
Post-COVID-19 Anosmia and Therapies: Stay Tuned for New Drugs to Sniff Out

 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Phase 1 Clinical Trials
3.2. Phase 2 Clinical Trials
3.3. Phase 1–2 Clinical Trials
3.4. Phase 2–3 Clinical Trials
3.5. Phase 3 Clinical Trials
3.6. Phase 4 Clinical Trials
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Petrella, C.; Zingaropoli, M.A.; Ceci, F.M.; Pasculli, P.; Latronico, T.; Liuzzi, G.M.; Ciardi, M.R.; Angeloni, A.; Ettorre, E.; Menghi, M.; et al. COVID-19 Affects Serum Brain-Derived Neurotrophic Factor and Neurofilament Light Chain in Aged Men: Implications for Morbidity and Mortality. Cells 2023, 12, 655. [Google Scholar] [CrossRef]
- Tong, J.Y.; Wong, A.; Zhu, D.; Fastenberg, J.H.; Tham, T. The Prevalence of Olfactory and Gustatory Dysfunction in COVID-19 Patients: A Systematic Review and Meta-analysis. Otolaryngol. Neck Surg. 2020, 163, 3–11. [Google Scholar] [CrossRef]
- Kaye, R.; Chang, C.W.D.; Kazahaya, K.; Brereton, J.; Denneny, I.J.C. COVID-19 Anosmia Reporting Tool: Initial Findings. Otolaryngol. Head Neck Surg. 2020, 163, 132–134. [Google Scholar] [CrossRef]
- Fatuzzo, I.; Niccolini, G.F.; Zoccali, F.; Cavalcanti, L.; Bellizzi, M.G.; Riccardi, G.; de Vincentiis, M.; Fiore, M.; Petrella, C.; Minni, A.; et al. Neurons, Nose, and Neurodegenerative Diseases: Olfactory Function and Cognitive Impairment. Int. J. Mol. Sci. 2023, 24, 2117. [Google Scholar] [CrossRef]
- Meng, X.; Deng, Y.; Dai, Z.; Meng, Z. COVID-19 and anosmia: A review based on up-to-date knowledge. Am. J. Otolaryngol. 2020, 41, 102581. [Google Scholar] [CrossRef] [PubMed]
- Rocha-Filho, P.A.S.; Albuquerque, P.M.; Carvalho, L.C.L.S.; Gama, M.D.P.; Magalhães, J.E. Headache, anosmia, ageusia and other neurological symptoms in COVID-19: A cross-sectional study. J. Headache Pain 2022, 23, 2. [Google Scholar] [CrossRef] [PubMed]
- Sayin, I.; Devecioğlu, I.; Yazıcı, Z.M. A Closed Chamber ENT Examination Unit for Aerosol-Generating Endoscopic Examinations of COVID-19 Patients. Ear. Nose Throat J. 2020, 99, 594–596. [Google Scholar] [CrossRef]
- Hummel, T.; Podlesek, D. Clinical assessment of olfactory function. Chem. Senses 2021, 46, bjab053. [Google Scholar] [CrossRef] [PubMed]
- Hummel, T.; Kobal, G.; Gudziol, H.; Mackay-Sim, A. Normative data for the “Sniffin’ Sticks” including tests of odor identification, odor discrimination, and olfactory thresholds: AN upgrade based on a group of more than 3000 subjects. Eur. Arch. Otorhinolaryngol. 2007, 264, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Rombaux, P.; Duprez, T.; Hummel, T. Olfactory bulb volume in the clinical assessment of olfactory dysfunction. Rhinology 2009, 47, 3–9. [Google Scholar]
- Boesveldt, S.; Postma, E.M.; Boak, D.; Welge-Luessen, A.; Schöpf, V.; Mainland, J.D.; Martens, J.; Ngai, J.; Duffy, V.B. Anosmia—A Clinical Review. Chem. Senses 2017, 42, 513–523. [Google Scholar] [CrossRef]
- Le Bon, S.-D.; Konopnicki, D.; Pisarski, N.; Prunier, L.; Lechien, J.R.; Horoi, M. Efficacy and safety of oral corticosteroids and olfactory training in the management of COVID-19-related loss of smell. Eur. Arch. Oto-Rhino-Laryngology 2021, 278, 3113–3117. [Google Scholar] [CrossRef]
- Lerner, D.; Garvey, K.; Arrighi-Allisan, A.; Filimonov, A.; Filip, P.; Liu, K.; Ninan, S.; Schaberg, M.; Colley, P.; Del Signore, A.; et al. Letter to the editor: Study Summary Randomized Control Trial of Omega-3 Fatty Acid Supplementation for the Treatment of COVID-19 Related Olfactory Dysfunction. Trials 2020, 21, 942. [Google Scholar] [CrossRef] [PubMed]
- Elkazzaz, M.; Haydara, T.; Abo-Amer, Y.E.-E.; Sahyon, H.; Shamkh, I.S.; El Magd, M.F.A.; Ahmed, A. STRA6, as A Novel Binding Receptor of COVID-19, A Breakthrough that Could Explain COVID-19 Symptoms with Unknown Aetiology. 27 September 2021, PREPRINT (Version 1) Available at Research Square. Available online: https://doi.org/10.21203/rs.3.rs-936697/v1 (accessed on 25 February 2023).
