
Neuromuscular and Biomechanical Jumping and Landing Deficits in Young Female Handball Players


 , ,
, ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Measurements
2.3.1. Single Leg Countermovement Jump
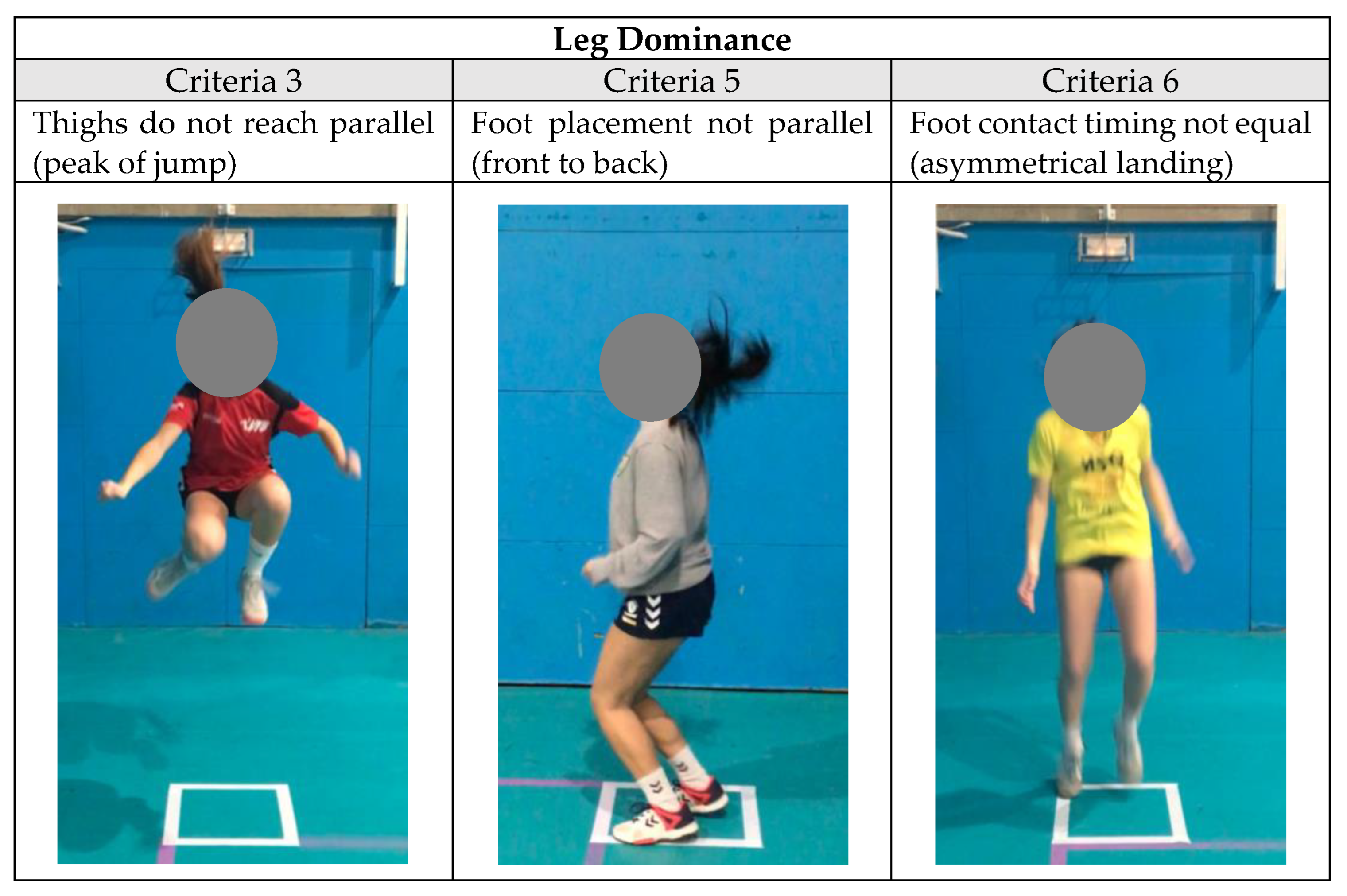
2.3.2. Tuck Jump Assessment
2.4. Statistical Analysis
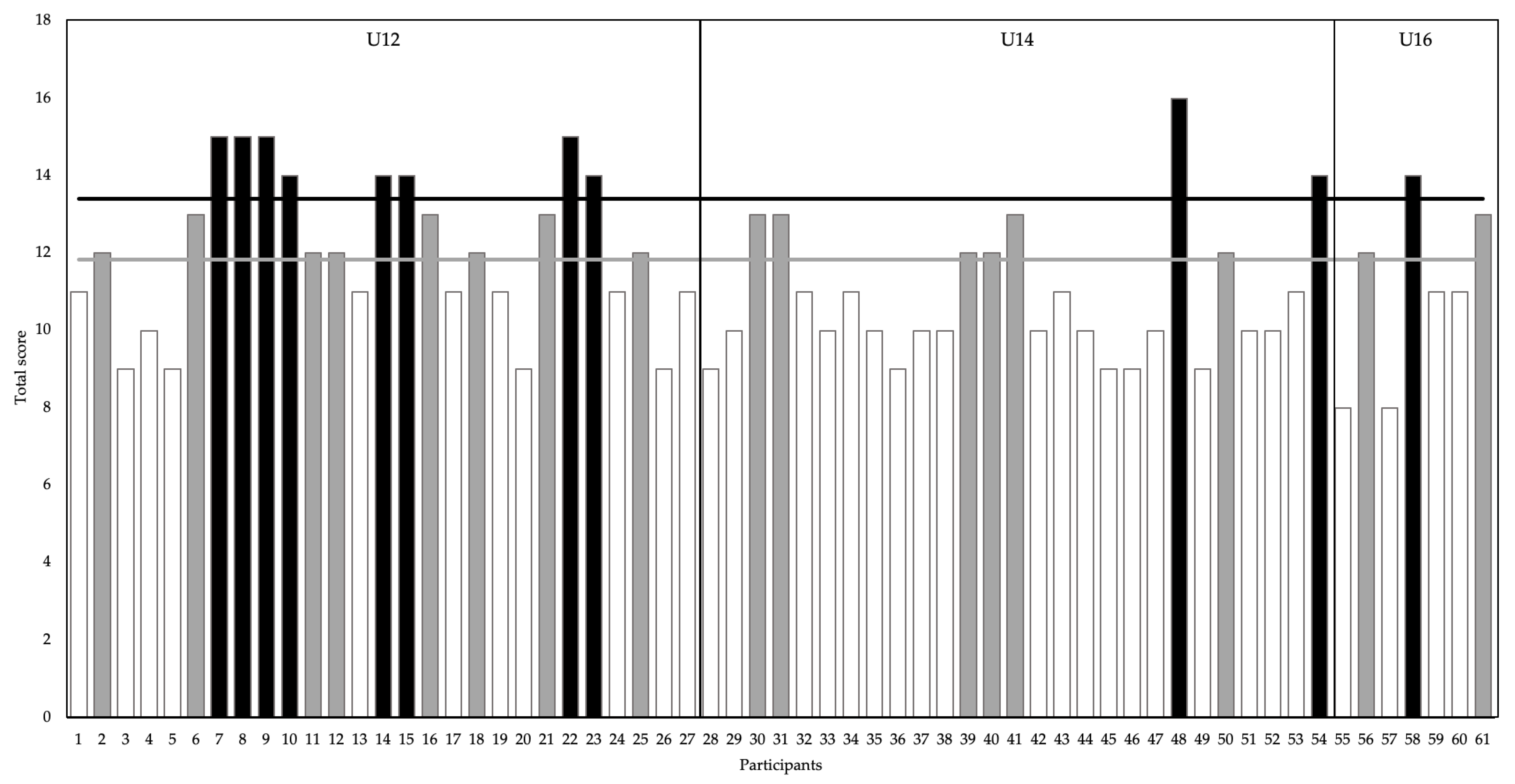
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lie, M.M.; Risberg, M.A.; Storheim, K.; Engebretsen, L.; Øiestad, B.E. What’s the rate of knee osteoarthritis 10 years after anterior cruciate ligament injury? An updated systematic review. Br. J. Sports Med. 2019, 53, 1162–1167. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.C.H.; Ardern, C.L.; Feller, J.A.; Webster, K.E. Eighty-three per cent of elite athletes return to preinjury sport after anterior cruciate ligament reconstruction: A systematic review with meta-analysis of return to sport rates, graft rupture rates and performance outcomes. Br. J. Sports Med. 2018, 52, 128–138. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, S.; Nagano, Y.; Ito, W.; Kido, Y.; Okuwaki, T. A retrospective study of mechanisms of anterior cruciate ligament injuries in high school basketball, handball, judo, soccer, and volleyball. Medicine 2019, 98, e16030. [Google Scholar] [CrossRef] [PubMed]
- Fort-Vanmeerhaeghe, A.; Romero, D. Análisis de los factores de riesgo neuromusculares de las lesiones deportivas. Apunt. Med. l’Esport 2013, 48, 109–120. [Google Scholar] [CrossRef]
- Hewett, T.E.; Myer, G.D.; Ford, K.R. Decrease in neuromuscular control about the knee with maturation in female athletes. J. Bone Jt. Surg. 2004, 86, 1601–1608. [Google Scholar] [CrossRef] [PubMed]
- Myer, G.D. Real-Time Assessment and Neuromuscular Training Feedback Techniques to Prevent Anterior Cruciate Ligament Injury in Female Athletes. Strength Cond. J. 2011, 33, 21. [Google Scholar] [CrossRef]
- Fort-Vanmeerhaeghe, A.; Benet, A.; Miranda, S.; Montalvo, A.M.; Myer, G.D.; Mirada, S.; Montalvo, A.M.; Myer, G.D. Sex and maturation differences in performance of functional jumping and landing deficits in youth athletes. J. Sport Rehabil. 2018, 28, 606–613. [Google Scholar] [CrossRef]
- Bencke, J.; Aagaard, P.; Zebis, M.K. Muscle Activation During ACL Injury Risk Movements in Young Female Athletes: A Narrative Review. Front. Physiol. 2018, 9, 445. [Google Scholar] [CrossRef]
