
Acute Effect of Three Aerobic Exercise Intensities on Glomerular Filtration Rate in Healthy Older Adults


Abstract
1. Introduction
2. Materials and Methods
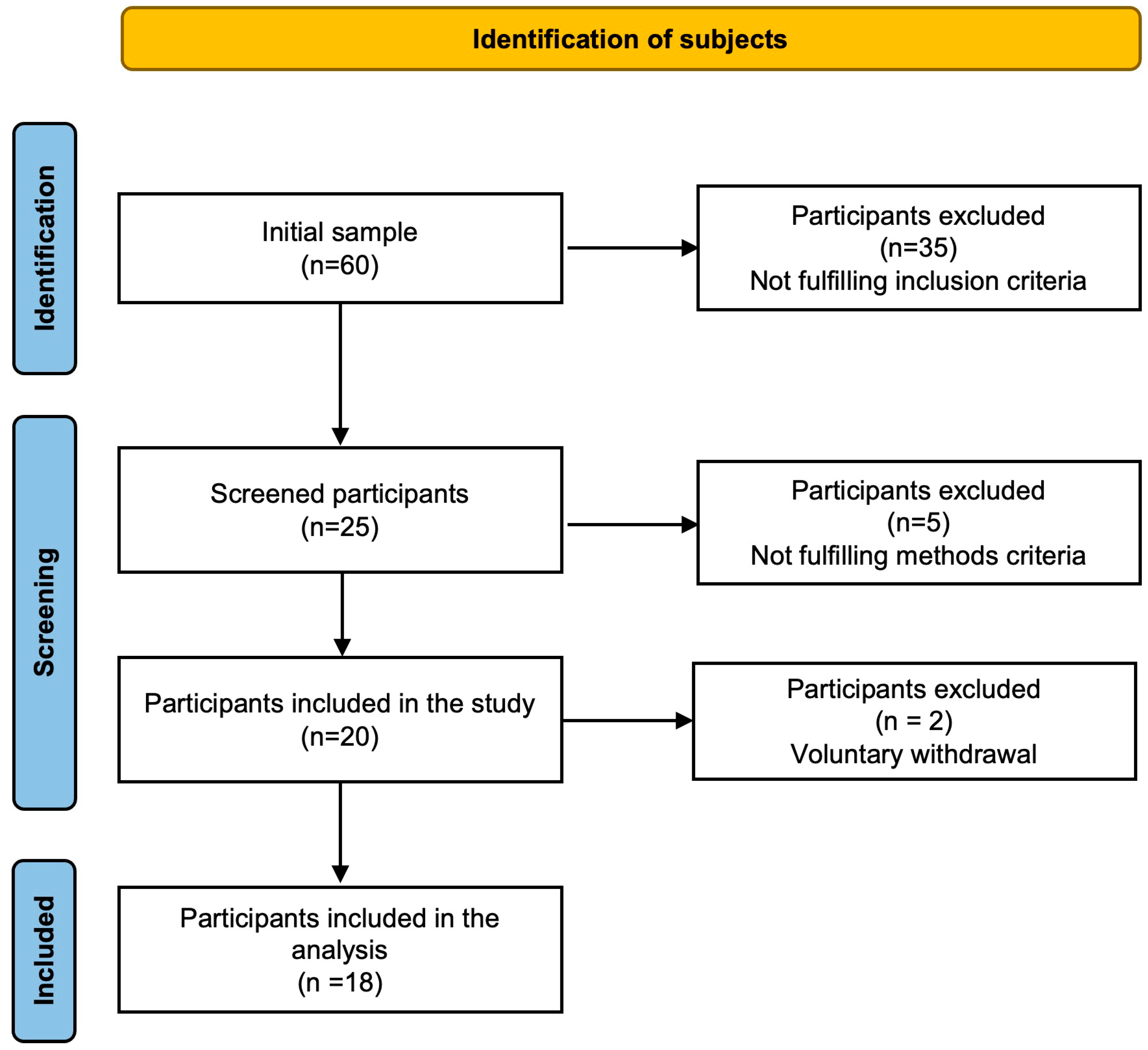
2.1. Participants
2.2. Ethical Considerations
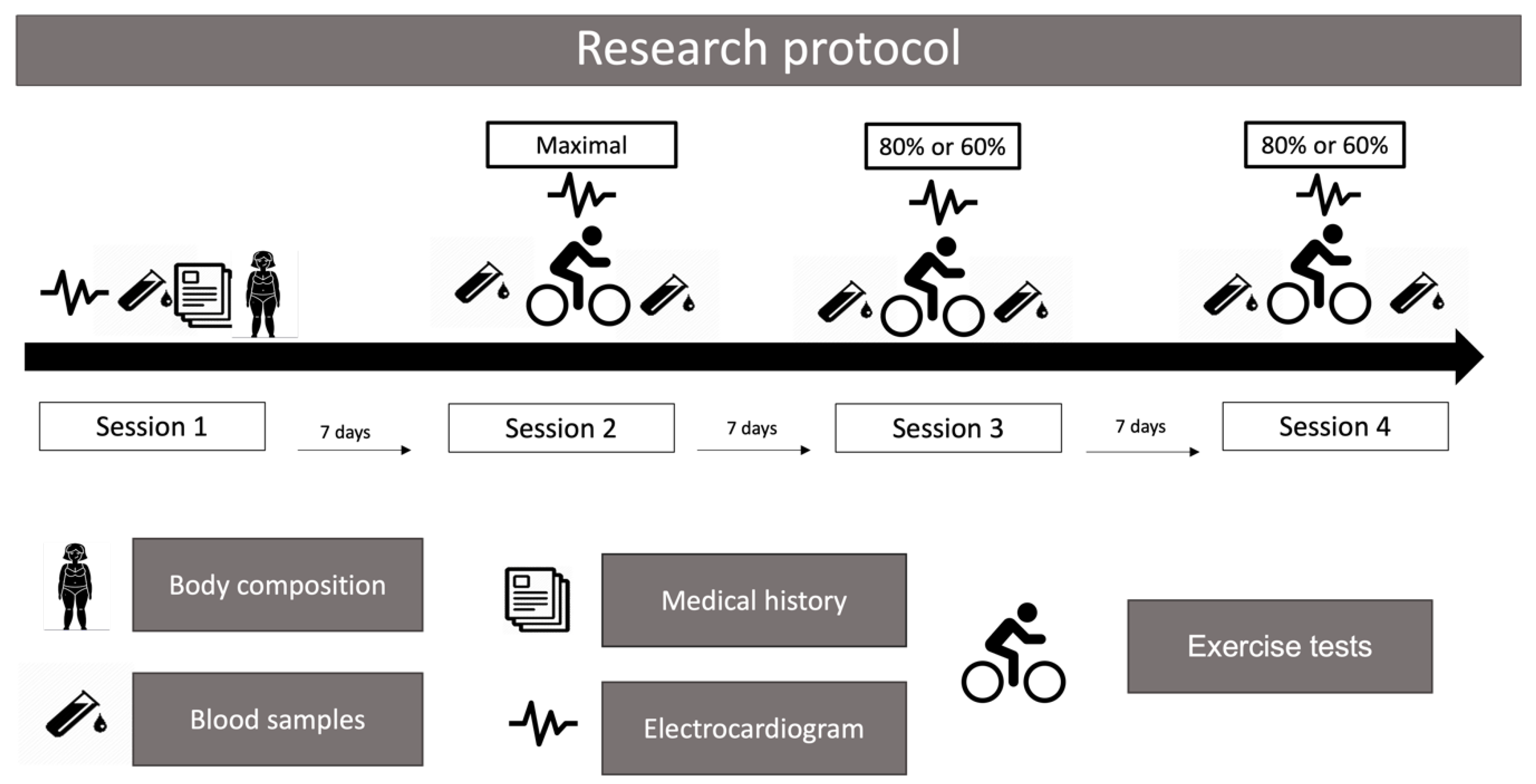
2.3. Research Protocol
2.3.1. First Session
2.3.2. Second Session
2.3.3. Third and Fourth Sessions
2.4. Measurements of Concentrations of Cr and CysC
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
6. Future Research Directions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hill, N.R.; Fatoba, S.T.; Oke, J.L.; Hirst, J.A.; O’Callaghan, C.A.; Lasserson, D.S.; Hobbs, F.D.R. Global Prevalence of Chronic Kidney Disease—A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0158765. [Google Scholar] [CrossRef]
- Amaral, T.L.M.; Amaral, C.d.A.; Vasconcellos, M.T.L.d.; Monteiro, G.T.R. Prevalence and factors associated to chronic kidney disease in older adults. Rev. Saude Publica 2019, 53, 44. [Google Scholar] [CrossRef]
- Villanego, F.; Naranjo, J.; Vigara, L.A.; Cazorla, J.M.; Montero, M.E.; García, T.; Torrado, J.; Mazuecos, A. Impact of physical exercise in patients with chronic kidney disease: Systematic review and meta-analysis. Nefrologia 2020, 40, 237–252. [Google Scholar] [CrossRef]
- Forsse, J.S.; Peterson, M.N.; Papadakis, Z.; Taylor, J.K.; Hess, B.W.; Schwedock, N.; Allison, D.C.; Griggs, J.O.; Wilson, R.L.; Grandjean, P.W. The Effect of Acute Aerobic Exercise on Biomarkers of Renal Health and Filtration in Moderate-CKD. Res. Q. Exerc. Sport 2024, 95, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Spada, T.C.; Silva, J.M.R.D.; Francisco, L.S.; Marçal, L.J.; Antonangelo, L.; Zanetta, D.M.T.; Yu, L.; Burdmann, E.A. High Intensity Resistance Training Causes Muscle Damage and Increases Biomarkers of Acute Kidney Injury in Healthy Individuals. PLoS ONE 2018, 13, e0205791. [Google Scholar] [CrossRef]
- Poortmans, J.R.; Ouchinsky, M. Glomerular Filtration Rate and Albumin Excretion after Maximal Exercise in Aging Sedentary and Active Men. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 1181–1185. [Google Scholar] [CrossRef]
