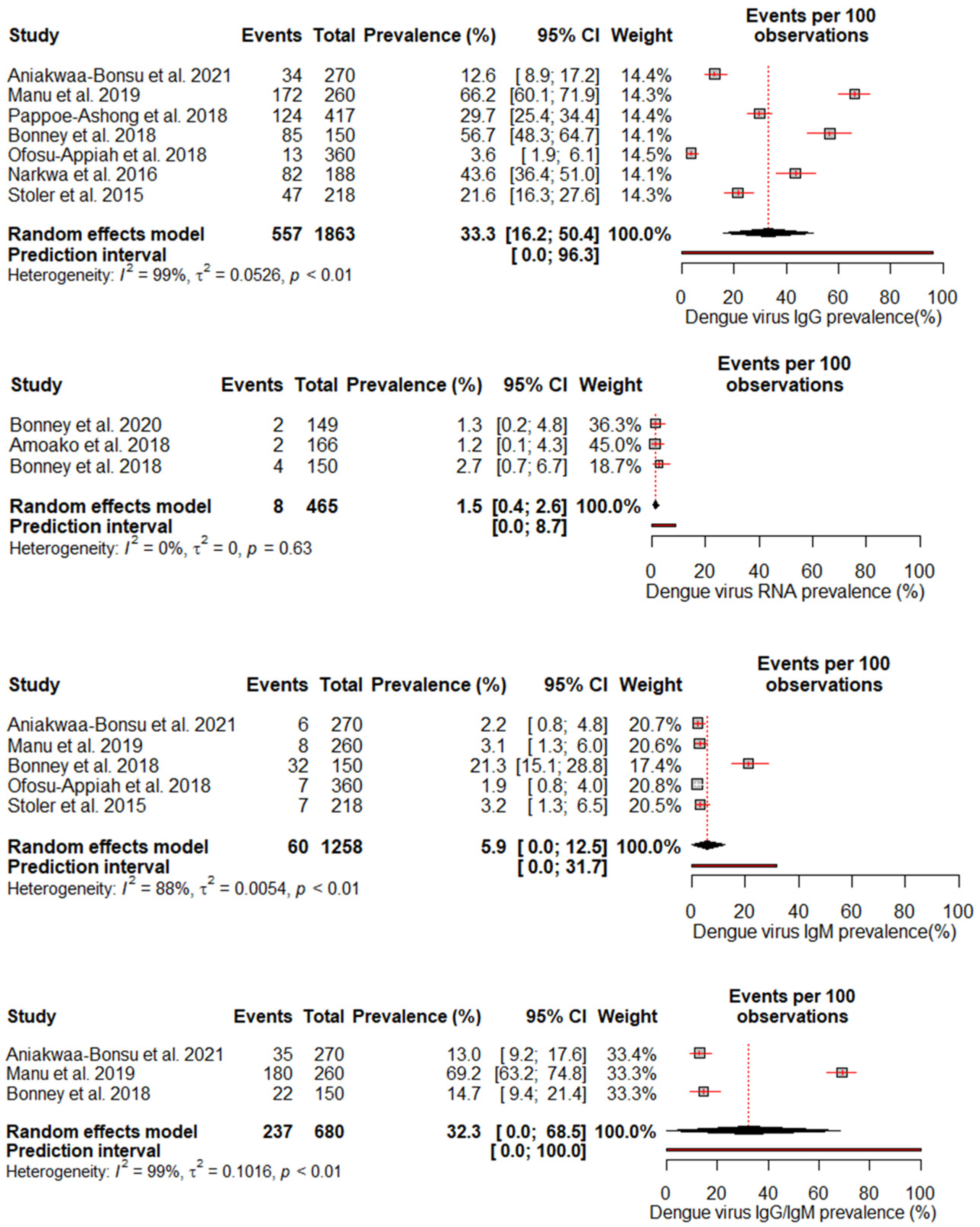
3.3. Pool Prevalence of DENV in Ghana
3.4. Risk of Bias
4. Discussion
Limitations and Recommendations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Sabir, M.J.; Al-Saud, N.B.S.; Hassan, S.M. Dengue and human health: A global scenario of its occurrence, diagnosis and therapeutics. Saudi J. Biol. Sci. 2021, 28, 5074–5080. [Google Scholar] [PubMed]
- Murugesan, A.; Manoharan, M. Dengue Virus. In Emerging and Reemerging Viral Pathogens; Elsevier: Amsterdam, The Netherlands, 2020; pp. 281–359. [Google Scholar]
- Diamond, M.S.; Pierson, T.C. Molecular Insight into Dengue Virus Pathogenesis and Its Implications for Disease Control. Cell 2015, 162, 488–492. [Google Scholar] [CrossRef] [PubMed]
- Sinha, S.; Singh, K.; Ravi Kumar, Y.S.; Roy, R.; Phadnis, S.; Meena, V.; Bhattacharyya, S.; Verma, B. Dengue virus pathogenesis and host molecular machineries. J. Biomed. Sci. 2024, 31, 43. [Google Scholar] [CrossRef]
- Dhole, P.; Zaidi, A.; Nariya, H.K.; Sinha, S.; Jinesh, S.; Srivastava, S. Host Immune Response to Dengue Virus Infection: Friend or Foe? Immuno 2024, 4, 549–577. [Google Scholar]
- Kularatne, S.A.; Dalugama, C. Dengue infection: Global importance, immunopathology and management. Clin. Med. 2022, 22, 9–13. [Google Scholar] [CrossRef]
- Dengue and Severe Dengue. Available online: https://www.who.int/news-room/fact-sheets/detail/dengue-and-severe-dengue (accessed on 25 September 2024).
- Singh, R.K.; Tiwari, A.; Satone, P.D.; Priya, T.; Meshram, R.J. Updates in the management of dengue shock syndrome: A comprehensive review. Cureus 2023, 15, e46713. [Google Scholar]