- Chia, L.; De Oliveira, D.; Matthew, S.; Mckay, M.J.; Sullivan, J.; Fuller, C.W.; Pappas, E. Non-contact Anterior Cruciate Ligament Injury Epidemiology in Team—Ball Sports: A Systematic Review with Meta-analysis by Sex, Age, Sport, Participation Level, and Exposure Type. Sport. Med. 2022, 52, 2447–2467. [Google Scholar] [CrossRef]
- Hewett, T.E. Neuromuscular and Hormonal Factors Associated With Knee Injuries in Female Athletes. Sport. Med. 2000, 29, 313–327. [Google Scholar] [CrossRef]
- Leppanen, M.; Pasanen, K.; Kujala, U.M.; Vasankari, T.; Kannus, P.; Ayramo, S.; Krosshaug, T.; Bahr, R.; Avela, J.; Perttunen, J.; et al. Stiff Landings Are Associated With Increased ACL Injury Risk in Young Female Basketball and Floorball Players. Am. J. Sports Med. 2017, 45, 386–393. [Google Scholar] [CrossRef] [PubMed]
- DiStefano, L.J.; Martinez, J.C.; Crowley, E.; Matteau, E.; Kerner, M.S.; Boling, M.C.; Nguyen, A.D.; Trojian, T.H. Maturation and sex differences in neuromuscular characteristics of youth athletes. J. Strength Cond. Res. 2015, 29, 2465–2473. [Google Scholar] [CrossRef] [PubMed]
- Nasseri, A.; Lloyd, D.G.; Minahan, C.; Sayer, T.A.; Paterson, K.; Vertullo, C.J.; Bryant, A.L.; Saxby, D.J. Effects of Pubertal Maturation on ACL Forces During a Landing Task in Females. Am. J. Sports Med. 2021, 49, 3322–3334. [Google Scholar] [CrossRef] [PubMed]
- Pedley, J.S.; Lloyd, R.S.; Read, P.J.; Moore, I.S.; Ste, M. De Utility of Kinetic and Kinematic Jumping and Landing Variables as Predictors of Injury Risk: A Systematic Review. J. Sci. Sport Exerc. 2020, 2, 287–304. [Google Scholar] [CrossRef]
- Fort-Vanmeerhaeghe, A.; Milà-Villarroel, R.; Pujol-Marzo, M.; Arboix-Alió, J.; Bishop, C. Higher Vertical Jumping Asymmetries and Lower Physical Performance are Indicators of Increased Injury Incidence in Youth Team-Sport Athletes. J. Strength Cond. Res. 2020, 36, 2204–2211. [Google Scholar] [CrossRef]
- King, E.; Richter, C.; Franklyn-Miller, A.; Wadey, R.; Moran, R.; Strike, S. Back to Normal Symmetry? Biomechanical Variables Remain More Asymmetrical Than Normal During Jump and Change-of-Direction Testing 9 Months After Anterior Cruciate Ligament Reconstruction. Am. J. Sports Med. 2019, 47, 1175–1185. [Google Scholar] [CrossRef]
