1. Introduction
Atrial fibrillation (AF) is the most common clinical arrhythmia, threatening patient health and profoundly increasing morbidity, mortality, and healthcare-related costs [
1]. At present, the estimated prevalence of AF in adults is between 2% and 4%, with a 2.3-fold increase projected due to increased lifespan in the general population [
2]. The risk of developing AF increases with age. Approximately 60% of patients with AF are between the ages of 65 and 85 years [
3]. Various diseases have been associated with AF, such as stroke, heart failure, coronary artery disease, and systemic thromboembolism [
4,
5]. Thus, the timely detection and prevention of AF is significant [
6]. However, a significant proportion of patients with atrial fibrillation are asymptomatic or have mild symptoms, a phenomenon known as subclinical atrial fibrillation. Thus, without the use of cardiac monitoring devices, timely and accurate diagnoses are difficult. Therefore, a cardiac monitoring device that can be used for daily monitoring and early detection of AF is needed.
At present, electrocardiography (ECG) is the main method for diagnosing AF. The typical features of AF include the absence of P-waves, which are replaced by rapid oscillations or fibrillatory waves, and the irregular variability of RR intervals. These features have allowed various AF detection methods to be developed, including the template-based algorithm [
7], feature analysis based on the RR intervals [
8], the application of symbolic dynamics, Shannon entropy based on the support vector machine (SVM) [
9], and the combination of the genetic algorithm and random forest classifier [
10]. In recent years, convolutional neural networks (CNNs) have been used for AF detection due to their strong feature extraction ability. Limam et al. [
11] proposed a convolutional recurrent neural network (CRNN) consisting of two independent CNNs to extract related features, one from ECG and the other from heart rates. Dang et al. [
12] combined CNN and bidirectional long short-term memory (Bi-LSTM) to automatically detect AF from ECG signals. Yao et al. [
13] proposed a multi-scale CNN which applied time scaling on input ECG signals and detected AF based on scaled inputs. The residual network [
14] is a type of deep neural network (DNN) that was first proposed for image classification tasks. The residual network has recently been successfully applied to ECG AF detection due to its excellent classification performance and characteristics that can alleviate the degradation problem of DNNs. He et al. [
15] proposed a model consisting of residual CNN and Bi-LSTM to extract features from raw ECG signals. Cao et al. [
16] used an improved multi-scale decomposition enhanced residual CNN to detect AF from a single short ECG lead recording. Faust et al. [
17] proposed a method using residual CNN model to extract features from RR intervals of ECG signals. However, the above methods are based on the acquisition of ECG signals and usually require that electrodes are in direct contact with the skin of the subject, which can be uncomfortable and inconvenient for long-term use, and is thus not suitable for monitoring cardiac activity in daily life. Therefore, researchers have proposed some noncontact cardiac activity monitoring techniques.
Previous studies have shown that noncontact cardiac monitoring techniques can be used by subjects in daily life for long-term cardiac activity monitoring [
18]. The ballistocardiogram (BCG) [
19] and seismocardiogram (SCG) [
20] capture the body’s mechanical responses to cardiac activity and blood circulation. The difference between them is that the BCG measures pressure changes of the body against the measurement plane, while the SCG measures local vibrations of the chest wall. The BCG is a noncontact body vibration detection method. In addition to the mechanical activity of the heart, other physiological factors that cause body vibrations include breathing, noise, and motion artifacts (MA) [
21,
22,
23]. BCG signals can be acquired by placing piezoelectric sensors on the measurement plane, such as under mattresses [
24] and chairs cushions [
25]. In recent years, researchers have proposed many cardiac activity detection algorithms based on BCG signals, such as heart rate detection [
26,
27], J peak feature extraction [
28], and cardiovascular disease classification [
29].
