
Knee Flexor Eccentric Strength, Hamstring Muscle Volume and Sprinting in Elite Professional Soccer Players with a Prior Strained Hamstring

 ,
,  , , and
, , and
Abstract
:Simple Summary
Abstract

1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.3. Imaging Technique and Hamstring Muscle Volume
2.4. Eccentric Knee Flexor Strength
2.5. Sprinting Performance
2.6. Retrospectively HSI Reporting
2.7. Statistical Analyses
3. Results
3.1. Players and Prior Injury Details
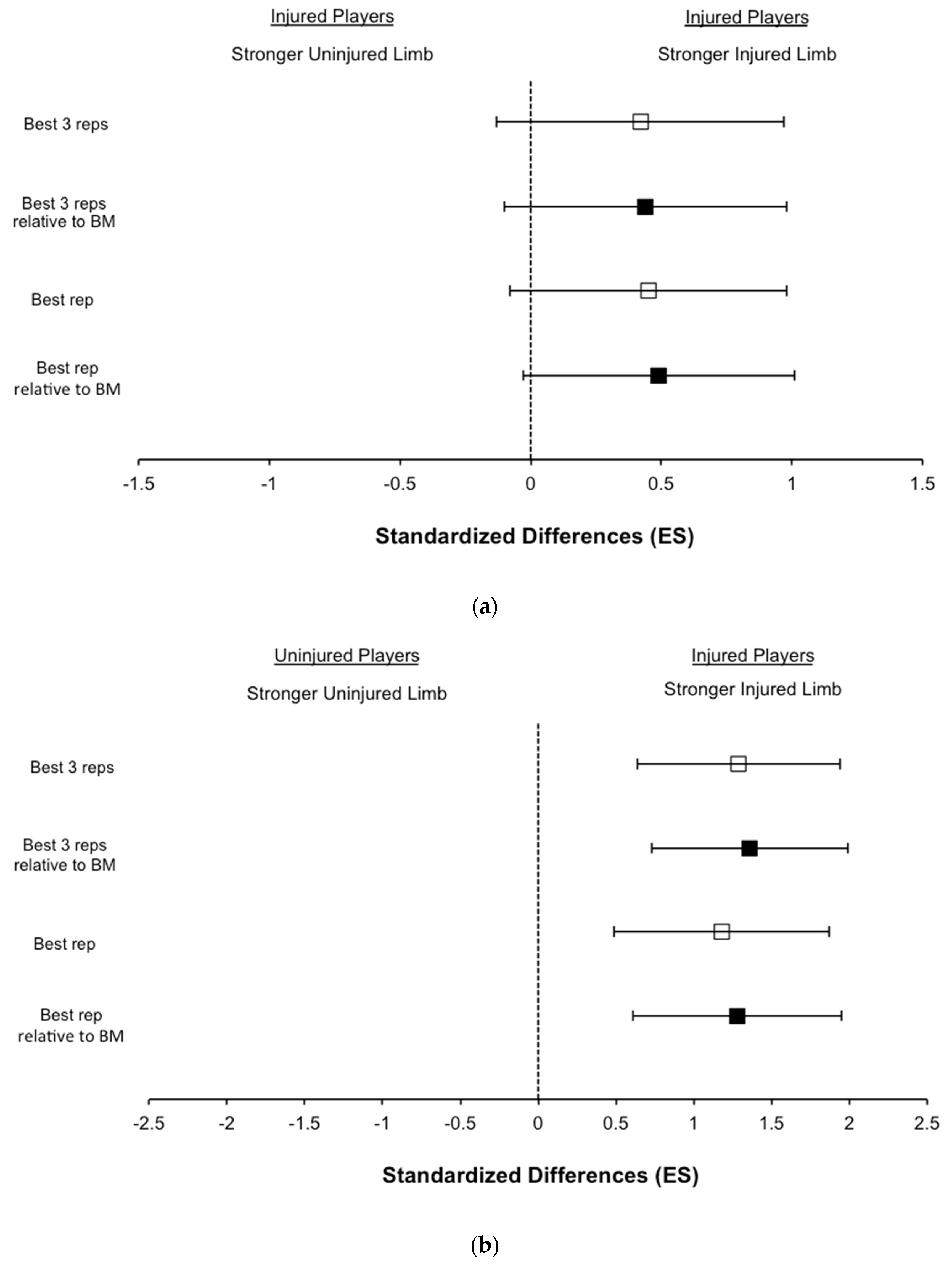
3.2. Eccentric Knee Flexor Strength
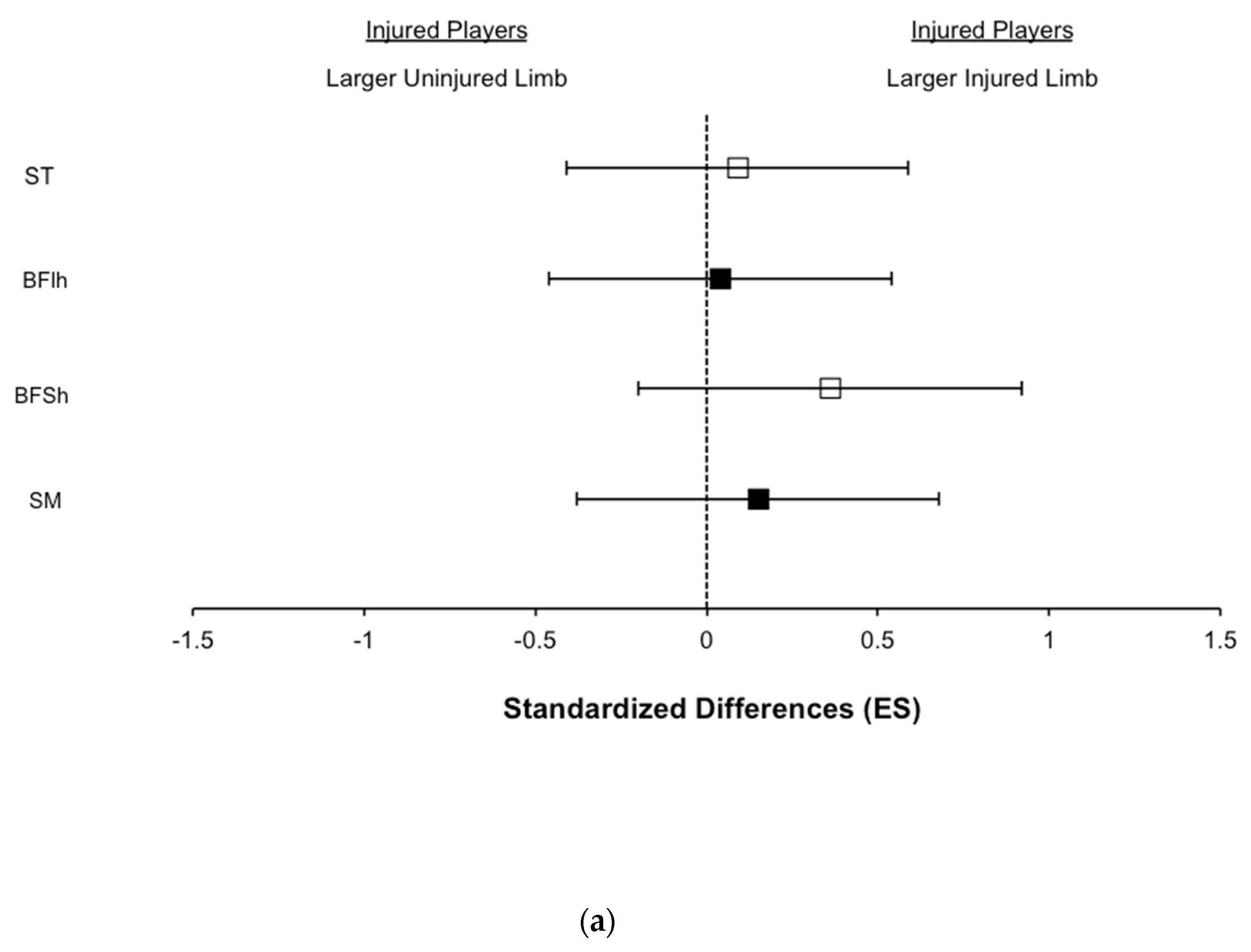
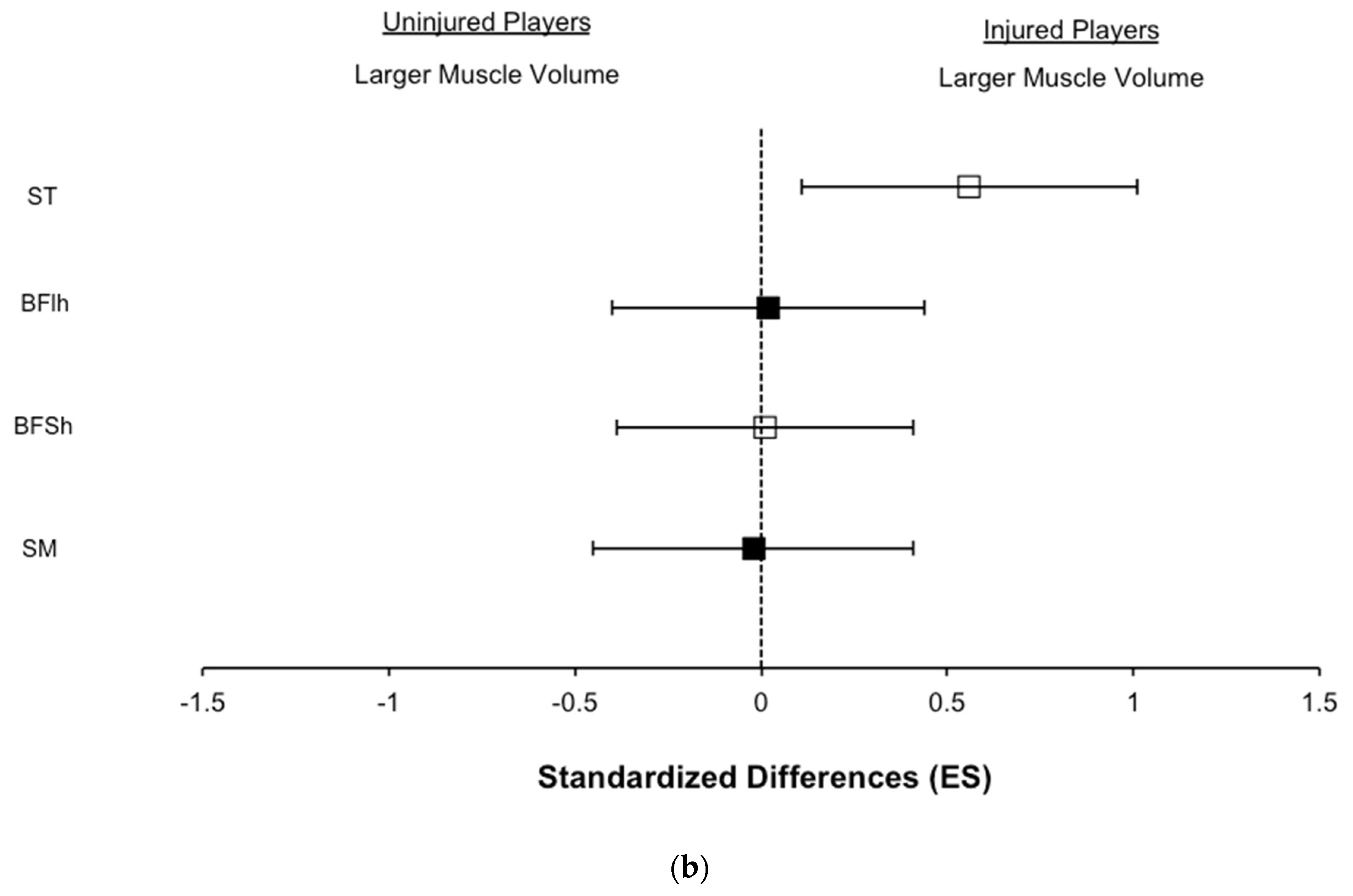
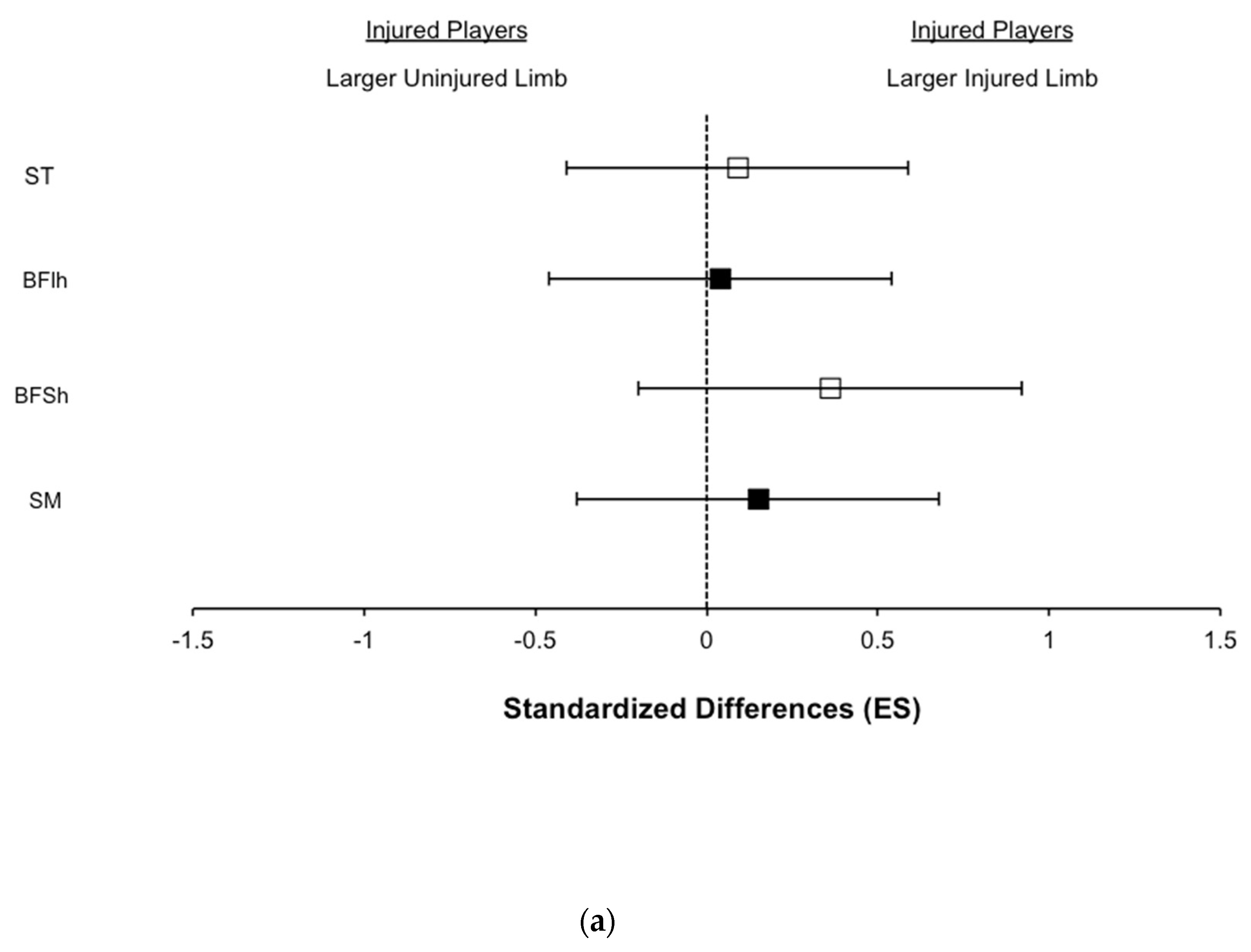
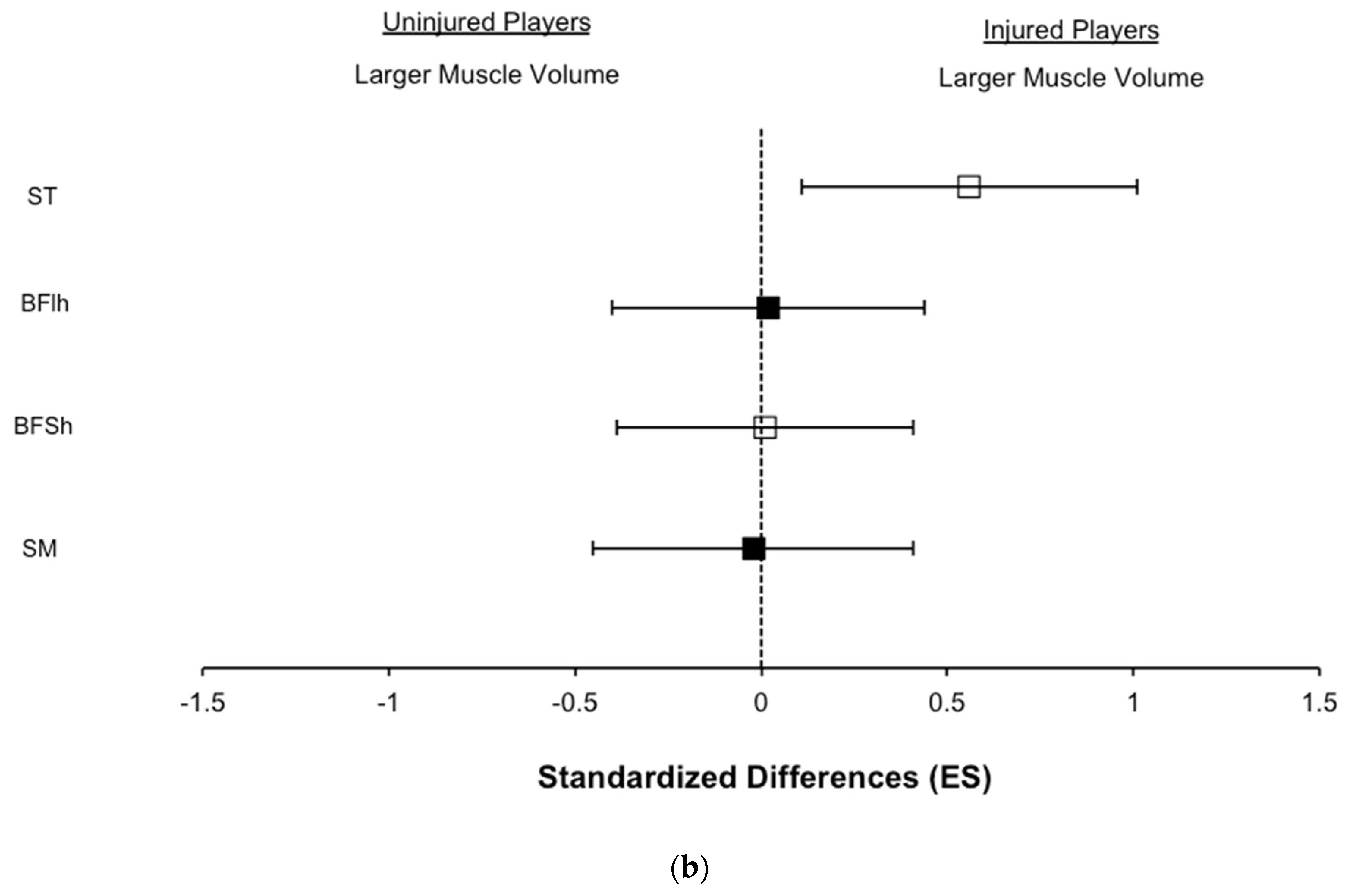
3.3. Hamstring Muscle Volume
3.4. Sprinting Performance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Woods, C.; Hawkins, R.D.; Hulse, M.; Hodson, A. The Football Association Medical Research Programme: An audit of injuries in professional football—Analysis of preseason injuries. Br. J. Sports Med. 2002, 36, 436–441. [Google Scholar] [CrossRef] [Green Version]
- Woods, C.; Hawkins, R.D.; Maltby, S.; Hulse, M.; Hodson, A. The Football Association Medical Research Programme: An audit of injuries in professional football—Analysis of hamstring injuries. Br. J. Sports Med. 2004, 38, 36–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekstrand, J.; Walden, M.; Hagglund, M. Hamstring injuries have increased by 4% annually in men’s professional football, since 2001: A 13-year longitudinal analysis of the UEFA Elite Club injury study. Br. J. Sports Med. 2016, 50, 731–737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekstrand, J.; Hagglund, M.; Walden, M. Epidemiology of muscle injuries in professional football (soccer). Am. J. Sports Med. 2011, 39, 1226–1232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCall, A.; Carling, C.; Davison, M.; Nedelec, M.; Le