
Reproductive Health Practices in Spanish Women Who Underwent Voluntary Termination of Pregnancy



Abstract
1. Introduction
2. Methods
2.1. Study Design and Setting
2.2. Study Subjects, Inclusion and Exclusion Criteria
2.3. Study Instruments
2.4. Data Analysis
2.5. Ethics Statement
3. Results
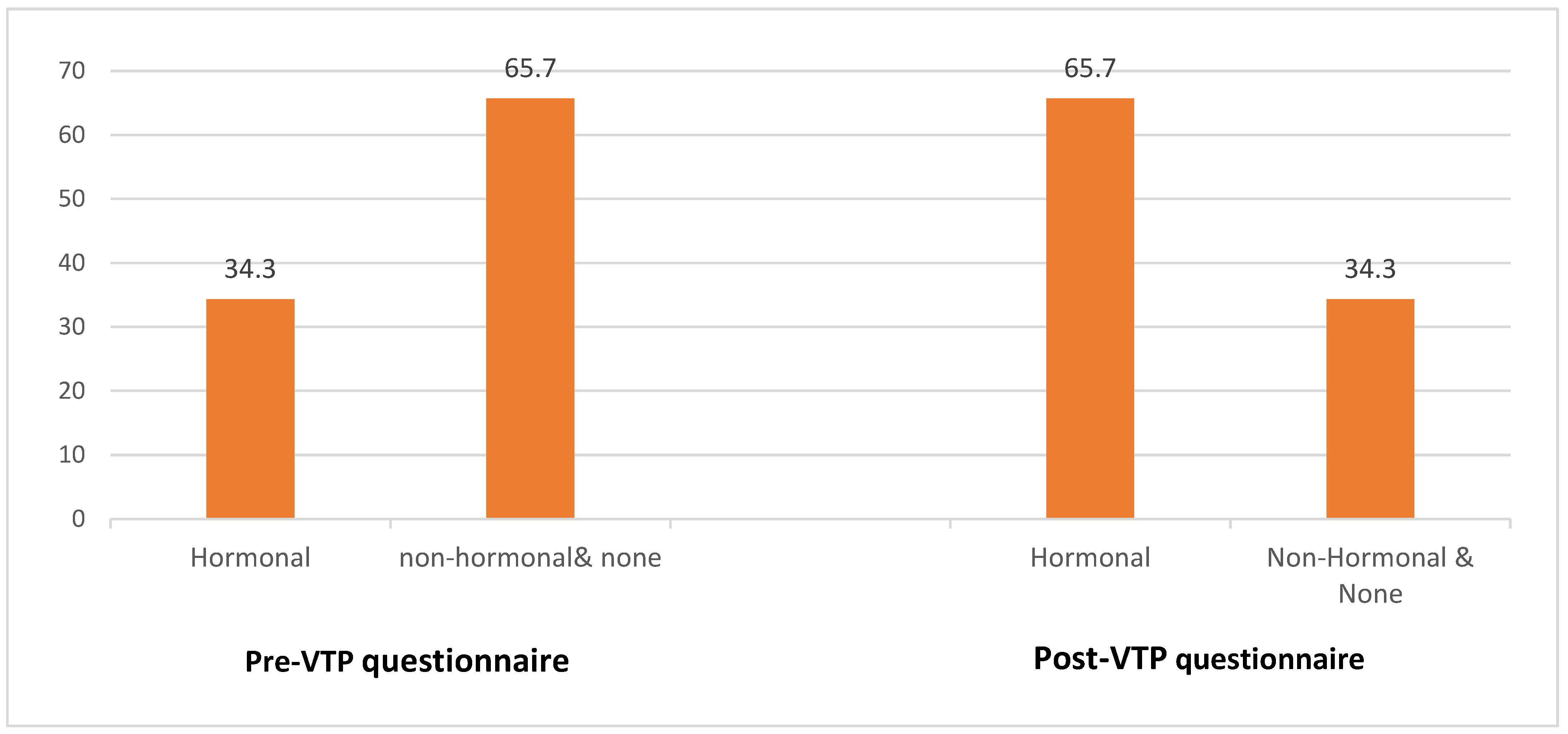
3.1. Pre-VTP Questionnaire
3.2. Post-VTP Questionnaire
4. Discussion
4.1. Strengths and Limitations
4.2. Clinical Implication
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cara Rodriguez, M.; Garcia Senso, S.; Rodriguez Arenas, M.A. Factors related to the voluntary interruption of pregnancy in Spain. J. Prev. Med. Hyg. 2022, 63, E69–E75. [Google Scholar] [CrossRef]
- Llorente-Marrón, M.; Díaz-Fernández, M.; Méndez-Rodríguez, P. Contextual determinants of induced abortion: A panel analysis. Rev. Saúde Pública 2016, 50, 8. [Google Scholar] [CrossRef] [PubMed]
- Perez, G.; Ruiz-Munoz, D.; Gotsens, M.; Cases, M.C.; Rodriguez-Sanz, M. Social and economic inequalities in induced abortion in Spain as a function of individual and contextual factors. Eur. J. Public Health 2014, 24, 162–169. [Google Scholar] [CrossRef]
- De España, J.C.I.R. Ley Orgánica 2/2010, de 3 de Marzo, de Salud Sexual y Reproductiva y de la Interrupción Voluntaria del Embarazo; Boletín Oficial del Estado: Madrid, Spain, 2010. [Google Scholar]
- De España, J.C.I.R. Ley Orgánica 9/1985, de 5 de Julio, de Reforma del Artículo 417 bis del Código Penal; Boletín Oficial del Estado: Madrid, Spain, 1985; Available online: https://www.boe.es/boe/dias/1985/07/12/pdfs/A22041-22041.pdf (accessed on 8 March 2021).
- Vila-Vives, J.M.; Soler-Ferrero, I.; Gimeno-Clemente, N.; Hidalgo-Mora, J.J.; Vila-Martínez, J.M.; Pellicer, A. Perfil de la paciente que solicita una interrupción voluntaria del embarazo. Gac. Sanit. 2013, 27, 565–566. [Google Scholar] [CrossRef] [PubMed]
- Serrano, I.; Doval, J.L.; Lete, I.; Arbat, A.; Coll, C.; Martínez-Salmeán, J.; Pérez-Campos, E.; Dueñas, J.L. Contraceptive practices of women requesting induced abortion in Spain: A cross-sectional multicentre study. Eur. J. Contracept. Reprod. Health Care 2012, 17, 205–211. [Google Scholar] [CrossRef]
- Laanpere, M.; Ringmets, I.; Part, K.; Allvee, K.; Veerus, P.; Karro, H. Abortion trends from 1996 to 2011 in Estonia: Special emphasis on repeat abortion. BMC Women’s Health 2014, 14, 81. [Google Scholar] [CrossRef]