Although BCG-based cardiac activity monitoring research has developed rapidly in recent years, the use of BCG signals for AF detection remains an unexplored technique. Brüser et al. [
30] proposed a feature selection algorithm based on the mutual information between the features and class labels, as well as the first- and second-order interactions among features, and evaluated seven machine learning algorithms (naive Bayes, linear and quadratic discriminant analysis, support vector machine, random forest, and bagged and boosted trees) for their performance in separating 30 s-long BCG epochs into AF, SR, and MA. The best classifier (random forest) achieved a mean sensitivity and specificity of 93.8% and 98.2%, respectively. Yu et al. [
31] extracted features from stationary wavelet transform of 30 s BCG epochs and used three machine learning classifiers (support vector machine, K-nearest neighbor, and ensemble learning) to detect AF. The ensemble classifier achieved a mean accuracy, sensitivity, and specificity of 94.4%, 97.0%, and 89.1%, respectively. Wen et al. [
32] extracted features from BCG energy signals and used five machine learning algorithms (support vector machine, naive Bayes, decision tree, bootstrap aggregated decision tree, and random forest) to identify AF and SR. The algorithm achieved a sensitivity, precision, and accuracy of 96.8%, 92.8%, and 94.5%, respectively. Jiang et al. [
33] proposed a deep learning method for AF and SR classification that integrated features extracted from a Bi-LSTM network and features extracted from phase space. The method achieved an accuracy, specificity, sensitivity, and precision of 94.7%, 93.5%, 95.9%, and 93.7%, respectively.
Some effective methods for BCG-based AF detection have been proposed thus far, but certain issues remain. First, most previous studies [
30,
31,
32] have focused on traditional machine learning. However, manual feature extraction is subjective and may lead to the loss of important information, especially considering the morphological diversity of BCG signals. Second, the BCG datasets used with the previously proposed methods [
30,
31,
32,
33] are small in scale, while machine learning, especially deep learning methods, require a large amount of data for training and validation.
In this manuscript, we focus on developing a noncontact AF detection method based on BCG signals. An offline residual CNN model, inspired by ECG-based AF detection methods [
15,
16,
17], was proposed to detect AF in BCG segments, which can be applied in household long-term AF monitoring and screening. To summarize, the main contributions are: (1) To the best of our knowledge, this manuscript is the first to apply residual CNN to extract features from BCG segments for AF detection. (2) The number of BCG segments in our dataset is currently the largest in relevant research, which ensures the feasibility and reliability of the proposed deep learning method. This manuscript is organized as follows:
Section 2 describes the proposed method including dataset construction, residual CNN model construction, and the detailed experimental process.
Section 3 presents our study results and analysis.
Section 4 provides discussions of our findings and potential future work.
Section 5 concludes the whole passage.
3. Results
The effect of the number of residual blocks on the experimental results was explored to determine the final model structure first (
Table 5).
For models with number of residual blocks ranging from 2 to 6, the performance for each class, as well as the mean performance over all classes, are given. We highlighted the best results for each performance measure. When the number of residual blocks was set to 4, most of the metrics achieved the best performance. In particular, the sensitivity of AF is significantly better than others, which is an important screening metric because it measures the ability of the method to correctly detect AF.