Gall, F.; Berthoin, S.; Dupont, G. Injury risk factors, screening tests and preventative strategies: A systematic review of the evidence that underpins the perceptions and practices of 44 football (soccer) teams from various premier leagues. Br. J. Sports Med. 2015, 49, 583–589. [Google Scholar] [CrossRef] [PubMed]
- Timmins, R.G.; Bourne, M.N.; Shield, A.J.; Williams, M.D.; Lorenzen, C.; Opar, D.A. Short biceps femoris fascicles and eccentric knee flexor weakness increase the risk of hamstring injury in elite football (soccer): A prospective cohort study. Br. J. Sports Med. 2016, 50, 1524–1535. [Google Scholar] [CrossRef] [PubMed]
- Schuermans, J.; Van Tiggelen, D.; Danneels, L.; Witvrouw, E. Susceptibility to Hamstring Injuries in Soccer: A Prospective Study Using Muscle Functional Magnetic Resonance Imaging. Am. J. Sports Med. 2016, 44, 1276–1285. [Google Scholar] [CrossRef]
- Bayer, M.L.; Hoegberget-Kalisz, M.; Jensen, M.H.; Olesen, J.L.; Svensson, R.B.; Couppé, C.; Kjaer, M. Role of tissue perfusion, muscle strength recovery, and pain in rehabilitation after acute muscle strain injury: A randomized controlled trial comparing early and delayed rehabilitation. Scand. J. Med. Sci. Sports 2018, 28, 2579–2591. [Google Scholar] [CrossRef] [PubMed]
- Silder, A.; Heiderscheit, B.C.; Thelen, D.G.; Enright, T.; Tuite, M.J. MR observations of long-term musculotendon remodeling following a hamstring strain injury. Skelet. Radiol. 2008, 37, 1101–1109. [Google Scholar] [CrossRef] [Green Version]
- Askling, C.M.; Tengvar, M.; Thorstensson, A. Acute hamstring injuries in Swedish elite football: A prospective randomised controlled clinical trial comparing two rehabilitation protocols. Br. J. Sports Med. 2013, 47, 953–959. [Google Scholar] [CrossRef] [Green Version]
- Hallen, A.; Ekstrand, J. Return to play following muscle injuries in professional footballers. J. Sports Sci. 2014, 32, 1229–1236. [Google Scholar] [CrossRef]
