

A New Smartphone-Based Method for Remote Health Monitoring: Assessment of Respiratory Kinematics

 , , ,
, , ,  , ,
, ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Validation
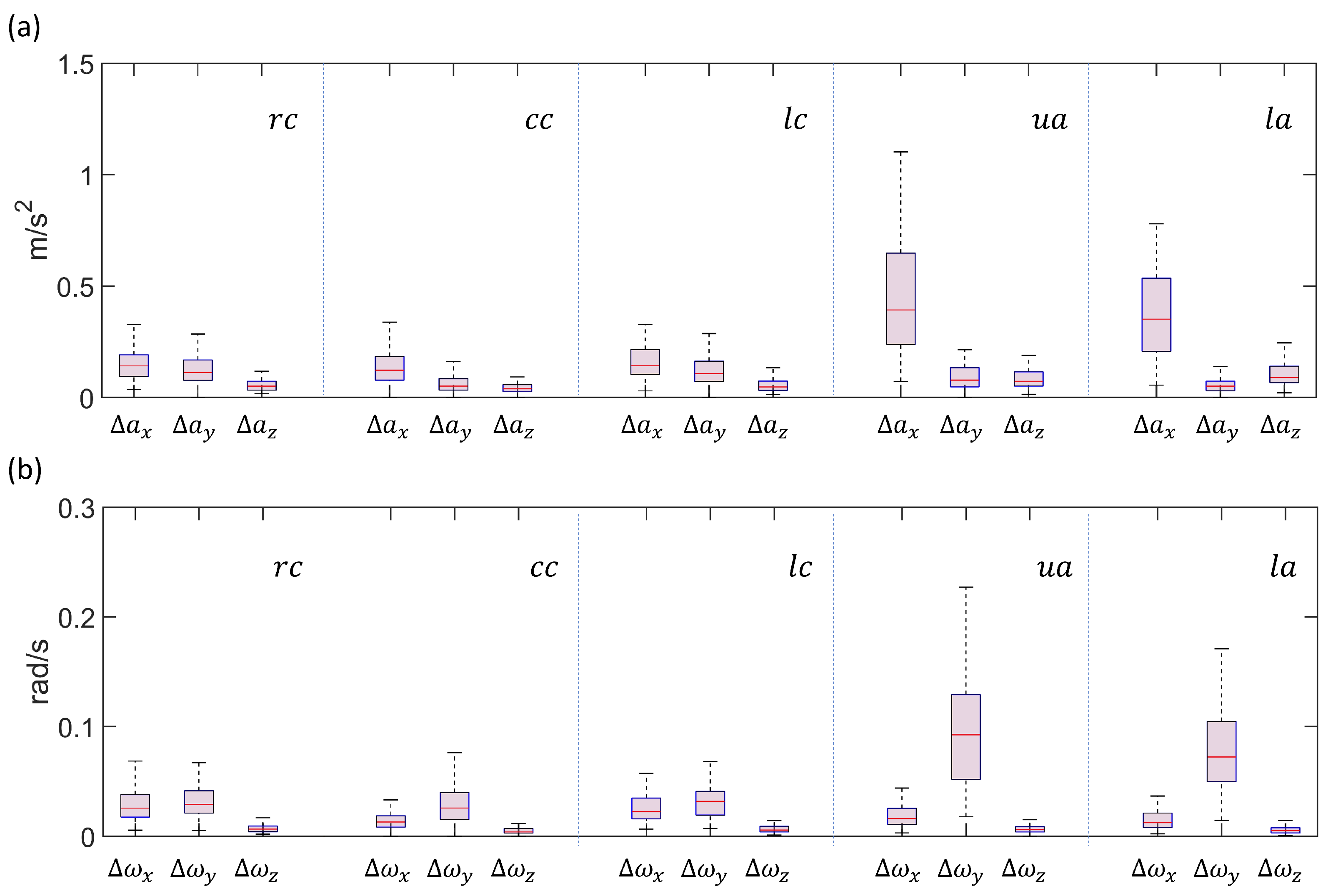