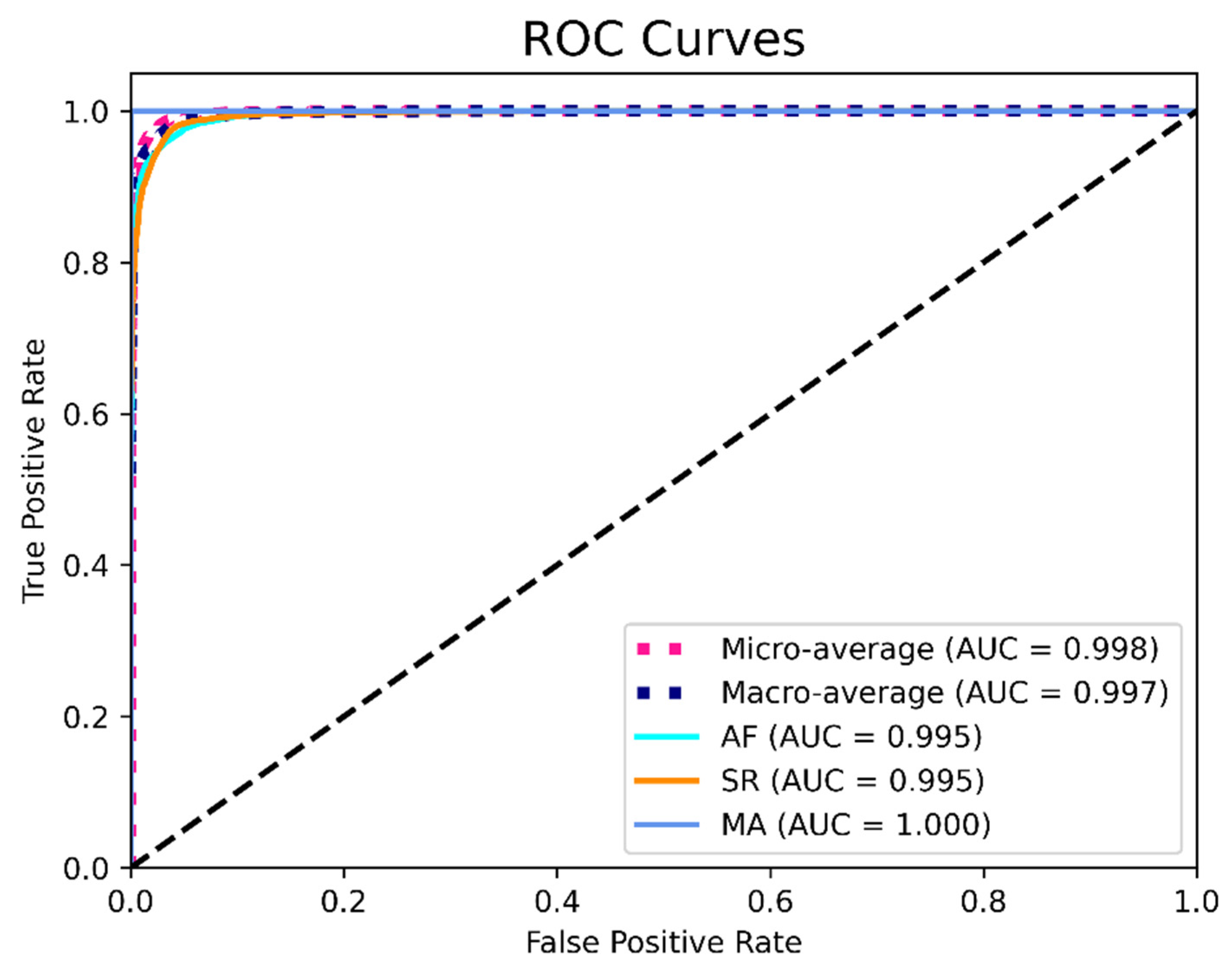
To further evaluate the generalizability and stability of the model, we used tenfold cross validation when the number of residual blocks was set to 4. The final cross validation confusion matrix (the sum of the results of 10 computational experiments) and performance evaluation are shown in
Table 6 and
Table 7. The ROC curves shown in
Figure 7 provides a graphical representation of the classification results of all 10 folds.
