The Tumor–Fat Interface Volume of Breast Cancer on Pretreatment MRI Is Associated with a Pathologic Response to Neoadjuvant Chemotherapy

 , ,
, ,  ,
,
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
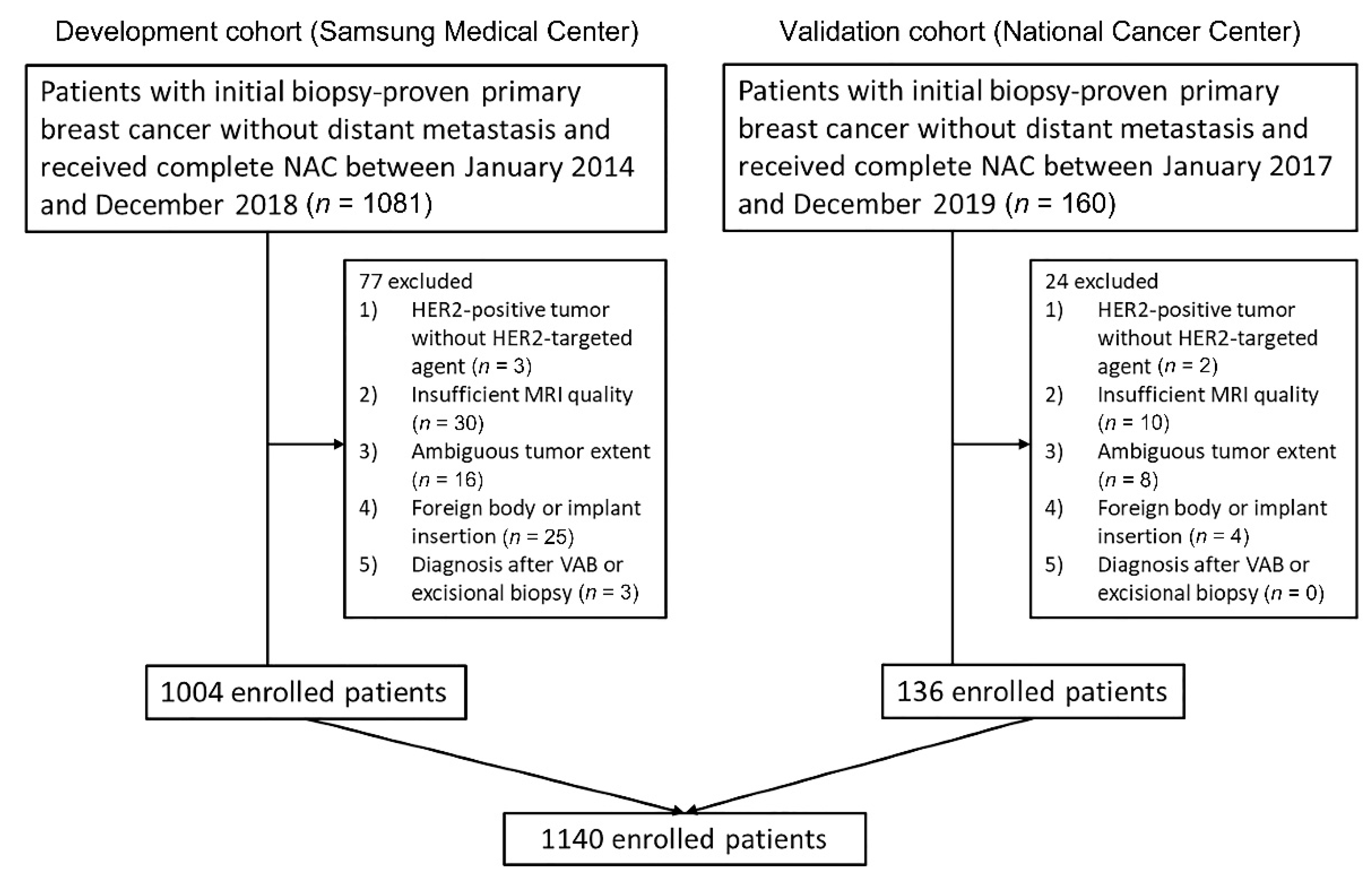
2.1. Patients
2.2. MRI Protocol
2.3. Preparation of MRI for Measurement
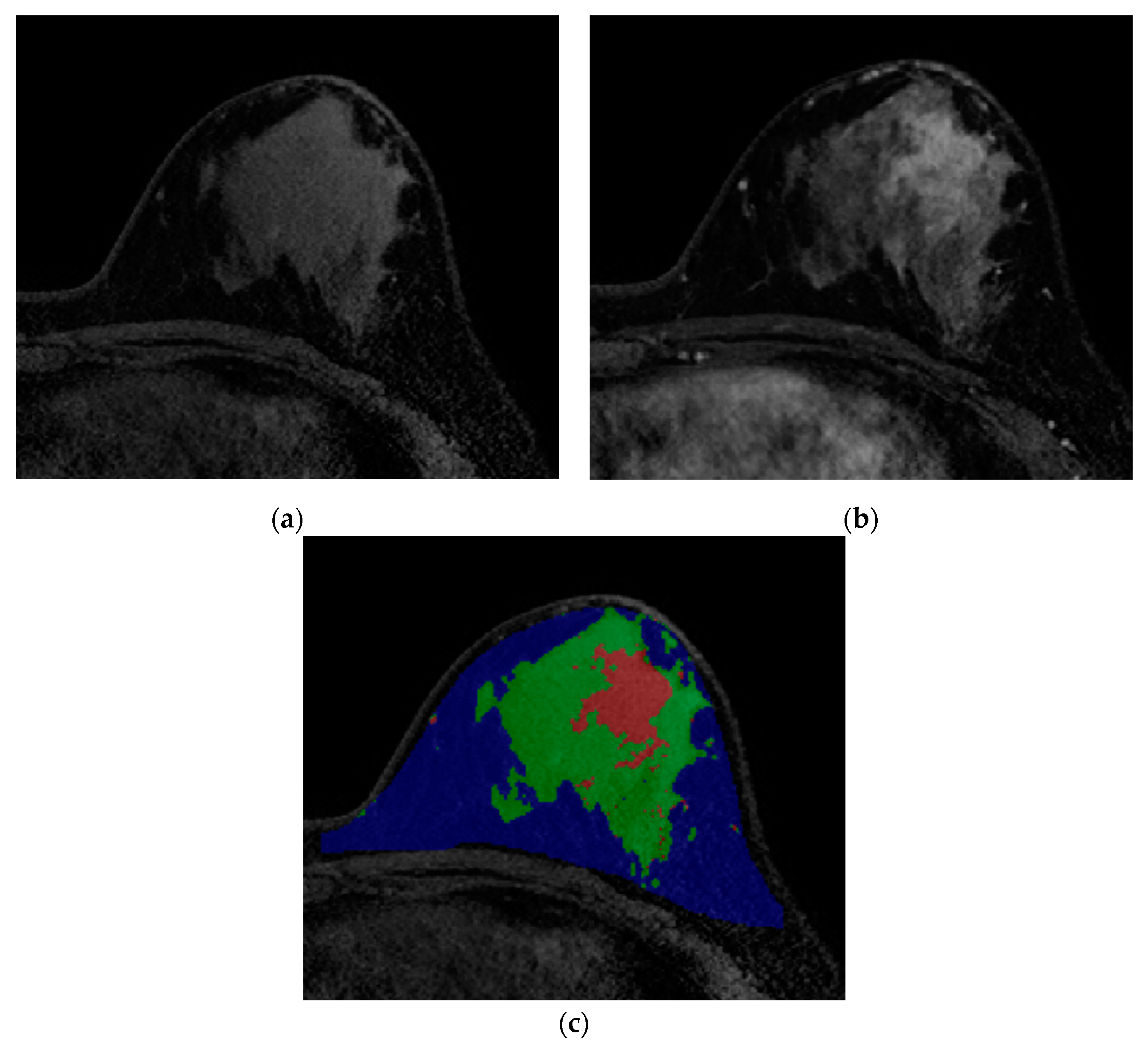
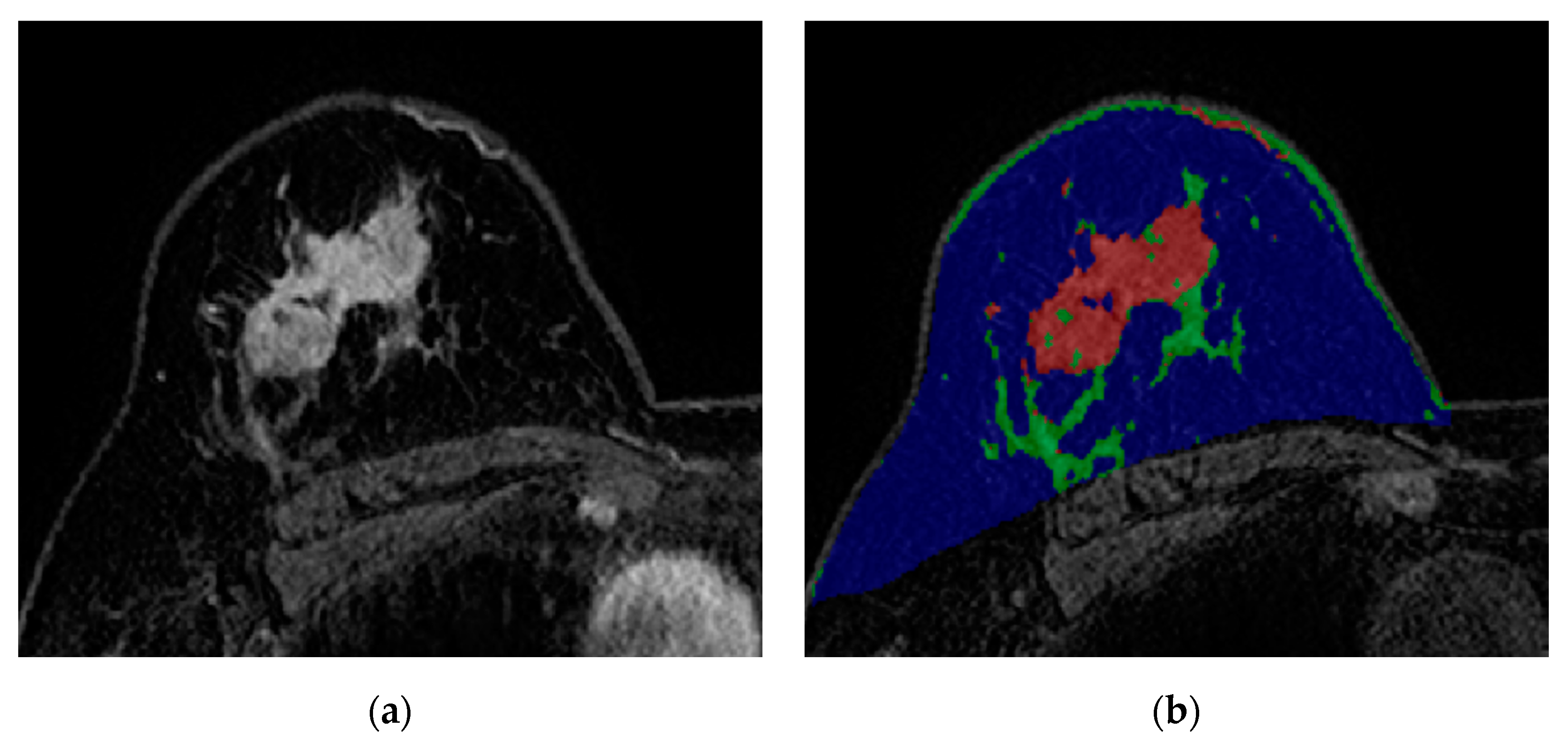
2.4. Quantitative Measurements of Tumor–Fat Interface
2.5. Clinical and Pathological Evaluation
2.6. Statistical Analysis
3. Results
3.1. Patient Outcomes
3.2. Relationship between the Tumor-Fat Interface Volume and Clinicopathological Factors
3.3. Factors Associated with Pathologic Response in the Development Cohort
3.4. Validation of the Tumor-Fat Interface Volume in the Validation Cohort and Comparison of Model Performance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Chen, X.S.; Yuan, Y.; Garfield, D.H.; Wu, J.; Huang, O.; Shen, K. Both carboplatin and bevacizumab improve pathological complete remission rate in neoadjuvant treatment of triple negative breast cancer: A meta-analysis. PLoS ONE 2014, 9, e108405. [Google Scholar] [CrossRef] [PubMed]
- Schneeweiss, A.; Chia, S.; Hickish, T.; Harvey, V.; Enju, A.; Hegg, R.; Tausch, C.; Seo, J.H.; Tsai, Y.F.; Ratnayake, J.; et al. Pertuzumab plus trastuzumab in combination with standard neoadjuvant anthracycline-containing and anthracycline-free chemotherapy regimens in patients with HER2-positive early breast cancer: A randomized phase II cardiac safety study (TRYPHAENA). Ann. Oncol. 2013, 24, 2278–2284. [Google Scholar] [CrossRef] [PubMed]
- Cortazar, P.; Zhang, L.; Untch, M.; Mehta, K.; Constantino, J.P.; Wolmark, N.; Bonnefoi, H.; Cameron, D.; Gianni, L.; Valagussa, P.; et al. Pathological complete response and long-term clinical benefit in breast cancer: The CTNeoBC pooled analysis. Lancet 2014, 384, 164–172. [Google Scholar] [CrossRef]
- Cameron, D.A.; Anderson, E.D.; Levack, P.; Hawkins, R.A.; Anderson, T.J.; Leonard, R.C.; Forrest, A.P.; Chetty, U. Primary systemic therapy for operable breast cancer--10-year survival data after chemotherapy and hormone therapy. Br. J. Cancer 1997, 76, 1099–1105. [Google Scholar] [CrossRef]
- Liedtke, C.; Mazouni, C.; Hess, K.R.; André, F.; Tordai, A.; Mejia, J.A.; Symmans, W.F.; Gonzalez-Angulo, A.M.; Hennessy, B.; Green, M.; et al. Response to neoadjuvant therapy and long-term survival in patients with triple-negative breast cancer. J. Clin. Oncol. 2008, 26, 1275–1281. [Google Scholar] [CrossRef]
- Buchholz, T.A.; Lehman, C.D.; Harris, J.R.; Pockaj, B.A.; Khouri, N.; Hylton, N.F.; Miller, M.J.; Whelan, T.; Pierce, L.J.; Esserman, L.J.; et al. Statement of the science concerning locoregional treatments after preoperative chemotherapy for breast cancer: A National Cancer Institute conference. J. Clin. Oncol. 2008, 26, 791–797. [Google Scholar] [CrossRef]
