
Cytokine Storms and Anaphylaxis Following COVID-19 mRNA-LNP Vaccination: Mechanisms and Therapeutic Approaches


{kind=link}
{kind=link}
Abstract
1. Introduction
2. Mechanism, Treatment, and Prevention of Cytokine Release Following COVID-19 mRNA-LNP Vaccination
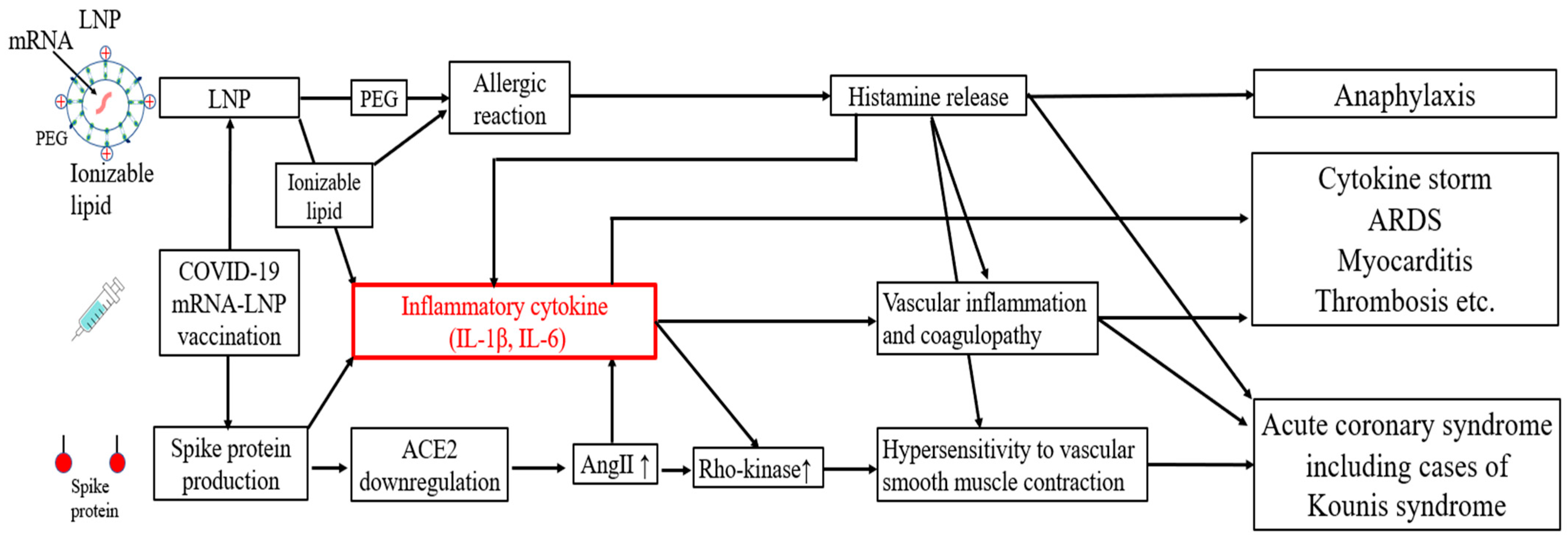
2.1. Mechanism of Cytokine Release Following COVID-19 mRNA-LNP Vaccination
2.2. Treatment of Cytokine Release Following COVID-19 mRNA-LNP Vaccination
2.3. Prevention of Cytokine Release Following COVID-19 mRNA-LNP Vaccination
3. IL-6 Levels and Symptoms Underlying Cytokine Release Following COVID-19 mRNA-LNP Vaccination
4. Mechanisms of Allergic Reactions to COVID-19 mRNA-LNP Vaccines
5. Kounis Syndrome Induced by Allergic Reactions to COVID-19 mRNA-LNP Vaccines
5.1. Mechanism of Kounis Syndrome
5.2. Diagnosis and Treatment of Kounis Syndrome
5.3. Medical History of Kounis Syndrome
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| COVID-19 | coronavirus disease 2019 |
| mRNA | messenger RNA |
| LNPs | lipid nanoparticles |
| PEG | polyethylene glycol |
| ACS | acute coronary syndrome |
| IL | interleukin |
| ACE2 | angiotensin-converting enzyme 2 |
| AngII | angiotensin II |
| m1Ψ | N1-methyl-pseudouridine |
| ARDS | acute respiratory distress syndrome |
| MDA5 | melanoma differentiation-associated gene 5 |
| siRNA | small interfering RNA |
| CAR-T | chimeric antigen receptor T-cell |
| GR | glucocorticoid receptor |
| PAI-1 | plasminogen activator inhibitor-1 |
| NLRP3 | NOD-like receptor family pyrin domain-containing 3 |
| CRP | C-reactive protein |
| ECG | electrocardiogram |
| IgE | immunoglobulin E |
| CARPA | complement activation-related pseudoallergy |
| MRGPRx2 | Mas-related G protein-coupled receptor X2 |
| PAF | platelet activating factor |
| CK | creatine kinase |
| ARs | adrenoceptors |
| ALDH2 | aldehyde dehydrogenase 2 |
| DAO | diamine oxidase |
| HIT | histamine intolerance |
| sa-mRNA | self-amplifying mRNA |
References
- Rosenblum, H.G.; Gee, J.; Liu, R.; Marquez, P.L.; Zhang, B.; Strid, P.; Abara, W.E.; McNeil, M.M.; Myers, T.R.; Hause, A.M.; et al. Safety of mRNA vaccines administered during the initial 6 months of the US COVID-19 vaccination programme: An observational study of reports to the Vaccine Adverse Event Reporting System and v-safe. Lancet Infect. Dis. 2022, 22, 802–812. [Google Scholar] [CrossRef] [PubMed]
- Murata, K.; Nakao, N.; Ishiuchi, N.; Fukui, T.; Katsuya, N.; Fukumoto, W.; Oka, H.; Yoshikawa, N.; Nagao, T.; Namera, A.; et al. Four cases of cytokine storm after COVID-19 vaccination: Case report. Front. Immunol. 2022, 13, 967226. [Google Scholar] [CrossRef] [PubMed]
- Nushida, H.; Ito, A.; Kurata, H.; Umemoto, H.; Tokunaga, I.; Iseki, H.; Nishimura, A. A case of fatal multi-organ inflammation following COVID-19 vaccination. Leg. Med. 2023, 63, 102244. [Google Scholar] [CrossRef]
- Guglin, M.E.; Etuk, A.; Shah, C.; Ilonze, O.J. Fulminant Myocarditis and Cardiogenic Shock Following COVID-19 Infection Versus COVID-19 Vaccination: A Systematic Literature Review. J. Clin. Med. 2023, 12, 1849. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Choi, J.H.; Jang, J.Y.; So, O.; Cho, E.; Choi, H.; Hong, K.S.; Park, K.T. A Case Report for Myopericarditis after BNT162b2 COVID-19 mRNA Vaccination in a Korean Young Male. J. Korean Med. Sci. 2021, 36, e277. [Google Scholar] [CrossRef]