- Bongers, C.C.W.G.; Alsady, M.; Nijenhuis, T.; Tulp, A.D.M.; Eijsvogels, T.M.H.; Deen, P.M.T.; Hopman, M.T.E. Impact of Acute versus Prolonged Exercise and Dehydration on Kidney Function and Injury. Physiol. Rep. 2018, 6, e13734. [Google Scholar] [CrossRef]
- Pryor, R.R.; Pryor, J.L.; Vandermark, L.W.; Adams, E.L.; Brodeur, R.M.; Schlader, Z.J.; Armstrong, L.E.; Lee, E.C.; Maresh, C.M.; Casa, D.J. Acute Kidney Injury Biomarker Responses to Short-Term Heat Acclimation. Int. J. Environ. Res. Public Health 2020, 17, 1325. [Google Scholar] [CrossRef]
- Ariev, A.L.; Kayukov, I.G.; Beresneva, O.N.; Parastaeva, M.M.; Essaian, A.M.; Kucher, A.G. Aging and kidneys: Problems in evaluating of the glomerular filtration rate in elderly. Adv. Gerontol. 2019, 32, 614–626. [Google Scholar]
- Bibbo, G.; Munn, C.; Kirkwood, I. Comparison of Glomerular Filtration Rates Determined Using Two- and Single-Blood Sample Methods with a Three-Blood Sample Technique for 2922 Paediatric Studies. Nucl. Med. Commun. 2019, 40, 1204–1210. [Google Scholar] [CrossRef]
- Gaspari, F.; Perico, N.; Remuzzi, G. Application of Newer Clearance Techniques for the Determination of Glomerular Filtration Rate. Curr. Opin. Nephrol. Hypertens. 1998, 7, 675–680. [Google Scholar] [CrossRef]
- Inoue, Y.; Ohtake, T.; Homma, Y.; Yoshikawa, K.; Nishikawa, J.; Sasaki, Y. Evaluation of Glomerular Filtration Rate by Camera-Based Method in Both Children and Adults. J. Nucl. Med. 1998, 39, 1784–1788. [Google Scholar]
- Agarwal, R. Chromatographic Estimation of Iothalamate and P-Aminohippuric Acid to Measure Glomerular Filtration Rate and Effective Renal Plasma Flow in Humans. J. Chromatogr. B Biomed. Sci. Appl. 1998, 705, 3–9. [Google Scholar] [CrossRef]
- Laterza, O.F.; Price, C.P.; Scott, M.G. Cystatin C: An Improved Estimator of Glomerular Filtration Rate? Clin. Chem. 2002, 48, 699–707. [Google Scholar] [CrossRef]