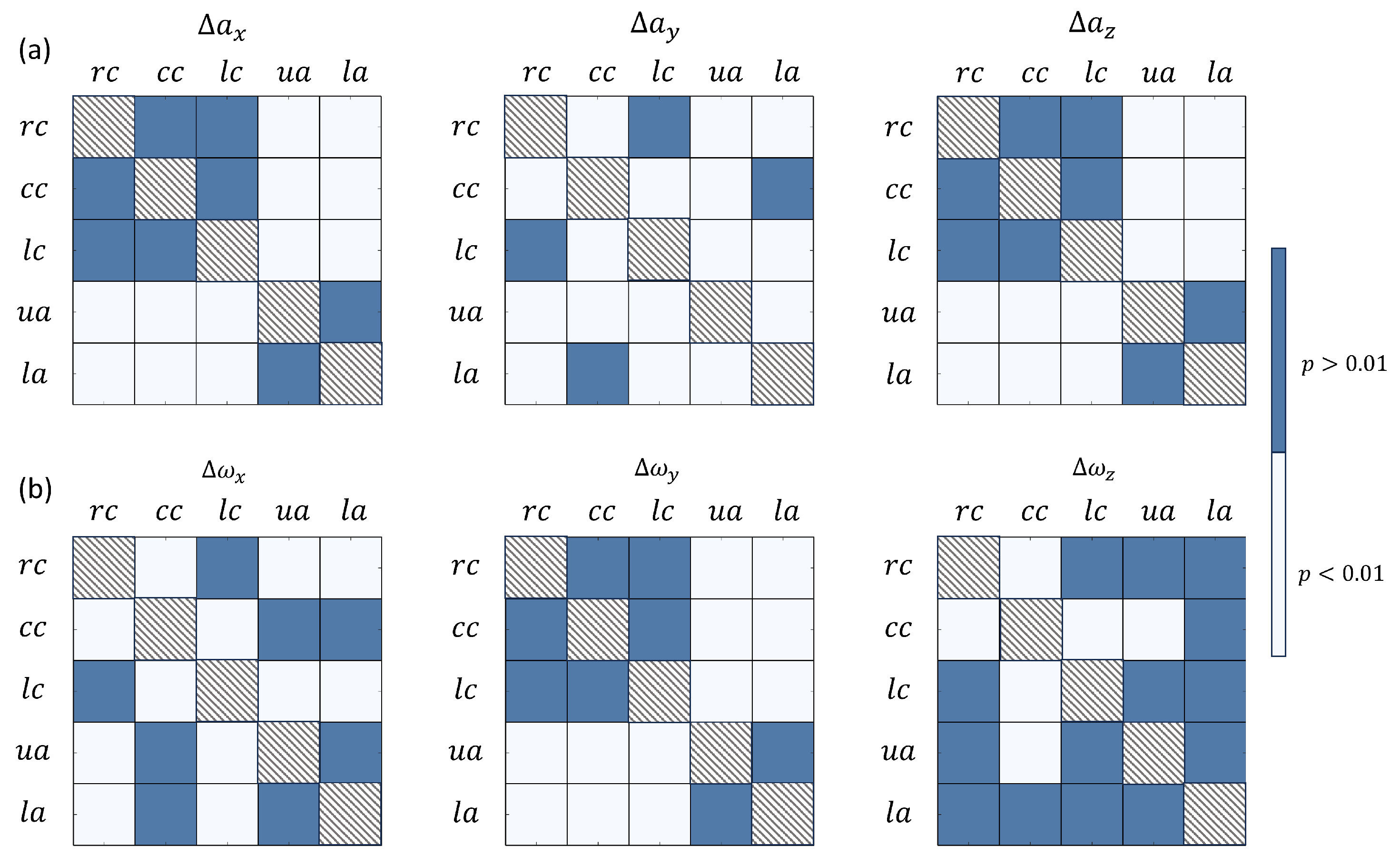
- Position 1—right side of chest ();
- Position 2—left side of chest ();
- Position 3—chest center ();
- Position 4—upper abdomen ();
- Position 5—lower abdomen ().