- Ndeupen, S.; Qin, Z.; Jacobsen, S.; Bouteau, A.; Estanbouli, H.; Igyarto, B.Z. The mRNA-LNP platform’s lipid nanoparticle component used in preclinical vaccine studies is highly inflammatory. iScience 2021, 24, 103479. [Google Scholar] [CrossRef] [PubMed]
- Bergamaschi, C.; Terpos, E.; Rosati, M.; Angel, M.; Bear, J.; Stellas, D.; Karaliota, S.; Apostolakou, F.; Bagratuni, T.; Patseas, D.; et al. Systemic IL-15, IFN-gamma, and IP-10/CXCL10 signature associated with effective immune response to SARS-CoV-2 in BNT162b2 mRNA vaccine recipients. Cell Rep. 2021, 36, 109504. [Google Scholar] [CrossRef]
- Theobald, S.J.; Simonis, A.; Georgomanolis, T.; Kreer, C.; Zehner, M.; Eisfeld, H.S.; Albert, M.C.; Chhen, J.; Motameny, S.; Erger, F.; et al. Long-lived macrophage reprogramming drives spike protein-mediated inflammasome activation in COVID-19. EMBO Mol. Med. 2021, 13, e14150. [Google Scholar] [CrossRef]
- Allam, C.; Kounis, N.G.; Chlawit, R.; Saouma, M.; Badaoui, G. Kounis syndrome following COVID-19 vaccination. Bayl. Univ. Med. Cent. Proc. 2022, 35, 369–370. [Google Scholar] [CrossRef]
- Kuba, K.; Imai, Y.; Penninger, J.M. Multiple functions of angiotensin-converting enzyme 2 and its relevance in cardiovascular diseases. Circ. J. 2013, 77, 301–308. [Google Scholar] [CrossRef]
- Takahashi, J.; Suda, A.; Nishimiya, K.; Godo, S.; Yasuda, S.; Shimokawa, H. Pathophysiology and Diagnosis of Coronary Functional Abnormalities. Eur. Cardiol. 2021, 16, e30. [Google Scholar] [CrossRef] [PubMed]
- Morita, S.; Takagi, T.; Inaba, H.; Furukawa, Y.; Kishimoto, S.; Uraki, S.; Shimo, N.; Takeshima, K.; Uraki, S.; Doi, K.; et al. Effect of SARS-CoV-2 BNT162b2 mRNA vaccine on thyroid autoimmunity: A twelve-month follow-up study. Front. Endocrinol. 2023, 14, 1058007. [Google Scholar] [CrossRef] [PubMed]
- Irrgang, P.; Gerling, J.; Kocher, K.; Lapuente, D.; Steininger, P.; Habenicht, K.; Wytopil, M.; Beileke, S.; Schäfer, S.; Zhong, J.; et al. Class switch toward noninflammatory, spike-specific IgG4 antibodies after repeated SARS-CoV-2 mRNA vaccination. Sci. Immunol. 2023, 8, eade2798. [Google Scholar] [CrossRef] [PubMed]
- Rubio-Casillas, A.; Cowley, D.; Raszek, M.; Uversky, V.N.; Redwan, E.M. Review: N1-methyl-pseudouridine (m1Ψ): Friend or foe of cancer? Int. J. Biol. Macromol. 2024, 267, 131427. [Google Scholar] [CrossRef]
- Lonez, C.; Bessodes, M.; Scherman, D.; Vandenbranden, M.; Escriou, V.; Ruysschaert, J.M. Cationic lipid nanocarriers activate Toll-like receptor 2 and NLRP3 inflammasome pathways. Nanomedicine 2014, 10, 775–782. [Google Scholar] [CrossRef]
- Cullis, P.R.; Hope, M.J. Lipid Nanoparticle Systems for Enabling Gene Therapies. Mol. Ther. 2017, 25, 1467–1475. [Google Scholar] [CrossRef]
- Tenchov, R.; Bird, R.; Curtze, A.E.; Zhou, Q. Lipid Nanoparticles horizontal line From Liposomes to mRNA Vaccine Delivery, a Landscape of Research Diversity and Advancement. ACS Nano 2021, 15, 16982–17015. [Google Scholar] [CrossRef]
