

A Real-World Longitudinal Study in Non-Functioning Pituitary Incidentalomas: A PRECES Micro-Adenomas Sub-Analysis


 ,
, 

 and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
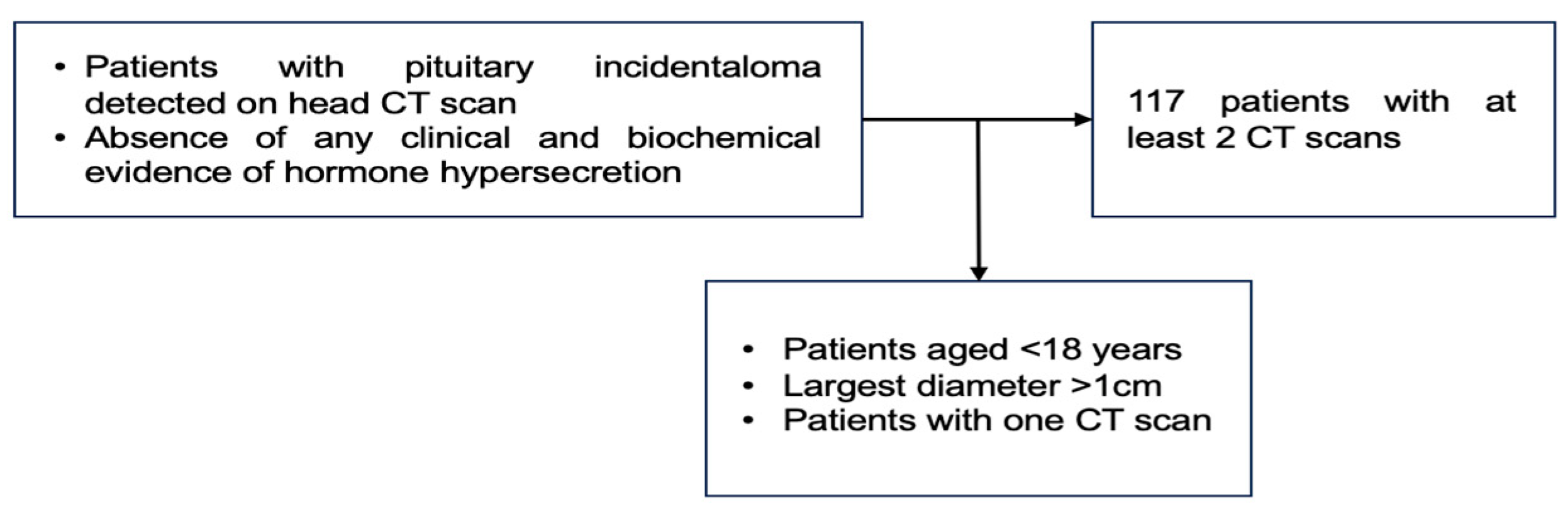
2.2. Studied Population
2.3. Study Protocol
2.3.1. Imaging Scans
2.3.2. Hormonal Assays
2.4. Statistical Analysis
2.5. Ethical Aspects
3. Results
3.1. Cross-Sectional (Baseline) Analysis
3.2. Analysis Based on the Patients’ Age Groups
3.3. Longitudinal Analysis
3.3.1. Analysis between the Baseline (First) CT Scan and the Second (2nd) CT Scan
3.3.2. Analysis between the Increase Group versus the Non-Increase Group