- Lechien, J.R.; Chiesa-Estomba, C.M.; De Siati, D.R.; Horoi, M.; Le Bon, S.D.; Rodriguez, A.; Dequanter, D.; Blecic, S.; El Afia, F.; Distinguin, L.; et al. Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): A multicenter European study. Eur. Arch. Oto-Rhino-Laryngol. 2020, 277, 2251–2261. [Google Scholar] [CrossRef] [PubMed]
- O’Byrne, L.; Webster, K.E.; MacKeith, S.; Philpott, C.; Hopkins, C.; Burton, M.J. Interventions for the treatment of persistent post-COVID-19 olfactory dysfunction. Cochrane Database Syst. Rev. 2022, 9, CD013876. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.M.; Kallogjeri, D.; Piccirillo, J.F. Growing Public Health Concern of COVID-19 Chronic Olfactory Dysfunction. JAMA Otolaryngol. Neck Surg. 2022, 148, 81. [Google Scholar] [CrossRef]
- Aref, Z.F.; Bazeed, S.E.E.S.; Hassan, M.H.; Hassan, A.S.; Ghweil, A.A.; Sayed, M.A.A.; Rashad, A.; Mansour, H.; Abdelmaksoud, A.A. Possible Role of Ivermectin Mucoadhesive Nanosuspension Nasal Spray in Recovery of Post-COVID-19 Anosmia. Infect. Drug Resist. 2022, 15, 5483–5494. [Google Scholar] [CrossRef]
- Gupta, S.; Lee, J.J.; Perrin, A.; Khan, A.; Smith, H.J.; Farrell, N.; Kallogjeri, D.; Piccirillo, J.F. Efficacy and Safety of Saline Nasal Irrigation Plus Theophylline for Treatment of COVID-19–Related Olfactory Dysfunction: The SCENT2 Phase 2 Randomized Clinical Trial. JAMA Otolaryngol. Neck Surg. 2022, 148, 830. [Google Scholar] [CrossRef]
- Gupta, S.; Kallogjeri, D.; Farrell, N.F.; Lee, J.J.; Smith, H.J.; Khan, A.M.; Piccirillo, J.F. Development and Validation of a Novel At-home Smell Assessment. JAMA Otolaryngol. Neck Surg. 2022, 148, 252. [Google Scholar] [CrossRef]
- Rezaeian, A. Effect of Intranasal Insulin on Olfactory Recovery in Patients with Hyposmia: A Randomized Clinical Trial. Otolaryngol. Neck Surg. 2018, 158, 1134–1139. [Google Scholar] [CrossRef] [PubMed]
- Spoorenberg, S.M.C.; Deneer, V.H.M.; Grutters, J.C.; Pulles, A.E.; Voorn, G.P.P.; Rijkers, G.T.; Bos, W.J.W.; van de Garde, E.M.W. Pharmacokinetics of oral vs. intravenous dexamethasone in patients hospitalized with community-acquired pneumonia. Br. J. Clin. Pharmacol. 2014, 78, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Dupuis, J.; Laurin, P.; Tardif, J.-C.; Hausermann, L.; Rosa, C.; Guertin, M.-C.; Thibaudeau, K.; Gagnon, L.; Cesari, F.; Robitaille, M.; et al. Fourteen-Day Evolution of COVID-19 Symptoms during the Third Wave in Nonvaccinated Subjects and Effects of Hesperidin Therapy: A Randomized, Double-Blinded, Placebo-Controlled Study. Evid. Based Complement. Altern. Med. 2022, 2022, 3125662. [Google Scholar] [CrossRef]
- Rashid, R.A.; Zgair, A.; Al-Ani, R.M. Effect of nasal corticosteroid in the treatment of anosmia due to COVID-19: A randomised double-blind placebo-controlled study. Am. J. Otolaryngol. 2021, 42, 103033. [Google Scholar] [CrossRef]
- Steffens, Y.; Le Bon, S.-D.; Lechien, J.; Prunier, L.; Rodriguez, A.; Saussez, S.; Horoi, M. Effectiveness and safety of PRP on persistent olfactory dysfunction related to COVID-19. Eur. Arch. Oto-Rhino-Laryngology 2022, 279, 5951–5953. [Google Scholar] [CrossRef]
- Popovych, V.; Koshel, I.; Haman, Y.; Leschak, V.; Malofiichuk, O.; Kapustina, N.; Shevaga, I.; Shevaga, O.; Kunytska, T. A randomized, open-label, multicentre, comparative study of therapeutic efficacy, safety, and tolerability of BNO 1030 extract, containing marshmallow root, chamomile flowers, horsetail herb, walnut leaves, yarrow herb, oak bark, dandelion herb, in the treatment of mild forms of COVID-19. Clin. Phytoscience 2021, 7, 72. [Google Scholar] [CrossRef]