- Alameh, M.G.; Tombacz, I.; Bettini, E.; Lederer, K.; Sittplangkoon, C.; Wilmore, J.R.; Gaudette, B.T.; Soliman, O.Y.; Pine, M.; Hicks, P.; et al. Lipid nanoparticles enhance the efficacy of mRNA and protein subunit vaccines by inducing robust T follicular helper cell and humoral responses. Immunity 2021, 54, 2877–2892.e7. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Lee, A.; Grigoryan, L.; Arunachalam, P.S.; Scott, M.K.D.; Trisal, M.; Wimmers, F.; Sanyal, M.; Weidenbacher, P.A.; Feng, Y.; et al. Mechanisms of innate and adaptive immunity to the Pfizer-BioNTech BNT162b2 vaccine. Nat. Immunol. 2022, 23, 543–555. [Google Scholar] [CrossRef]
- Kobiyama, K.; Ishii, K.J. Making innate sense of mRNA vaccine adjuvanticity. Nat. Immunol. 2022, 23, 474–476. [Google Scholar] [CrossRef]
- Suhr, O.B.; Coelho, T.; Buades, J.; Pouget, J.; Conceicao, I.; Berk, J.; Schmidt, H.; Waddington-Cruz, M.; Campistol, J.M.; Bettencourt, B.R.; et al. Efficacy and safety of patisiran for familial amyloidotic polyneuropathy: A phase II multi-dose study. Orphanet J. Rare Dis. 2015, 10, 109. [Google Scholar] [CrossRef] [PubMed]
- Adams, D.; Gonzalez-Duarte, A.; O’Riordan, W.D.; Yang, C.C.; Ueda, M.; Kristen, A.V.; Tournev, I.; Schmidt, H.H.; Coelho, T.; Berk, J.L.; et al. Patisiran, an RNAi Therapeutic, for Hereditary Transthyretin Amyloidosis. N. Engl. J. Med. 2018, 379, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Staedtke, V.; Bai, R.Y.; Kim, K.; Darvas, M.; Davila, M.L.; Riggins, G.J.; Rothman, P.B.; Papadopoulos, N.; Kinzler, K.W.; Vogelstein, B.; et al. Disruption of a self-amplifying catecholamine loop reduces cytokine release syndrome. Nature 2018, 564, 273–277. [Google Scholar] [CrossRef] [PubMed]
- Neelapu, S.S.; Tummala, S.; Kebriaei, P.; Wierda, W.; Gutierrez, C.; Locke, F.L.; Komanduri, K.V.; Lin, Y.; Jain, N.; Daver, N.; et al. Chimeric antigen receptor T-cell therapy—Assessment and management of toxicities. Nat. Rev. Clin. Oncol. 2018, 15, 47–62. [Google Scholar] [CrossRef]
- Tay, S.H.; Toh, M.M.X.; Thian, Y.L.; Vellayappan, B.A.; Fairhurst, A.M.; Chan, Y.H.; Aminkeng, F.; Bharwani, L.D.; Huang, Y.; Mak, A.; et al. Cytokine Release Syndrome in Cancer Patients Receiving Immune Checkpoint Inhibitors: A Case Series of 25 Patients and Review of the Literature. Front. Immunol. 2022, 13, 807050. [Google Scholar] [CrossRef]
- Lee, D.W.; Santomasso, B.D.; Locke, F.L.; Ghobadi, A.; Turtle, C.J.; Brudno, J.N.; Maus, M.V.; Park, J.H.; Mead, E.; Pavletic, S.; et al. ASTCT Consensus Grading for Cytokine Release Syndrome and Neurologic Toxicity Associated with Immune Effector Cells. Biol. Blood Marrow Transpl. 2019, 25, 625–638. [Google Scholar] [CrossRef]
- Shen, J.; Li, J.; Lei, Y.; Chen, Z.; Wu, L.; Lin, C. Frontiers and hotspots evolution in cytokine storm: A bibliometric analysis from 2004 to 2022. Heliyon 2024, 10, e30955. [Google Scholar] [CrossRef] [PubMed]
- Le, R.Q.; Li, L.; Yuan, W.; Shord, S.S.; Nie, L.; Habtemariam, B.A.; Przepiorka, D.; Farrell, A.T.; Pazdur, R. FDA Approval Summary: Tocilizumab for Treatment of Chimeric Antigen Receptor T Cell-Induced Severe or Life-Threatening Cytokine Release Syndrome. Oncologist 2018, 23, 943–947. [Google Scholar] [CrossRef]
- Tuckermann, J.P.; Kleiman, A.; Moriggl, R.; Spanbroek, R.; Neumann, A.; Illing, A.; Clausen, B.E.; Stride, B.; Forster, I.; Habenicht, A.J.; et al. Macrophages and neutrophils are the targets for immune suppression by glucocorticoids in contact allergy. J. Clin. Investig. 2007, 117, 1381–1390. [Google Scholar] [CrossRef]