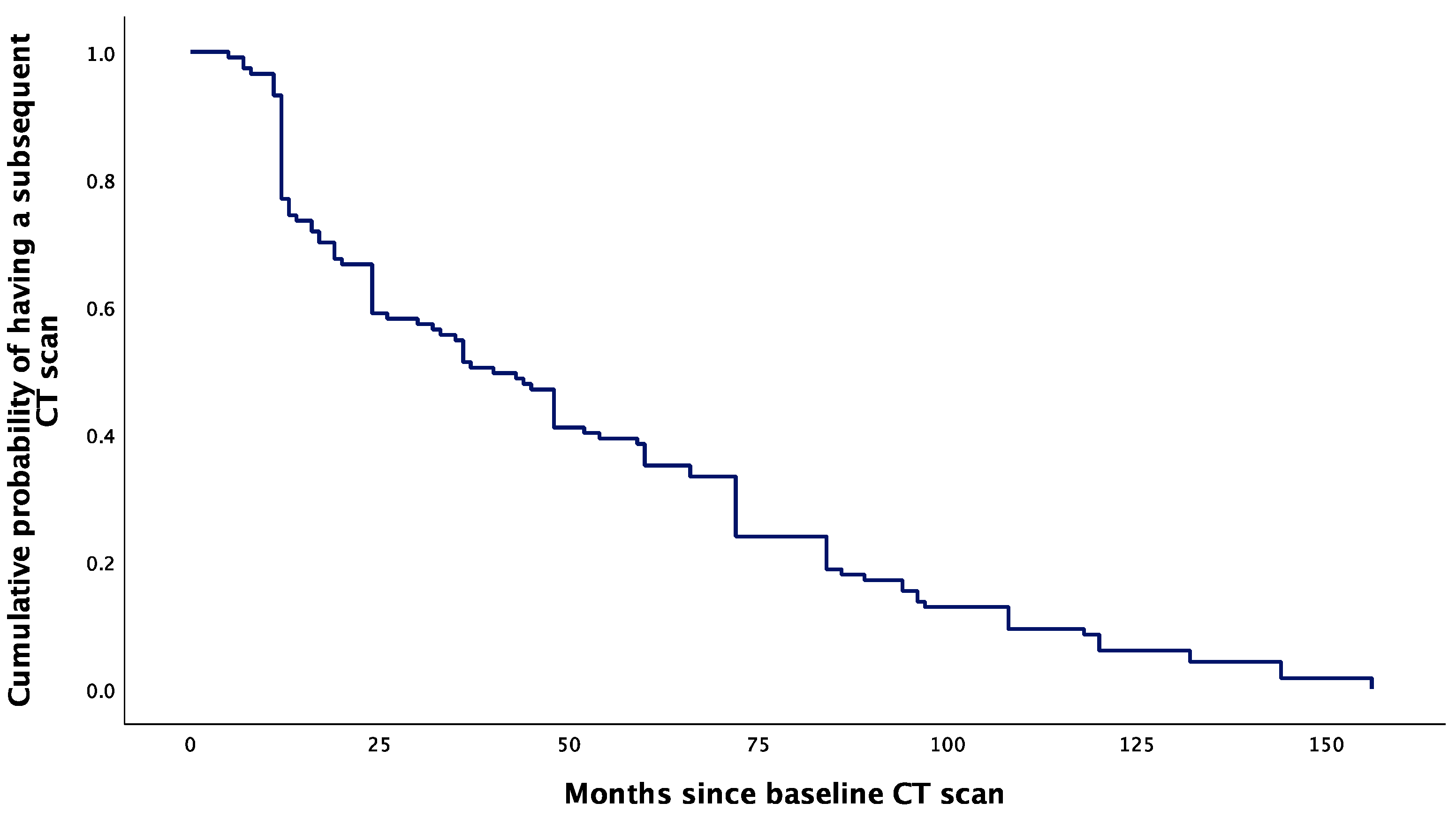
3.3.3. Analysis of Time Window between Assessments
3.3.4. Arbitrary Cut-Off and Receiver Operating Characteristic (ROC) Curve to Predict PI Increase
4. Discussion
5. Conclusions
- This was a longitudinal study in 117 adults (aged between 20 and 70 years) diagnosed with non-functioning micro-PIs followed for a mean period of 50.93 months.
- No PI became functioning during follow-up, nor associated hypopituitarism or increased beyond the diameter of 1 cm; no case of pituitary apoplexy was found.
- The analysis based on patients’ decades of age showed that most of them were between the ages of 31 and 60 with similar diameters.
