

Ocular Tics and Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections (PANDAS)
 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Children with Motor Tics
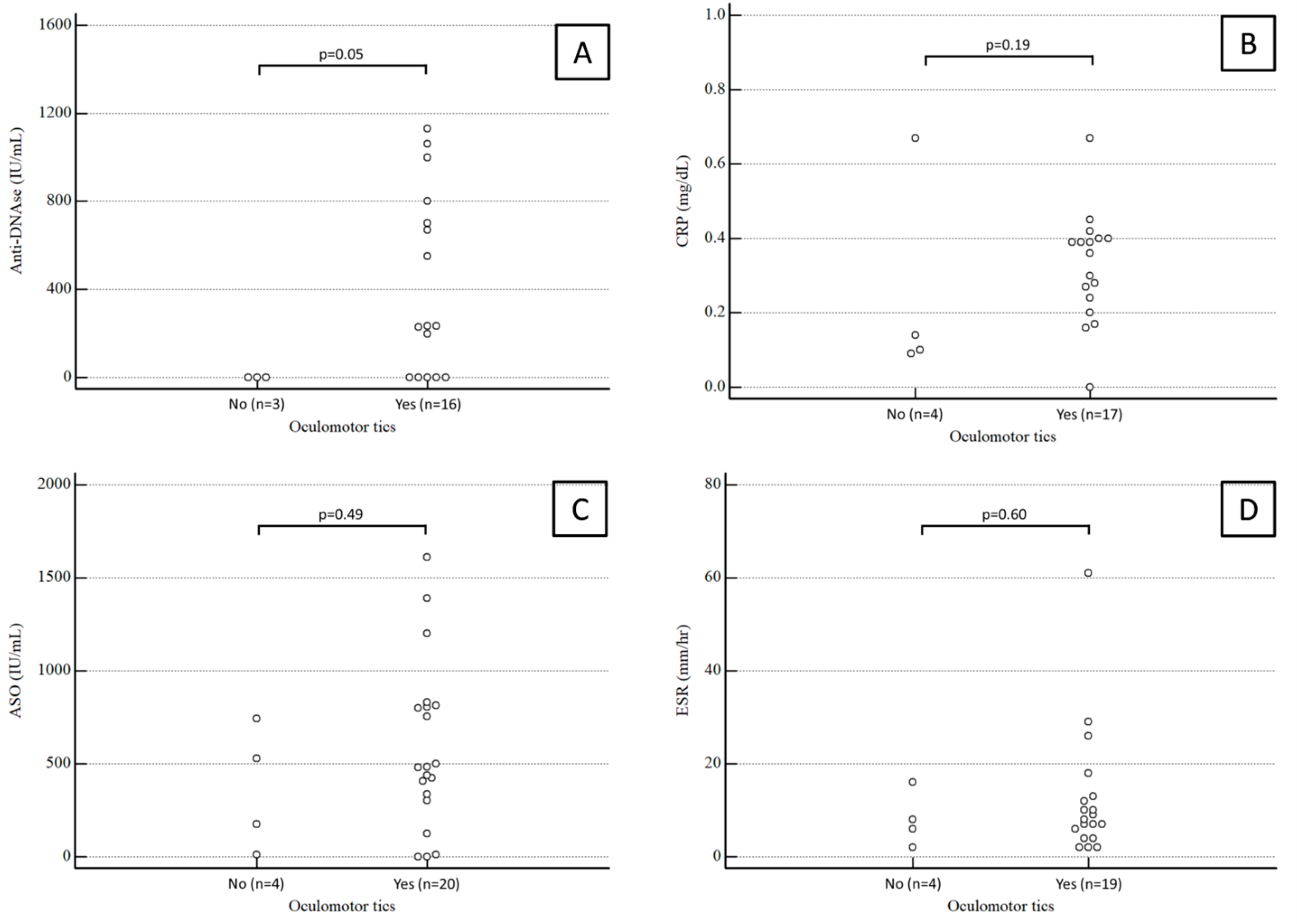
3.2. PANDAS Children
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kurlan, R. Clinical Practice: Tourette’s syndrome. N. Eng. J. Med. 2010, 363, 2332–2338. [Google Scholar] [CrossRef] [PubMed]
- Swedo, S.E.; Leonard, H.L.; Garvey, M.; Mittleman, B.; Allen, A.J.; Perlmutter, S.; Lougee, L.; Dow, S.; Zamkoff, J.; Dubbert, B.K. Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections: Clinical description of the first 50 cases. Am. J. Psychiatry 1998, 155, 264–271. [Google Scholar] [CrossRef] [PubMed]
- Dop, D.; Marcu, I.R.; Padureanu, R.; Niculescu, C.E.; Padureanu, V. Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections (Review). Exp. Ther. Med. 2021, 21, 94. [Google Scholar] [CrossRef] [PubMed]
- Estivill-Domènech, C.; Rodriguez-Morilla, B.; Estivill, E.; Madrid, J.A. Case report: Diagnosis and intervention of a non-24-h sleep-wake disorder in a sighted child with a psychiatric disorder. Front. Psychiatry 2024, 14, 1129153. [Google Scholar] [CrossRef] [PubMed]
- Lepri, G.; Rigante, D.; Bellando Randone, S.; Meini, A.; Ferrari, A.; Tarantino, G.; Cunningham, M.W.; Falcini, F. Clinical-Serological Characterization and Treatment Outcome of a Large Cohort of Italian Children with Pediatric Autoimmune Neuropsychiatric Disorder Associated with Streptococcal Infection and Pediatric Acute Neuropsychiatric Syndrome. J. Child. Adolesc. Psychopharmacol. 2019, 29, 608–614. [Google Scholar] [CrossRef] [PubMed]
- Knight, T.; Steeves, T.; Day, L.; Lowerison, M.; Jette, N.; Pringsheim, T. Prevalence of tic disorders: A systematic review and meta-analysis. Pediatr. Neurol. 2012, 47, 77–90. [Google Scholar] [CrossRef] [PubMed]
- Bisker, E.R.; McClelland, C.M.; Brown, L.W.; Liu, G.T. The long-term outcomes of ocular tics in a pediatric neuro-ophthalmology practice. J. AAPOS 2014, 18, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Martino, D.; Cavanna, A.E.; Robertson, M.M.; Orth, M. Prevalence and phenomenology of eye tics in Gilles de la Tourette syndrome. J. Neurol. 2012, 259, 2137–2140. [Google Scholar] [CrossRef]
- Swedo, S.E.; Leonard, H.L.; Rapoport, J.L. The pediatric autoimmune neuropsychiatric disorders associated with streptococcal infection (PANDAS) subgroup: Separating fact from fiction. Pediatrics 2004, 113, 907–911. [Google Scholar] [CrossRef]
- Wrighton, S.; Ahnlide, V.K.; André, O.; Bahnan, W.; Nordenfelt, P. Group A streptococci induce stronger M protein-fibronectin interaction when specific human antibodies are bound. Front. Microbiol. 2023, 14, 1069789. [Google Scholar] [CrossRef]