- von Minckwitz, G.; Blohmer, J.U.; Costa, S.D.; Denkert, C.; Eidtmann, H.; Eiermann, W.; Gerber, B.; Hanusch, C.; Hilfrich, J.; Huober, J.; et al. Response-guided neoadjuvant chemotherapy for breast cancer. J. Clin. Oncol. 2013, 31, 3623–3630. [Google Scholar] [CrossRef]
- Park, J.; Morley, T.S.; Kim, M.; Clegg, D.J.; Scherer, P.E. Obesity and cancer--mechanisms underlying tumour progression and recurrence. Nat. Rev. Endocrinol. 2014, 10, 455–465. [Google Scholar] [CrossRef]
- Waki, H.; Tontonoz, P. Endocrine functions of adipose tissue. Annu. Rev. Pathol. 2007, 2, 31–56. [Google Scholar] [CrossRef]
- Tan, J.; Buache, E.; Chenard, M.P.; Dali-Youcef, N.; Rio, M.C. Adipocyte is a non-trivial, dynamic partner of breast cancer cells. Int. J. Dev. Biol. 2011, 55, 851–859. [Google Scholar] [CrossRef]
- Hefetz-Sela, S.; Scherer, P.E. Adipocytes: Impact on tumor growth and potential sites for therapeutic intervention. Pharmacol. Ther. 2013, 138, 197–210. [Google Scholar] [CrossRef] [PubMed]
- Bochet, L.; Meulle, A.; Imbert, S.; Salles, B.; Valet, P.; Muller, C. Cancer-associated adipocytes promotes breast tumor radioresistance. Biochem. Biophys. Res. Commun. 2011, 411, 102–106. [Google Scholar] [CrossRef] [PubMed]
- Behan, J.W.; Yun, J.P.; Proektor, M.P.; Ehsanipour, E.A.; Arutyunyan, A.; Moses, A.S.; Avramis, V.I.; Louie, S.G.; Butturini, A.; Heisterkamp, N.; et al. Adipocytes impair leukemia treatment in mice. Cancer Res. 2009, 69, 7867–7874. [Google Scholar] [CrossRef] [PubMed]
- Duong, M.N.; Cleret, A.; Matera, E.L.; Chettab, K.; Mathé, D.; Valsesia-Wittmann, S.; Clémenceau, B.; Dumontet, C. Adipose cells promote resistance of breast cancer cells to trastuzumab-mediated antibody-dependent cellular cytotoxicity. Breast Cancer Res. 2015, 17, 57. [Google Scholar] [CrossRef]
- Khan, S.; Shukla, S.; Sinha, S.; Meeran, S.M. Role of adipokines and cytokines in obesity-associated breast cancer: Therapeutic targets. Cytokine Growth Factor Rev. 2013, 24, 503–513. [Google Scholar] [CrossRef]
- Iyengar, P.; Combs, T.P.; Shah, S.J.; Gouon-Evans, V.; Pollard, J.W.; Albanese, C.; Flanagan, L.; Tenniswood, M.P.; Guha, C.; Lisanti, M.P.; et al. Adipocyte-secreted factors synergistically promote mammary tumorigenesis through induction of anti-apoptotic transcriptional programs and proto-oncogene stabilization. Oncogene 2003, 22, 6408–6423. [Google Scholar] [CrossRef]
- Edge, S.B.; Compton, C.C. The American Joint Committee on Cancer: The 7th edition of the AJCC cancer staging manual and the future of TNM. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef]
- WHO. Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 2004, 363, 157–163. [Google Scholar] [CrossRef]
- Fujii, T.; Kogawa, T.; Dong, W.; Sahin, A.A.; Moulder, S.; Litton, J.K.; Tripathy, D.; Iwamoto, T.; Hunt, K.R.; Pusztai, L.; et al. Revisiting the definition of estrogen receptor positivity in HER2-negative primary breast cancer. Ann. Oncol. 2017, 28, 2420–2428. [Google Scholar] [CrossRef]