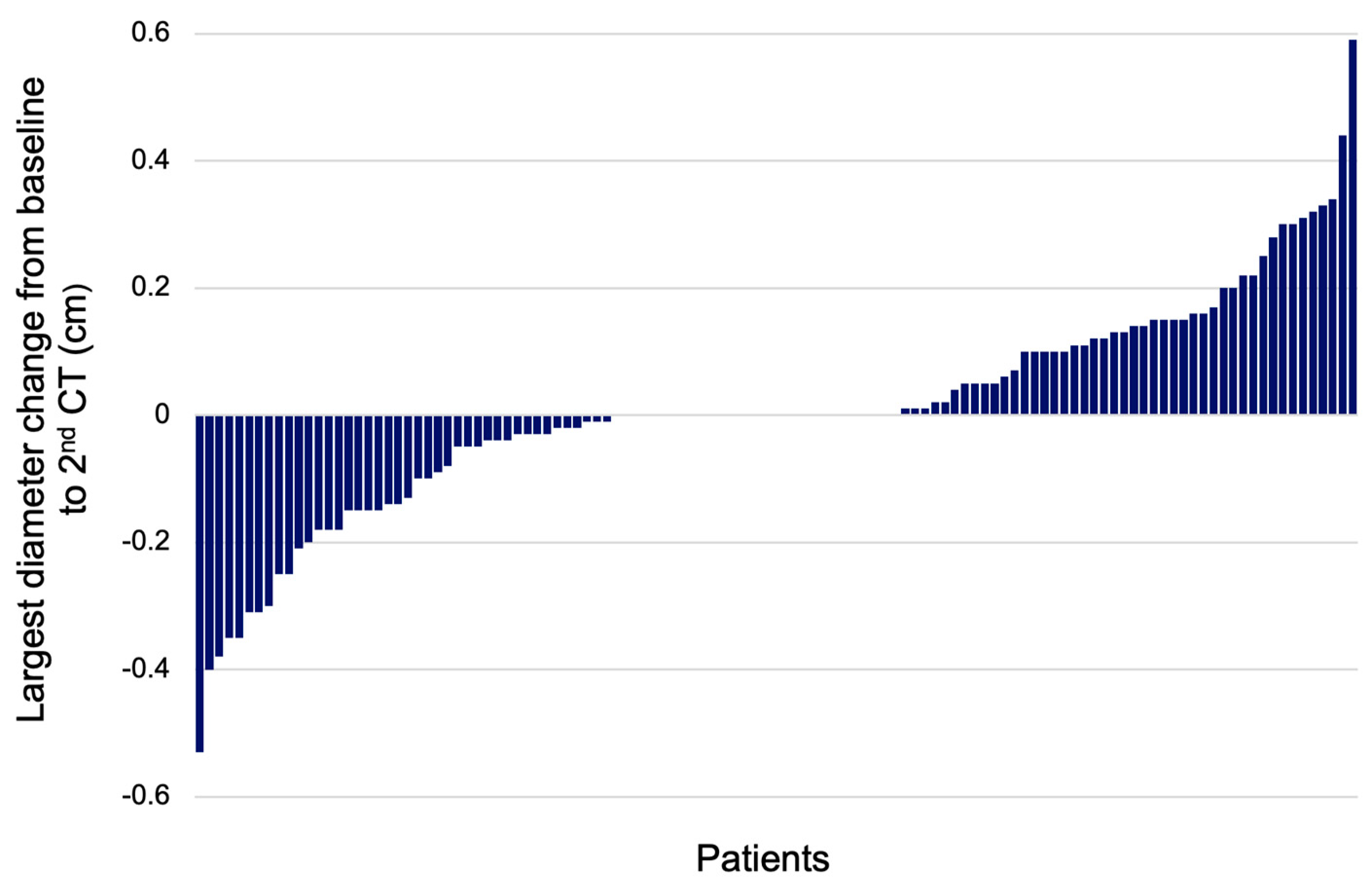
- A total of 46/117 (39.32%) patients had a larger diameter during follow-up (increase group) versus the non-increase group (N = 71, 60.68%) that included the subjects with stationary or decreased diameters.
- The increase group had lower initial transverse, longitudinal, and largest diameter versus the non-increase group: 0.45 ± 0.12 versus 0.57 ± 0.17 (p < 0.0001), 0.36 ± 0.11 versus 0.43 ± 0.13 (p = 0.004), and 0.46 ± 0.12 versus 0.6 ± 0.16 (p < 0.0001).
- The increase group versus the non-increase group had a larger period of surveillance: a median of 48 (24, 84) versus 32.5 (12, 72) months (p = 0.045) and presented a similar age, pituitary hormone profile, and tumour lateralisation profile at baseline.
- We found a median diameter change of +0.14 cm versus −0.03 cm in the increase versus the non-increase groups (p < 0.0001).