- Madruga-Parera, M.; Bishop, C.; Read, P.; Lake, J.; Brazier, J.; Romero-Rodriguez, D. Jumping-based Asymmetries are Negatively Associated with Jump, Change of Direction, and Repeated Sprint Performance, but not Linear Speed, in Adolescent Handball Athletes. J. Hum. Kinet. 2020, 71, 47–58. [Google Scholar] [CrossRef]
- Bishop, C.; Read, P.; Chavda, S.; Jarvis, P.; Turner, A. Using Unilateral Strength, Power and Reactive Strength Tests to Detect the Magnitude and Direction of Asymmetry: A Test-Retest Design. Sports 2019, 7, 58. [Google Scholar] [CrossRef]
- Myer, G.D.; Ford, K.R.; Hewett, T.E. Tuck Jump Assessment for Reducing Anterior Cruciate Ligament Injury Risk. Athl. Ther. Today 2008, 13, 39–44. [Google Scholar] [CrossRef]
- Read, P.J.; Oliver, J.L.; De Ste Croix, M.B.A.; Myer, G.D.; Lloyd, R.S. Reliability of the Tuck Jump injury risk screening assessment in elite male youth soccer players. J. Strength Cond. Res. 2015, 30, 1510–1516. [Google Scholar] [CrossRef]
- Arundale, A.J.H.H.; Kvist, J.; Hagglund, M.; Faltstrom, A.; Hägglund, M.; Fältström, A. Jump performance in male and female football players. Knee Surg. Sport. Traumatol. Arthrosc. 2020, 28, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Benet-Vigo, A.; Arboix-Alió, J.; Montalvo, A.M.; Myer, G.; Fort-Vanmeerhaeghe, A. Detección de déficits neuromusculares a través del análisis del patrón de salto y aterrizaje en deportistas adolescentes. Cuad. Psicol. Deport. 2021, 21, 224–232. [Google Scholar] [CrossRef]
- Mirwald, R.L.; Baxter-Jones, A.D.G.; Bailey, D.A.; Beunen, G.P. An assessment of maturity from anthropometric measurements. Med. Sci. Sports Exerc. 2002, 34, 689–694. [Google Scholar] [CrossRef] [PubMed]
- Sherar, L.B.; Mirwald, R.L.; Baxter-Jones, A.D.G.; Thomis, M. Prediction of adult height using maturity-based cumulative height velocity curves. J. Pediatr. 2005, 147, 508–514. [Google Scholar] [CrossRef]
- Jeffreys, I. El Calentamiento. Maximizar el Rendimiento y Mejorar el Desarrollo Físico a Largo Plazo; Ediciones Tutor, S.A.: Madrid, Spain, 2019. [Google Scholar]
- Bosco, C.; Luhtanen, P.; Komi, P.V. A simple method for measurement of mechanical power in jumping. Eur. J. Appl. Physiol. 1983, 50, 271–282. [Google Scholar] [CrossRef]
- Read, P.J.; Oliver, J.L.; Myer, G.D.; De Ste Croix, M.B.A.; Lloyd, R.S. The Effects of Maturation on Measures of Asymmetry During Neuromuscular Control Tests in Elite Male Youth Soccer Players. Pediatr. Exerc. Sci. 2017, 30, 168–175. [Google Scholar] [CrossRef]