- Uzair, H.; Waseem, R.; Kumar, N.; Hussain, M.S.; Shah, H.H. Fatal outcome of dengue fever with multi-organ failure and hemorrhage: A case report. SAGE Open Med. Case Rep. 2023, 60, 425. [Google Scholar]
- Ilic, I.; Ilic, M. Global Patterns of Trends in Incidence and Mortality of Dengue, 1990–2019: An Analysis Based on the Global Burden of Disease Study. Medicina 2024, 60, 425. [Google Scholar] [CrossRef]
- Schaefer, T.J.; Panda, P.K.; Wolford, R.W. Dengue Fever. BMJ Best Pract. 2024, 5, 475. [Google Scholar]
- Nakase, T.; Giovanetti, M.; Obolski, U.; Lourenço, J. Population at risk of dengue virus transmission has increased due to coupled climate factors and population growth. Commun. Earth Environ. 2024, 5, 475. [Google Scholar]
- Dengue—Global Situation. Available online: https://www.who.int/emergencies/disease-outbreak-news/item/2024-DON518 (accessed on 25 September 2024).
- Lessa, C.L.; Hodel, K.V.; Gonçalves, M.D.; Machado, B.A. Dengue as a disease threatening global health: A narrative review focusing on Latin America and Brazil. Trop. Med. Infect. Dis. 2023, 8, 241. [Google Scholar] [CrossRef]
- Hossain, M.S.; Noman, A.A.; Mamun, S.M.; Mosabbir, A.A. Twenty-two years of dengue outbreaks in Bangladesh: Epidemiology, clinical spectrum, serotypes, and future disease risks. Trop. Med. Health 2023, 51, 37. [Google Scholar]
- Gainor, E.M.; Harris, E.; LaBeaud, A.D. Uncovering the Burden of Dengue in Africa: Considerations on Magnitude, Misdiagnosis, and Ancestry. Viruses 2022, 14, 233. [Google Scholar] [CrossRef]
- HEALTH ALERT ON DENGUE FEVER—Ministry Of Health [Internet]. Available online: https://www.moh.gov.gh/health-alert-on-dengue-fever/ (accessed on 29 November 2024).