- Poussel, M.; Touzé, C.; Allado, E.; Frimat, L.; Hily, O.; Thilly, N.; Rousseau, H.; Vauthier, J.-C.; Chenuel, B. Ultramarathon and Renal Function: Does Exercise-Induced Acute Kidney Injury Really Exist in Common Conditions? Front. Sports Act. Living 2019, 1, 71. [Google Scholar] [CrossRef] [PubMed]
- Hellmann, F.; Verdi, M.; Schlemper, B.R.J.; Caponi, S. 50th Anniversary of the Declaration of Helsinki: The Double Standard Was Introduced. Arch. Med. Res. 2014, 45, 600–601. [Google Scholar] [CrossRef]
- Aström, H.; Jonsson, B. Design of Exercise Test, with Special Reference to Heart Patients. Heart 1976, 38, 289–296. [Google Scholar] [CrossRef]
- Miura, K.; Nakagawa, H.; Ohashi, Y.; Harada, A.; Taguri, M.; Kushiro, T.; Takahashi, A.; Nishinaga, M.; Soejima, H.; Ueshima, H. Four Blood Pressure Indexes and the Risk of Stroke and Myocardial Infarction in Japanese Men and Women: A Meta-Analysis of 16 Cohort Studies. Circulation 2009, 119, 1892–1898. [Google Scholar] [CrossRef]
- Mexican Ministry of Health Mexican Official Standard. NORMA Oficial Mexicana NOM-167-SSA1-1997, Para la Prestación de Servicios de Asistencia Social Para Menores y Adultos Mayores. Diario Oficial de la Federación 17/11/1999. Available online: https://www.dof.gob.mx/nota_detalle.php?codigo=4956386&fecha=17/11/1999#gsc.tab=0 (accessed on 9 October 2024).
- Ramos-Jiménez, A.; Wall-Medrano, A.; Hernández-Lepe, M.A.; Chávez-Treviño, G.; Guereca-Arvizuo, J.; Hernández-Torres, R.P. Borg’s category ratio-scale (CR-10) is useful to predict the onset of blood lactate accumulation (OBLA) in young Mexicans adults, regardless their body mass. CIENCIA ergo-sum 2019, 26, 7. [Google Scholar] [CrossRef]
- Gellish, R.L.; Goslin, B.R.; Olson, R.E.; McDonald, A.; Russi, G.D.; Moudgil, V.K. Longitudinal Modeling of the Relationship between Age and Maximal Heart Rate. Med. Sci. Sports Exerc. 2007, 39, 822–829. [Google Scholar] [CrossRef]
- Storer, T.W.; Davis, J.A.; Caiozzo, V.J. Accurate Prediction of VO2max in Cycle Ergometry. Med. Sci. Sports Exerc. 1990, 22, 704–712. [Google Scholar] [CrossRef]