- Loo, C.E.; Rigter, L.S.; Pengel, K.E.; Wesseling, J.; Rodenhuis, S.; Peeters, M.J.; Sikorska, K.; Gilhuijs, K.G.A. Survival is associated with complete response on MRI after neoadjuvant chemotherapy in ER-positive HER2-negative breast cancer. Breast Cancer Res. 2016, 18, 82. [Google Scholar] [CrossRef]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- Copson, E.; Eccles, B.; Maishman, T.; Gerty, S.; Stanton, L.; Cutress, R.I.; Altman, D.G.; Durcan, L.; Simmonds, P.; Lawrence, G.; et al. Prospective observational study of breast cancer treatment outcomes for UK women aged 18–40 years at diagnosis: The POSH study. J. Natl. Cancer Inst. 2013, 105, 978–988. [Google Scholar] [CrossRef] [PubMed]
- Azim, H.A., Jr.; Partridge, A.H. Biology of breast cancer in young women. Breast Cancer Res. 2014, 16, 427. [Google Scholar] [CrossRef] [PubMed]
- James, F.R.; Wootton, S.; Jackson, A.; Wiseman, M.; Copson, E.R.; Cutress, R.I. Obesity in breast cancer--what is the risk factor? Eur. J. Cancer 2015, 51, 705–720. [Google Scholar] [CrossRef]
- Erbes, T.; Stickeler, E.; Rücker, G.; Buroh, S.; Asberger, J.; Dany, N.; Thornton, S.; Ilborra, S.; Hirschfeld, M.; Gitsch, G.; et al. BMI and Pathologic Complete Response to Neoadjuvant Chemotherapy in Breast Cancer: A Study and Meta-Analysis. Clin. Breast Cancer 2016, 16, e119–e132. [Google Scholar] [CrossRef]
- Stacey-Clear, A.; McCarthy, K.A.; Hall, D.A.; Pile-Spellman, E.; White, G.; Hulka, C.A.; Whitman, G.J.; Halpern, E.F.; Kopans, D.B. Mammographically detected breast cancer: Location in women under 50 years old. Radiology 1993, 186, 677–680. [Google Scholar] [CrossRef]
- Kim, W.H.; Li, M.; Han, W.; Ryu, H.S.; Moon, W.K. The Spatial Relationship of Malignant and Benign Breast Lesions with Respect to the Fat-Gland Interface on Magnetic Resonance Imaging. Sci. Rep. 2016, 6, 39085. [Google Scholar] [CrossRef]
- Obeid, J.P.; Stoyanova, R.; Kwon, D.; Patel, M.; Padgett, K.; Slingerland, J.; Takita, C.; Alperin, N.; Yepes, M.L.; Zeidan, Y.H. Multiparametric evaluation of preoperative MRI in early stage breast cancer: Prognostic impact of peri-tumoral fat. Clin. Transl. Oncol. 2017, 19, 211–218. [Google Scholar] [CrossRef]
- Chen, J.H.; Zhang, Y.; Chan, S.; Chang, R.F.; Su, M.Y. Quantitative analysis of peri-tumor fat in different molecular subtypes of breast cancer. Magn. Reson. Imaging 2018, 53, 34–39. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Development Cohort | Validation Cohort | ||||
|---|---|---|---|---|---|---|
| pCR (n = 369) | Non-pCR (n = 635) | p-Value | pCR (n = 45) | Non-pCR (n = 91) | p-Value | |
| Age (median [IQR]) | 49.00 [41.00, 56.00] | 47.00 [40.00, 54.00] | 0.028 | 50.00 [45.00, 58.00] | 52.00 [46.00, 57.50] | 0.985 |