- Ngo, B.T.; Marik, P.; Kory, P.; Shapiro, L.; Thomadsen, R.; Iglesias, J.; Ditmore, S.; Rendell, M.; Varon, J.; Dubé, M.; et al. The time to offer treatments for COVID-19. Expert Opin. Investig. Drugs 2021, 30, 505–518. [Google Scholar] [CrossRef] [PubMed]
- Fonteyn, S.; Huart, C.; Deggouj, N.; Collet, S.; Eloy, P.; Rombaux, P. Non-sinonasal-related olfactory dysfunction: A cohort of 496 patients. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2014, 131, 87–91. [Google Scholar] [CrossRef]
- Schlosser, R.J.; Desiato, V.M.; Storck, K.A.; Nguyen, S.A.; Hill, J.B.; Washington, B.J.; Noonan, T.E.; Lamira, J.; Mulligan, J.K.; Rowan, N.R.; et al. A Community-Based Study on the Prevalence of Olfactory Dysfunction. Am. J. Rhinol. Allergy 2020, 34, 661–670. [Google Scholar] [CrossRef]
- Doty, R.L.; Shaman, P.; Kimmelman, C.P.; Dann, M.S. University of pennsylvania smell identification test: A rapid quantitative olfactory function test for the clinic. Laryngoscope 1984, 94, 176–178. [Google Scholar] [CrossRef]
- Mathieson, S.; Lin, C.-W.C.; Underwood, M.; Eldabe, S. Pregabalin and gabapentin for pain. BMJ 2020, 369, m1315. [Google Scholar] [CrossRef]
- Adhikari, B.; Marasini, B.P.; Rayamajhee, B.; Bhattarai, B.R.; Lamichhane, G.; Khadayat, K.; Adhikari, A.; Khanal, S.; Parajuli, N. Potential roles of medicinal plants for the treatment of viral diseases focusing on COVID-19: A review. Phytotherapy Res. 2021, 35, 1298–1312. [Google Scholar] [CrossRef] [PubMed]
- Neta, F.I.; Fernandes, A.C.L.; Vale, A.J.M.; Pinheiro, F.I.; Cobucci, R.N.; de Azevedo, E.P.; Guzen, F.P. Pathophysiology and possible treatments for olfactory-gustatory disorders in patients affected by COVID-19. Curr. Res. Pharmacol. Drug Discov. 2021, 2, 100035. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.D.; Duricka, D.L. Stellate ganglion block reduces symptoms of Long COVID: A case series. J. Neuroimmunol. 2022, 362, 577784. [Google Scholar] [CrossRef] [PubMed]
- Abdelalim, A.A.; Mohamady, A.A.; Elsayed, R.A.; Elawady, M.A.; Ghallab, A.F. Corticosteroid nasal spray for recovery of smell sensation in COVID-19 patients: A randomized controlled trial. Am. J. Otolaryngol. 2021, 42, 102884. [Google Scholar] [CrossRef]
- Hura, N.; Xie, D.X.; Choby, G.W.; Schlosser, R.J.; Orlov, C.P.; Seal, S.M.; Rowan, N.R. Treatment of post-viral olfactory dysfunction: An evidence-based review with recommendations. Int. Forum Allergy Rhinol. 2020, 10, 1065–1086. [Google Scholar] [CrossRef]
- Daval, M.; Corré, A.; Palpacuer, C.; Housset, J.; Poillon, G.; Eliezer, M.; Verillaud, B.; Slama, D.; Ayache, D.; Herman, P.; et al. Efficacy of local budesonide therapy in the management of persistent hyposmia in COVID-19 patients without signs of severity: A structured summary of a study protocol for a randomised controlled trial. Trials 2020, 21, 666. [Google Scholar] [CrossRef]
- Mohamad, S.A.; Badawi, A.M.; Mansour, H.F. Insulin fast-dissolving film for intranasal delivery via olfactory region, a promising approach for the treatment of anosmia in COVID-19 patients: Design, in-vitro characterization and clinical evaluation. Int. J. Pharm. 2021, 601, 120600. [Google Scholar] [CrossRef]