- The subject was asked to position supine on the bed and breathe normally;
- The operator, after ensuring the correct positioning of the volunteer subject, placed the smartphone designated for acquisition in one of the 10 defined configurations and started the recording;
- The subject was asked to hold breath for 2 s, in order to allow for zero-input reference registration, necessary for noise estimation;
- The subject was then asked to breathe normally for 20 s, at the end of which the recording was stopped;
- At this point, the operator can place the smartphone in the next position and repeat the previous steps, until the prescribed configurations are completed.

2.2. Application Development
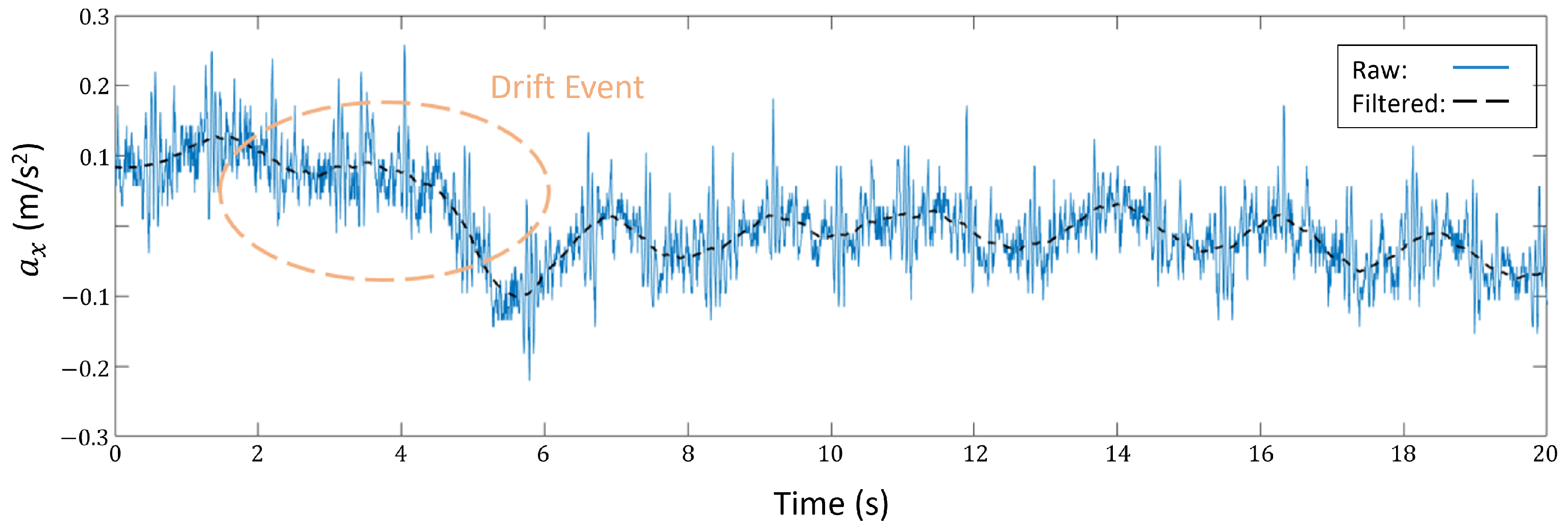
2.3. Signal Processing
2.4. Acquisition Campaign
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| accelerometer components | |
| apm | acts per minute |
| BLE | Bluetooth Low Energy |
| BMI | Body Mass Index |
| ECG | electrocardiogram |
| chest central | |
| IMU | inertial measurement unit |
| lower abdomen | |
| left chest | |
| right chest | |
| RR | respiratory rate |
| signal-to-noise ratio | |
| upper abdomen | |
| gyroscope components |
References
- Mohammed, K.; Zaidan, A.; Zaidan, B.; Albahri, O.S.; Alsalem, M.; Albahri, A.S.; Hadi, A.; Hashim, M. Real-time remote-health monitoring systems: A review on patients prioritisation for multiple-chronic diseases, taxonomy analysis, concerns and solution procedure. J. Med. Syst. 2019, 43, 223. [Google Scholar] [CrossRef] [PubMed]
- Dawes, A.; Lin, A.; Varghese, C.; Russell, M.; Lin, A. Mobile health technology for remote home monitoring after surgery: A meta-analysis. Br. J. Surg. 2021, 108, 1304–1314. [Google Scholar] [CrossRef] [PubMed]
- Shaji, S.; Pathinarupothi, R.K.; Rangan, E.S.; Menon, K.U.; Ramesh, M.V. Heart lung health monitor: Remote at-home patient surveillance for pandemic management. In Proceedings of the 2021 IEEE Global Humanitarian Technology Conference (GHTC), Seattle, WA, USA, 19–23 October 2021; pp. 127–130. [Google Scholar]
- Vedaei, S.S.; Fotovvat, A.; Mohebbian, M.R.; Rahman, G.M.; Wahid, K.A.; Babyn, P.; Marateb, H.R.; Mansourian, M.; Sami, R. COVID-SAFE: An IoT-based system for automated health monitoring and surveillance in post-pandemic life. IEEE Access 2020, 8, 188538–188551. [Google Scholar] [CrossRef] [PubMed]