- Ekstrand, J.; Healy, J.C.; Waldén, M.; Lee, J.C.; English, B.; Hägglund, M. Hamstring muscle injuries in professional football: The correlation of MRI findings with return to play. Br. J. Sports Med. 2012, 46, 112–117. [Google Scholar] [CrossRef] [Green Version]
- Petersen, J.; Thorborg, K.; Nielsen, M.B.; Skjødt, T.; Bolvig, L.; Bang, N.; Hölmich, P. The diagnostic and prognostic value of ultrasonography in soccer players with acute hamstring injuries. Am. J. Sports Med. 2014, 42, 399–404. [Google Scholar] [CrossRef]
- Timmins, R.G.; Shield, A.J.; Williams, M.D.; Lorenzen, C.; Opar, D.A. Biceps femoris long head architecture: A reliability and retrospective injury study. Med. Sci. Sports Exerc. 2015, 47, 905–913. [Google Scholar] [CrossRef] [Green Version]
- Sanfilippo, J.L.; Silder, A.; Sherry, M.A.; Tuite, M.J.; Heiderscheit, B.C. Hamstring strength and morphology progression after return to sport from injury. Med. Sci. Sports Exerc. 2013, 45, 448–454. [Google Scholar] [CrossRef] [Green Version]
- Askling, C.; Karlsson, J.; Thorstensson, A. Hamstring injury occurrence in elite soccer players after preseason strength training with eccentric overload. Scand. J. Med. Sci. Sports 2003, 13, 244–250. [Google Scholar] [CrossRef]
- Schache, A.G.; Dorn, T.W.; Blanch, P.D.; Brown, N.A.; Pandy, M.G. Mechanics of the human hamstring muscles during sprinting. Med. Sci. Sports Exerc. 2012, 44, 647–658. [Google Scholar] [CrossRef] [Green Version]
- Morin, J.B.; Gimenez, P.; Edouard, P.; Arnal, P.; Jiménez-Reyes, P.; Samozino, P.; Brughelli, M.; Mendiguchia, J. Sprint Acceleration Mechanics: The Major Role of Hamstrings in Horizontal Force Production. Front. Physiol. 2015, 6, 404. [Google Scholar] [CrossRef] [PubMed]
- Tol, J.L.; Hamilton, B.; Eirale, C.; Muxart, P.; Jacobsen, P.; Whiteley, R. At return to play following hamstring injury the majority of professional football players have residual isokinetic deficits. Br. J. Sports Med. 2014, 48, 1364–1369. [Google Scholar] [CrossRef] [PubMed]