- Zurriaga, O.; Martínez-Beneito, M.A.; Galmés Truyols, A.; Torne, M.M.; Bosch, S.; Bosser, R.; Arbona, M.P. Recourse to induced abortion in Spain: Profiling of users and the influence of migrant populations. Gac. Sanit. 2009, 23, 57–63. [Google Scholar] [CrossRef]
- Font-Ribera, L.; Pérez, G.; Salvador, J.; Borrell, C. Socioeconomic Inequalities in Unintended Pregnancy and Abortion Decision. J. Urban Health 2008, 85, 125–135. [Google Scholar] [CrossRef]
- Rasch, V.; Gammeltoft, T.; Knudsen, L.B.; Tobiassen, C.; Ginzel, A.; Kempf, L. Induced abortion in Denmark: Effect of socio-economic situation and country of birth. Eur. J. Public Health 2007, 18, 144–149. [Google Scholar] [CrossRef]
- Ruiz-Ramos, M.; Ivañez-Gimeno, L.; García León, F.J. Características sociodemográficas de la interrupción voluntaria del embarazo en Andalucía: Diferencias entre población autóctona y extranjera. Gac. Sanit. 2012, 26, 504–511. [Google Scholar] [CrossRef]
- Dueñas, J.L.; Lete, I.; Bermejo, R.; Arbat, A.; Pérez-Campos, E.; Martínez-Salmeán, J.; Serrano, I.; Doval, J.L.; Coll, C. Trends in the use of contraceptive methods and voluntary interruption of pregnancy in the Spanish population during 1997–2007. Contraception 2011, 83, 82–87. [Google Scholar] [CrossRef]
- Aneblom, G.; Larsson, M.; Odlind, V.; Tyden, T. Knowledge, use and attitudes towards emergency contraceptive pills among swedish women presenting for induced abortion. BJOG Intern. J. Obs. Gyn. 2002, 109, 155–160. [Google Scholar] [CrossRef]
- Pereira, J.; Pires, R.; Araújo Pedrosa, A.; Vicente, L.; Bombas, T.; Canavarro, M.C. Sociodemographic, sexual, reproductive and relationship characteristics of adolescents having an abortion in Portugal: A homogeneous or a heterogeneous group? Eur. J. Contracept. Reprod. Health Care 2017, 22, 53–61. [Google Scholar] [CrossRef]
- Moreau, C.; Trussell, J.; Bajos, N. Contraceptive Paths of Adolescent Women Undergoing an Abortion in France. J. Adolesc. Health 2012, 50, 389–394. [Google Scholar] [CrossRef]
- Sociedad Española de Contracepción (SEC). Estudio Sobre Sexualidad y Anticoncepción: Jóvenes Españoles. 2019. Available online: http://hosting.sec.es/descargas/Encuesta2019_SEXUALIDAD_ANTICONCEPCION_JOVENES.pdf (accessed on 17 November 2020).