- Di Stadio, A.; D’ascanio, L.; Vaira, L.A.; Cantone, E.; De Luca, P.; Cingolani, C.; Motta, G.; De Riu, G.; Vitelli, F.; Spriano, G.; et al. Ultramicronized Palmitoylethanolamide and Luteolin Supplement Combined with Olfactory Training to Treat Post-COVID-19 Olfactory Impairment: A Multi-Center Double-Blinded Randomized Placebo-Controlled Clinical Trial. Curr. Neuropharmacol. 2022, 20, 2001–2012. [Google Scholar] [CrossRef]
- Skaper, S.D.; Facci, L.; Giusti, P. Glia and Mast Cells as Targets for Palmitoylethanolamide, an Anti-inflammatory and Neuroprotective Lipid Mediator. Mol. Neurobiol. 2013, 48, 340–352. [Google Scholar] [CrossRef]
- Muresanu, D.F.; Florian, S.; Hömberg, V.; Matula, C.; Von Steinbüchel, N.; Vos, P.E.; Von Wild, K.; Birle, C.; Muresanu, I.; Slavoaca, D.; et al. Efficacy and safety of cerebrolysin in neurorecovery after moderate-severe traumatic brain injury: Results from the CAPTAIN II trial. Neurol. Sci. 2020, 41, 1171–1181. [Google Scholar] [CrossRef]
- Fiani, B.; Covarrubias, C.; Wong, A.; Doan, T.; Reardon, T.; Nikolaidis, D.; Sarno, E. Cerebrolysin for stroke, neurodegeneration, and traumatic brain injury: Review of the literature and outcomes. Neurol. Sci. 2021, 42, 1345–1353. [Google Scholar] [CrossRef]
- Cui, S.; Chen, N.; Yang, M.; Guo, J.; Zhou, M.; Zhu, C.; He, L. Cerebrolysin for vascular dementia. Cochrane Database Syst. Rev. 2019, 2019, CD008900. [Google Scholar] [CrossRef] [PubMed]
- Brainin, M. Cerebrolysin: A multi-target drug for recovery after stroke. Expert Rev. Neurother. 2018, 18, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Alzoubi, K.H.; Al-Jamal, F.F.; Mahasneh, A.F. Cerebrolysin prevents sleep deprivation induced memory impairment and oxidative stress. Physiol. Behav. 2020, 217, 112823. [Google Scholar] [CrossRef]
- Tran, H.T.T.; Peterburs, P.; Seibel, J.; Abramov-Sommariva, D.; Lamy, E. In vitro Screening of Herbal Medicinal Products for Their Supportive Curing Potential in the Context of SARS-CoV-2. Evid. Based Complement. Altern. Med. 2022, 2022, 8038195. [Google Scholar] [CrossRef] [PubMed]
- Noy, N. Vitamin A Transport and Cell Signaling by the Retinol-Binding Protein Receptor STRA6. Subcell Biochem. 2016, 81, 77–93. [Google Scholar] [CrossRef]
- Elkazzaz, M.; Abo-Amer, Y.E.-E.; Ahmed, A.; Haydara, T. 13 cis retinoic acid improved the outcomes of COVID-19 patients. A randomized clinical trial. medRxiv 2022, 2022-03.22271959. [Google Scholar] [CrossRef]
- Nguyen, T.P.; Patel, Z.M. Budesonide irrigation with olfactory training improves outcomes compared with olfactory training alone in patients with olfactory loss. Int. Forum Allergy Rhinol. 2018, 8, 977–981. [Google Scholar] [CrossRef] [PubMed]
- Clayton, P.; Hill, M.; Bogoda, N.; Subah, S.; Venkatesh, R. Palmitoylethanolamide: A Natural Compound for Health Management. Int. J. Mol. Sci. 2021, 22, 5305. [Google Scholar] [CrossRef]
- Costa, B.; Comelli, F.; Bettoni, I.; Colleoni, M.; Giagnoni, G. The endogenous fatty acid amide, palmitoylethanolamide, has anti-allodynic and anti-hyperalgesic effects in a murine model of neuropathic pain: Involvement of CB1, TRPV1 and PPARγ receptors and neurotrophic factors. Pain 2008, 139, 541–550. [Google Scholar] [CrossRef] [PubMed]
- Cordaro, M.; Cuzzocrea, S.; Crupi, R. An Update of Palmitoylethanolamide and Luteolin Effects in Preclinical and Clinical Studies of Neuroinflammatory Events. Antioxidants 2020, 9, 216. [Google Scholar] [CrossRef] [PubMed]