- Magnocavallo, M.; Vetta, G.; Bernardini, A.; Piro, A.; Mei, M.C.; Di Iorio, M.; Mariani, M.V.; Della Rocca, D.G.; Severino, P.; Quaglione, R.; et al. Impact of COVID-19 pandemic on cardiac electronic device management and role of remote monitoring. Card. Electrophysiol. Clin. 2022, 14, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Strik, M.; Caillol, T.; Ramirez, F.D.; Abu-Alrub, S.; Marchand, H.; Welte, N.; Ritter, P.; Haïssaguerre, M.; Ploux, S.; Bordachar, P. Validating QT-interval measurement using the Apple Watch ECG to enable remote monitoring during the COVID-19 pandemic. Circulation 2020, 142, 416–418. [Google Scholar] [CrossRef] [PubMed]
- Alugubelli, N.; Abuissa, H.; Roka, A. Wearable Devices for Remote Monitoring of Heart Rate and Heart Rate Variability—What We Know and What Is Coming. Sensors 2022, 22, 8903. [Google Scholar] [CrossRef] [PubMed]
- Turakhia, M.P.; Desai, M.; Hedlin, H.; Rajmane, A.; Talati, N.; Ferris, T.; Desai, S.; Nag, D.; Patel, M.; Kowey, P.; et al. Rationale and design of a large-scale, app-based study to identify cardiac arrhythmias using a smartwatch: The Apple Heart Study. Am. Heart J. 2019, 207, 66–75. [Google Scholar] [CrossRef]
- Golinelli, D.; Boetto, E.; Carullo, G.; Nuzzolese, A.G.; Landini, M.P.; Fantini, M.P. Adoption of digital technologies in health care during the COVID-19 pandemic: Systematic review of early scientific literature. J. Med. Internet Res. 2020, 22, e22280. [Google Scholar] [CrossRef]
- Beduk, T.; Beduk, D.; Hasan, M.R.; Guler Celik, E.; Kosel, J.; Narang, J.; Salama, K.N.; Timur, S. Smartphone-based multiplexed biosensing tools for health monitoring. Biosensors 2022, 12, 583. [Google Scholar] [CrossRef]
- Alzughaibi, A.A.; Ibrahim, A.M.; Na, Y.; El-Tawil, S.; Eltawil, A.M. Community-Based Multi-Sensory Structural Health Monitoring System: A Smartphone Accelerometer and Camera Fusion Approach. IEEE Sens. J. 2021, 21, 20539–20551. [Google Scholar] [CrossRef]
- Brown, C.; Chauhan, J.; Grammenos, A.; Han, J.; Hasthanasombat, A.; Spathis, D.; Xia, T.; Cicuta, P.; Mascolo, C. Exploring automatic diagnosis of COVID-19 from crowdsourced respiratory sound data. In Proceedings of the 26th ACM SIGKDD International Conference on Knowledge Discovery & Data Mining, Virtual Event, 6–10 July 2020; pp. 3474–3484. [Google Scholar]
- Kvapilova, L.; Boza, V.; Dubec, P.; Majernik, M.; Bogar, J.; Jamison, J.; Goldsack, J.C.; Kimmel, D.J.; Karlin, D.R. Continuous sound collection using smartphones and machine learning to measure cough. Digit. Biomark. 2020, 3, 166–175. [Google Scholar]
- Nascimento, L.M.S.d.; Bonfati, L.V.; Freitas, M.L.B.; Mendes Junior, J.J.A.; Siqueira, H.V.; Stevan, S.L., Jr. Sensors and systems for physical rehabilitation and health monitoring—A review. Sensors 2020, 20, 4063. [Google Scholar] [CrossRef] [PubMed]