- Meylan, C.; McMaster, T.; Cronin, J.; Mohammad, N.I.; Rogers, C.; Deklerk, M. Single-leg lateral, horizontal, and vertical jump assessment: Reliability, interrelationships, and ability to predict sprint and change-of-direction performance. J. Strength Cond. Res. 2009, 23, 1140–1147. [Google Scholar] [CrossRef]
- Sommerfield, L.M.; Harrison, C.B.; Whatman, C.S.; Maulder, P.S. Relationship Between Strength, Athletic Performance, and Movement Skill in Adolescent Girls. J. Strength Cond. Res. 2022, 36, 674–679. [Google Scholar] [CrossRef]
- Fort-Vanmeerhaeghe, A.; Montalvo, A.M.; Lloyd, R.S.; Read, P.; Myer, G.D. Intra- and Inter-Rater Reliability of the Modified Tuck Jump Assessment. J. Sports Sci. Med. 2017, 16, 117–124. [Google Scholar]
- Myer, G.D.; Ford, K.R.; Hewettt, T.E. Rationale and Clinical Techniques for Anterior Cruciate Ligament Injury Prevention Among Female Athletes. J. Athl. Train. 2004, 39, 352–364. [Google Scholar]
- Viera, A.J.; Garrett, J.M. Understanding interobserver agreement: The kappa statistic. Fam. Med. 2005, 37, 360–363. [Google Scholar]
- Turner, A.; Cscs, D.; Brazier, J.; Bishop, C.; Chavda, S.; Cree, J.; Read, P. Data analysis for strength and conditioning coaches: Using excel to analyze reliability, differences, and relationships. Strength Cond. J. 2015, 37, 76–83. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Dos’Santos, T.; Thomas, C.; Jones, P.A. Assessing Interlimb Asymmetries: Are We Heading in the Right Direction? Strength Cond. J. 2020, 43, 91–100. [Google Scholar] [CrossRef]
- Bishop, C.; Read, P.; Lake, J.; Chavda, S.; Turner, A. Interlimb asymmetries: Understanding how to calculate differences from bilateral and unilateral tests. Strength Cond. J. 2018, 40, 1–6. [Google Scholar] [CrossRef]
- Read, P.J.; Oliver, J.L.; De Ste Croix, M.B.A.; Myer, G.D.; Lloyd, R.S. Landing kinematics in elite male youth soccer players of different chronologic ages and stages of maturation. J. Athl. Train. 2018, 53, 372–378. [Google Scholar] [CrossRef] [PubMed]
- Turner, A.; Jones, B.; Stewart, P.; Bishop, C.; Parmar, N.; Chavda, S.; Read, P. Total Score of Athleticism: Holistic Athlete Profiling to Enhance Decision-Making. Strength Cond. J. 2019, 41, 91–101. [Google Scholar] [CrossRef]
- Hewett, T.E.; Myer, G.D.; Ford, K.R.; Heidt, R.S.; Colosimo, A.J.; McLean, S.G.; Van Den Bogert, A.J.; Paterno, M.V.; Succop, P. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: A prospective study. Am. J. Sports Med. 2005, 33, 492–501. [Google Scholar] [CrossRef]