- Rankin, L.; Fowler, C.J. The basal pharmacology of palmitoylethanolamide. Int. J. Mol. Sci. 2020, 21, 7942. [Google Scholar] [CrossRef] [PubMed]
- Jaggar, S.I.; Hasnie, F.S.; Sellaturay, S.; Rice, A.S. The anti-hyperalgesic actions of the cannabinoid anandamide and the putative CB2 receptor agonist palmitoylethanolamide in visceral and somatic inflammatory pain. Pain 1998, 76, 189–199. [Google Scholar] [CrossRef]
- Verme, J.L.; Fu, J.; Astarita, G.; La Rana, G.; Russo, R.; Calignano, A.; Piomelli, D. The nuclear receptor peroxisome proliferator-activated receptor-α mediates the anti-inflammatory actions of palmitoylethanolamide. Mol. Pharmacol. 2005, 67, 15–19. [Google Scholar] [CrossRef]
- Chalamaiah, M.; Yu, W.; Wu, J. Immunomodulatory and anticancer protein hydrolysates (peptides) from food proteins: A review. Food Chem. 2017, 245, 205–222. [Google Scholar] [CrossRef] [PubMed]
- Solorzano, C.; Zhu, C.; Battista, N.; Astarita, G.; Lodola, A.; Rivara, S.; Mor, M.; Russo, R.; Maccarrone, M.; Antonietti, F.; et al. Selective N-acylethanolamine-hydrolyzing acid amidase inhibition reveals a key role for endogenous palmitoylethanolamide in inflammation. Proc. Natl. Acad. Sci. USA 2009, 106, 20966–20971. [Google Scholar] [CrossRef]
- Paterniti, I.; Cordaro, M.; Campolo, M.; Siracusa, R.; Cornelius, C.; Navarra, M.; Cuzzocrea, S.; Esposito, E. Neuroprotection by Association of Palmitoylethanolamide with Luteolin in Experimental Alzheimer’s Disease Models: The Control of Neuroinflammation. CNS Neurol. Disord. Drug Targets 2014, 13, 1530–1541. [Google Scholar] [CrossRef]
- Brotini, S.; Schievano, C.; Guidi, L. Ultra-Micronized Palmitoylethanolamide: An Efficacious Adjuvant Therapy for Parkinson’s Disease. CNS Neurol. Disord. Drug Targets 2017, 16, 705–713. [Google Scholar] [CrossRef]
- Assogna, M.; Casula, E.P.; Borghi, I.; Bonnì, S.; Samà, D.; Motta, C.; Di Lorenzo, F.; D’acunto, A.; Porrazzini, F.; Minei, M.; et al. Effects of Palmitoylethanolamide Combined with Luteoline on Frontal Lobe Functions, High Frequency Oscillations, and GABAergic Transmission in Patients with Frontotemporal Dementia. J. Alzheimer’s Dis. 2020, 76, 1297–1308. [Google Scholar] [CrossRef]
- Campolo, M.; Crupi, R.; Cordaro, M.; Cardali, S.M.; Ardizzone, A.; Casili, G.; Scuderi, S.A.; Siracusa, R.; Esposito, E.; Conti, A.; et al. Co-Ultra PEALut Enhances Endogenous Repair Response Following Moderate Traumatic Brain Injury. Int. J. Mol. Sci. 2021, 22, 8717. [Google Scholar] [CrossRef]
- Beggiato, S.; Tomasini, M.C.; Cassano, T.; Ferraro, L. Chronic Oral Palmitoylethanolamide Administration Rescues Cognitive Deficit and Reduces Neuroinflammation, Oxidative Stress, and Glutamate Levels in A Transgenic Murine Model of Alzheimer’s Disease. J. Clin. Med. 2020, 9, 428. [Google Scholar] [CrossRef]
- Imran, M.; Rauf, A.; Abu-Izneid, T.; Nadeem, M.; Shariati, M.A.; Khan, I.A.; Imran, A.; Orhan, I.E.; Rizwan, M.; Atif, M.; et al. Luteolin, a flavonoid, as an anticancer agent: A review. Biomed. Pharmacother. 2019, 112, 108612. [Google Scholar] [CrossRef]
- Formichi, P.; Radi, E.; Battisti, C.; Di Maio, G.; Dotti, M.T.; Muresanu, D.; Federico, A. Effects of cerebrolysin administration on oxidative stress-induced apoptosis in lymphocytes from CADASIL patients. Neurol. Sci. 2013, 34, 553–556. [Google Scholar] [CrossRef] [PubMed]