- Avire, N.J.; Whiley, H.; Ross, K. A Review of Streptococcus pyogenes: Public Health Risk Factors, Prevention and Control. Pathogens 2021, 10, 248. [Google Scholar] [CrossRef]
- La Bella, S.; Scorrano, G.; Rinaldi, M.; Di Ludovico, A.; Mainieri, F.; Attanasi, M.; Spalice, A.; Chiarelli, F.; Breda, L. Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections (PANDAS): Myth or Reality? The State of the Art on a Controversial Disease. Microorganisms 2023, 11, 2549. [Google Scholar] [CrossRef]
- Kirvan, C.A.; Swedo, S.E.; Kurahara, D.; Cunningham, M.W. Streptococcal mimicry and antibody-mediated cell signaling in the pathogenesis of Sydenham’s chorea. Autoimmunity 2006, 39, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Cox, C.J.; Sharma, M.; Leckman, J.F.; Zuccolo, J.; Zuccolo, A.; Kovoor, A.; Swedo, S.E.; Cunningham, M.W. Brain human monoclonal autoantibody from Sydenham chorea targets dopaminergic neurons in transgenic mice and signals dopamine D2 receptor: Implications in human disease. J. Immunol. 2013, 191, 5524–5541. [Google Scholar] [CrossRef] [PubMed]
- Kirvan, C.A.; Swedo, S.E.; Snider, L.A.; Cunningham, M.W. Antibody-mediated neuronal cell signaling in behavior and movement disorders. J. Neuroimmunol. 2006, 179, 173–179. [Google Scholar] [CrossRef]
- Kirvan, C.A.; Swedo, S.E.; Heuser, J.S.; Cunningham, M.W. Mimicry and autoantibody-mediated neuronal cell signaling in Sydenham chorea. Nat. Med. 2003, 9, 914–920. [Google Scholar] [CrossRef] [PubMed]
- Kirvan, C.A.; Cox, C.J.; Swedo, S.E.; Cunningham, M.W. Tubulin is a neuronal target of autoantibodies in Sydenham’s chorea. J. Immunol. 2007, 178, 7412–7421. [Google Scholar] [CrossRef] [PubMed]
- Vreeland, A.; Thienemann, M.; Cunningham, M.; Muscal, E.; Pittenger, C.; Frankovich, J. Neuroinflammation in Obsessive-Compulsive Disorder: Sydenham Chorea, Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections, and Pediatric Acute Onset Neuropsychiatric Syndrome. Psychiatr. Clin. N. Am. 2023, 46, 69–88. [Google Scholar] [CrossRef] [PubMed]
- Brimberg, L.; Benhar, I.; Mascaro-Blanco, A.; Alvarez, K.; Lotan, D.; Winter, C.; Klein, J.; Moses, A.E.; Somnier, F.E.; Leckman, J.F.; et al. Behavioral, pharmacological, and immunological abnormalities after streptococcal exposure: A novel rat model of Sydenham chorea and related neuropsychiatric disorders. Neuropsychopharmacology 2012, 37, 2076–2087. [Google Scholar] [CrossRef]
- Lotan, D.; Benhar, I.; Alvarez, K.; Mascaro-Blanco, A.; Brimberg, L.; Frenkel, D.; Cunningham, M.W.; Joel, D. Behavioral and neural effects of intra-striatal infusion of anti-streptococcal antibodies in rats. Brain Behav. Immun. 2014, 38, 249–262. [Google Scholar] [CrossRef]