| Breast volume (cm3) (median [IQR]) | 560.96 [388.82, 770.62] | 580.17 [395.30, 805.52] | 0.548 | 618.33 [427.09, 811.17] | 675.34 [430.01, 944.99] | 0.200 |
| Fat volume (cm3) (median [IQR]) | 415.50 [250.97, 603.07] | 407.79 [263.06, 623.10] | 0.859 | 467.77 [308.59, 567.21] | 508.43 [322.12, 749.08] | 0.289 |
| Normal fibroglandular tissue volume (cm3) (median [IQR]) | 125.32 [88.26, 177.29] | 126.58 [88.27, 178.84] | 0.792 | 115.51 [81.39, 186.44] | 142.64 [87.27, 200.07] | 0.420 |
| Tumor volume (cm3) (median [IQR]) | 9.93 [6.05, 18.21] | 13.45 [7.54, 24.81] | <0.001 | 9.67 [6.75, 19.48] | 14.62 [6.65, 22.13] | 0.184 |
| Tumor-fat interface volume (cm3) (median [IQR]) | 1.64 [0.86, 2.85] | 1.93 [1.08, 3.66] | 0.003 | 1.36 [0.83, 2.21] | 2.26 [1.33, 3.66] | 0.004 |
| Operation method | <0.001 | >0.999 | ||||
| Breast-conserving surgery | 298 (80.8) | 361 (56.9) | 33 (73.3) | 68 (74.7) | ||
| Mastectomy | 71 (19.2) | 274 (43.1) | 12 (26.7) | 23 (25.3) | ||
| BMI | 23.60 [21.80, 25.83] | 23.63 [21.67, 26.13] | 0.817 | 25.22 [22.43, 27.73] | 24.95 [23.18, 27.76] | 0.627 |
| BMI | 0.775 | >0.999 | ||||
| <25 (kg/m2) | 240 (65.0) | 420 (66.1) | 22 (48.9) | 46 (50.5) | ||
| ≥25 (kg/m2) | 129 (35.0) | 215 (33.9) | 23 (51.1) | 45 (49.5) | ||
| NAC regimen | <0.001 | 0.004 | ||||
| AC-T | 133 (36.0) | 443 (69.8) | 17 (37.8) | 56 (61.5) | ||
| AC-T/Herceptin | 111 (30.1) | 132 (20.8) | 9 (20.0) | 16 (17.6) | ||
| TCHP | 122 (33.1) | 55 (8.7) | 19 (42.2) | 15 (16.5) | ||
| AC | 3 (0.8) | 5 (0.8) | 0 (0.0) | 4 (4.4) | ||
| cT stage at diagnosis | <0.001 | 0.671 | ||||
| 1 | 20 (5.4) | 26 (4.1) | 2 (4.4) | 3 (3.3) | ||
| 2 | 260 (70.5) | 381 (60.0) | 33 (73.3) | 59 (64.8) | ||
| 3 | 82 (22.2) | 181 (28.5) | 9 (20.0) | 24 (26.4) | ||
| 4 | 7 (1.9) | 47 (7.4) | 1 (2.2) | 5 (5.5) | ||
| cN stage at diagnosis | <0.001 | 0.901 | ||||
| 0 | 58 (15.7) | 58 (9.1) | 4 (8.9) | 6 (6.6) | ||
| 1 | 131 (35.5) | 193 (30.4) | 31 (68.9) | 60 (65.9) | ||
| 2 | 129 (35.0) | 228 (35.9) | 4 (8.9) | 10 (11.0) | ||
| 3 | 51 (13.8) | 156 (24.6) | 6 (13.3) | 15 (16.5) | ||
| Estrogen receptor | <0.001 | <0.001 | ||||
| Positive | 122 (33.1) | 329 (51.8) | 16 (35.6) | 64 (70.3) | ||
| Negative | 247 (66.9) | 306 (48.2) | 29 (64.4) | 27 (29.7) | ||
| Progesterone receptor | <0.001 | <0.001 | ||||
| Positive | 61 (16.5) | 258 (40.6) | 12 (26.7) | 55 (60.4) | ||
| Negative | 308 (83.5) | 377 (59.4) | 33 (73.3) | 36 (39.6) | ||
| HER2 | <0.001 | 0.003 | ||||
| Positive | 233 (63.1) | 187 (29.4) | 28 (62.2) | 31 (34.1) | ||
| Negative | 136 (36.9) | 448 (70.6) | 17 (37.8) | 60 (65.9) | ||
| Ki-67 | 0.007 | 0.012 | ||||
| ≥20% | 336 (91.1) | 539 (84.9) | 43 (95.6) | 72 (79.1) | ||
| <20% | 33 (8.9) | 96 (15.1) | 2 (4.4) | 19 (20.9) | ||
| Molecular subtype | <0.001 | <0.001 | ||||
| HR+/HER2− | 38 (10.3) | 236 (37.2) | 5 (11.1) | 45 (49.5) | ||
| HR+/HER2+ | 89 (24.1) | 105 (16.5) | 13 (28.9) | 20 (22.0) | ||