- Alcock, J.; Masters, A. Cytokine storms, evolution and COVID-19. Evol. Med. Public Health 2021, 9, 83–92. [Google Scholar] [CrossRef]
- Cruz-Topete, D.; Cidlowski, J.A. Glucocorticoids: Molecular Mechanisms of Action. In Immunopharmacology and Inflammation; Springer: Cham, Switzerland, 2018; pp. 249–266. [Google Scholar] [CrossRef]
- Kang, S.; Tanaka, T.; Inoue, H.; Ono, C.; Hashimoto, S.; Kioi, Y.; Matsumoto, H.; Matsuura, H.; Matsubara, T.; Shimizu, K.; et al. IL-6 trans-signaling induces plasminogen activator inhibitor-1 from vascular endothelial cells in cytokine release syndrome. Proc. Natl. Acad. Sci. USA 2020, 117, 22351–22356. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Minaga, K.; Hara, A.; Yoshikawa, T.; Kamata, K.; Kudo, M. Case Report: New-Onset Rheumatoid Arthritis Following COVID-19 Vaccination. Front. Immunol. 2022, 13, 859926. [Google Scholar] [CrossRef] [PubMed]
- Alunno, A.; Carubbi, F.; Ferri, C. Colchicine and cardiovascular prevention. Eur. J. Intern. Med. 2024, 121, 30–34. [Google Scholar] [CrossRef] [PubMed]
- Olsen, M.B.; Gregersen, I.; Sandanger, O.; Yang, K.; Sokolova, M.; Halvorsen, B.E.; Gullestad, L.; Broch, K.; Aukrust, P.; Louwe, M.C. Targeting the Inflammasome in Cardiovascular Disease. JACC Basic Transl. Sci. 2022, 7, 84–98. [Google Scholar] [CrossRef]
- Lee, S.Y.; Jeong, Y.H.; Yun, K.H.; Cho, J.Y.; Gorog, D.A.; Angiolillo, D.J.; Kim, J.W.; Jang, Y. P2Y(12) Inhibitor Monotherapy Combined with Colchicine Following PCI in ACS Patients: The MACT Pilot Study. JACC Cardiovasc. Interv. 2023, 16, 1845–1855. [Google Scholar] [CrossRef]
- Jadhav, K.P. Is Colchicine the New “Aspirin”? Indian J. Clin. Cardiol. 2024, 5, 42–49. [Google Scholar] [CrossRef]
- Yamamoto, J.; Awaya, T.; Nakagawa, T.; Tamura, A.; Hiroi, Y. Myocarditis with ventricular tachycardia following bivalent COVID-19 mRNA vaccination. CJC Open 2023, 5, 654–657. [Google Scholar] [CrossRef]
- Flego, D.; Cesaroni, S.; Romiti, G.F.; Corica, B.; Marrapodi, R.; Scafa, N.; Maiorca, F.; Lombardi, L.; Pallucci, D.; Pulcinelli, F.; et al. Platelet and immune signature associated with a rapid response to the BNT162b2 mRNA COVID-19 vaccine. J. Thromb. Haemost. 2022, 20, 961–974. [Google Scholar] [CrossRef]
- Tardif, J.C.; Kouz, S.; Waters, D.D.; Bertrand, O.F.; Diaz, R.; Maggioni, A.P.; Pinto, F.J.; Ibrahim, R.; Gamra, H.; Kiwan, G.S.; et al. Efficacy and Safety of Low-Dose Colchicine after Myocardial Infarction. N. Engl. J. Med. 2019, 381, 2497–2505. [Google Scholar] [CrossRef]
- Hoekstra, S.P.; Bishop, N.C.; Faulkner, S.H.; Bailey, S.J.; Leicht, C.A. Acute and chronic effects of hot water immersion on inflammation and metabolism in sedentary, overweight adults. J. Appl. Physiol. 2018, 125, 2008–2018. [Google Scholar] [CrossRef]
- Awaya, T.; Moroi, M.; Enomoto, Y.; Kunimasa, T.; Nakamura, M. What Should We Do after the COVID-19 Vaccination? Vaccine-Associated Diseases and Precautionary Measures against Adverse Reactions. Vaccines 2022, 10, 866. [Google Scholar] [CrossRef] [PubMed]