- Ford, K.R.; Myer, G.D.; Hewett, T.E. Valgus knee motion during landing in high school female and male basketball players. Med. Sci. Sports Exerc. 2003, 35, 1745–1750. [Google Scholar] [CrossRef]
- Myer, G.D.; Ford, K.R.; Brent, J.L.; Hewett, T.E. Differential neuromuscular training effects onACL injury risk factors in”high-risk” versus “low-risk” athletes. BMC Musculoskelet. Disord. 2007, 8, 39. [Google Scholar] [CrossRef]
- Maloney, S. The relationship between asymmetry and athletic performance: A critical review. J. Strength Cond. Res. 2019, 33, 2579–2593. [Google Scholar] [CrossRef] [PubMed]
- Lininger, M.R.; Smith, C.A.; Chimera, N.J.; Hoog, P.; Warren, M. Tuck Jump Assessment: An Exploratory Factor Analysis in a College Age Population. J. Strength Cond. Res. 2015, 31, 653–659. [Google Scholar] [CrossRef] [PubMed]
- Bishop, C.; Lake, J.; Loturco, I.; Papadopoulos, K.; Turner, A.; Read, P. Interlimb Asymmetries: The Need For An Individual Approach To Data Analysis. J. Strength Cond. Res. 2018, 35, 695–701. [Google Scholar] [CrossRef]
- Lockie, R.G.; Callaghan, S.J.; Berry, S.P.; Cooke, E.R.A.; Jordan, C.A.; Luczo, T.M.; Jeffriess, M.D. Relationship between unilateral jumping ability and asymmetry on multidirectional speed in team-sport athletes. J. Strength Cond. Res. 2014, 28, 3557–3566. [Google Scholar] [CrossRef] [PubMed]
- Arboix-Alió, J.; Bishop, C.; Benet, A.; Buscà, B.; Aguilera-Castells, J.; Fort-Vanmeerhaeghe, A. Assessing the Magnitude and Direction of Asymmetry in Unilateral Jump and Change of Direction Speed Tasks in Youth Female Team-Sport Athletes. J. Hum. Kinet. 2021, 79, 15–27. [Google Scholar] [CrossRef]
- Pullen, B.J.; Oliver, J.L.; Lloyd, R.S.; Knight, C.J. Relationships between Athletic Motor Skill Competencies and Maturity, Sex, Physical Performance, and Psychological Constructs in Boys and Girls. Children 2022, 9, 375. [Google Scholar] [CrossRef]
- Kotsifaki, A.; Korakakis, V.; Graham-Smith, P.; Sideris, V.; Whiteley, R. Vertical and Horizontal Hop Performance: Contributions of the Hip, Knee, and Ankle. Sports Health 2021, 13, 128–135. [Google Scholar] [CrossRef]
- Cadens, M.; Planas Anzano, A.; Matas-García, S.; Peirau Terés, X. Preventive Training of Anterior Cruciate Ligament Injuries in Female Handball Players: A Systematic Review. Apunt. Educ. Física Esports 2021, 146, 68–77. [Google Scholar]