- Lazdane, G. Mejorar la salud familiar y comunitaria a través del fortalecimiento de los sistemas de salud. Entre Nous 2009, 68, 6–7. [Google Scholar]
- Calatrava, M.; López-Del Burgo, C.; de Irala, J. Factores de riesgo relacionados con la salud sexual en los jóvenes europeos. Med. Clínica 2012, 138, 534–540. [Google Scholar] [CrossRef]
- Scott, M.E.; Wildsmith, E.; Welti, K.; Ryan, S.; Schelar, E.; Steward-Streng, N.R. Risky Adolescent Sexual Behaviors and Reproductive Health in Young Adulthood. Perspect. Sex. Reprod. Health 2011, 43, 110–118. [Google Scholar] [CrossRef]
- Sociedad Española de Contracepción (SEC). Encuesta de Anticoncepción en España, 2018. (Hábitos de la Población Femenina en Relación al Uso de los Métodos Anticonceptivos). 2018. Available online: http://hosting.sec.es/descargas/encuesta2018.pdf (accessed on 17 November 2020).
- Lapresa Alcalde, M.V. Perfil Epidemiológico y Prácticas en Salud Reproductiva de la Interrupción Voluntaria de Embarazo en Salamanca. Ph.D. Thesis, Universidad de Salamanca, Salamanca, Spain, 2021. [Google Scholar]
- Morillo García, Á.; Aldana Espinal, J.M.; Moreno Nieto, J.; Sillero Sánchez, R.; Nieto Cervera, P. Experiencia de mujeres que solicitan interrupción voluntaria del embarazo: Relación con el entorno sanitario. Atención Primaria 2007, 39, 313–318. [Google Scholar] [CrossRef]
- Biggs, M.A.; Upadhyay, U.D.; McCulloch, C.E.; Foster, D.G. Women’s Mental Health and Well-being 5 Years after Receiving or Being Denied an Abortion: A Prospective, Longitudinal Cohort Study. JAMA Psychiatry 2017, 74, 169. [Google Scholar] [CrossRef]
- Munk-Olsen, T.; Laursen, T.M.; Pedersen, C.B.; Lidegaard, Ø.; Mortensen, P.B. Induced First-Trimester Abortion and Risk of Mental Disorder. N. Engl. J. Med. 2011, 364, 332–339. [Google Scholar] [CrossRef]
- Harris, L.F.; Roberts, S.C.; Biggs, M.A.; Rocca, C.H.; Foster, D.G. Perceived stress and emotional social support among women who are denied or receive abortions in the United States: A prospective cohort study. BMC Women’s Health 2014, 14, 76. [Google Scholar] [CrossRef] [PubMed]
- Kumar, U.; Pollard, L.; Campbell, L.; Yurdakul, S.; Calvete, C.C.; Coker, B.; Chen, T.; Douiri, A. Specialist follow-up contraceptive support after abortion—Impact on effective contraceptive use at six months and subsequent abortions: A randomised controlled trial. PLoS ONE 2019, 14, e0217902. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Categories | TOTAL (176) |
|---|---|---|
| Frec. (%) | ||
| Age | 15–19 years | 28 (15′9) |
| 20–25 years | 63 (35′7) | |
| 26–30 years | 39 (22′2) | |
| >30 years | 45 (25′6) | |
| Missing | 1 (0′6) | |
| Educational level | Primary | 28 (15′9) |
| High school | 106 (60′2) | |
| University | 40 (22′8) | |
| Missing | 2 (1′1) | |
| Proffesion | Student | 54 (30′7) |
| Employee | 55 (31′3) | |
| Unemployed | 37 (21) | |
| Housewife | 20 (11′4) | |
| Self-employed | 8 (4′5) | |