| HR−/HER2+ | 144 (39.0) | 82 (12.9) | 15 (33.3) | 11 (12.1) | ||
| HR−/HER2− | 98 (26.6) | 212 (33.4) | 12 (26.7) | 15 (16.5) | ||
| Menopausal status | 0.027 | >0.999 | ||||
| Postmenopausal | 170 (46.1) | 246 (38.7) | 24 (53.3) | 48 (52.7) | ||
| Premenopausal | 199 (53.9) | 389 (61.3) | 21 (46.7) | 43 (47.3) | ||
| Background parenchymal enhancement (BPE) | 0.579 | 0.465 | ||||
| 1 | 166(45.0) | 290(45.7) | 27 (60.0) | 43 (47.3) | ||
| 2 | 102 (27.6) | 156 (24.6) | 11 (24.4) | 26 (28.6) | ||
| 3 | 52 (14.1) | 88 (13.9) | 6 (13.3) | 15 (16.5) | ||
| 4 | 49 (13.3) | 101 (15.9) | 1 (2.2) | 7 (7.7) | ||
| Mammographic breast density | 0.788 | 0.695 | ||||
| 1 | 7 (1.9) | 11 (1.7) | 0 (0.0) | 1 (1.1) | ||
| 2 | 57 (15.4) | 114 (18.0) | 7 (15.6) | 13 (14.3) | ||
| 3 | 183 (49.6) | 305 (48.0) | 18 (40.0) | 45 (49.5) | ||
| 4 | 122 (33.1) | 205 (32.3) | 20 (44.4) | 32 (35.2) | ||
| Characteristics | Development Cohort | Validation Cohort | ||||
|---|---|---|---|---|---|---|
| Low (n = 608) | High (n = 396) | p-Value | Low (n = 81) | High (n = 55) | p-Value | |
| Age (median [IQR]) | 49.00 [42.00, 56.00] | 45.00 [38.00, 53.00] | <0.001 | 53.00 [48.00, 59.00] | 48.00 [43.00, 55.00] | 0.008 |
| Breast volume (cm3) (median [IQR]) | 509.50 [353.82, 717.03] | 664.70 [455.60, 904.62] | <0.001 | 628.36 [426.52, 806.93] | 684.99 [505.84, 1032.36] | 0.073 |
| Fat volume (cm3) (median [IQR]) | 384.16 [230.58, 550.14] | 477.44 [288.45, 687.47] | <0.001 | 455.51 [319.60, 593.58] | 535.64 [295.53, 822.07] | 0.178 |
| Normal fibroglandular tissue volume (cm3) (median [IQR]) | 115.10 [80.72, 158.67] | 147.88 [103.89, 202.52] | <0.001 | 121.35 [82.63, 164.36] | 152.97 [89.65, 227.67] | 0.063 |
| Tumor volume (cm3) (median [IQR]) | 8.01 [5.35, 12.07] | 23.82 [16.15, 35.74] | <0.001 | 7.08 [5.32, 11.64] | 22.04 [15.80, 32.68] | <0.001 |
| Operation method | ||||||
| Breast-conserving surgery | 442 (72.7) | 217 (54.8) | <0.001 | 65 (80.3) | 36 (65.5) | 0.053 |
| Mastectomy | 166 (27.3) | 179 (45.2) | 16 (19.7) | 19 (34.5) | ||
| BMI (median [IQR]) | 23.47 [21.61, 25.65] | 23.99 [21.82, 26.64] | 0.006 | 24.87 [22.49 26.73] | 25.20 [23.21 28.65] | 0.188 |
| BMI | ||||||
| <25 (kg/m2) | 420 (69.1) | 240 (60.6) | 0.007 | 42 (51.8) | 26 (47.3) | 0.600 |
| ≥25 (kg/m2) | 188 (30.9) | 156 (39.4) | 39 (48.2) | 29 (52.7) | ||
| NAC regimen | ||||||
| AC-T | 334 (54.9) | 242 (61.1) | 0.103 | 45 (55.5) | 28 (50.9) | 0.519 |
| AC-T/Herceptin | 157 (25.8) | 86 (21.7) | 17 (21.0) | 8 (45.6) | ||
| TCHP | 114 (18.8) | 63 (15.9) | 17 (21.0) | 17 (30.9) | ||
| AC | 3 (0.5) | 5 (1.3) | 2 (2.5) | 2 (3.6) | ||
| cT stage at diagnosis | ||||||
| 1 | 27 (4.4) | 19 (4.8) | <0.001 | 3 (3.7) | 2 (3.6) | 0.008 |
| 2 | 446 (73.4) | 195 (49.2) | 63 (77.8) | 29 (52.7) | ||
| 3 | 122 (20.1) | 141 (35.6) | 12 (14.8) | 21 (38.2) | ||
| 4 | 13 (2.1) | 41 (10.4) | 3 (3.7) | 3 (5.5) | ||