- Halloran, S.; Tang, L.; Guan, Y.; Shi, J.Q.; Eyre, J. Remote monitoring of stroke patients’ rehabilitation using wearable accelerometers. In Proceedings of the 2019 ACM International Symposium on Wearable Computers, London, UK, 9–13 September 2019; pp. 72–77. [Google Scholar]
- Aliverti, A.; Lacca, D.; LoMauro, A. Quantitative Analysis by 3D Graphics of Thoraco-Abdominal Surface Shape and Breathing Motion. Front. Bioeng. Biotechnol. 2022, 10, 910499. [Google Scholar] [CrossRef]
- Bianchi, R.; Gigliotti, F.; Romagnoli, I.; Lanini, B.; Castellani, C.; Binazzi, B.; Stendardi, L.; Grazzini, M.; Scano, G. Patterns of chest wall kinematics during volitional pursed-lip breathing in COPD at rest. Respir. Med. 2007, 101, 1412–1418. [Google Scholar] [CrossRef] [PubMed]
- Takashima, S.; Nozoe, M.; Mase, K.; Kouyama, Y.; Matsushita, K.; Ando, H. Effects of posture on chest-wall configuration and motion during tidal breathing in normal men. J. Phys. Ther. Sci. 2017, 29, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Tukanova, K.; Papi, E.; Jamel, S.; Hanna, G.B.; McGregor, A.H.; Markar, S.R. Assessment of chest wall movement following thoracotomy: A systematic review. J. Thorac. Dis. 2020, 12, 1031. [Google Scholar] [CrossRef] [PubMed]
- Grimby, G.; Fugl-Meyer, A.R.; Blomstrand, A. Partitioning of the contributions of rib cage and abdomen to ventilation in ankylosing spondylitis. Thorax 1974, 29, 179–184. [Google Scholar] [CrossRef][Green Version]
- Lunardi, A.C.; Miranda, C.S.; Silva, K.M.; Cecconello, I.; Carvalho, C.R. Weakness of expiratory muscles and pulmonary complications in malnourished patients undergoing upper abdominal surgery. Respirology 2012, 17, 108–113. [Google Scholar] [CrossRef]
- Kristjánsdóttir, Á.; Ragnarsdóttir, M.; Hannesson, P.; Beck, H.J.; Torfason, B. Respiratory movements are altered three months and one year following cardiac surgery. Scand. Cardiovasc. J. 2004, 38, 98–103. [Google Scholar] [CrossRef]
- Monaco, V.; Giustinoni, C.; Ciapetti, T.; Maselli, A.; Stefanini, C. Assessing Respiratory Activity by Using IMUs: Modeling and Validation. Sensors 2022, 22, 2185. [Google Scholar] [CrossRef]
- Massaroni, C.; Nicolò, A.; Lo Presti, D.; Sacchetti, M.; Silvestri, S.; Schena, E. Contact-based methods for measuring respiratory rate. Sensors 2019, 19, 908. [Google Scholar] [CrossRef] [PubMed]
- De la Fuente, C.; Weinstein, A.; Guzman-Venegas, R.; Arenas, J.; Cartes, J.; Soto, M.; Carpes, F.P. Use of accelerometers for automatic regional chest movement recognition during tidal breathing in healthy subjects. J. Electromyogr. Kinesiol. 2019, 47, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Angelucci, A.; Camuncoli, F.; Galli, M.; Aliverti, A. A wearable system for respiratory signal filtering based on activity: A preliminary validation. In Proceedings of the 2022 IEEE International Workshop on Sport, Technology and Research (STAR), Cavalese, Italy, 13–15 July 2022; pp. 19–23. [Google Scholar]