- A rather high percent of patients might experience PI diameter increase during a longer period of follow-up, including those with a smaller initial size, while the age at diagnosis does not predict the tumour growth. This might help practitioners for long-standing surveillance according to our mentioned duration of follow-up.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACTH | adrenocorticotropic hormone |
| CT | computed tomography |
| FSH | follicle-stimulating hormone |
| GH | growth hormone |
| IGF1 | insulin-like growth factor 1 |
| LH | luteinising hormone |
| PI | pituitary incidentalomas |
| PitNET | pituitary neuroendocrine tumour |
| ROC | receiver operating characteristic |
| Q | quartiles |
| SD | standard deviation |
| TSH | thyroid stimulating hormone |
| WHO | World Health Organization |
References
- Hamblin, R.; Fountas, A.; Lithgow, K.; Loughrey, P.B.; Bonanos, E.; Shinwari, S.K.; Mitchell, K.; Shah, S.; Grixti, L.; Matheou, M.; et al. Natural history of non-functioning pituitary microadenomas: Results from the UK non-functioning pituitary adenoma consortium. Eur. J. Endocrinol. 2023, 189, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Anghel, A.; Stanciu, S.; Ciobica, M.L.; Stoicescu, D.; Muresan, M.M. Contrast-enhanced ultrasound-clinical applications. Rom. J. Mil. Med. 2011, 114, 25–30. [Google Scholar]
- Stanciu, S.; Enciu, C.; Raduta, I.; Stoicescu, D.; Anghel, A.; Anghel, D.; Olan, B.; Ciobica, L. The role of contrast-enhanced ultrasound in risk assessment of carotid atheroma. Rom. J. Mil. Med. 2016, 119, 9–11. [Google Scholar] [CrossRef]
- Nistor, C.; Ciuche, A.I. Emergency surgical tracheal decompression in a huge retrosternal goiter. Acta Endocrinol. 2017, 13, 370–374. [Google Scholar] [CrossRef]
- Costanzo, R.; Scalia, G.; Strigari, L.; Ippolito, M.; Paolini, F.; Brunasso, L.; Sciortino, A.; Iacopino, D.G.; Maugeri, R.; Ferini, G.; et al. Nuclear medicine imaging modalities to detect incidentalomas and their impact on patient management: A systematic review. J. Cancer Res. Clin. Oncol. 2024, 150, 368. [Google Scholar] [CrossRef]
- Unger, N.; Theodoropoulou, M.; Schilbach, K. Clinically active pituitary tumors. Inn. Med. 2024, 65, 672–680. [Google Scholar] [CrossRef]
- Nistor, C.E.; Găvan, C.S.; Ciritel, A.A.; Nemes, A.F.; Ciuche, A. The Association of Minimally Invasive Surgical Approaches and Mortality in Patients with Malignant Pleuropericarditis-A 10 Year Retrospective Observational Study. Medicina 2022, 58, 718. [Google Scholar] [CrossRef]
- Carsote, M.; Valea, A.; Dumitru, N.; Terzea, D.; Petrova, E.; Albu, S.; Buruiana, A.; Ghemigian, A. Metastases in daily endocrine practice. Arch. Balk. Med. Union 2016, 51, 476–480. [Google Scholar]
- Nistor, C.E.; Ciuche, A.; Cucu, A.P.; Serban, B.; Cursaru, A.; Cretu, B.; Cirstoiu, C. Clavicular Malignancies: A Borderline Surgical Management. Medicina 2022, 58, 910. [Google Scholar] [CrossRef]
- Kolbeinsson, H.M.; Dandamudi, S.; Gira, J.; Krech, L.; Pounders, S.; Fisk, C.; Wright, G.P.; Chapman, A.J.; Chadwick, C. Expecting the unexpected: Incidental findings at a level 1 trauma center. Emerg. Radiol. 2023, 30, 343–349. [Google Scholar] [CrossRef]