- Stoler, J.; Delimini, R.K.; Bonney, J.K.; Oduro, A.R.; Owusu-Agyei, S.; Fobil, J.N.; Awandare, G.A. Evidence of recent dengue exposure among malaria parasite-positive children in three urban centers in Ghana. Am. J. Trop. Med. Hygiene. 2015, 92, 497–500. [Google Scholar]
- Narkwa, P.W.; Mutocheluh, M.; Kwofie, T.B.; Owusu, M.; Annan, A.; Ali, I.; Boamah, J.K. Dengue virus exposure among blood donors in Ghana. J. Med. Biomed. Sci. 2016, 5, 30–35. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2020, 5, 210. [Google Scholar]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar]
- JBI Critical Appraisal Tools|JBI. Available online: https://jbi.global/critical-appraisal-tools (accessed on 25 September 2024).
- Aniakwaa-Bonsu, E.; Amoako-Sakyi, D.; Dankwa, K.; Prah, J.K.; Nuvor, S.V. Seroprevalence of Dengue Viral Infection among Adults Attending the University of Cape Coast Hospital. Adv. Infect. Dis. 2021, 11, 60–72. [Google Scholar]
- Amoako, N.; Duodu, S.; Dennis, F.E.; Bonney, J.H.; Asante, K.P.; Ameh, J.; Mosi, L.; Hayashi, T.; Agbosu, E.E.; Pratt, D.; et al. Detection of dengue virus among children with suspected malaria, Accra, Ghana. Emerg. Infect. Dis. 2018, 24, 1544–1547. [Google Scholar]
- Bonney, J.H.; Asigbee, T.W.; Kotey, E.; Attiku, K.; Asiedu-Bekoe, F.; Mawuli, G.; Bonney, E.Y.; Asante, I.A.; Abana, C.; Pratt, D.; et al. Molecular detection of viral pathogens from suspected viral hemorrhagic fever patients in Ghana. Health Sci. Investig. J. 2020, 1, 31–35. [Google Scholar]
- Bonney, J.H.; Hayashi, T.; Dadzie, S.; Agbosu, E.; Pratt, D.; Nyarko, S.; Asiedu-Bekoe, F.; Ido, E.; Sarkodie, B.; Ohta, N.; et al. Molecular detection of dengue virus in patients suspected of Ebola virus disease in Ghana. PLoS ONE 2018, 13, e0208907. [Google Scholar]
- Manu, S.K.; Bonney, J.H.; Pratt, D.; Abdulai, F.N.; Agbosu, E.E.; Frimpong, P.O.; Adiku, T.K. Arbovirus circulation among febrile patients at the greater Accra Regional Hospital, Ghana. BMC Res. Notes 2019, 12, 332. [Google Scholar]
- Pappoe-Ashong, P.J.; Ofosu-Appiah, L.H.; Mingle, J.A.; Jassoy, C. Seroprevalence of dengue virus infections in Ghana. East Afr. Med. J. 2018, 95, 2132–2140. [Google Scholar]
- Ofosu-Appiah, L.; Kutame, R.; Ayensu, B.; Bonney, J.; Boateng, G.; Adade, R.; Opare, D.; Odoom, J. Detection of Dengue Virus in Samples from Suspected Yellow Fever Cases in Ghana. Microbiol. Res. J. Int. 2018, 24, 1–10. [Google Scholar]
- Nigussie, E.; Atlaw, D.; Negash, G.; Gezahegn, H.; Baressa, G.; Tasew, A.; Zembaba, D. A dengue virus infection in Ethiopia: A systematic review and meta-analysis. BMC Infect Dis. 2024, 24, 297. [Google Scholar]
- Simo, F.B.; Bigna, J.J.; Kenmoe, S.; Ndangang, M.S.; Temfack, E.; Moundipa, P.F.; Demanou, M. Dengue virus infection in people residing in Africa: A systematic review and meta-analysis of prevalence studies. Sci. Rep. 2019, 9, 13626. [Google Scholar]