- Bloomer, R.J.; Farney, T.M. Acute Plasma Volume Change with High-Intensity Sprint Exercise. J. Strength Cond. Res. 2013, 27, 2874–2878. [Google Scholar] [CrossRef] [PubMed]
- Van Beaumont, W. Evaluation of Hemoconcentration from Hematocrit Measurements. J. Appl. Physiol. 1972, 32, 712–713. [Google Scholar] [CrossRef] [PubMed]
- Held, L.; Ott, M. On P-Values and Bayes Factors. Annu. Rev. Stat. Its Appl. 2018, 5, 393–419. [Google Scholar] [CrossRef]
- Morris, S.B. Estimating Effect Sizes From Pretest-Posttest-Control Group Designs. Organ. Res. Methods 2008, 11, 364–386. [Google Scholar] [CrossRef]
- Fadel, P.J. Reflex Control of the Circulation during Exercise. Scand. J. Med. Sci. Sports 2015, 25 (Suppl. 4), 74–82. [Google Scholar] [CrossRef]
- Crecelius, A.R.; Kirby, B.S.; Luckasen, G.J.; Larson, D.G.; Dinenno, F.A. Mechanisms of Rapid Vasodilation after a Brief Contraction in Human Skeletal Muscle. Am. J. Physiol. Heart Circ. Physiol. 2013, 305, H29–H40. [Google Scholar] [CrossRef]
- Tschakovsky, M.E.; Rogers, A.M.; Pyke, K.E.; Saunders, N.R.; Glenn, N.; Lee, S.J.; Weissgerber, T.; Dwyer, E.M. Immediate Exercise Hyperemia in Humans Is Contraction Intensity Dependent: Evidence for Rapid Vasodilation. J. Appl. Physiol. (1985) 2004, 96, 639–644. [Google Scholar] [CrossRef]
- Momen, A.; Handly, B.; Kunselman, A.; Leuenberger, U.A.; Sinoway, L.I. Influence of Sex and Active Muscle Mass on Renal Vascular Responses during Static Exercise. Am. J. Physiol. Heart Circ. Physiol. 2006, 291, H121–H126. [Google Scholar] [CrossRef]
- García-Trabanino, R.; Jarquín, E.; Wesseling, C.; Johnson, R.J.; González-Quiroz, M.; Weiss, I.; Glaser, J.; José Vindell, J.; Stockfelt, L.; Roncal, C.; et al. Heat Stress, Dehydration, and Kidney Function in Sugarcane Cutters in El Salvador--A Cross-Shift Study of Workers at Risk of Mesoamerican Nephropathy. Environ. Res. 2015, 142, 746–755. [Google Scholar] [CrossRef]
- Denic, A.; Glassock, R.J.; Rule, A.D. Structural and Functional Changes With the Aging Kidney. Adv. Chronic Kidney Dis. 2016, 23, 19–28. [Google Scholar] [CrossRef]