- Ameti, A.; Chouchane, K.; Fontana, E.; Papadakis, G.E. Endocrinology: What’s new in 2023. Rev. Medicale Suisse 2024, 20, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Giraldi, E.; Allen, J.W.; Ioachimescu, A.G. Pituitary Incidentalomas: Best Practices and Looking Ahead. Endocr. Pract. 2023, 29, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Tahara, S.; Hattori, Y.; Suzuki, K.; Ishisaka, E.; Teramoto, S.; Morita, A. An Overview of Pituitary Incidentalomas: Diagnosis, Clinical Features, and Management. Cancers 2022, 14, 4324. [Google Scholar] [CrossRef]
- Langlois, F.; Fleseriu, M. What to Do with Incidentally Discovered Pituitary Abnormalities? Med. Clin. N. Am. 2021, 105, 1081–1098. [Google Scholar] [CrossRef]
- Ono, M.; Fukuda, I.; Soga, A.; Tahara, S.; Morita, A.; Sugihara, H. A survey of surgically resected pituitary incidentalomas and a comparison of the clinical features and surgical outcomes of non-functioning pituitary adenomas discovered incidentally versus symptomatically. Endocr. J. 2021, 68, 561–571. [Google Scholar] [CrossRef]
- Kageyama, K.; Nishiyama, M. Pituitary Tumors: Molecular Insights, Diagnosis, and Targeted Therapy. Cancers 2023, 15, 5526. [Google Scholar] [CrossRef]
- Constantinescu, S.M.; Maiter, D. Pituitary incidentaloma. Presse Med. 2021, 50, 104081. [Google Scholar] [CrossRef]
- Vasilev, V.; Rostomyan, L.; Daly, A.F.; Potorac, I.; Zacharieva, S.; Bonneville, J.F.; Beckers, A. Management of endocrine disease: Pituitary ‘incidentaloma’: Neuroradiological assessment and differential diagnosis. Eur. J. Endocrinol. 2016, 175, R171–R184. [Google Scholar] [CrossRef] [PubMed]
- Sanno, N.; Oyama, K.; Tahara, S.; Teramoto, A.; Kato, Y. A survey of pituitary incidentaloma in Japan. Eur. J. Endocrinol. 2003, 149, 123–127. [Google Scholar] [CrossRef]
- Wang, M.T.M.; Meyer, J.A.; Danesh-Meyer, H.V. Neuro-ophthalmic evaluation and management of pituitary disease. Eye 2024, 38, 2279–2288. [Google Scholar] [CrossRef]
- Donovan, L.E.; Corenblum, B. The natural history of the pituitary incidentaloma. Arch. Intern. Med. 1995, 155, 181–183. [Google Scholar] [CrossRef] [PubMed]
- Westall, S.J.; Aung, E.T.; Kejem, H.; Daousi, C.; Thondam, S.K. Management of pituitary incidentalomas. Clin. Med 2023, 23, 129–134. [Google Scholar] [CrossRef]
- Hamblin, R.; Fountas, A.; Levy, M.; Karavitaki, N. UK practice on incidentally detected non-functioning pituitary microadenomas: Analysis of two national surveys during a 12-year interval. Pituitary 2023, 26, 94–104. [Google Scholar] [CrossRef] [PubMed]
- Sanno, N.; Oyama, K.; Tahara, S.; Teramoto, A. Clinical aspects of pituitary incidentalomas. Nihon Rinsho 2004, 62, 946–950. [Google Scholar]
- Oyama, K.; Sanno, N.; Tahara, S.; Teramoto, A. Management of pituitary incidentalomas: According to a survey of pituitary incidentalomas in Japan. In Seminars in Ultrasound, CT and MRI; WB Saunders: Philadelphia, PA, USA, 2005; Volume 26, pp. 47–50. [Google Scholar] [CrossRef]
- Donckier, J.E.; Gustin, T. Pituitary incidentaloma: To operate or not to operate? Acta Chir. Belg. 2012, 112, 255–260. [Google Scholar] [CrossRef]
- Jung, H.; Yang, S.Y.; Cho, K.T. Suggestion of Follow-Up Period in Nonfunctioning Pituitary Incidentaloma Based on MRI Characteristics. Brain Tumor Res. Treat. 2024, 12, 40–49. [Google Scholar] [CrossRef]