The data in
Table 6 and
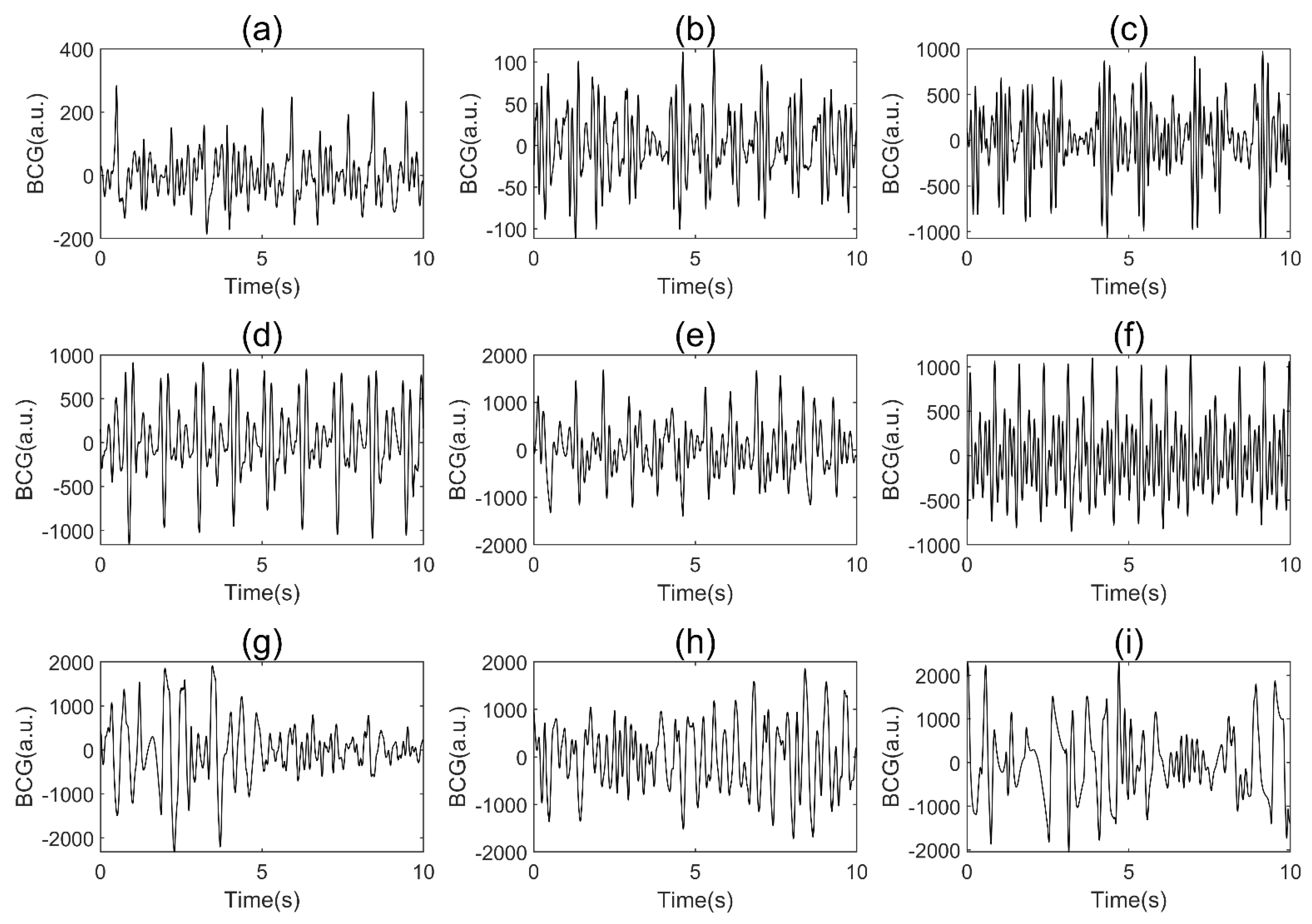
Table 7 indicate that MA could be identified without error, while AF and SR were sometimes misidentified. This result may have occurred because the MA among subjects generally has much larger amplitudes than the two other classes (
Figure 5), which tends to be easily identified due to strong feature extraction ability of the CNN model. The AF and SR signals are closer in amplitude, and the BCG signal itself has considerable individual variability, which contributes to the confusion between them. In addition, the sensitivity was observed to be lower than the specificity in AF, which indicates that AF is more likely to be misjudged than SR. This result may be due to the high variability of BCG signals. When AF occurs, complex and diverse internal forces cause the BCG signal to exhibit very irregular waveforms, which are difficult to interpret. At the same time, the rhythm of some SR BCG signals is not very regular (
Figure 5), which makes AF more likely to be misjudged as SR.