- Khakroo Abkenar, I.; Rahmani-Nia, F.; Lombardi, G. The Effects of Acute and Chronic Aerobic Activity on the Signaling Pathway of the Inflammasome NLRP3 Complex in Young Men. Medicina 2019, 55, 105. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.R.; Abshire, K.M.; Farokhnia, M.; Akhlaghi, F.; Leggio, L. Effect of oral alcohol administration on plasma cytokine concentrations in heavy drinking individuals. Drug Alcohol. Depend. 2021, 225, 108771. [Google Scholar] [CrossRef]
- Amioka, N.; Nakamura, K.; Kimura, T.; Ohta-Ogo, K.; Tanaka, T.; Toji, T.; Akagi, S.; Nakagawa, K.; Toh, N.; Yoshida, M.; et al. Pathological and clinical effects of interleukin-6 on human myocarditis. J. Cardiol. 2021, 78, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.W.; Yap, S.F.; Amin-Nordin, S.; Ngeow, Y.F. Cardiac and Neurological Complications Post COVID-19 Vaccination: A Systematic Review of Case Reports and Case Series. Vaccines 2024, 12, 575. [Google Scholar] [CrossRef]
- Eriksson, U.; Kurrer, M.O.; Schmitz, N.; Marsch, S.C.; Fontana, A.; Eugster, H.P.; Kopf, M. Interleukin-6-deficient mice resist development of autoimmune myocarditis associated with impaired upregulation of complement C3. Circulation 2003, 107, 320–325. [Google Scholar] [CrossRef]
- Tall, A.R.; Bornfeldt, K.E. Inflammasomes and Atherosclerosis: A Mixed Picture. Circ. Res. 2023, 132, 1505–1520. [Google Scholar] [CrossRef] [PubMed]
- Koizumi, T.; Awaya, T.; Yoshioka, K.; Kitano, S.; Hayama, H.; Amemiya, K.; Enomoto, Y.; Yazaki, Y.; Moroi, M.; Nakamura, M. Myocarditis after COVID-19 mRNA vaccines. QJM 2021, 114, 741–743. [Google Scholar] [CrossRef]
- Oster, M.E.; Shay, D.K.; Su, J.R.; Gee, J.; Creech, C.B.; Broder, K.R.; Edwards, K.; Soslow, J.H.; Dendy, J.M.; Schlaudecker, E.; et al. Myocarditis Cases Reported After mRNA-Based COVID-19 Vaccination in the US From December 2020 to August 2021. JAMA 2022, 327, 331–340. [Google Scholar] [CrossRef]
- Noe, A.; Dang, T.D.; Axelrad, C.; Burrell, E.; Germano, S.; Elia, S.; Burgner, D.; Perrett, K.P.; Curtis, N.; Messina, N.L. BNT162b2 COVID-19 vaccination in children alters cytokine responses to heterologous pathogens and Toll-like receptor agonists. Front. Immunol. 2023, 14, 1242380. [Google Scholar] [CrossRef]
- Pisoschi, A.M.; Pop, A.; Iordache, F.; Stanca, L.; Geicu, O.I.; Bilteanu, L.; Serban, A.I. Antioxidant, anti-inflammatory and immunomodulatory roles of vitamins in COVID-19 therapy. Eur. J. Med. Chem. 2022, 232, 114175. [Google Scholar] [CrossRef] [PubMed]
- Moghimi, S.M. Allergic Reactions and Anaphylaxis to LNP-Based COVID-19 Vaccines. Mol. Ther. 2021, 29, 898–900. [Google Scholar] [CrossRef]
- Kounis, N.G.; Koniari, I.; de Gregorio, C.; Velissaris, D.; Petalas, K.; Brinia, A.; Assimakopoulos, S.F.; Gogos, C.; Kouni, S.N.; Kounis, G.N.; et al. Allergic Reactions to Current Available COVID-19 Vaccinations: Pathophysiology, Causality, and Therapeutic Considerations. Vaccines 2021, 9, 221. [Google Scholar] [CrossRef]
- Risma, K.A. COVID-19 mRNA vaccine allergy. Curr. Opin. Pediatr. 2021, 33, 610–617. [Google Scholar] [CrossRef] [PubMed]
- Dézsi, L.; Mészáros, T.; Kozma, G.; H-Velkei, M.; Oláh, C.Z.; Patkó, Z.; Fülöp, T.; Hennies, M.; Szebeni, M.; Barta, B.A.; et al. A naturally hypersensitive porcine model may help understand the mechanism of COVID-19 mRNA vaccine-induced rare (pseudo) allergic reactions: Complement activation as a possible contributing factor. Geroscience 2022, 44, 597–618. [Google Scholar] [CrossRef] [PubMed]