- Mendiguchia, J.; Samozino, P.; Martinez-Ruiz, E.; Brughelli, M.; Schmikli, S.; Morin, J.B.; Mendez-Villanueva, A. Progression of mechanical properties during on-field sprint running after returning to sports from a hamstring muscle injury in soccer players. Int. J. Sports Med. 2014, 35, 690–695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Opar, D.A.; Piatkowski, T.; Williams, M.D.; Shield, A.J. A novel device using the Nordic hamstring exercise to assess eccentric knee flexor strength: A reliability and retrospective injury study. J. Orthop. Sports Phys. Ther. 2013, 43, 636–640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Earlbaum Associates: Hillsdale, MI, USA, 1988. [Google Scholar]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.J.; Reid, S.L.; Elliott, B.C.; Lloyd, D.G. Running biomechanics and lower limb strength associated with prior hamstring injury. Med. Sci. Sports Exerc. 2009, 41, 1942–1951. [Google Scholar] [CrossRef] [PubMed]
- Opar, D.A.; Williams, M.D.; Timmins, R.G.; Dear, N.M.; Shield, A.J. Knee flexor strength and bicep femoris electromyographical activity is lower in previously strained hamstrings. J. Electromyogr. Kinesiol. 2013, 23, 696–703. [Google Scholar] [CrossRef] [Green Version]
- Opar, D.A.; Williams, M.D.; Timmins, R.G.; Hickey, J.; Duhig, S.J.; Shield, A.J. The effect of previous hamstring strain injuries on the change in eccentric hamstring strength during preseason training in elite Australian footballers. Am. J. Sports Med. 2015, 43, 377–384. [Google Scholar] [CrossRef] [Green Version]
- Wangensteen, A.; Vermeulen, R.; Whiteley, R.; Bahr, R.; Tol, J.L.; Witvrouw, E. Similar Isokinetic Strength Preinjury and at Return to Sport after Hamstring Injury. Med. Sci. Sports Exerc. 2019, 51, 1091–1098. [Google Scholar]