- Escobedo, P.; Bhattacharjee, M.; Nikbakhtnasrabadi, F.; Dahiya, R. Smart bandage with wireless strain and temperature sensors and batteryless NFC tag. IEEE Internet Things J. 2020, 8, 5093–5100. [Google Scholar] [CrossRef]
- Valentine, S.; Cunningham, A.C.; Klasmer, B.; Dabbah, M.; Balabanovic, M.; Aral, M.; Vahdat, D.; Plans, D. Smartphone movement sensors for the remote monitoring of respiratory rates: Technical validation. Digit. Health 2022, 8, 20552076221089090. [Google Scholar] [CrossRef]
- Aly, H.; Youssef, M. Zephyr: Ubiquitous accurate multi-sensor fusion-based respiratory rate estimation using smartphones. In Proceedings of the IEEE INFOCOM 2016-The 35th Annual IEEE International Conference on Computer Communications, San Francisco, CA, USA, 10–14 April 2016; pp. 1–9. [Google Scholar]
- Ladjal, H.; Shariat, B.; Azencot, J.; Beuve, M. Appropriate biomechanics and kinematics modeling of the respiratory system: Human diaphragm and thorax. In Proceedings of the 2013 IEEE/RSJ International Conference on Intelligent Robots and Systems, Tokyo, Japan, 3–7 November 2013; pp. 2004–2009. [Google Scholar]
- Torres-Tamayo, N.; García-Martínez, D.; Lois Zlolniski, S.; Torres-Sánchez, I.; García-Río, F.; Bastir, M. 3D analysis of sexual dimorphism in size, shape and breathing kinematics of human lungs. J. Anat. 2018, 232, 227–237. [Google Scholar] [CrossRef] [PubMed]
- Shaw, B.S.; Shaw, I. Pulmonary function and abdominal and thoracic kinematic changes following aerobic and inspiratory resistive diaphragmatic breathing training in asthmatics. Lung 2011, 189, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Rousanoglou, E.; Foskolou, A.; Emmanouil, A.; Boudolos, K. Inertial Sensing of the Abdominal Wall Kinematics during Diaphragmatic Breathing in Head Standing. Biomechanics 2024, 4, 63–83. [Google Scholar] [CrossRef]
- Yang, L.; Qu, S.; Zhang, Y.; Zhang, G.; Wang, H.; Yang, B.; Xu, C.; Dai, M.; Cao, X. Removing clinical motion artifacts during ventilation monitoring with electrical impedance tomography: Introduction of methodology and validation with simulation and patient data. Front. Med. 2022, 9, 817590. [Google Scholar] [CrossRef]
- Simone, L.; Miglior, L.; Gervasi, V.; Moroni, L.; Vignali, E.; Gasparotti, E.; Celi, S. Early Screening of Cardiorespiratory Diseases Through Smartphone IMU Sensors and Bidirectional LSTM. Available online: http://dx.doi.org/10.2139/ssrn.4676194 (accessed on 13 March 2024).