| cN stage at diagnosis | ||||||
| 0 | 76 (12.5) | 40 (10.1) | 0.107 | 7 (8.6) | 3 (5.5) | 0.633 |
| 1 | 206 (33.9) | 118 (29.8) | 55 (67.9) | 36 (65.4) | ||
| 2 | 214 (35.2) | 143 (36.1) | 9 (11.1) | 5 (9.1) | ||
| 3 | 112 (18.4) | 95 (24.0) | 10 (12.4) | 11 (20.0) | ||
| Estrogen receptor | ||||||
| Positive | 273 (44.9) | 178 (44.9) | >0.999 | 43 (53.1) | 37 (67.3) | 0.099 |
| Negative | 335 (55.1) | 218 (55.1) | 38 (46.9) | 18 (32.7) | ||
| Progesterone receptor | ||||||
| Positive | 191 (31.4) | 128 (32.3) | 0.816 | 34 (42.0) | 33 (60.0) | 0.039 |
| Negative | 417 (68.6) | 268 (67.7) | 47 (58.0) | 22 (40.0) | ||
| HER2 | ||||||
| Positive | 271 (44.6) | 149 (37.6) | 0.034 | 34 (42.0) | 25 (45.4) | 0.688 |
| Negative | 337 (55.4) | 247 (62.4) | 47 (58.0) | 30 (54.6) | ||
| Ki-67 | ||||||
| ≥20% | 524 (86.2) | 351 (88.6) | 0.299 | 66 (81.5) | 49 (89.1) | 0.228 |
| <20% | 84 (13.8) | 45 (11.4) | 15 (18.5) | 6 (10.9) | ||
| Molecular subtype | ||||||
| HR+/HER2− | 154 (25.3) | 120 (30.3) | 0.12 | 27 (33.3) | 23 (41.8) | 0.335 |
| HR+/HER2+ | 129 (21.2) | 65 (16.4) | 18 (22.2) | 15 (27.3) | ||
| HR−/HER2+ | 142 (23.4) | 84 (21.2) | 16 (19.8) | 10 (18.2) | ||
| HR−/HER2− | 183 (30.1) | 127 (32.1) | 20 (24.7) | 7 (12.7) | ||
| Menopausal status | ||||||
| Postmenopausal | 278 (45.7) | 138 (34.8) | 0.001 | 48 (59.3) | 24 (43.6) | 0.073 |
| Premenopausal | 330 (54.3) | 258 (65.2) | 33 (40.7) | 31 (56.4) | ||
| Background parenchymal enhancement (BPE) | ||||||
| 1 | 308 (50.7) | 148 (37.4) | <0.001 | 47 (58.0) | 23 (41.8) | 0.027 |
| 2 | 154 (25.3) | 104 (26.3) | 21 (25.9) | 16 (29.1) | ||
| 3 | 76 (12.5) | 64 (16.2) | 12 (14.8) | 9 (16.4) | ||
| 4 | 70 (11.5) | 80 (20.2) | 1 (1.2) | 7 (12.7) | ||
| Mammographic breast density | ||||||
| 1 | 10 (1.6) | 8 (2.0) | 0.439 | 2 (2.5) | 2 (3.6) | 0.960 |
| 2 | 108 (17.8) | 63 (15.9) | 12 (14.8) | 8 (14.6) | ||
| 3 | 303 (49.8) | 185 (46.7) | 37 (45.7) | 23 (41.8) | ||
| 4 | 187 (30.8) | 140 (35.4) | 30 (37.0) | 22 (40.0) | ||
| Pathologic response | ||||||
| pCR | 250 (41.1) | 119 (30.1) | <0.001 | 34 (42.0) | 11 (20.0) | 0.008 |
| Non-pCR | 358 (58.9) | 277 (69.9) | 47 (58.0) | 44 (80.0) | ||
| Variable | Univariable | Multivariable | ||||
|---|---|---|---|---|---|---|
| Odds Ratio | 95% CI | p-Value | Odds Ratio | 95% CI | p-Value | |
| Age | 0.986 | 0.973, 0.999 | 0.036 | 1.009 | 0.985, 1.033 | 0.478 |
| Breast volume (cm3) | 1.0002 | 0.9996, 1.0008 | 0.456 | |||
| Fat volume (cm3) | 1.0003 | 0.9995, 1.0010 | 0.719 | |||
| Normal fibroglandular tissue volume (cm3) | 1.0000 | 0.9979, 1.0020 | 0.496 | |||
| Tumor volume (cm3) | 1.0098 | 0.9990, 1.0206 | <0.001 | |||
| BMI | ||||||
| <25 (kg/m2) | Ref. | Ref | ||||
| ≥25 (kg/m2) | 0.952 | 0.727, 1.247 | 0.723 | 0.925 | 0.679, 1.258 | 0.618 |
| NAC regimen | <0.001 | |||||
| AC-T | Ref. | |||||
| AC-T/Herceptin | 0.357 | 0.260, 0.491 | <0.001 | |||