- Bedoya, A.A.; Miltenberger, M.R.; Lopez, R.M. Plyometric Training Effects On Athletic Performance In Youth Soccer Athletes: A Systematic Review. J. Strength Cond. Res. 2015, 29, 2351–2360. [Google Scholar] [CrossRef]
- Ford, P.; de Ste Croix, M.; Lloyd, R.; Meyers, R.; Moosavi, M.; Oliver, J.; Till, K.; Williams, C. The Long-Term Athlete Development model: Physiological evidence and application. J. Sports Sci. 2011, 29, 389–402. [Google Scholar] [CrossRef]
- Fort-Vanmeerhaeghe, A.; Romero-Rodriguez, D.; Lloyd, R.S.; Kushner, A.; Myer, G.D. Integrative Neuromuscular Training in Youth Athletes. Part II: Strategies to Prevent Injuries and Improve Performance. Strength Cond. J. 2016, 38, 9–27. [Google Scholar] [CrossRef]
- Lloyd, R.S.; Oliver, J.L. The youth physical development model: A new approach to long-term athletic development. Strength Cond. J. 2012, 34, 61–72. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total (n = 61) | U12 (n = 27) | U14 (n = 27) | U16 (n = 7) | |
|---|---|---|---|---|
| Chronological age (years) | 14.3 ± 1.5 | 13 ± 1 | 15.1 ± 0.62 | 16.6 ± 0.3 |
| Years of PHV 1 | 1.63 ± 1.09 | 0.79 ± 0.95 | 2.11 ± 0.48 | 3.01 ± 0.68 |
| Pre-PHV 2 | 2 (3.23%) | 2 (7%) | ||
| Circa-PHV 2 | 10 (16.39%) | 10 (37%) | ||
| Post-PHV 2 | 49 (80.33%) | 15 (56%) | 27 (100%) | 7 (100%) |
| Experience (years) | 4.71 ± 2.50 | 4.14 ± 2.52 | 4.82 ± 2.51 | 6.43 ± 1.62 |
| Body mass (kg) | 54.34± 6.9 | 51.3 ± 10.7 | 55.9 ± 7.8 | 59.8 ± 9.1 |
| Height (m) | 1.59 ± 0.07 | 1.58 ± 0.07 | 1.60 ± 0.05 | 1.62 ± 0.11 |
| BMI (kg/m2) | 21.32 ± 3.12 | 20.56 ± 3.57 | 21.71 ± 2.67 | 22.72 ± 2.38 |
| Criterion | None (0) | Small (1) | Large (2) |
|---|---|---|---|
| (1) Lower extremity valgus at landing | No valgus | Slight valgus | Both knees touch |
| (2) Thighs do not reach parallel (peak of jump) | The knees are higher or at the same level as the hips | The middle of the knees are at a lower level than the middle of the hips | The whole knees are under the entire hips |
| (3) Thighs not equal side-to-side during flight | Thighs equal side to side | Thighs slightly unequal side-to-side | Thighs completely unequal side-to-side (one knee us over the other) |