- Alzoubi, K.; Al-Ibbini, A.M.; Nuseir, K.Q. Prevention of memory impairment induced by post-traumatic stress disorder by cerebrolysin. Psychiatry Res. 2018, 270, 430–437. [Google Scholar] [CrossRef]
- Alsulaimani, R.A.; Quinn, T.J. The efficacy and safety of animal-derived nootropics in cognitive disorders: Systematic review and meta-analysis. Cereb. Circ. Cogn. Behav. 2021, 2, 100012, Erratum in Cereb Circ. Cogn. Behav. 2022, 3, 100038. [Google Scholar] [CrossRef] [PubMed]
- Lu, W.; Zhu, Z.; Shi, D.; Li, X.; Luo, J.; Liao, X. Cerebrolysin alleviates early brain injury after traumatic brain injury by inhibiting neuroinflammation and apoptosis via TLR signaling pathway. Acta Cir. Bras. 2022, 37, e370605. [Google Scholar] [CrossRef] [PubMed]
- Schriever, V.; Merkonidis, C.; Gupta, N.; Hummel, C.; Hummel, T. Treatment of smell loss with systemic methylprednisolone. Rhinology 2012, 50, 284–289. [Google Scholar] [CrossRef]
- Elkazzaz, M.; Haydara, T.; Abo-Amer, Y.E.-E.; Shamkh, I.M.; Abo El Magd, M.F.; Ahmed, A. TRA6 (Vitamin A Receptor), as a Novel Binding Receptor of COVID-19 (A Breakthrough). Research Square (preprint). 2021. Available online: https://doi.org/10.21203/rs.3.rs-892203/v3 (accessed on 25 February 2023).
- Khare, P.; Sahu, U.; Pandey, S.C.; Samant, M. Current approaches for target-specific drug discovery using natural compounds against SARS-CoV-2 infection. Virus Res. 2020, 290, 198169. [Google Scholar] [CrossRef]
- Fornazieri, M.A.; Garcia, E.C.D.; Lopes, N.M.D.; Miyazawa, I.N.I.; Silva, G.D.S.; Monteiro, R.D.S.; Pinna, F.D.R.; Voegels, R.; Doty, R.L. Adherence and Efficacy of Olfactory Training as a Treatment for Persistent Olfactory Loss. Am. J. Rhinol. Allergy 2019, 34, 238–248. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, A.K.; Landis, B.; Altundag, A.; Fjaeldstad, A.W.; Gane, S.; Holbrook, E.H.; Huart, C.; Konstantinidis, I.; Lechner, M.; Macchi, A.; et al. Olfactory Nomenclature: An Orchestrated Effort to Clarify Terms and Definitions of Dysosmia, Anosmia, Hyposmia, Normosmia, Hyperosmia, Olfactory Intolerance, Parosmia, and Phantosmia/Olfactory Hallucination. ORL J Otorhinolaryngol. Relat. Spec. 2023, 14, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.J.; Yu, A.C.; Lee, J.T. Management of post-COVID-19 olfactory dysfunction. Curr. Treat. Options Allergy 2022, 9, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Kurtenbach, S.; Goss, G.; Goncalves, S.; Choi, R.; Hare, J.M.; Chaudhari, N.; Goldstein, B.J. Cell-Based Therapy Restores Olfactory Function in an Inducible Model of Hyposmia. Stem Cell Rep. 2019, 12, 1354–1365. [Google Scholar] [CrossRef]
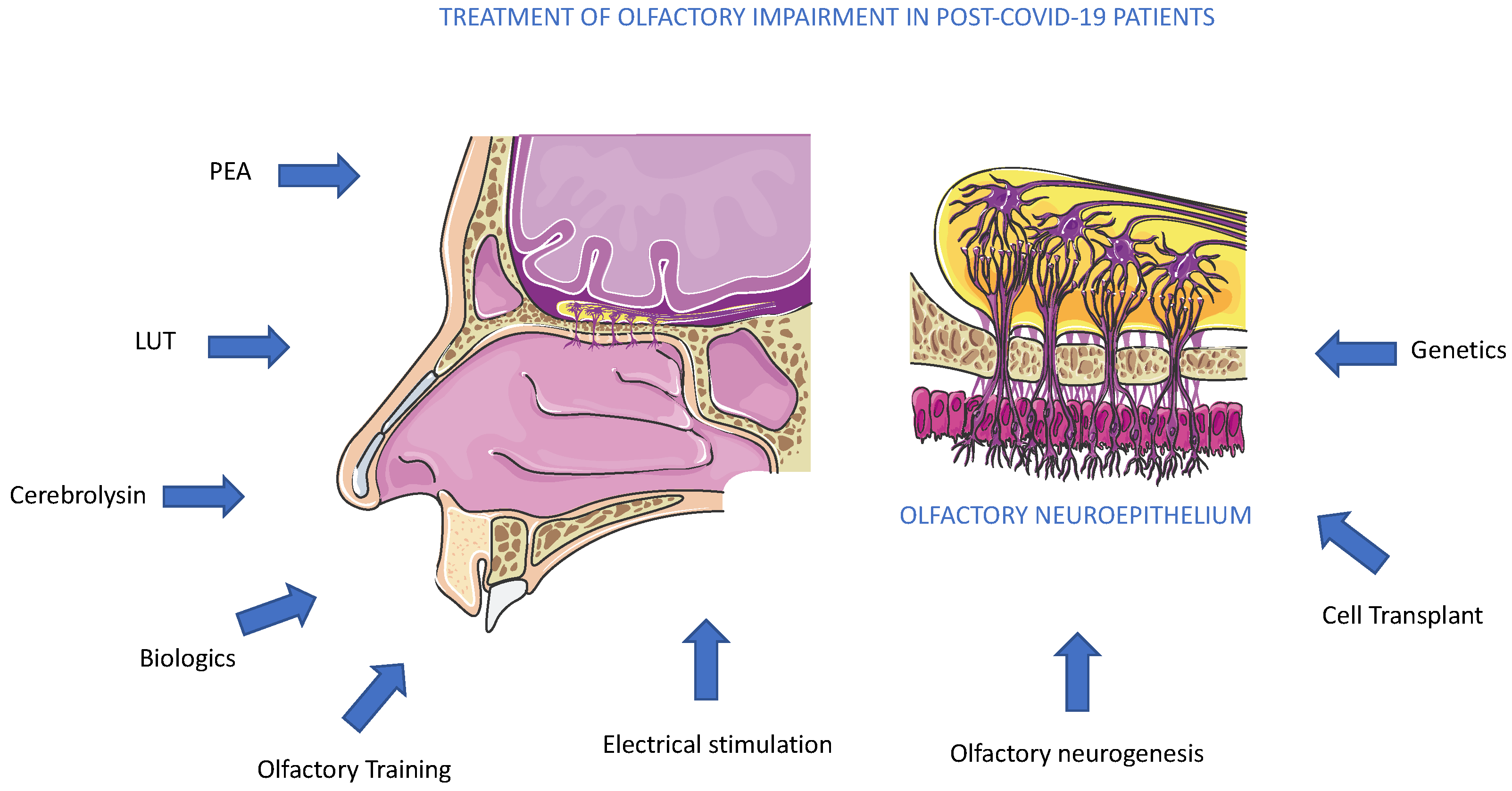
- Saussez, S.; Vaira, L.A.; De Riu, G.; Lechien, J.R. Therapies for COVID-19-Related Persistent Olfactory Disorders: One of the Good Fruits of the Pandemic. Pathogens 2023, 12, 72. [Google Scholar] [CrossRef] [PubMed]
- Barbato, C.; Di Certo, M.G.; Gabanella, F.; Petrella, C.; Fiore, M.; Passananti, C.; Colizza, A.; Cavalcanti, L.; Ralli, M.; Greco, A.; et al. Staying tuned for post-COVID-19 syndrome: Looking for new research to sniff out. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 5318–5321. [Google Scholar] [CrossRef] [PubMed]