- Chang, K.; Frankovich, J.; Cooperstock, M.; Cunningham, M.W.; Latimer, M.E.; Murphy, T.K.; Pasternack, M.; Thienemann, M.; Williams, K.; Walter, J.; et al. Clinical evaluation of youth with pediatric acute-onset neuropsychiatric syndrome (PANS): Recommendations from the 2013 PANS Consensus Conference. J. Child Adolesc. Psychopharmacol. 2015, 25, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Singer, H.S.; Mascaro-Blanco, A.; Alvarez, K.; Morris-Berry, C.; Kawikova, I.; Ben-Pazi, H.; Thompson, C.B.; Ali, S.F.; Kaplan, E.L.; Cunningham, M.W. Neuronal antibody biomarkers for Sydenham’s chorea identify a new group of children with chronic recurrent episodic acute exacerbations of tic and obsessive-compulsive symptoms following a streptococcal infection. PLoS ONE 2015, 10, e0120499. [Google Scholar] [CrossRef] [PubMed]
- Morris-Berry, C.M.; Pollard, M.; Gao, S.; Thompson, C.; Tourette Syndrome Study Group; Singer, H.S. Anti-streptococcal, tubulin, and dopamine receptor 2 antibodies in children with PANDAS and Tourette syndrome: Single-point and longitudinal assessments. J. Neuroimmunol. 2013, 264, 106–113. [Google Scholar] [CrossRef]
- Dale, R.C. Tics and tourette: A clinical, pathophysiological and etiological review. Curr. Opin. Pediatr. 2017, 29, 665–673. [Google Scholar] [CrossRef] [PubMed]
- Chain, J.L.; Alvarez, K.; Mascaro-Blanco, A.; Reim, S.; Bentley, R.; Hommer, R.; Grant, P.; Leckman, J.F.; Kawikova, I.; Williams, K.; et al. Autoantibody Biomarkers for Basal Ganglia Encephalitis in Sydenham Chorea and Pediatric Autoimmune Neuropsychiatric Disorder Associated with Streptococcal Infections. Front. Psychiatry 2020, 11, 564. [Google Scholar] [CrossRef] [PubMed]
- Prato, A.; Gulisano, M.; Scerbo, M.; Barone, R.; Vicario, C.M.; Rizzo, R. Diagnostic Approach to Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections (PANDAS): A Narrative Review of Literature Data. Front. Pediatr. 2021, 9, 746639. [Google Scholar] [CrossRef] [PubMed]
- Catarina Prior, A.; Tavares, S.; Figueiroa, S.; Temudo, T. Tics en niños y adolescentes: Análisis retrospectivo de 78 casos [Tics in children and adolescents: A retrospective analysis of 78 cases]. An. Pediatría 2007, 66, 129–134. (In Spanish) [Google Scholar] [CrossRef] [PubMed]
- La Bella, S.; Attanasi, M.; Di Ludovico, A.; Scorrano, G.; Mainieri, F.; Ciarelli, F.; Lauriola, F.; Silvestrini, L.; Girlando, V.; Chiarelli, F.; et al. Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections (PANDAS) Syndrome: A 10-Year Retrospective Cohort Study in an Italian Centre of Pediatric Rheumatology. Microorganisms 2023, 12, 8. [Google Scholar] [CrossRef] [PubMed]
- Rea, I.; Guido, C.A.; Spalice, A. Clinical Features in Patients With PANDAS/PANS and Therapeutic Approaches: A Retrospective Study. Front. Neurol. 2021, 12, 741176. [Google Scholar] [CrossRef]