| Missing | 6 (3′4) | |
| Address | Alone | 109 (61′9) |
| Couple | 53 (30′1) | |
| Parents | 7 (4) | |
| Missing | 7 (4) | |
| Monthly income | <736€ | 113 (64′2) |
| 737–1500€ | 56 (31′9) | |
| >1500€ | 5 (2′8) | |
| Missing | 2 (1′1) | |
| Birth country | Spain | 142 (80′7) |
| Other | 32 (18′2) | |
| Missing | 2 (1′1) | |
| Children | 0 | 81 (46) |
| 1 | 23 (13) | |
| 2 | 17 (9′7) | |
| 3 | 6 (3′4) | |
| 5 | 1 (0′6) | |
| Missing | 48 (27′3) |
| Variable | Categories | TOTAL (176) |
|---|---|---|
| CONTRACEPTION | Frec. (%) | |
| Contraceptives 1 | Condom | 79 (44′9) |
| Pill | 37 (21) | |
| Inj./IUD/Implant | 3 (1′7) | |
| Withdrawal | 9 (5′1) | |
| Ring/patch | 3 (1′7) | |
| None | 26 (14′8) | |
| Condom + withdrawl/none | 11 (6′3) | |
| Condom + pill | 7 (3′9) | |
| Missing | 1 (0′6) | |
| Reason for rejecting hormonal methods 1 | Secondary effects | 49 (27′8) |
| Difficulty of use | 4 (2′3) | |
| Low pregnancy possibility | 2 (1′1) | |
| Lack of information | 18 (10′2) | |
| Contraindicated | 8 (4′5) | |
| Missing | 95 (53′9) | |
| Contraceptive method information 1 | Friends | 16 (9′1) |
| Internet | 12 (6′8) | |
| Primary care physician | 43 (24′4) | |
| Midwife | 42 (23′9) | |
| Gynecologist | 41 (23′3) | |
| Other | 24 (13′6) | |
| Friends and internet | 10 (5′7) | |
| Missing | 8 (4′5) | |
| If they have no method of contraception 1 | Withdrawal | 65 (36′9) |
| Buy condom | 52 (29′5) | |
| Abstention | 31 (17′6) | |
| Emergency contraception | 20 (11′4) | |
| Confident that she will not become pregnant | 18 (10′2) | |
| Missing | 6 (3′4) | |
| Alcohol: less condom use | Yes | 27 (15′3) |
| No | 120 (68′2) | |
| Sometimes | 19 (10′8) | |
| Missing | 10 (5′7) | |
| REPRODUCTIVE HEALTH | ||
| First sexual intercourse | 10–13 years | 3 (1′7) |
| 14–17 years | 100 (56′8) | |
| >18 years | 59 (33′5) | |
| Missing | 14 (8) | |
| Number of sexual partners | Less than 2 | 42 (23′9) |
| 2 to 5 | 90 (51′1) | |
| More than 5 | 29 (16′5) | |
| Missing | 15 (8′5) | |
| Sexuality information | Yes | 136 (77′3) |
| No | 31 (17′6) | |
| Missing | 9 (5′1) | |
| Sufficient | 73 (41′5) | |
| Insufficient | 48 (27′3) | |
| Missing | 55 (31′2) | |
| Family environment | 13 (7′3) | |
| Academic setting | 64 (36′2) | |
| Both | 27 (15′2) | |
| Missing | 73 (41′3) | |
| Knowledge of LARCs | No | 107 (60′8) |
| A little | 36 (20′5) | |
| Yes, with correct/incorrect example | 16/3 (10′8) | |
| Missing | 14 (7′9) | |
| Option for her | 45 (25′6) | |
| Not for her | 16 (9′1) | |
| Missing | 115 (65′3) | |
| TERMINATION OF PREGNANCY | ||
| Cause of pregnancy | No method | 57 (32′4) |
| Misuse | 62 (35′2) | |
| Do not know | 41 (23′3) | |
| Missing | 16 (9′1) | |
| EC in this pregnancy | No | 144 (81′8) |
| Yes, first 24 h | 10 (5′7) | |
| Yes, >24 h | 7 (4) | |
| Missing | 15 (8′5) | |
| EC in other occasions | No | 91 (51′8) |
| Once | 49 (27′8) | |
| More than 1 | 21 (11′9) | |
| Missing | 15 (8′5) | |