| TCHP | 0.135 | 0.093, 0.196 | <0.001 | |||
| AC | 0.500 | 0.118, 2.121 | 0.347 | |||
| cT stage at diagnosis | <0.001 | |||||
| 1 | Ref | Ref | ||||
| 2 | 1.127 | 0.616, 2.062 | 0.698 | 1.472 | 0.758, 2.856 | 0.253 |
| 3 | 1.698 | 0.896, 3.216 | 0.104 | 2.122 | 1.046, 4.306 | 0.037 |
| 4 | 5.165 | 1.929, 13.831 | 0.001 | 5.655 | 1.903, 16.808 | 0.002 |
| cN stage at diagnosis | <0.001 | |||||
| 0 | Ref | Ref | ||||
| 1 | 1.473 | 0.962, 2.256 | 0.075 | 1.271 | 0.793, 2.038 | 0.318 |
| 2 | 1.767 | 1.158, 2.699 | 0.008 | 1.555 | 0.973, 2.485 | 0.065 |
| 3 | 3.059 | 1.889, 4.954 | <0.001 | 2.237 | 1.304, 3.837 | 0.003 |
| Estrogen receptor | ||||||
| Positive | Ref | Ref | ||||
| Negative | 0.459 | 0.352, 0.600 | <0.001 | 0.892 | 0.606, 1.313 | 0.562 |
| Progesterone receptor | ||||||
| Positive | Ref | Ref | ||||
| Negative | 0.289 | 0.211, 0.397 | <0.001 | 0.268 | 0.169, 0.425 | <0.001 |
| HER2 | ||||||
| Positive | Ref | Ref | ||||
| Negative | 4.104 | 3.128, 5.386 | <0.001 | 5.002 | 3.691, 6.777 | <0.001 |
| Ki-67 | ||||||
| ≥20% | Ref | Ref | ||||
| <20% | 1.813 | 1.194, 2.755 | 0.005 | 1.521 | 0.932, 2.482 | 0.093 |
| Molecular subtype | <0.001 | |||||
| HR+/HER2− | Ref | <0.001 | ||||
| HR+/HER2+ | 0.190 | 0.122, 0.296 | <0.001 | |||
| HR−/HER2+ | 0.092 | 0.059, 0.142 | <0.001 | |||
| HR−/HER2− | 0.348 | 0.229, 0.529 | <0.001 | |||
| Menopausal status | ||||||
| Postmenopausal | Ref | Ref | ||||
| Premenopausal | 1.351 | 1.042, 1.751 | 0.023 | 0.889 | 0.561, 1.409 | 0.617 |
| Background parenchymal enhancement (BPE) | 0.580 | |||||
| 1 | Ref. | |||||
| 2 | 0.875 | 0.639, 1.199 | 0.407 | |||
| 3 | 0.969 | 0.654, 1.434 | 0.874 | |||
| 4 | 1.180 | 0.798, 1.744 | 0.407 | |||
| Mammographic breast density | 0.788 | |||||
| 1 | Ref | |||||
| 2 | 1.273 | 0.468, 3.458 | 0.636 | |||
| 3 | 1.061 | 0.404, 2.784 | 0.905 | |||
| 4 | 1.069 | 0.404, 2.831 | 0.893 | |||
| Tumor-fat interface volume | ||||||
| Low | Ref | Ref | ||||
| High | 1.626 | 1.242, 2.127 | <0.001 | 1.412 | 1.033, 1.929 | 0.030 |
| Variable | Univariable | Multivariable | ||||
|---|---|---|---|---|---|---|
| Odds Ratio | 95% CI | p-Value | Odds Ratio | 95% CI | p-Value | |
| Age | 1.0004 | 0.958, 1.044 | 0.985 | |||
| Breast volume (cm3) | 1.003 | 1.001, 1.005 | 0.154 | |||
| Fat volume (cm3) | 1.003 | 1.000, 1.005 | 0.139 | |||
| Normal fibroglandular tissue volume (cm3) | 1.004 | 0.998, 1.109 | 0.731 | |||
| Tumor volume (cm3) | 1.055 | 1.003, 1.109 | 0.104 | |||
| BMI | ||||||
| <25 (kg/m2) | Ref | |||||
| ≥25 (kg/m2) | 0.936 | 0.458, 1.912 | 0.855 | |||
| NAC regimen | 0.015 | |||||
| AC-T | Ref. | |||||
| AC-T/Herceptin | 0.540 | 0.202, 1.439 | 0.218 | |||
| TCHP | 0.240 | 0.101, 0.571 | 0.001 | |||
| AC | >999.999 | <0.001, >999.999 | 0.990 | |||
| cT stage at diagnosis | 0.658 | |||||
| 1 | Ref | |||||
| 2 | 1.192 | 0.189, 7.499 | 0.852 | |||