- Mendiguchia, J.; Martinez-Ruiz, E.; Morin, J.B.; Samozino, P.; Edouard, P.; Alcaraz, P.E.; Esparza-Ros, F.; Mendez-Villanueva, A. Effects of hamstring-emphasized neuromuscular training on strength and sprinting mechanics in football players. Scand. J. Med. Sci. Sports 2015, 25, e621–e629. [Google Scholar] [CrossRef]
- Ishøi, L.; Hölmich, P.; Aagaard, P.; Thorborg, K.; Bandholm, T.; Serner, A. Effects of the Nordic Hamstring exercise on sprint capacity in male football players: A randomized controlled trial. J. Sports Sci. 2018, 36, 1663–1672. [Google Scholar] [CrossRef] [PubMed]
- Mjolsnes, R.; Arnason, A.; Osthagen, T.; Raastad, T.; Bahr, R. A 10-week randomized trial comparing eccentric vs. concentric hamstring strength training in well-trained soccer players. Scand. J. Med. Sci. Sports 2004, 14, 311–317. [Google Scholar] [CrossRef]
- Fernandez-Gonzalo, R.; Tesch, P.A.; Linnehan, R.M.; Kreider, R.B.; Di Salvo, V.; Suarez-Arrones, L.; Alomar, X.; Mendez-Villanueva, A.; Rodas, G. Individual Muscle use in Hamstring Exercises by Soccer Players Assessed using Functional MRI. Int. J. Sports Med. 2016, 37, 559–564. [Google Scholar] [CrossRef]
- Mendez-Villanueva, A.; Suarez-Arrones, L.; Rodas, G.; Fernandez-Gonzalo, R.; Tesch, P.; Linnehan, R.; Kreider, R.; Di Salvo, V. MRI-Based Regional Muscle Use during Hamstring Strengthening Exercises in Elite Soccer Players. PLoS ONE 2016, 11, e0161356. [Google Scholar] [CrossRef] [Green Version]
- Bourne, M.N.; Duhig, S.J.; Timmins, R.G.; Williams, M.D.; Opar, D.A.; Al Najjar, A.; Graham, K.; Shield, A.J. Impact of the Nordic hamstring and hip extension exercises on hamstring architecture and morphology: Implications for injury prevention. Br. J. Sports Med. 2017, 51, 469–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faude, O.; Koch, T.; Meyer, T. Straight sprinting is the most frequent action in goal situations in professional football. J. Sports Sci. 2012, 30, 625–631. [Google Scholar] [CrossRef] [PubMed]