Table 7 shows that the model has good stability, with low standard deviations for all metrics.
Figure 7 indicates that the model achieved an AUC score of 0.995, 0.995, and 1.000 for AF, SR and MA, respectively, which shows good performance of the algorithm. To summarize, the final performance of the proposed residual CNN model achieved a mean precision, sensitivity, specificity, F1 score, and accuracy of 96.8%, 93.7%, 98.4%, 95.2%, and 96.8%, respectively.
4. Discussion
4.1. Method Analysis
In this study, we focused on developing a BCG-based method for household daily AF screening, which is mainly required by people with paroxysmal AF or with a high risk of AF. We first constructed a balanced BCG signal dataset containing AF, SR, and MA through data acquisition, preprocessing, labeling, and segmentation. The number of BCG segments in our dataset is larger than any other previous BCG-based study, ensuring enough BCG data for training the model. In previous studies [
31,
32,
33], MA BCG signals were discarded during data preprocessing to focus on classification between AF and SR. We added the MA to dataset for two reasons. First, incorporating MA into the dataset allows the algorithm to handle the MA signals common in BCG recordings in real scenes, which improves the robustness of the algorithm. Second, the binary classification has the characteristics of either-or and three-class classification task is more challenging.
We applied the residual CNN to AF detection based on BCG segments for the first time in related studies. The proposed model has four modules: the downsampling convolutional module, local feature learning module, global feature learning module, and classification module. The downsampling convolutional module mainly undertakes two functions: to quickly reduce the dimension of the feature vector and to concentrate the contextual information of the BCG signal to prevent overfitting. The local and global feature learning modules are core components of the model. Stacked residual blocks are used for local feature extraction, and GlobalAvgPooling layer can capture global features from the feature vectors output by local feature learning module, which attempts more in-depth feature learning of BCG segment. We explored the impact of different numbers of residual blocks on the classification performance to determine the final network structure. Tenfold cross validation was applied to further confirm the stability of the model. The final confusion matrix and the values of various metrics show that our proposed method achieved good performance on the task of off-line BCG segment-based AF detection.
4.2. Method Comparison
We compared the proposed method with four previously published methods [
30,
31,
32,
33]. All four methods are based on the noncontact acquisition of BCG signals for AF detection. The methods published in [
30,
31,
32] are based on traditional machine learning, which require artificial feature engineering. Jiang et al. [
33] applied a DNN consisting of CNN and Bi-LSTM into BCG-AF detection. A detailed comparison is shown in
Table 8.
The data in
Table 8 clearly show that the proposed method performs better than the previous methods in terms of the Pre, Spe, F1, and Acc, which indicates that our method is suitable for AF screening. In addition, we compared the segment length, number of segments, number of subjects, and number of classes to evaluate the feasibility and credibility of our method from multiple perspectives. Our BCG data were collected from 45 subjects and divided into 28,214 ten-second segments after preprocessing. The dataset contains a similar number of signals for all three signal types. The increased number of segments increases the size and diversity of the BCG dataset and the balanced data distribution improves the model training efficiency while ensuring that the generalizability of the classification algorithm is not reduced due to too much data from a certain class. In this manuscript, we completed a three-class classification task similar to Brüser et al. [
30], which is more difficult than the two-class (only AF and SR) classification problem [
31,
32,
33]. The addition of a motion artifacts class allows our method to handle motion artifacts that are common in BCG recordings, thus enabling unsupervised processing of the BCG signal [
30]. The results show that the ability of our method to detect AF is not reduced by motion artifacts, which indicates that the method performs well in terms of anti-noise interference.