- Mullol, J.; Bachert, C.; Amin, N.; Desrosiers, M.; Hellings, P.W.; Han, J.K.; Jankowski, R.; Vodicka, J.; Gevaert, P.; Daizadeh, N.; et al. Olfactory outcomes with dupilumab in chronic rhinosinusitis with nasal polyps. J. Allergy Clin. Immunol Pract. 2022, 10, 1086–1095.e5. [Google Scholar] [CrossRef]
- von Bartheld, C.S.; Wang, L. Prevalence of Olfactory Dysfunction with the Omicron Variant of SARS-CoV-2: A Systematic Review and Meta-Analysis. Cells 2023, 12, 430. [Google Scholar] [CrossRef] [PubMed]
- Leng, A.; Shah, M.; Ahmad, S.A.; Premraj, L.; Wildi, K.; Bassi, G.L.; Pardo, C.A.; Choi, A.; Cho, S.-M. Pathogenesis Underlying Neurological Manifestations of Long COVID Syndrome and Potential Therapeutics. Cells 2023, 12, 816. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Title | Intervention/Drug | Phase | Location | Age | Intervention Model and Allocation | Masking |
|---|---|---|---|---|---|---|
| Investigating the Potential Role of Aerosolized Retinoic Acid, a Potent Vitamin A Metabolite, for Treating COVID-19 Anosmia and Retinoic Acid Insufficiency. A Novel Approach for Regaining Sense of Smell. (NCT05002530) [14]. | Aerosolized 13-cis retinoic acid plus Vitamin D/Aerosolized All trans-retinoic acid plus Vitamin D | Phase 4 | Quan Liu Foshan, Guangdong, China Tamer Haydara Kafr Ash Shaykh, Kafr Elshiekh, Egypt Ministry of Health, Saudi Arabia. | 18 years to 70 years | Parallel Assignment Randomized | None (Open Label) |
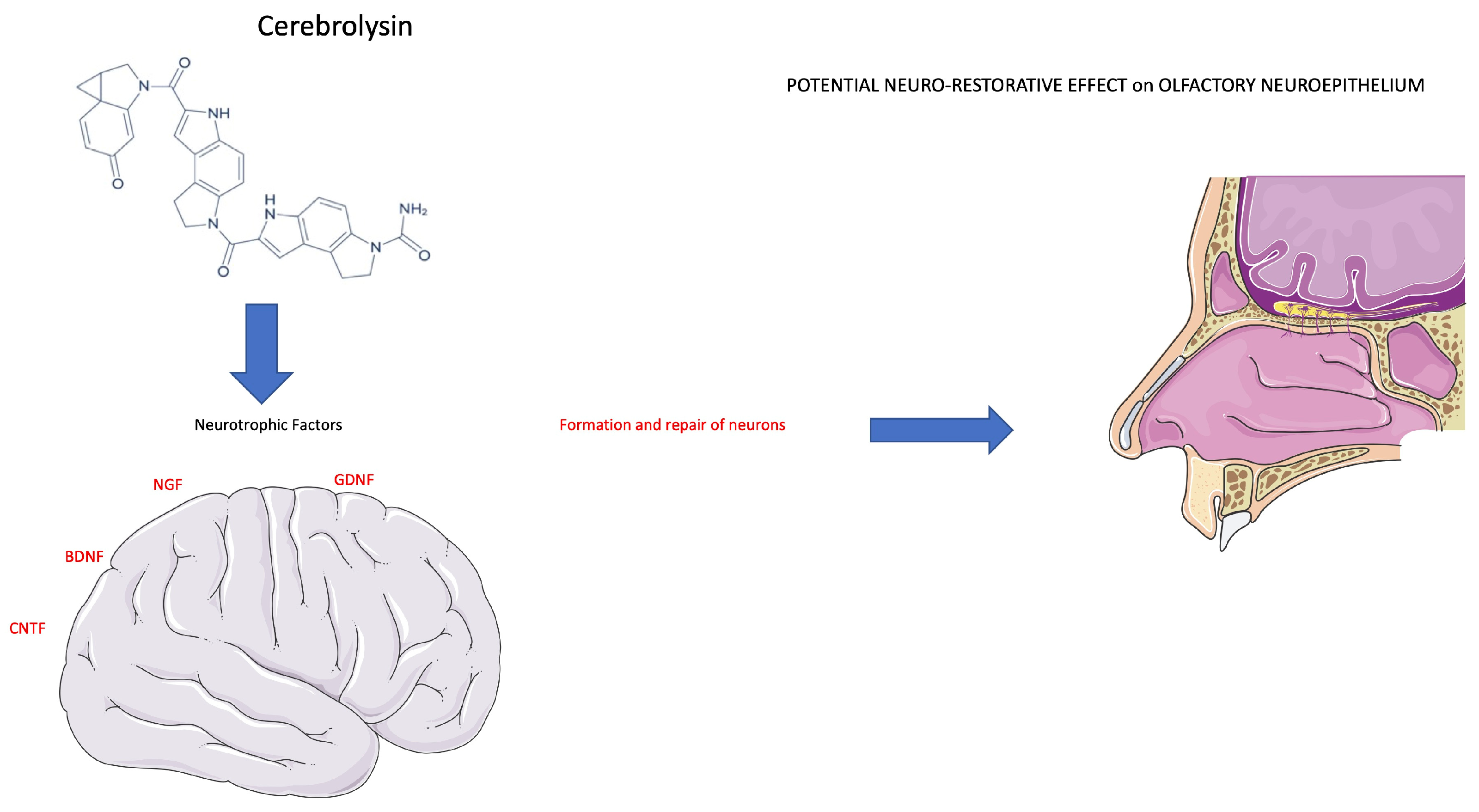
| Cerebrolysin for Treatment of COVID-related Anosmia and Ageusia NCT04830943 [15]. | Cerebrolysin | Phase 4 | Assiut University Hospitals, Faculty of Medicine Assiut, Egypt | 20 years to 50 years | Parallel Assignment Randomized | None (Open Label) |
| COVID-19 Anosmia Study NCT04495816 [13]. | Omega-3 Fatty Acid Supplement | Phase 2 | Mount Sinai Hospital New York, New York, United States | 18 years and older | Parallel Assignment Randomized | Double (Participant, Investigator) |
| Corticosteroid Nasal Spray in COVID-19 Anosmia NCT04484493 [16]. | Mometasone furoate nasal spray | Phase 3 | Benha University Hospital, Faculty of Medicine Banhā, Qalubia, Egypt | 18 years and older | Parallel Assignment Randomized | None (Open Label) |
| Stellate Ganglion Block for COVID-19-Induced Olfactory Dysfunction NCT05445921 [17]. | Stellate Ganglion Block | Phase 1 Phase 2 | Washington University School of Medicine/Barnes Jewish Hospital Saint Louis, Missouri, United States | 18 years to 70 years | Single Group Assignment | None (Open Label) |
| Role of Ivermectin Nanosuspension as Nasal Spray in Treatment of Persistent Post COVID19 Anosmia NCT04951362 [18]. | Intranasal spray ivermectin | Phase 2 Phase 3 | Zaky Aref Qina, Egypt | 18 years to 70 years | Parallel Assignment Randomized | None (Open Label) |
| Efficacy of Gabapentin for Post-COVID-19 Olfactory Dysfunction NCT05184192 [19,20]. | Gabapentin gelatine capsules 300 mg | Phase 2 | Washington University Saint Louis, Missouri, United States | 18 years to 65 years | Parallel Assignment Randomized | Triple (Participant, Investigator, Outcomes Assessor) |
| Smell in COVID-19 and Efficacy of Nasal Theophylline NCT04789499 [19]. | Theophylline Powder | Phase 2 | Washington University School of Medicine in Saint Louis Saint Louis, Missouri, United States | 18 years to 70 years | Parallel Assignment Randomized | Double (Participant, Investigator) |