- Hommos, M.S.; Glassock, R.J.; Rule, A.D. Structural and Functional Changes in Human Kidneys with Healthy Aging. J. Am. Soc. Nephrol. 2017, 28, 2838–2844. [Google Scholar] [CrossRef]
- Levin, A.; Stevens, P.E.; Bilous, R.W.; Coresh, J.; De Francisco, A.L.; De Jong, P.E.; Griffith, K.E.; Hemmelgarn, B.R.; Iseki, K.; Lamb, E.J. Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. Suppl. 2013, 3, 1–150. [Google Scholar] [CrossRef]
- Gu, X.; Fang, X.; Ji, X.; Tang, Z.; Wang, C.; Guan, S.; Wu, X.; Liu, H.; Zhang, Z. Kidney Dysfunction Is Associated with Risk of Cardiovascular Events in Middle-Aged and Elderly Population with Hypertension: A 5-Year Community-Based Cohort Study in China. Clin. Nephrol. 2020, 93, 130–139. [Google Scholar] [CrossRef]
- Verbeeck, R.K.; Musuamba, F.T. Pharmacokinetics and Dosage Adjustment in Patients with Renal Dysfunction. Eur. J. Clin. Pharmacol. 2009, 65, 757–773. [Google Scholar] [CrossRef]
- Abdulkader, R.C.R.M.; Burdmann, E.A.; Lebrão, M.L.; Duarte, Y.A.O.; Zanetta, D.M.T. Aging and Decreased Glomerular Filtration Rate: An Elderly Population-Based Study. PLoS ONE 2017, 12, e0189935. [Google Scholar] [CrossRef]
- Mohan, S.G.; Holmgren, N.J.; Jacobson, L.E.; Saxe, J.M.; West-Sell, S.A.; Williams, J.; Harper, P.; Jensen, C.D. Climate Factors May Influence Glomerular Filtration Rate in Nephrology Patients. FASEB J. 2022, 36. [Google Scholar] [CrossRef]
- Koulouridis, E.; Georgalidis, K.; Kostimpa, I.; Koulouridis, I.; Krokida, A.; Houliara, D. Metabolic Syndrome Risk Factors and Estimated Glomerular Filtration Rate among Children and Adolescents. Pediatr. Nephrol. 2010, 25, 491–498. [Google Scholar] [CrossRef]
- Wang, Y.; Qiu, X.; Lv, L.; Wang, C.; Ye, Z.; Li, S.; Liu, Q.; Lou, T.; Liu, X. Correlation between Serum Lipid Levels and Measured Glomerular Filtration Rate in Chinese Patients with Chronic Kidney Disease. PLoS ONE 2016, 11, e0163767. [Google Scholar] [CrossRef]