- O’Dor, S.L.; Homayoun, S.; Downer, O.M.; Hamel, M.A.; Zagaroli, J.S.; Williams, K.A. A Survey of Demographics, Symptom Course, Family History, and Barriers to Treatment in Children with Pediatric Acute-Onset Neuropsychiatric Disorders and Pediatric Autoimmune Neuropsychiatric Disorder Associated with Streptococcal Infections. J. Child. Adolesc. Psychopharmacol. 2022, 32, 476–487. [Google Scholar] [CrossRef]
- Thienemann, M.; Murphy, T.; Leckman, J.; Shaw, R.; Williams, K.; Kapphahn, C.; Frankovich, J.; Geller, D.; Bernstein, G.; Chang, K.; et al. Clinical Management of Pediatric Acute-Onset Neuropsychiatric Syndrome: Part I—Psychiatric and Behavioral Interventions. J. Child. Adolesc. Psychopharmacol. 2017, 27, 566–573. [Google Scholar] [CrossRef] [PubMed]
- Frankovich, J.; Swedo, S.; Murphy, T.; Dale, R.C.; Agalliu, D.; Williams, K.; Daines, M.; Hornig, M.; Chugani, H.; Sanger, T.; et al. Clinical Management of Pediatric Acute-Onset Neuropsychiatric Syndrome: Part II—Use of Immunomodulatory Therapies. J. Child. Adolesc. Psychopharmacol. 2017, 27, 574–593. [Google Scholar] [CrossRef]
- Cooperstock, M.S.; Swedo, S.E.; Pasternack, M.S.; Murphy, T.K. Clinical Management of Pediatric Acute-Onset Neuropsychiatric Syndrome: Part III-Treatment and Prevention of Infections. J. Child. Adolesc. Psychopharmacol. 2017, 27, 594–606. [Google Scholar] [CrossRef]
- Snider, L.A.; Lougee, L.; Slattery, M.; Grant, P.; Swedo, S.E. Antibiotic prophylaxis with azithromycin or penicillin for childhood-onset neuropsychiatric disorders. Biol. Psychiatry 2005, 57, 788–792. [Google Scholar] [CrossRef]
- Murphy, T.K.; Parker-Athill, E.C.; Lewin, A.B.; Storch, E.A.; Mutch, P.J. Cefdinir for recent-onset pediatric neuropsychiatric disorders: A pilot randomized trial. J. Child. Adolesc. Psychopharmacol. 2015, 25, 57–64. [Google Scholar] [CrossRef]
- Prus, K.; Weidner, K.; Alquist, C. Therapeutic plasma exchange in adolescent and adult patients with autoimmune neuropsychiatric disorders associated with streptococcal infections. J. Clin. Apher. 2022, 37, 597–599. [Google Scholar] [CrossRef]
- Eremija, J.; Patel, S.; Rice, S.; Daines, M. Intravenous immunoglobulin treatment improves multiple neuropsychiatric outcomes in patients with pediatric acute-onset neuropsychiatric syndrome. Front. Pediatr. 2023, 11, 1229150. [Google Scholar] [CrossRef] [PubMed]
- Obregon, D.; Parker-Athill, E.C.; Tan, J.; Murphy, T. Psychotropic effects of antimicrobials and immune modulation by psychotropics: Implications for neuroimmune disorders. Neuropsychiatry 2012, 2, 331–343. [Google Scholar] [CrossRef]
- Babyak, M.A. What you see may not be what you get: A brief, nontechnical introduction to overfitting in regression-type models. Psychosom. Med. 2004, 66, 411–421. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| All Patients (n = 40) | Children with Ocular Tics (n = 33) | Children without Ocular Tics (n = 7) | p-Value | |
|---|---|---|---|---|
| Age (years) ± SD | 7.65 ± 2.45 | 7.63 ± 2.55 | 7.71 ± 2.14 | 0.94 § |