- Baldo, F.; Marin, M.; Murru, F.M.; Barbi, E.; Tornese, G. Dealing With Brain MRI Findings in Pediatric Patients With Endocrinological Conditions: Less Is More? Front. Endocrinol. 2022, 12, 780763. [Google Scholar] [CrossRef]
- Morinaga, Y.; Abe, I.; Nii, K.; Hanada, H.; Takemura, Y.; Takashi, Y.; Sakamoto, K.; Inoue, R.; Mitsutake, T.; Kobayashi, K.; et al. Characteristics and clinical outcomes in pituitary incidentalomas and non-incidental pituitary tumors treated with endoscopic transsphenoidal surgery. Medicine 2020, 99, e22713. [Google Scholar] [CrossRef]
- Souteiro, P.; Maia, R.; Santos-Silva, R.; Figueiredo, R.; Costa, C.; Belo, S.; Castro-Correia, C.; Carvalho, D.; Fontoura, M. Pituitary incidentalomas in paediatric age are different from those described in adulthood. Pituitary 2019, 22, 124–128. [Google Scholar] [CrossRef]
- Tsukamoto, T.; Miki, Y. Imaging of pituitary tumors: An update with the 5th WHO Classifications-part 2. Neoplasms other than PitNET and tumor-mimicking lesions. Jpn. J. Radiol. 2023, 41, 808–829. [Google Scholar] [CrossRef] [PubMed]
- Zenoaga-Barbăroșie, C.; Berca, L.; Vassu-Dimov, T.; Toma, M.; Nica, M.I.; Alexiu-Toma, O.A.; Ciornei, C.; Albu, A.; Nica, S.; Nistor, C.; et al. The Predisposition for Type 2 Diabetes Mellitus and Metabolic Syndrome. Balk. J. Med. Genet. 2023, 26, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Gontarz-Nowak, K.; Szklarz, M.; Szychlińska, M.; Matuszewski, W.; Bandurska-Stankiewicz, E. A Brief Look at Hashimoto’s Disease, Adrenal Incidentalomas, Obesity and Insulin Resistance-Could Endocrine Disruptors Be the Other Side of the Same Coin? Medicina 2023, 59, 1234. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| Age (years) mean ± SD | 43.86 ± 11.99 |
| Sex | |
| Female, number of patients (%) | 110 (94.02%) |
| Male, number of patients (%) | 7 (5.98%) |
| Baseline CT scan diameters | |
| Transverse diameter (cm), mean ± SD | 0.53 ± 0.16 |
| Longitudinal diameter (cm), mean ± SD | 0.41 ± 0.13 |
| Largest diameter (cm), mean ± SD | 0.55 ± 0.16 |
| Tumour location | |
| Left side, number of patients (%) | 38 (32.48%) |
| Right side, number of patients (%) | 55 (47.01%) |
| Median part, number of patients (%) | 24 (20.51%) |
| Endocrine panel | |
| FSH (mIU/mL), median (Q1, Q3) | 33.40 (4.99, 67.24) |
| LH (mIU/mL), median (Q1, Q3) | 5.66 (3.05, 44.18) |
| ACTH (pg/mL), mean ± SD | 20.57 ± 13.09 |
| Morning plasma cortisol (µg/dL), mean ± SD | 12.79 ± 3.87 |
| GH baseline (ng/mL), median (Q1, Q3) | 0.30 (0.10, 0.76) |
| IGF1 baseline (ng/mL), mean ± SD | 167.28 ± 42.31 |
| Prolactin (ng/mL), mean ± SD | 8.24 ± 4.46 |
| TSH (µIU/mL), median (Q1, Q3) | 1.40 (0.97, 2.34) |
| Age Group (Years) | N (% from the Entire Group) | Transverse Diameter Median (Q1, Q3) | Longitudinal Diameter Median (Q1, Q3) | Largest Diameter Median (Q1, Q3) | Left Side N (% from the Age Group) | Right Side N (% from the Age Group) | Median Part N (% from the Age Group) |
|---|---|---|---|---|---|---|---|
| 21–30 | 9 (16.23) | 0.45 (0.40, 0.59) | 0.36 (0.31, 0.45) | 0.45 (0.40, 0.59) | 5 (26.32) | 11 (57.89) | 3 (15.79) |
| 31–40 | 27 (23.07) | 0.50 (0.40, 0.55) | 0.40 (0.35, 0.50) | 0.54 (0.45, 0.60) | 13 (48.15) | 7 (25.93) | 7 (25.93) |
| 41–50 | 30 (25.64) | 0.51 (0.45, 0.73) | 0.39 (0.32, 0.41) | 0.51 (0.45, 0.73) | 8 (26.67) | 19 (63.33) | 3 (10.00) |