- Arnason, A.; Sigurdsson, S.B.; Gudmundsson, A.; Holme, I.; Engebretsen, L.; Bahr, R. Risk factors for injuries in football. Am. J. Sports Med. 2004, 32, 5S–16S. [Google Scholar] [CrossRef]
- Coratella, G.; Bellin, G.; Beato, M.; Schena, F. Fatigue affects peak joint torque angle in hamstrings but not in quadriceps. J. Sports Sci. 2015, 33, 1276–1282. [Google Scholar] [CrossRef] [PubMed]
- Mendiguchia, J.; Martinez-Ruiz, E.; Edouard, P.; Morin, J.B.; Martinez-Martinez, F.; Idoate, F.; Mendez-Villanueva, A. A Multifactorial, Criteria-based Progressive Algorithm for Hamstring Injury Treatment. Med. Sci. Sports Exerc. 2017, 49, 1482–1492. [Google Scholar] [CrossRef] [PubMed]
- Farì, G.; Fischetti, F.; Zonno, A.; Marra, F.; Maglie, A.; Bianchi, F.P.; Messina, G.; Ranieri, M.; Megna, M. Musculoskeletal Pain in Gymnasts: A Retrospective Analysis on a Cohort of Professional Athletes. Int. J. Environ. Res. Public Health 2021, 18, 5460. [Google Scholar] [CrossRef]
- Farì, G.; Notarnicola, A.; Covelli, I.; Moretti, B. Epidemiology of injuries in water board sports: Trauma versus overuse injury. J. Sports Med. Phys. Fit. 2021, 61, 707–711. [Google Scholar] [CrossRef] [PubMed]
- Robinson, M.E.; Dannecker, E.A. Critical issues in the use of muscle testing for the determination of sincerity of effort. Clin. J. Pain 2004, 20, 392–398. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Previously Injured Players (n = 11) | Uninjured Players (n = 31) | Standardized Differences (± 95%CL) | p Value | |
|---|---|---|---|---|
| Age (yr) | 19.4 ± 1.4 | 18.7 ± 2.0 | 0.56 ± 0.55 | 0.156 |
| Body mass (kg) | 71.7 ± 6.0 | 71.9 ± 5.9 | 0.03 ± 0.48 | 0.917 |
| Height (cm) | 178.6 ± 9.1 | 178.1 ± 7.4 | 0.04 ± 0.42 | 0.828 |
| Player Position, n (%) | ||||
| Goalkeeper | 0 (0) | 2 (6) | ||
| Defender | 4 (36) | 8 (26) | ||