| Gender (males/females) | 34/6 | 28/5 | 6/1 | 1.00 * |
| Family history of tics (no/yes) | 37/3 | 30/3 | 7/0 | 1.00 * |
| Family history of psychiatric disorders (no/yes) | 23/17 | 20/13 | 3/4 | 0.43 * |
| Family history of autoimmune disorders (no/yes) | 24/16 | 18/15 | 6/1 | 0.21 * |
| Simple motor tics (no/yes) | 2/38 | 0/33 | 2/5 | 0.03 * |
| Complex motor tics (no/yes) | 12/28 | 11/22 | 1/6 | 0.65 * |
| Facial tics (no/yes) | 17/23 | 14/19 | 3/4 | 1.00 * |
| Comorbidities (no/yes) | 22/18 | 18/15 | 4/3 | 1.00 * |
| PANDAS diagnosis (no/yes) | 16/24 | 13/20 | 3/4 | 1.00 * |
| All Patients (n = 24) | Children with Ocular Tics (n = 20) | Children without Ocular Tics (n = 4) | p-Value | |
|---|---|---|---|---|
| Age (years) ± SD | 7.25 ± 2.2 | 7.35 ± 2.18 | 6.75 ± 2.36 | 0.63 § |
| Gender (males/females) | 19/5 | 16/4 | 3/1 | 1.00 * |
| Family history of tics (no/yes) | 21/3 | 17/3 | 4/0 | 1.00 * |
| Family history of psychiatric disorders (no/yes) | 16/8 | 14/6 | 2/2 | 0.58 * |
| Family history of autoimmune disorders (no/yes) | 12/12 | 8/12 | 4/0 | 0.93 * |
| Simple motor tics (no/yes) | 2/22 | 0/20 | 2/2 | 0.02 * |
| Complex motor tics (no/yes) | 5/19 | 5/15 | 0/4 | 0.54 * |
| Facial tics (no/yes) | 12/12 | 9/11 | 3/1 | 0.59 * |
| Comorbidities (no/yes) | 17/7 | 13/7 | 4/0 | 0.28 * |
| Patients (n = 7) | |
|---|---|
| Age (years) ± standard deviation | 7 ± 1.9 |
| Gender (males/females) | 6/1 |
| Family history of tics (no/yes) | 7/0 |
| Family history of psychiatric disorders (no/yes) | 7/0 |
| Family history of autoimmune disorders (no/yes) | 0/7 |
| Simple motor tics (no/yes) | 0/7 |
| Complex motor tics (no/yes) | 0/7 |
| Facial tics (no/yes) | 2/5 |
| Oculomotor tics (no/yes) | 0/7 |
| Comorbidities (no/yes) | 3/4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dore, S.; Satta, D.; Zinellu, A.; Boscia, G.; Carta, A.; Fruschelli, M.; Serra, R.; Pinna, A. Ocular Tics and Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections (PANDAS). Diseases 2024, 12, 83. https://doi.org/10.3390/diseases12050083
Dore S, Satta D, Zinellu A, Boscia G, Carta A, Fruschelli M, Serra R, Pinna A. Ocular Tics and Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections (PANDAS). Diseases. 2024; 12(5):83. https://doi.org/10.3390/diseases12050083
Chicago/Turabian StyleDore, Stefano, Daniele Satta, Angelo Zinellu, Giacomo Boscia, Arturo Carta, Mario Fruschelli, Rita Serra, and Antonio Pinna. 2024. "Ocular Tics and Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections (PANDAS)" Diseases 12, no. 5: 83. https://doi.org/10.3390/diseases12050083
APA StyleDore, S., Satta, D., Zinellu, A., Boscia, G., Carta, A., Fruschelli, M., Serra, R., & Pinna, A. (2024). Ocular Tics and Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections (PANDAS). Diseases, 12(5), 83. https://doi.org/10.3390/diseases12050083