- Kozma, G.T.; Meszaros, T.; Berenyi, P.; Facsko, R.; Patko, Z.; Olah, C.Z.; Nagy, A.; Fulop, T.G.; Glatter, K.A.; Radovits, T.; et al. Role of anti-polyethylene glycol (PEG) antibodies in the allergic reactions to PEG-containing COVID-19 vaccines: Evidence for immunogenicity of PEG. Vaccine 2023, 41, 4561–4570. [Google Scholar] [CrossRef] [PubMed]
- Kounis, N.G. Kounis syndrome: An update on epidemiology, pathogenesis, diagnosis and therapeutic management. Clin. Chem. Lab. Med. 2016, 54, 1545–1559. [Google Scholar] [CrossRef]
- Brancaccio, R.; Bonzano, L.; Cocconcelli, A.; Boyko, R.; Ienopoli, G.; Motolese, A. Recurrent Kounis Syndrome: A Case Report and Literature Review. J. Clin. Med. 2024, 13, 1647. [Google Scholar] [CrossRef]
- Masuda, M.; Fujimoto, W.; Yamashita, S.; Takemoto, M.; Kuroda, K.; Imanishi, J.; Iwasaki, M.; Todoroki, T.; Okuda, M.; Hayashi, T. Recurrent cardiac arrests caused by Kounis syndrome without typical allergic symptoms. J. Cardiol. Cases 2023, 27, 47–51. [Google Scholar] [CrossRef]
- Awaya, T.; Moroi, M.; Nakamura, F.; Toi, S.; Wakiya, M.; Enomoto, Y.; Kunimasa, T.; Nakamura, M. A Possibility of Vasospastic Angina after mRNA COVID-19 Vaccination. Vaccines 2022, 10, 1998. [Google Scholar] [CrossRef]
- Choi, Y.J.; Lim, J.; Bea, S.; Lee, J.; Choi, J.Y.; Rho, S.Y.; Lee, D.I.; Na, J.O.; Kim, H.K. Thromboembolism after coronavirus disease 2019 vaccination in atrial fibrillation/flutter: A self-controlled case series study. Eur. Heart J. 2024, 45, 2983–2991. [Google Scholar] [CrossRef]
- Aye, Y.N.; Mai, A.S.; Zhang, A.; Lim, O.Z.H.; Lin, N.; Ng, C.H.; Chan, M.Y.; Yip, J.; Loh, P.H.; Chew, N.W.S. Acute Myocardial Infarction and Myocarditis following COVID-19 Vaccination. QJM 2021, 116, 279–283. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, R.A.; Regateiro, F.S.; Pita, J.; Ribeiro, C.; Carrapatoso, I.; Todo-Bom, A.; Faria, E. Severe Anaphylaxis with Cardiac Arrest Caused by Prick Test with Cefuroxime. J. Investig. Allergol. Clin. Immunol. 2018, 28, 426–428. [Google Scholar] [CrossRef]
- Sakaue, T.; Inaba, S.; Sumimoto, T.; Saito, M. Intravascular ultrasound-confirmed plaque rupture following multiple bee stings. Eur. Heart J. 2020, 41, 1374. [Google Scholar] [CrossRef]
- Ng, B.H.; Tan, H.X.; Vijayasingham, S. Kounis syndrome following solenopsis (fire ant) bite. Med. J. Malays. 2019, 74, 344–346. [Google Scholar]
- Filipiak, K.J.; Tarchalska-Krynska, B.; Opolski, G.; Rdzanek, A.; Kochman, J.; Kosior, D.A.; Czlonkowski, A. Tryptase levels in patients after acute coronary syndromes: The potential new marker of an unstable plaque? Clin. Cardiol. 2003, 26, 366–372. [Google Scholar] [CrossRef] [PubMed]
- Khan, S. Mast cell tryptase level should be checked in all patients with suspected Kounis syndrome. Eur. Heart J. 2020, 41, 3018. [Google Scholar] [CrossRef]
- Kounis, N.G. Coronary hypersensitivity disorder: The Kounis syndrome. Clin. Ther. 2013, 35, 563–571. [Google Scholar] [CrossRef] [PubMed]
- Shamizadeh, S.; Brockow, K.; Ring, J. Rupatadine: Efficacy and safety of a non-sedating antihistamine with PAF-antagonist effects. Allergo J. Int. 2014, 23, 87–95. [Google Scholar] [CrossRef]