- Mwanyika, G.O.; Mboera, L.E.; Rugarabamu, S.; Ngingo, B.; Sindato, C.; Lutwama, J.J.; Paweska, J.T.; Misinzo, G. Dengue Virus Infection and Associated Risk Factors in Africa: A Systematic Review and Meta-Analysis. Viruses 2021, 13, 536. [Google Scholar] [CrossRef]
- Eltom, K.; Enan, K.; El Hussein, A.R.M.; Elkhidir, I.M. Dengue Virus Infection in Sub-Saharan Africa Between 2010 and 2020: A Systematic Review and Meta-Analysis. Front. Cell. Infect. Microbiol. 2021, 11, 678945. [Google Scholar]
- Ganeshkumar, P.; Murhekar, M.V.; Poornima, V.; Saravanakumar, V.; Sukumaran, K.; Anandaselvasankar, A.; John, D.; Mehendale, S.M. Dengue infection in India: A systematic review and meta-analysis. PLoS Negl. Trop. Dis. 2018, 12, e0006618. [Google Scholar]
- Raafat, N.; Blacksell, S.D.; Maude, R.J. A review of dengue diagnostics and implications for surveillance and control. Trans. R. Soc. Trop. Med. Hyg. 2019, 113, 653–660. [Google Scholar]
- Alfsnes, K.; Eldholm, V.; Gaunt, M.W.; de Lamballerie, X.; Gould, E.A.; Pettersson, J.H.O. Tracing and tracking the emergence, epidemiology and dispersal of dengue virus to Africa during the 20th century. One Health 2021, 92, 999–1005. [Google Scholar]
- Mercy, K.; Youm, E.; Aliddeki, D.; Faria, N.R.; Kebede, Y.; Ndembi, N. The Looming Threat of Dengue Fever: The Africa Context. Open Forum Infect Dis. 2024, 11, ofae362. [Google Scholar]
- Yung, C.F.; Lee, K.S.; Thein, T.L.; Tan, L.K.; Gan, V.C.; Wong, J.G.; Lye, D.C.; Ng, L.C.; Leo, Y.S. Dengue Serotype-Specific Differences in Clinical Manifestation, Laboratory Parameters and Risk of Severe Disease in Adults, Singapore. Am. Soc. Trop. Med. Hyg. 2015, 92, 999–1005. [Google Scholar]
- Fibriansah, G.; Lim, X.N.; Lok, S.M. Morphological Diversity and Dynamics of Dengue Virus Affecting Antigenicity. Viruses 2021, 13, 1446. [Google Scholar] [CrossRef]
- Goh, G.K.M.; Dunker, A.K.; Uversky, V.N. Correlating Flavivirus virulence and levels of intrinsic disorder in shell proteins: Protective roles vs. immune evasion. Mol. Biosyst. 2016, 12, 1881–1891. [Google Scholar]
- Goh, G.; Dunker, A.; Foster, J.; Uversky, V. Zika and Flavivirus Shell Disorder: Virulence and Fetal Morbidity. Biomolecules 2019, 9, 710. [Google Scholar] [CrossRef]
- Dumre, S.P.; Bhandari, R.; Shakya, G.; Shrestha, S.K.; Cherif, M.S.; Ghimire, P.; Klungthong, C.; Yoon, I.K.; Hirayama, K.; Na-Bangchang, K.; et al. Dengue Virus Serotypes 1 and 2 Responsible for Major Dengue Outbreaks in Nepal: Clinical, Laboratory, and Epidemiological Features. Am. J. Trop. Med. Hyg. 2017, 97, 1062–1069. [Google Scholar]
- Vicente, C.R.; Herbinger, K.H.; Fröschl, G.; Malta Romano, C.; de Souza Areias Cabidelle, A.; Cerutti Junior, C. Serotype influences on dengue severity: A cross-sectional study on 485 confirmed dengue cases in Vitória, Brazil. BMC Infect. Dis. 2016, 16, 320. [Google Scholar]