| Cause of Interruption 1 | Too young | 58 (32′9) |
| Economy | 84 (47′7) | |
| Disrupts personal development | 44 (25) | |
| Family or partner pressures | 14 (7′9) | |
| Couple instability | 48 (27′3) | |
| More children | 10 (5′7) | |
| Unwilling/afraid | 6 (3′4) | |
| Lack of support | 1 (0′6) | |
| Mistreatment | 1 (0′6) | |
| Advanced age | 1 (0′6) | |
| Risky pregnancy | 7 (3′9) | |
| Missing | 18 (10′2) | |
| Previous interruptions | No | 123 (69′9) |
| Yes | 37 (21) | |
| Missing | 16 (9′1) | |
| 1 | 30 (17) | |
| 2 | 6 (3′4) | |
| >2 | 1 (0′6) | |
| Support 1 | No | 15 (8′5) |
| Yes | 146 (83) | |
| Missing | 15 (8′5) | |
| Partner | 94 (53′4) | |
| Family | 54 (30′7) | |
| Friend | 58 (32′9) | |
| Variable | Categories | TOTAL (80) |
|---|---|---|
| SATISFACTION WITH THE PROCESS | Frec. (%) | |
| Formalities | 1 = easy to execute | 35 (43′7) |
| 2 | 18 (22′5) | |
| 3 | 11 (13′8) | |
| 4 | 10 (12′5) | |
| 5 = too many | 6 (7′5) | |
| Missing | _ | |
| Travelling | I prefer it this way | 13 (16′3) |
| Not relevant | 22 (27′5) | |
| Effort that can be assumed | 31 (38′7) | |
| Major problems | 8 (10) | |
| Private preferred | 6 (7′5) | |
| Missing | _ | |
| Psychological impact | Nothing, forgotten | 19 (23′7) |
| Moderate | 40 (50) | |
| A before and after | 21 (26′3) | |
| Missing | ||
| Subsequent review | No, nobody informed me | 3 (3′8) |
| No, she cannot attend | 28 (35) | |
| Yes, with ultrasound | 47 (58′7) | |
| Missing | 2 (2′5) | |
| Change of contraceptive method | Yes, hormonal | 47 (58′7) |
| Yes, non-hormonal | 13 (16′3) | |
| Same, better use | 20 (25) | |
| Missing | _ | |
| Aspects to be improved | None | 44 (55) |
| Speeding up procedures | 4 (5) | |
| Accessibility | 11 (13′8) | |
| Improve treatment | 2 (2′5) | |
| Anaesthesia | 3 (3′8) | |
| Further information | 6 (7′5) | |
| Other | 2 (2′5) | |
| Missing | _ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lapresa-Alcalde, M.V.; Cubo, A.M.; Alonso-Sardón, M.; Doyague-Sánchez, M.J. Reproductive Health Practices in Spanish Women Who Underwent Voluntary Termination of Pregnancy. Diseases 2023, 11, 37. https://doi.org/10.3390/diseases11010037
Lapresa-Alcalde MV, Cubo AM, Alonso-Sardón M, Doyague-Sánchez MJ. Reproductive Health Practices in Spanish Women Who Underwent Voluntary Termination of Pregnancy. Diseases. 2023; 11(1):37. https://doi.org/10.3390/diseases11010037
Chicago/Turabian StyleLapresa-Alcalde, M. V., A. M. Cubo, M. Alonso-Sardón, and M. J. Doyague-Sánchez. 2023. "Reproductive Health Practices in Spanish Women Who Underwent Voluntary Termination of Pregnancy" Diseases 11, no. 1: 37. https://doi.org/10.3390/diseases11010037
APA StyleLapresa-Alcalde, M. V., Cubo, A. M., Alonso-Sardón, M., & Doyague-Sánchez, M. J. (2023). Reproductive Health Practices in Spanish Women Who Underwent Voluntary Termination of Pregnancy. Diseases, 11(1), 37. https://doi.org/10.3390/diseases11010037