| (4) Foot placement not shoulder width apart | Foot placement exactly shoulder width apart | Foot placement mostly shoulder width apart | Both feet fully together and touch at landing |
| (5) Foot placement not parallel (front to back) | Foot (the end of the feet) placement parallel | Foot placement mostly parallel | Foot placement obviously unparalleled (one foot is over half the distance of the other foot/leg) |
| (6) Foot contact timing not equal (asymmetrical landing) | Foot contact timing equal side-to-side | Foot contact timing slightly unequal | Foot contact timing completely unequal |
| (7) Excessive landing contact noise | Subtle noise at landing (landing on the balls of their feet) | Audible noise at landing (heels almost touch the ground at landing) | Loud and pronounced noise at landing (contact of the entire foot and heel on the ground between jumps) |
| (8) Pause between jumps | Reactive and reflex jumps | Small pause between jumps | Large pause between jumps (or double contact between jumps) |
| (9) Technique declines prior to ten seconds | No decline in technique | Technique declines after five seconds | Technique declines before five seconds |
| (10) Does not land in same foot print (consistent point of landing) | Lands in same footprint | Does not land in same footprint, but inside the shape | Lands outside the shape |
| Criterion | Kappa Value |
|---|---|
| 0.86 |
| 0.86 |
| 0.75 |
| 0.77 |
| 0.72 |
| 0.67 |
| 0.64 |
| 0.83 |
| 0.65 |
| 0.88 |
| U12 (n = 27) | U14 (n = 27) | U16 (n = 7) | ||||
|---|---|---|---|---|---|---|
| CV (%) | ICC (95% IC) | CV (%) | ICC (95% IC) | CV (%) | ICC (95% IC) | |
| SL-CMJL | 12.88 | 0.82 (0.66–0.91) | 8.22 | 0.96 (0.92–0.98) | 10.58 | 0.64 (−0.01–0.93) |
| SL-CMJR | 10.7 | 0.89 (0.79–0.95) | 7.48 | 0.96 (0.92–0.98) | 5.82 | 0.95 (0.83–0.99) |
| TJA | 4.78 | 0.92 (0.82–0.96) | 5.34 | 0.92 (0.83–0.97) | 4.61 | 0.95 (0.76–0.99) |
| C | U12 (n = 27) | U14 (n = 27) | U16 (n = 7) | p | χ2 | V | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 0 | 1 | 2 | 0 | 1 | 2 | ||||
| 1 | 0 | 0 | 27 | 0 | 8 | 19 | 1 | 1 | 5 | 0.002 * | 17.31 | 0.38 |
| 0% | 0% | 100% | 0% | 30% | 70% | 14% | 14% | 71% | ||||
| 2 | 5 | 8 | 14 | 9 | 11 | 7 | 0 | 3 | 4 | 0.172 | 6.39 | 0.23 |
| 19% | 30% | 52% | 33% | 41% | 26% | 0% | 43% | 57% | ||||
| 3 | 0 | 20 | 7 | 0 | 16 | 11 | 0 | 4 | 3 | 0.458 | 1.56 | 0.16 |
| 0% | 74% | 26% | 0% | 59% | 41% | 0% | 57% | 43% | ||||
| 4 | 3 | 16 | 8 | 2 | 19 | 6 | 0 | 7 | 0 | 0.358 | 4.37 | 0.19 |