| Midfielder | 3 (27) | 13 (42) | ||
| Attacker | 4 (36) | 8 (26) | ||
| Limb Dominance, n (%) | ||||
| Right | 7 (64) | 22 (71) | ||
| Left | 4 (36) | 9 (29) | ||
| Type of injury, n (%) | ||||
| Functional disorder | 7 (33) | |||
| Muscle strain injury I | 12 (57) | |||
| Muscle strain injury II | 2 (10) | |||
| Muscle strain injury III | 0 (0) | |||
| Severity of injury, n (%) | ||||
| Slight/minimal (0–3 d) | 2 (10) | |||
| Mild (4–7 d) | 4 (19) | |||
| Moderate (8–28 d) | 12 (57) | |||
| Severe (>28 d) | 3 (14) | |||
| Side of the Injury, n (%) | ||||
| Dominant | 13 (62) | |||
| Non-dominant | 8 (38) |
| Previously Injured Player | Uninjured Player | ||||||
|---|---|---|---|---|---|---|---|
| Injured Limb | Uninjured Limb | % Differences (± 95%CL) | p Value | All Uninjured Limbs | % Differences (± 95%CL) | p Value | |
| Best three reps (N) | 330.1 ± 31.3 | 317.4 ± 33.8 | +4.0 ± 5.1 | 0.077 | 298.1 ± 64.7 | +11.8 ± 5.6 | 0.033 |
| Relative to BM | 4.6 ± 0.4 | 4.4 ± 0.4 | +4.0 ± 4.8 | 0.061 | 4.2 ± 0.8 | +11.8 ± 5.1 | 0.013 |
| Best rep (N) | 344.6 ± 28.5 | 331.8 ± 30.2 | +3.8 ± 4.4 | 0.077 | 318.3 ± 66.5 | +9.7 ± 5.3 | 0.083 |
| Relative to BM | 4.8 ± 0.4 | 4.6 ± 0.4 | +3.8 ± 4.0 | 0.064 | 4.4 ± 0.8 | +9.7 ± 4.8 | 0.001 |
| Previously Injured Player | Uninjured Player | ||||||
|---|---|---|---|---|---|---|---|
| Injured Limb | Uninjured Limb | % Differences (95%CL) | p Value | All Uninjured Limbs | % Differences (95%CL) | p Value | |
| ST (cm3) | 271 ± 30 | 268 ± 30 | +1.1 ± 5.8 | 0.36 | 255 ± 37 | +6.3 ± 4.9 | 0.07 |
| BFlh (cm3) | 221 ± 41 | 219 ± 41 | +0.8 ± 9.7 | 0.66 | 220 ± 30 | +0.5 ± 8.2 | 0.95 |
| BFSh (cm3) | 141 ± 33 | 131 ± 31 | +7.7 ± 11.4 | 0.09 | 140 ± 25 | +0.3 ± 8.9 | 0.85 |
| SM (cm3) | 258 ± 36 | 252 ± 39 | +2.2 ± 7.7 | 0.33 | 259 ± 44 | −0.3 ± 6.4 | 0.88 |
| Injured Players | Uninjured Players | % Differences (95%CL) | Standardized Differences (95%CL) | p Value | |