- Inker, L.A.; Schmid, C.H.; Tighiouart, H.; Eckfeldt, J.H.; Feldman, H.I.; Greene, T.; Kusek, J.W.; Manzi, J.; Van Lente, F.; Zhang, Y.L.; et al. Estimating Glomerular Filtration Rate from Serum Creatinine and Cystatin C. N. Engl. J. Med. 2012, 367, 20–29. [Google Scholar] [CrossRef]
- Ferguson, T.W.; Komenda, P.; Tangri, N. Cystatin C as a Biomarker for Estimating Glomerular Filtration Rate. Curr. Opin. Nephrol. Hypertens. 2015, 24, 295–300. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Age (years) | 70.1 ± 5.1 |
| Weight (kg) | 71.0 ± 10.9 |
| Height (cm) | 163.3 ± 7.6 |
| BMI (kg·m−2) | 26.8 ± 3.3 |
| Fat mass (%) | 24.1 ± 5.5 |
| Systolic blood pressure (mmHg) | 124.7 ± 13.1 |
| Diastolic blood pressure (mmHg) | 78.9 ± 10.2 |
| Mean blood pressure (mmHg) | 94.2 ± 10.3 |
| Glucose (mg·dL−1) | 103 ± 13 |
| Cholesterol (mg·dL−1) | 185 ± 34 |
| Triacylglycerols (mg·dL−1) | 127 ± 41 |
| Creatinine (mg·dL−1) | 0.937 ± 0.246 |
| Cystatin C (mg·dL−1) | 0.753 ± 0.161 |
| eGFR by Cr (mL·min·1.73 m2) | 76.5 ± 16.7 |
| eGFR by CysC (mL·min·1.73 m2) | 99.3 ± 15.4 |
| VO2 max (ml·kg−1·min−1) | 28.6 ± 7.1 |
| HRmax (beats·min−1) | 148 ± 13 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trejo-Trejo, M.; Gómez-Miranda, L.M.; Ramos-Jiménez, A. Acute Effect of Three Aerobic Exercise Intensities on Glomerular Filtration Rate in Healthy Older Adults. Diseases 2024, 12, 249. https://doi.org/10.3390/diseases12100249
Trejo-Trejo M, Gómez-Miranda LM, Ramos-Jiménez A. Acute Effect of Three Aerobic Exercise Intensities on Glomerular Filtration Rate in Healthy Older Adults. Diseases. 2024; 12(10):249. https://doi.org/10.3390/diseases12100249
Chicago/Turabian StyleTrejo-Trejo, Marina, Luis M. Gómez-Miranda, and Arnulfo Ramos-Jiménez. 2024. "Acute Effect of Three Aerobic Exercise Intensities on Glomerular Filtration Rate in Healthy Older Adults" Diseases 12, no. 10: 249. https://doi.org/10.3390/diseases12100249
APA StyleTrejo-Trejo, M., Gómez-Miranda, L. M., & Ramos-Jiménez, A. (2024). Acute Effect of Three Aerobic Exercise Intensities on Glomerular Filtration Rate in Healthy Older Adults. Diseases, 12(10), 249. https://doi.org/10.3390/diseases12100249