| 51–60 | 33 (28.20) | 0.49 (0.49, 0.55) | 0.35 (0.30, 0.48) | 0.50 (0.44, 0.56) | 7 (21.21) | 16 (48.48) | 10 (30.30) |
| 61–70 | 8 (6.83) | 0.54 (0.44, 0.79) | 0.44 (0.35, 0.50) | 0.54 (0.44, 0.79) | 5 (62.50) | 2 (25.00) | 1 (12.50) |
| Variable | Baseline CT Scan | 2nd CT Scan | p-Value |
|---|---|---|---|
| Increase group (N = 46, 39.32%) | |||
| Transverse diameter (cm), mean ± SD | 0.45 ± 0.12 | 0.61 ± 0.16 | 0.000 |
| Transverse diameter (cm), median (Q1, Q3) | 0.45(0.40, 0.50) | 0.60(0.52, 0.70) | |
| Longitudinal diameter (cm), mean ± SD | 0.36 ± 0.11 | 0.42 ± 0.13 | 0.003 |
| Longitudinal diameter (cm), median (Q1, Q3) | 0.35(0.30, 0.40) | 0.40(0.30, 0.53) | |
| Largest diameter (cm), mean ± SD | 0.46 ± 0.12 | 0.62 ± 0.15 | 0.000 |
| Largest diameter (cm), median (Q1, Q3) | 0.45 (0.40, 0.50) | 0.60 (0.53, 0.70) | |
| Non-increase group (N = 71, 60.68%) | |||
| Transverse diameter (cm), mean ± SD | 0.57 ± 0.16 | 0.49 ± 0.14 | 0.000 |
| Transverse diameter (cm), median (Q1, Q3) | 0.55 (0.45, 0.70) | 0.49(0.40, 0.55) | |
| Longitudinal diameter (cm), mean ± SD | 0.43 ± 0.13 | 0.39 ± 0.10 | 0.001 |
| Longitudinal diameter (cm), median (Q1, Q3) | 0.40 (0.33,0.50) | 0.38(0.30, 0.45) | |
| Largest diameter (cm), mean ± SD | 0.60 ± 0.16 | 0.51 ± 0.14 | 0.000 |
| Largest diameter (cm), median (Q1, Q3) | 0.56 (0.49, 0.75) | 0.49 (0.40, 0.55) | |
| Entire group (N = 117, 100%) | |||
| Transverse diameter (cm), mean ± SD | 0.52 ± 0.01 | 0.54 ± 0.01 | 0.253 |
| Transverse diameter (cm), median (Q1, Q3) | 0.50 (0.42, 0.60) | 0.53 (0.42, 0.63) | |
| Longitudinal diameter (cm), mean ± SD | 0.40 ± 0.01 | 0.40 ± 0.01 | 0.727 |
| Longitudinal diameter (cm), median (Q1, Q3) | 0.38 (0.32, 0.46) | 0.39 (0.30, 0.47) | |
| Largest diameter (cm), mean ± SD | 0.54 ± 0.14 | 0.55 ± 0.01 | 0.453 |
| Largest diameter (cm), median (Q1, Q3) | 0.50 (0.44, 0.60) | 0.54 (0.45, 0.66) | |
| Variable | Increase Group | Non-Increase Group | p-Value |
|---|---|---|---|
| Number (%) | 46 (39.32%) | 71 (60.68%) | |
| Age (years), mean ± SD | 43.57 ± 12.22 | 44.06 ± 11.92 | 0.83 |
| Baseline CT scan diameters | |||
| Transverse diameter (cm), mean ± SD | 0.45 ± 0.12 | 0.57 ± 0.17 | 0.000 |
| Transverse diameter (cm), median (Q1, Q3) | 0.45 (0.40, 0.50) | 0.55 (0.45, 0.70) | |
| Longitudinal diameter (cm), mean ± SD | 0.36 ± 0.11 | 0.43 ± 0.13 | 0.004 |
| Longitudinal diameter (cm), median (Q1, Q3) | 0.35 (0.30, 0.41) | 0.40 (0.33, 0.50) | |
| Largest diameter (cm), mean ± SD | 0.46 ± 0.12 | 0.60 ± 0.16 | 0 |
| Largest diameter (cm), median (Q1, Q3) | 0.45 (0.40, 0.50) | 0.56 (0.49, 0.75 | |
| 2nd CT scan diameters | |||
| Transverse diameter (cm), mean ± SD | 0.61 ± 0.16 | 0.50 ± 0.14 | 0 |
| Transverse diameter (cm), median (Q1, Q3) | 0.60 (0.52, 0.70) | 0.49 (0.40, 0.55) | |
| Longitudinal diameter (cm), mean ± SD | 0.42 ± 0.13 | 0.39 ± 0.10 | 0 |
| Longitudinal diameter (cm), median (Q1, Q3) | 0.40 (0.30, 0.53) | 0.38 (0.30, 0.45) | |
| Largest diameter (cm), mean ± SD | 0.62 ± 0.15 | 0.51 ± 0.14 | 0 |
| Largest diameter (cm), median (Q1, Q3) | 0.60 (0.55, 0.70) | 0.49 (0.41, 0.55) | |
| Largest diameter change between baseline 2nd CT scan | |||
| Largest diameter change (cm), mean ± SD | 0.17 ± 0.13 | −0.09 ± 0.12 | 0 |