|---|---|---|---|---|---|
| 5-m sprint (s) | 1.03 ± 0.05 | 1.01 ± 0.05 | −2.1 ± 2.1 | −0.46 ± 0.47 | 0.11 |
| 10-m sprint (s) | 1.74 ± 0.07 | 1.72 ± 0.10 | −1.3 ± 2.3 | −0.34 ± 0.59 | 0.40 |
| 20-m sprint (s) | 2.97 ± 0.09 | 2.97 ± 0.09 | −0.2 ± 1.4 | −0.08 ± 0.46 | 0.79 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mendez-Villanueva, A.; Nuñez, F.J.; Lazaro-Ramirez, J.L.; Rodriguez-Sanchez, P.; Guitart, M.; Rodas, G.; Martin-Garetxana, I.; Lekue, J.; Di Salvo, V.; Suarez-Arrones, L. Knee Flexor Eccentric Strength, Hamstring Muscle Volume and Sprinting in Elite Professional Soccer Players with a Prior Strained Hamstring. Biology 2022, 11, 69. https://doi.org/10.3390/biology11010069
Mendez-Villanueva A, Nuñez FJ, Lazaro-Ramirez JL, Rodriguez-Sanchez P, Guitart M, Rodas G, Martin-Garetxana I, Lekue J, Di Salvo V, Suarez-Arrones L. Knee Flexor Eccentric Strength, Hamstring Muscle Volume and Sprinting in Elite Professional Soccer Players with a Prior Strained Hamstring. Biology. 2022; 11(1):69. https://doi.org/10.3390/biology11010069
Chicago/Turabian StyleMendez-Villanueva, Alberto, Francisco Javier Nuñez, Jose Luis Lazaro-Ramirez, Pablo Rodriguez-Sanchez, Marc Guitart, Gil Rodas, Imanol Martin-Garetxana, Josean Lekue, Valter Di Salvo, and Luis Suarez-Arrones. 2022. "Knee Flexor Eccentric Strength, Hamstring Muscle Volume and Sprinting in Elite Professional Soccer Players with a Prior Strained Hamstring" Biology 11, no. 1: 69. https://doi.org/10.3390/biology11010069
APA StyleMendez-Villanueva, A., Nuñez, F. J., Lazaro-Ramirez, J. L., Rodriguez-Sanchez, P., Guitart, M., Rodas, G., Martin-Garetxana, I., Lekue, J., Di Salvo, V., & Suarez-Arrones, L. (2022). Knee Flexor Eccentric Strength, Hamstring Muscle Volume and Sprinting in Elite Professional Soccer Players with a Prior Strained Hamstring. Biology, 11(1), 69. https://doi.org/10.3390/biology11010069