| 11% | 59% | 30% | 7% | 70% | 22% | 0% | 100% | 0% | ||||
| 5 | 0 | 19 | 8 | 0 | 24 | 3 | 0 | 5 | 2 | 0.222 | 3.01 | 0.22 |
| 0% | 70% | 30% | 0% | 89% | 11% | 0% | 71% | 29% | ||||
| 6 | 6 | 20 | 1 | 8 | 19 | 0 | 2 | 3 | 2 | 0.033 * | 10.47 | 0.29 |
| 22% | 74% | 4% | 30% | 70% | 0% | 29% | 43% | 29% | ||||
| 7 | 0 | 10 | 17 | 0 | 19 | 8 | 0 | 6 | 1 | 0.013 * | 8.73 | 0.38 |
| 0% | 37% | 63% | 0% | 70% | 30% | 0% | 86% | 14% | ||||
| 8 | 16 | 11 | 0 | 17 | 10 | 0 | 7 | 0 | 0 | 0.120 | 4.23 | 0.26 |
| 59% | 41% | 0% | 63% | 37% | 0% | 100% | 0% | 0% | ||||
| 9 | 0 | 24 | 3 | 0 | 23 | 4 | 1 | 5 | 1 | 0.089 | 8.06 | 0.26 |
| 0% | 89% | 11% | 0% | 85% | 15% | 14% | 71% | 14% | ||||
| 10 | 0 | 25 | 2 | 0 | 25 | 2 | 0 | 7 | 0 | 0.758 | 0.56 | 0.10 |
| 0% | 93% | 7% | 0% | 93% | 7% | 0% | 100% | 0% | ||||
| Total (n = 61) | U12 (n = 27) | U14 (n = 27) | U16 (n = 7) | |
|---|---|---|---|---|
| SL-CMJL | 13.85 ± 2.92 | 13.52 ± 2.53 | 14.07 ± 3.58 | 14.29 ± 1.04 |
| SL-CMJR | 13.36 ± 2.92 | 13.48 ± 2.69 | 13.36 ± 3.33 | 12.94 ± 2.37 |
| ASIM SL-CMJ (%) | 12.05 ± 8.29 | 11.55 ± 9.29 | 11.80 ± 8.05 | 14.88 ± 4.77 |
| TJA | 11.44 ± 1.97 | 12.11 ± 1.97 | 10.89 ± 1.74 | 11 ± 2.31 |
| ASIM TJA | 3.34 ± 0.89 | 3.37 ± 0.93 | 3.22 ± 0.80 | 3.71 ± 1.11 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cadens, M.; Planas-Anzano, A.; Peirau-Terés, X.; Benet-Vigo, A.; Fort-Vanmeerhaeghe, A. Neuromuscular and Biomechanical Jumping and Landing Deficits in Young Female Handball Players. Biology 2023, 12, 134. https://doi.org/10.3390/biology12010134
Cadens M, Planas-Anzano A, Peirau-Terés X, Benet-Vigo A, Fort-Vanmeerhaeghe A. Neuromuscular and Biomechanical Jumping and Landing Deficits in Young Female Handball Players. Biology. 2023; 12(1):134. https://doi.org/10.3390/biology12010134
Chicago/Turabian StyleCadens, Maria, Antoni Planas-Anzano, Xavier Peirau-Terés, Ariadna Benet-Vigo, and Azahara Fort-Vanmeerhaeghe. 2023. "Neuromuscular and Biomechanical Jumping and Landing Deficits in Young Female Handball Players" Biology 12, no. 1: 134. https://doi.org/10.3390/biology12010134
APA StyleCadens, M., Planas-Anzano, A., Peirau-Terés, X., Benet-Vigo, A., & Fort-Vanmeerhaeghe, A. (2023). Neuromuscular and Biomechanical Jumping and Landing Deficits in Young Female Handball Players. Biology, 12(1), 134. https://doi.org/10.3390/biology12010134