| 3 | 1.778 | 0.254, 12.450 | 0.562 | |||
| 4 | 3.333 | 0.204, 54.535 | 0.398 | |||
| cN stage at diagnosis | 0.902 | |||||
| 0 | Ref | |||||
| 1 | 1.290 | 0.339, 4.915 | 0.709 | |||
| 2 | 1.667 | 0.300, 9.272 | 0.560 | |||
| 3 | 1.667 | 0.343, 8.093 | 0.526 | |||
| Estrogen receptor | ||||||
| Positive | Ref | Ref | ||||
| Negative | 0.233 | 0.109, 0.497 | <0.001 | 0.302 | 0.092, 0.995 | 0.049 |
| Progesterone receptor | ||||||
| Positive | Ref | Ref | ||||
| Negative | 0.238 | 0.109, 0.521 | <0.001 | 0.838 | 0.245, 2.870 | 0.778 |
| HER2 | ||||||
| Positive | Ref | Ref | ||||
| Negative | 3.188 | 1.517, 6.697 | 0.002 | 3.481 | 1.482, 8.173 | 0.004 |
| Ki-67 | ||||||
| ≥20% | Ref | Ref | ||||
| <20% | 5.674 | 1.260, 25.556 | 0.024 | 5.463 | 0.997, 29.948 | 0.050 |
| Molecular subtype | 0.001 | |||||
| HR+/HER2− | Ref | |||||
| HR+/HER2+ | 0.171 | 0.054, 0.544 | 0.003 | |||
| HR−/HER2+ | 0.081 | 0.024, 0.273 | <0.001 | |||
| HR−/HER2− | 0.139 | 0.042, 0.459 | 0.001 | |||
| Menopausal status | ||||||
| Postmenopausal | Ref | |||||
| Premenopausal | 1.024 | 0.500, 2.095 | 0.949 | |||
| Background parenchymal enhancement (BPE) | 0.448 | |||||
| 1 | Ref. | |||||
| 2 | 1.484 | 0.632, 3.485 | 0.365 | |||
| 3 | 1.570 | 0.543, 4.540 | 0.405 | |||
| 4 | 4.395 | 0.512, 37.729 | 0.177 | |||
| Mammographic breast density | 0.735 | |||||
| 1 | Ref | |||||
| 2 | <0.001 | <0.001, >999.999 | 0.987 | |||
| 3 | <0.001 | <0.001, >999.999 | 0.988 | |||
| 4 | <0.001 | <0.001, >999.999 | 0.987 | |||
| Tumor-fat interface volume | ||||||
| Low | Ref | Ref | ||||
| High | 2.894 | 1.307, 6.405 | 0.009 | 3.488 | 1.403, 8.675 | 0.007 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, H.-h.; Park, M.; Park, H.; Ko, E.S.; Hwang, N.Y.; Im, Y.-H.; Ko, K.; Sim, S.H. The Tumor–Fat Interface Volume of Breast Cancer on Pretreatment MRI Is Associated with a Pathologic Response to Neoadjuvant Chemotherapy. Biology 2020, 9, 391. https://doi.org/10.3390/biology9110391
Cho H-h, Park M, Park H, Ko ES, Hwang NY, Im Y-H, Ko K, Sim SH. The Tumor–Fat Interface Volume of Breast Cancer on Pretreatment MRI Is Associated with a Pathologic Response to Neoadjuvant Chemotherapy. Biology. 2020; 9(11):391. https://doi.org/10.3390/biology9110391
Chicago/Turabian StyleCho, Hwan-ho, Minsu Park, Hyunjin Park, Eun Sook Ko, Na Young Hwang, Young-Hyuck Im, Kyounglan Ko, and Sung Hoon Sim. 2020. "The Tumor–Fat Interface Volume of Breast Cancer on Pretreatment MRI Is Associated with a Pathologic Response to Neoadjuvant Chemotherapy" Biology 9, no. 11: 391. https://doi.org/10.3390/biology9110391
APA StyleCho, H.-h., Park, M., Park, H., Ko, E. S., Hwang, N. Y., Im, Y.-H., Ko, K., & Sim, S. H. (2020). The Tumor–Fat Interface Volume of Breast Cancer on Pretreatment MRI Is Associated with a Pathologic Response to Neoadjuvant Chemotherapy. Biology, 9(11), 391. https://doi.org/10.3390/biology9110391