| Largest diameter change (cm), median (Q1, Q3) | 0.14 (0.07, 0.22) | −0.03 (−0.15, 0.00) | |
| Tumour location | |||
| Left side, number (%) | 19 (41.30%) | 19 (26.76%) | 0.088 |
| Right side, number (%) | 16 (34.78%) | 39 (54.93%) | |
| Median part, number (%) | 11 (23.91%) | 13 (18.31%) | |
| Endocrine panel | |||
| FSH (mIU/mL), median (Q1, Q3) | 36.38 (6.99, 64.91) | 23.75 (4.69, 79.41) | 0.846 |
| LH (mIU/mL), median (Q1, Q3) | 13.48 (3.06, 52.48) | 5.66 (2.02, 35.14) | 0.418 |
| ACTH (pg/mL), median (Q1, Q3) | 16.98 (12.00, 25.64) | 19.77 (12.04, 32.95) | 0.537 |
| Morning plasma cortisol (µg/dL), mean ± SD | 11.64 ± 3.39 | 13.73 ± 4.08 | 0.138 |
| GH baseline (ng/mL), mean (Q1, Q3) | 0.51 (0.11, 0.90) | 0.24 (0.06, 0.60) | 0.261 |
| IGF1 baseline (ng/mL), mean ± SD | 149.75 (133.35, 205.80) | 169.80 (147.15, 191.05) | 0.862 |
| Prolactin (ng/mL), mean ± SD | 8.19 ± 4.59 | 8.30 ± 4.42 | 0.93 |
| TSH (µIU/mL), median (Q1, Q3) | 1.21 (0.90, 1.74) | 1.94 (1.11, 3.17) | 0.28 |
| Surveillance duration | |||
| Months between baseline 2nd CT, median (Q1, Q3) | 48.00 (24.00, 84.00) | 32.50 (12.00, 72.00) | 0.045 |
| Age Group | Months of Follow-Up | |
|---|---|---|
| Mean ± SD | Median (Q1, Q3) | |
| 21–30 years | 55.26 ± 10.11 | 43.00 (17.00, 89.00) |
| 31–40 years | 52.33 ± 8.12 | 36.00 (16.00, 84.00) |
| 41–50 years | 45.63 ± 6.85 | 36.00 (12.00, 67.50) |
| 51–60 years | 51.06 ± 7.02 | 48.00 (12.50, 78.00) |
| 61–70 years | 55.25 ± 13.23 | 60.00 (15.00, 81.00) |
| Entire group | 50.93 ± 39.97 | 40.00 (13.50, 72.00) |
| Increase group | 58.11 ± 39.19 | 48.00 (24.00, 84.00) |
| Non-increase group | 46.28 ± 40.05 | 32.50 12.00, 72.00) |
| Cut-Off Value | Sensitivity | Specificity | Youden Index |
|---|---|---|---|
| 0.50 cm | 65.21% | 74.64% | 0.398 |
| 0.545 cm | 87.00% | 59.20% | 0.462 |
| Cut-Off Value | Sensitivity | Specificity | Youden Index |
|---|---|---|---|
| 0.50 cm | 65.21% | 74.64% | 0.398 |
| 0.545 cm | 87.00% | 59.20% | 0.462 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costachescu, M.; Nistor, C.; Valea, A.; Sima, O.-C.; Ciuche, A.; Stanciu, M.; Carsote, M.; Ciobica, M.-L. A Real-World Longitudinal Study in Non-Functioning Pituitary Incidentalomas: A PRECES Micro-Adenomas Sub-Analysis. Diseases 2024, 12, 240. https://doi.org/10.3390/diseases12100240
Costachescu M, Nistor C, Valea A, Sima O-C, Ciuche A, Stanciu M, Carsote M, Ciobica M-L. A Real-World Longitudinal Study in Non-Functioning Pituitary Incidentalomas: A PRECES Micro-Adenomas Sub-Analysis. Diseases. 2024; 12(10):240. https://doi.org/10.3390/diseases12100240
Chicago/Turabian StyleCostachescu, Mihai, Claudiu Nistor, Ana Valea, Oana-Claudia Sima, Adrian Ciuche, Mihaela Stanciu, Mara Carsote, and Mihai-Lucian Ciobica. 2024. "A Real-World Longitudinal Study in Non-Functioning Pituitary Incidentalomas: A PRECES Micro-Adenomas Sub-Analysis" Diseases 12, no. 10: 240. https://doi.org/10.3390/diseases12100240
APA StyleCostachescu, M., Nistor, C., Valea, A., Sima, O.-C., Ciuche, A., Stanciu, M., Carsote, M., & Ciobica, M.-L. (2024). A Real-World Longitudinal Study in Non-Functioning Pituitary Incidentalomas: A PRECES Micro-Adenomas Sub-Analysis. Diseases, 12(10), 240. https://doi.org/10.3390/diseases12100240