| Intranasal Insulin for COVID-19-related Smell Loss NCT05461365 [21]. | Insulin | Phase 3 | Universidad Panamerican Mexico City, Mexico | 18 years to 59 years | Single Assignment | None (Open Label) |
| Anosmia and/or Ageusia and Early Corticosteroid Use NCT04528329 [22]. | Early Dexamethasone/Late dexamethasone | Phase 4 | Asalam Maadi, Cairo, Egypt | 18 years and older | Parallel Assignment Randomized | None (Open Label) |
| Study of Hesperidin Therapy on COVID-19 Symptoms (HESPERIDIN) NCT04715932 [23]. | Hesperidin | Phase 2 | Montreal Heart Institute Montréal, Quebec, Canada | 18 years and older | Parallel Assignment Randomized | Quadruple (Participant, Care Provider, Investigator, Outcomes Assessor) |
| Effect of Nasal Steroid in the Treatment of Anosmia Due to COVID-19 Disease NCT04569825 [24]. | Ophtamesone | Phase 1 | Raid Muhmid Al-Ani Ramadi, Anbar, Iraq | 18 years and older | Parallel Assignment Randomized | Double (Participant, Investigator) |
| Effectiveness and Safety of Platelet Rich Plasma (PRP) on Persistent Olfactory Dysfunction Related to COVID-19 NCT05226546 [25]. | Platelet-rich plasma (PRP) | Phase 2 Phase 3 | CHU Saint Pierre Bruxelles, Belgium | 18 years and older | Parallel Assignment Non-Randomized | None (Open Label) |
| BNO 1030 Extract (Imupret) in the Treatment of Mild Forms of COVID-19 NCT04797936 [26]. | BNO 1030 | Phase 4 | Ivano-Frankivsk National Medical University Ivano-Frankivsk, Ukraine | 18 years to 70 years | Parallel Assignment Randomized | None (Open Label) |
| Olfactory Disfunction and Co-ultraPEALut NCT04853836 [16]. | PEA-LUT | Phase 4 | Multicentric Roma, Italy | 18 years to 85 years | Parallel Assignment Randomized | Double (Investigator, Outcomes Assessor) |
| Anosmia Rehabilitation in Patients Post Coronavirus Disease (COVID-19) NCT04374474 Withdrawn (Study withdrawn before any enrollment (site’s research goals adjustments) | Corticosteroid nasal irrigation | Phase 4 | St. Joseph’s Health Care London, Ontario, Canada | 18 years and older | Parallel Assignment Randomized | None (Open Label) |
| Olfactory and Neurosensory Rehabilitation in COVID-19-related Olfactory Dysfunction NCT04900415 [27] | Vitamin A | Phase 2 | Pamela Youde Nethersole Eastern Hospital Hong Kong, The University of Hong Kong, Queen Mary Hospital, Hong Kong | 18 years and older | Parallel Assignment Randomized | Double (Investigator, Outcomes Assessor) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Riccardi, G.; Niccolini, G.F.; Bellizzi, M.G.; Fiore, M.; Minni, A.; Barbato, C. Post-COVID-19 Anosmia and Therapies: Stay Tuned for New Drugs to Sniff Out. Diseases 2023, 11, 79. https://doi.org/10.3390/diseases11020079
Riccardi G, Niccolini GF, Bellizzi MG, Fiore M, Minni A, Barbato C. Post-COVID-19 Anosmia and Therapies: Stay Tuned for New Drugs to Sniff Out. Diseases. 2023; 11(2):79. https://doi.org/10.3390/diseases11020079
Chicago/Turabian StyleRiccardi, Gabriele, Giovanni Francesco Niccolini, Mario Giuseppe Bellizzi, Marco Fiore, Antonio Minni, and Christian Barbato. 2023. "Post-COVID-19 Anosmia and Therapies: Stay Tuned for New Drugs to Sniff Out" Diseases 11, no. 2: 79. https://doi.org/10.3390/diseases11020079
APA StyleRiccardi, G., Niccolini, G. F., Bellizzi, M. G., Fiore, M., Minni, A., & Barbato, C. (2023). Post-COVID-19 Anosmia and Therapies: Stay Tuned for New Drugs to Sniff Out. Diseases, 11(2), 79. https://doi.org/10.3390/diseases11020079