- Goto, K.; Kasama, S.; Sato, M.; Kurabayashi, M. Myocardial scintigraphic evidence of Kounis syndrome: What is the aetiology of acute coronary syndrome? Eur. Heart J. 2016, 37, 1157. [Google Scholar] [CrossRef]
- Church, M.K.; Hiroi, J. Inhibition of IgE-dependent histamine release from human dispersed lung mast cells by anti-allergic drugs and salbutamol. Br. J. Pharmacol. 1987, 90, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Urushidani, S.; Kuriyama, A. A potential association between myocardial ischemia and epinephrine for anaphylaxis. Am. J. Emerg. Med. 2020, 38, 1297.e1–1297.e3. [Google Scholar] [CrossRef] [PubMed]
- Shintani, R.; Sekino, M.; Egashira, T.; Yano, R.; Inoue, H.; Matsumoto, S.; Higashijima, U.; Matsumoto, S.; Yonekura, T.; Hara, T. Allergen-Related Coronary Vasospasm “Kounis Syndrome” Requiring Administration of Epinephrine and a Coronary Vasodilator. J. Cardiothorac. Vasc. Anesth. 2021, 35, 2768–2771. [Google Scholar] [CrossRef] [PubMed]
- Tan, P.Z.; Chew, N.W.S.; Tay, S.H.; Chang, P. The allergic myocardial infarction dilemma: Is it the anaphylaxis or the epinephrine? J. Thromb. Thrombolysis 2021, 52, 941–948. [Google Scholar] [CrossRef]
- Takagi, S.; Goto, Y.; Hirose, E.; Terashima, M.; Sakuragi, S.; Suzuki, S.; Tsutsumi, Y.; Miyazaki, S.; Nonogi, H. Successful treatment of refractory vasospastic angina with corticosteroids: Coronary arterial hyperactivity caused by local inflammation? Circ. J. 2004, 68, 17–22. [Google Scholar] [CrossRef]
- Mizuno, Y.; Hokimoto, S.; Harada, E.; Kinoshita, K.; Yoshimura, M.; Yasue, H. Variant Aldehyde Dehydrogenase 2 (ALDH2*2) in East Asians Interactively Exacerbates Tobacco Smoking Risk for Coronary Spasm—Possible Role of Reactive Aldehydes. Circ. J. 2016, 81, 96–102. [Google Scholar] [CrossRef]
- Schnedl, W.J.; Enko, D. Histamine Intolerance Originates in the Gut. Nutrients 2021, 13, 1262. [Google Scholar] [CrossRef]
- Jochum, C. Histamine Intolerance: Symptoms, Diagnosis, and Beyond. Nutrients 2024, 16, 1219. [Google Scholar] [CrossRef]
- Comas-Baste, O.; Sanchez-Perez, S.; Veciana-Nogues, M.T.; Latorre-Moratalla, M.; Vidal-Carou, M.D.C. Histamine Intolerance: The Current State of the Art. Biomolecules 2020, 10, 1181. [Google Scholar] [CrossRef]
- Molnar, E.L.; Hegyesi, H.; Toth, S.; Darvas, Z.; Laszlo, V.; Szalai, C.; Falus, A. Biosynthesis of interleukin-6, an autocrine growth factor for melanoma, is regulated by melanoma-derived histamine. Semin. Cancer Biol. 2000, 10, 25–28. [Google Scholar] [CrossRef]
- Morimitsu, A.; Sumigama, S.; Kotani, T.; Mano, Y.; Suzuki, K.; Araki-Taguchi, M.; Yamamoto, E.; Hayakawa, H.; Okada, M.; Itakura, A.; et al. Histamine stimulates interleukin-6 production through histamine H1 receptors in human amnion cells. Gynecol. Obs. Investig. 2010, 69, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Kuda, Y.; Shibamoto, T.; Yang, W.; Zhang, T.; Tanida, M.; Kurata, Y. Blockade of beta2-adrenoceptor, rather than beta1-adrenoceptor, deteriorates cardiac anaphylaxis in isolated blood-perfused rat hearts. Cardiol. J. 2017, 24, 403–408. [Google Scholar] [CrossRef]