Compared with traditional machine learning algorithms, one advantage of the proposed method is that there is no need to manually extract features of BCG signals [
30,
31,
32]. Compared with the deep learning method proposed by Jiang et al. [
33], the proposed method has two distinct advantages. First, the number of segments is considerably larger, which is of great significance for training a deep learning model and improving the credibility of the method. Second, the subjects in [
33] all suffered from paroxysmal AF, while the subjects in our research consisted of 19 people suffering from paroxysmal AF and 26 non-AF patients. Such an experimental setup enables MA BCG signals from both AF patients and non-AF individuals, increasing the diversity of the BCG dataset and making the AF detection experiments closer to real scenarios. The standard deviations of all metrics in
Table 7 were less than 0.02, demonstrating that our method performs well in terms of preventing overfitting and improving generalizability.
4.3. Application Issues and Limitations
Compared with ECG, the advantage of BCG is that the signals can be acquired in a noncontact way, which ensures comfort and convenience of signal acquisition. However, unlike ECG, for which there are already well-defined diagnostic criteria, the use of BCG to detect arrhythmias such as AF is still in its infancy. BCG is accompanied by a high degree of variability and suffers from inadequate interpretation, as the relationship between BCG and cardiac activity has not been fully elucidated. Therefore, BCG may not replace ECG as the gold standard for clinical diagnosis at the current stage.
The proposed method in this manuscript provides a feasible solution for detect AF in BCG segments. Considering the easy acquisition of BCG, this method can be applied to AF screening, providing tools for timely detection of AF and follow-up after AF drug or device treatment. In clinical application, it may be used to determine whether AF occurs during the sleep of the subject, and how many 10 s segments of AF have occurred. At the same time, it can also assist in determining whether these 10 s segments of AF are continuous, which all contribute to initial screening and subsequent more accurate clinical diagnosis and treatment of AF.
Furthermore, there are a few limitations to the proposed method. First, although we constructed a BCG dataset of 28,214 ten-second segments, which is greater in number than any other BCG study, and the number of subjects is considerable among related studies, the database still needs to be expanded to further evaluate the robustness of the deep learning algorithm. Second, the database mostly included older subjects. Third, arrhythmias other than AF were not considered.
4.4. Future Work
The purpose of our study is to apply an offline DNN model to identify AF segments based on BCG signals for long-term household AF screening. Considering practical application scenarios, we will continue to conduct research in the following aspects. First, due to the individual differences of BCG signals, we will attempt to collect more BCG signals of subjects of different ages to increase the size and diversity of the dataset. Different acquisition devices, acquisition conditions, and subject postures will also be taken into account to analyze performance of the method in different scenarios. Second, we will explore the structure and training method of the DNN model to accommodate the expansion of the dataset. Since ECG-based methods are relatively mature, DNNs that were widely used in the ECG detection of AF will be given priority. Third, other arrhythmias, which may cause false positives in AF discrimination, should be considered during classification if a big enough dataset can be built. Thus, we may expand the method to more classes of cardiac diseases in future research.
5. Conclusions
In this manuscript, we proposed a feasible method for AF detection by BCG signals of 10 s length. We collected BCG signals from 45 inpatients and constructed a large BCG dataset containing 28,214 ten-second nonoverlapping segments, including AF, SR, and MA. An offline residual CNN model was designed to classify the three types of BCG signals. The model has an end-to-end classification structure, with a downsampling convolutional module, a local feature learning module, a global feature learning module, and a classification module. The model achieved precision, sensitivity, specificity, F1 score, and accuracy of 96.8%, 93.7%, 98.4%, 95.2%, and 96.8%, respectively. The results suggest that the proposed method may be used as a tool for AF screening in long-term household cardiac monitoring devices.



 ,
, 







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}