- Guzman, M.G.; Vazquez, S. The Complexity of Antibody-Dependent Enhancement of Dengue Virus Infection. Viruses 2010, 2, 2649–2662. [Google Scholar] [CrossRef]
- Aynekulu Mersha, D.G.; van der Sterren, I.; van Leeuwen, L.P.; Langerak, T.; Hakim, M.S.; Martina, B.; van Lelyveld, S.F.; van Gorp, E.C. The role of antibody-dependent enhancement in dengue vaccination. Trop. Dis. Travel. Med. Vaccines 2024, 10, 22. [Google Scholar]
- Nivarthi, U.K.; Swanstrom, J.; Delacruz, M.J.; Patel, B.; Durbin, A.P.; Whitehead, S.S.; Kirkpatrick, B.D.; Pierce, K.K.; Diehl, S.A.; Katzelnick, L.; et al. A tetravalent live attenuated dengue virus vaccine stimulates balanced immunity to multiple serotypes in humans. Nat. Commun. 2021, 12, 1102. [Google Scholar] [CrossRef]
- Garcia-Bates, T.M.; Cordeiro, M.T.; Nascimento, E.J.; Smith, A.P.; Soares de Melo, K.M.; McBurney, S.P.; Evans, J.D.; Marques, E.T.; Barratt-Boyes, S.M. Association between Magnitude of the Virus-Specific Plasmablast Response and Disease Severity in Dengue Patients. J. Immunol. 2013, 190, 80–87. [Google Scholar] [CrossRef]
- Huynh, T.T.T.; Minakawa, N. A comparative study of dengue virus vectors in major parks and adjacent residential areas in Ho Chi Minh City, Vietnam. PLoS Negl. Trop. Dis. 2022, 16, e0010119. [Google Scholar] [CrossRef]
- Pham, H.V.; Doan, H.T.; Phan, T.T.; Tran Minh, N.N. Ecological factors associated with dengue fever in a central highlands Province, Vietnam. BMC Infect. Dis. 2011, 11, 172. [Google Scholar] [CrossRef]
- Lowe, R.; Lee, S.; Martins Lana, R.; Torres Codeço, C.; Castro, M.C.; Pascual, M. Emerging arboviruses in the urbanized Amazon rainforest. BMJ 2020, 11, 206. [Google Scholar] [CrossRef]
- Kabir, M.A.; Zilouchian, H.; Younas, M.A.; Asghar, W. Dengue Detection: Advances in Diagnostic Tools from Conventional Technology to Point of Care. Biosensors 2021, 11, 206. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boamah, I.; Odoom, A.; Sagoe, K.W.C.; Donkor, E.S. Seroprevalence and Serotypes of Dengue Virus Infection in Ghana: A Systematic Review and Meta-Analysis. Diseases 2025, 13, 114. https://doi.org/10.3390/diseases13040114
Boamah I, Odoom A, Sagoe KWC, Donkor ES. Seroprevalence and Serotypes of Dengue Virus Infection in Ghana: A Systematic Review and Meta-Analysis. Diseases. 2025; 13(4):114. https://doi.org/10.3390/diseases13040114
Chicago/Turabian StyleBoamah, Isaac, Alex Odoom, Kwamena W. C. Sagoe, and Eric S. Donkor. 2025. "Seroprevalence and Serotypes of Dengue Virus Infection in Ghana: A Systematic Review and Meta-Analysis" Diseases 13, no. 4: 114. https://doi.org/10.3390/diseases13040114
APA StyleBoamah, I., Odoom, A., Sagoe, K. W. C., & Donkor, E. S. (2025). Seroprevalence and Serotypes of Dengue Virus Infection in Ghana: A Systematic Review and Meta-Analysis. Diseases, 13(4), 114. https://doi.org/10.3390/diseases13040114