- Candan, B.; Soken, H.E. Robust attitude estimation using IMU-only measurements. IEEE Trans. Instrum. Meas. 2021, 70, 1–9. [Google Scholar] [CrossRef]
- Romei, M.; Mauro, A.L.; D’angelo, M.; Turconi, A.; Bresolin, N.; Pedotti, A.; Aliverti, A. Effects of gender and posture on thoraco-abdominal kinematics during quiet breathing in healthy adults. Respir. Physiol. Neurobiol. 2010, 172, 184–191. [Google Scholar] [CrossRef]
- Erfianto, B.; Rizal, A. IMU-Based Respiratory Signal Processing Using Cascade Complementary Filter Method. J. Sens. 2022, 2022, 7987159. [Google Scholar] [CrossRef]
- Sikora, M.; Mikołajczyk, R.; Łakomy, O.; Karpiński, J.; Żebrowska, A.; Kostorz-Nosal, S.; Jastrzębski, D. Influence of the breathing pattern on the pulmonary function of endurance-trained athletes. Sci. Rep. 2024, 14, 1113. [Google Scholar] [CrossRef]
- Kiesel, K.; Rhodes, T.; Mueller, J.; Waninger, A.; Butler, R. Development of a screening protocol to identify individuals with dysfunctional breathing. Int. J. Sport. Phys. Ther. 2017, 12, 774. [Google Scholar] [CrossRef]
- Russo, M.A.; Santarelli, D.M.; O’Rourke, D. The physiological effects of slow breathing in the healthy human. Breathe 2017, 13, 298–309. [Google Scholar] [CrossRef]
- De Fazio, R.; Greco, M.R.; De Vittorio, M.; Visconti, P. A Differential Inertial Wearable Device for Breathing Parameter Detection: Hardware and Firmware Development, Experimental Characterization. Sensors 2022, 22, 9953. [Google Scholar] [CrossRef] [PubMed]
- Vertens, J.; Fischer, F.; Heyde, C.; Hoeflinger, F.; Zhang, R.; Reindl, L.M.; Gollhofer, A. Measuring Respiration and Heart Rate using Two Acceleration Sensors on a Fully Embedded Platform. In Proceedings of the icSPORTS, Lisbon, Portugal, 15–17 November 2015; pp. 15–23. [Google Scholar]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Smartphone Positions | |||
|---|---|---|---|
| Vertical orientation | 19 dB | 18 dB | |
| 26 dB | 25 dB | ||
| 23 dB | 20 dB | ||
| 26 dB | 25 dB | ||
| 23 dB | 22 dB | ||
| Horizontal orientation | 20 dB | 23 dB | |
| 25 dB | 26 dB | ||
| 22 dB | 21 dB | ||
| 25 dB | 25 dB | ||
| 26 dB | 25 dB | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vignali, E.; Gasparotti, E.; Miglior, L.; Gervasi, V.; Simone, L.; Haxhiademi, D.; Frediani, L.; Borelli, G.; Berti, S.; Celi, S. A New Smartphone-Based Method for Remote Health Monitoring: Assessment of Respiratory Kinematics. Electronics 2024, 13, 1132. https://doi.org/10.3390/electronics13061132
Vignali E, Gasparotti E, Miglior L, Gervasi V, Simone L, Haxhiademi D, Frediani L, Borelli G, Berti S, Celi S. A New Smartphone-Based Method for Remote Health Monitoring: Assessment of Respiratory Kinematics. Electronics. 2024; 13(6):1132. https://doi.org/10.3390/electronics13061132
Chicago/Turabian StyleVignali, Emanuele, Emanuele Gasparotti, Luca Miglior, Vincenzo Gervasi, Lorenzo Simone, Dorela Haxhiademi, Lara Frediani, Gabriele Borelli, Sergio Berti, and Simona Celi. 2024. "A New Smartphone-Based Method for Remote Health Monitoring: Assessment of Respiratory Kinematics" Electronics 13, no. 6: 1132. https://doi.org/10.3390/electronics13061132
APA StyleVignali, E., Gasparotti, E., Miglior, L., Gervasi, V., Simone, L., Haxhiademi, D., Frediani, L., Borelli, G., Berti, S., & Celi, S. (2024). A New Smartphone-Based Method for Remote Health Monitoring: Assessment of Respiratory Kinematics. Electronics, 13(6), 1132. https://doi.org/10.3390/electronics13061132