- Sampson, H.A.; Munoz-Furlong, A.; Campbell, R.L.; Adkinson, N.F., Jr.; Bock, S.A.; Branum, A.; Brown, S.G.; Camargo, C.A., Jr.; Cydulka, R.; Galli, S.J.; et al. Second symposium on the definition and management of anaphylaxis: Summary report—Second National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network symposium. J. Allergy Clin. Immunol. 2006, 117, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Kiaie, S.H.; Majidi Zolbanin, N.; Ahmadi, A.; Bagherifar, R.; Valizadeh, H.; Kashanchi, F.; Jafari, R. Recent advances in mRNA-LNP therapeutics: Immunological and pharmacological aspects. J. Nanobiotechnology 2022, 20, 276. [Google Scholar] [CrossRef] [PubMed]
- Adams, D.; Tournev, I.L.; Taylor, M.S.; Coelho, T.; Plante-Bordeneuve, V.; Berk, J.L.; Gonzalez-Duarte, A.; Gillmore, J.D.; Low, S.C.; Sekijima, Y.; et al. Efficacy and safety of vutrisiran for patients with hereditary transthyretin-mediated amyloidosis with polyneuropathy: A randomized clinical trial. Amyloid 2023, 30, 18–26. [Google Scholar] [CrossRef]
- Abbasi, S.; Matsui-Masai, M.; Yasui, F.; Hayashi, A.; Tockary, T.A.; Mochida, Y.; Akinaga, S.; Kohara, M.; Kataoka, K.; Uchida, S. Carrier-free mRNA vaccine induces robust immunity against SARS-CoV-2 in mice and non-human primates without systemic reactogenicity. Mol. Ther. 2024, 32, 1266–1283. [Google Scholar] [CrossRef]
- Ho, N.T.; Hughes, S.G.; Ta, V.T.; Phan, L.T.; Do, Q.; Nguyen, T.V.; Pham, A.T.V.; Thi Ngoc Dang, M.; Nguyen, L.V.; Trinh, Q.V.; et al. Safety, immunogenicity and efficacy of the self-amplifying mRNA ARCT-154 COVID-19 vaccine: Pooled phase 1, 2, 3a and 3b randomized, controlled trials. Nat. Commun. 2024, 15, 4081. [Google Scholar] [CrossRef]
- Silva-Pilipich, N.; Beloki, U.; Salaberry, L.; Smerdou, C. Self-Amplifying RNA: A Second Revolution of mRNA Vaccines against COVID-19. Vaccines 2024, 12, 318. [Google Scholar] [CrossRef]
- Saputra, P.B.T.; Kurniawan, R.B.; Trilistyoati, D.; Farabi, M.J.A.; Susilo, H.; Alsagaff, M.Y.; Oktaviono, Y.H.; Sutanto, H.; Gusnanto, A.; Dyah Kencono Wungu, C. Myocarditis and coronavirus disease 2019 vaccination: A systematic review and meta-summary of cases. Biomol. Biomed. 2023, 23, 546–567. [Google Scholar] [CrossRef]
- CDC. CDC Vaccines & Immunizations. Interim Clinical Considerations for Use of COVID-19 Vaccines in the United States. Available online: https://www.cdc.gov/vaccines/covid-19/clinical-considerations/interim-considerations-us.html (accessed on 24 July 2024).

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Awaya, T.; Hara, H.; Moroi, M. Cytokine Storms and Anaphylaxis Following COVID-19 mRNA-LNP Vaccination: Mechanisms and Therapeutic Approaches. Diseases 2024, 12, 231. https://doi.org/10.3390/diseases12100231
Awaya T, Hara H, Moroi M. Cytokine Storms and Anaphylaxis Following COVID-19 mRNA-LNP Vaccination: Mechanisms and Therapeutic Approaches. Diseases. 2024; 12(10):231. https://doi.org/10.3390/diseases12100231
Chicago/Turabian StyleAwaya, Toru, Hidehiko Hara, and Masao Moroi. 2024. "Cytokine Storms and Anaphylaxis Following COVID-19 mRNA-LNP Vaccination: Mechanisms and Therapeutic Approaches" Diseases 12, no. 10: 231. https://doi.org/10.3390/diseases12100231
APA StyleAwaya, T., Hara, H., & Moroi, M. (2024). Cytokine Storms and Anaphylaxis Following COVID-19 mRNA-LNP Vaccination: Mechanisms and Therapeutic Approaches. Diseases, 12(10), 231. https://doi.org/10.3390/diseases12100231