
Effect of Sucrose Concentration on Streptococcus mutans Adhesion to Dental Material Surfaces

 , , , , and
, , , , and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Bacteria
2.2. Material Surfaces
2.3. Surface Characterization
2.4. Monitoring S. mutans Growth and Adhesion Extent
3. Results
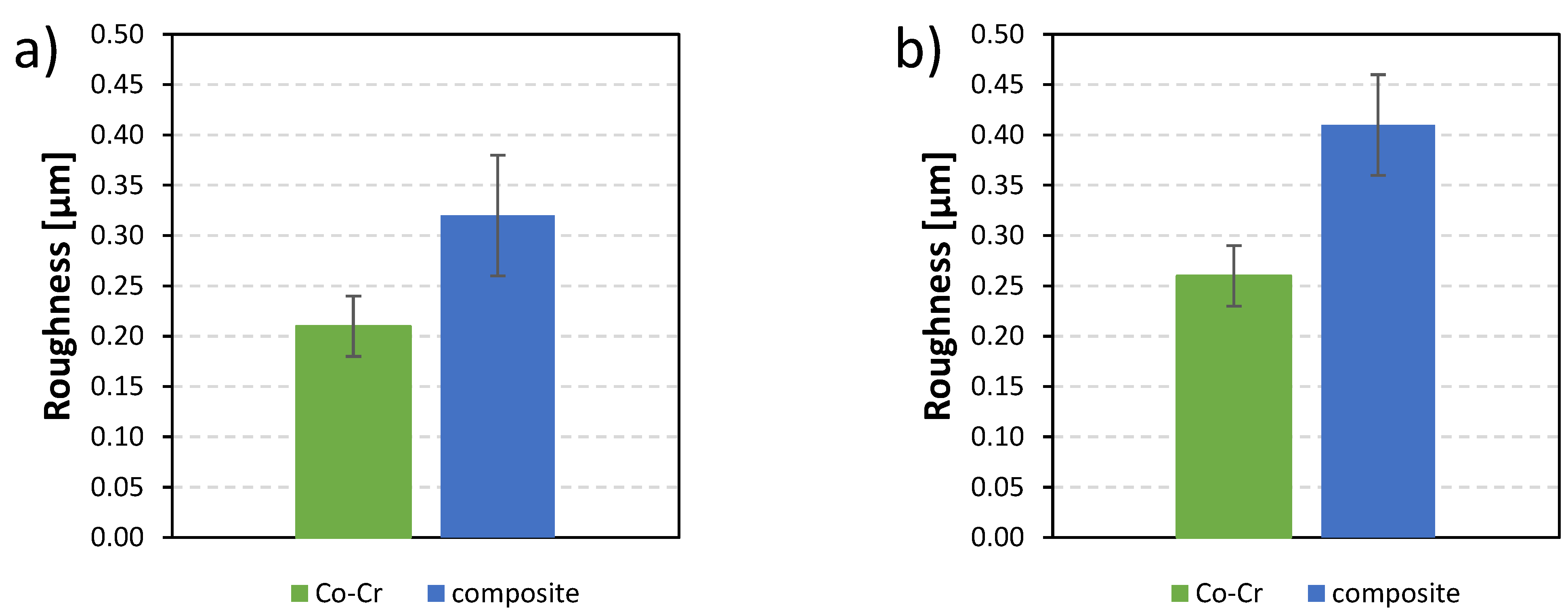
3.1. Roughness
3.2. Contact Angle
3.3. Zeta Potential
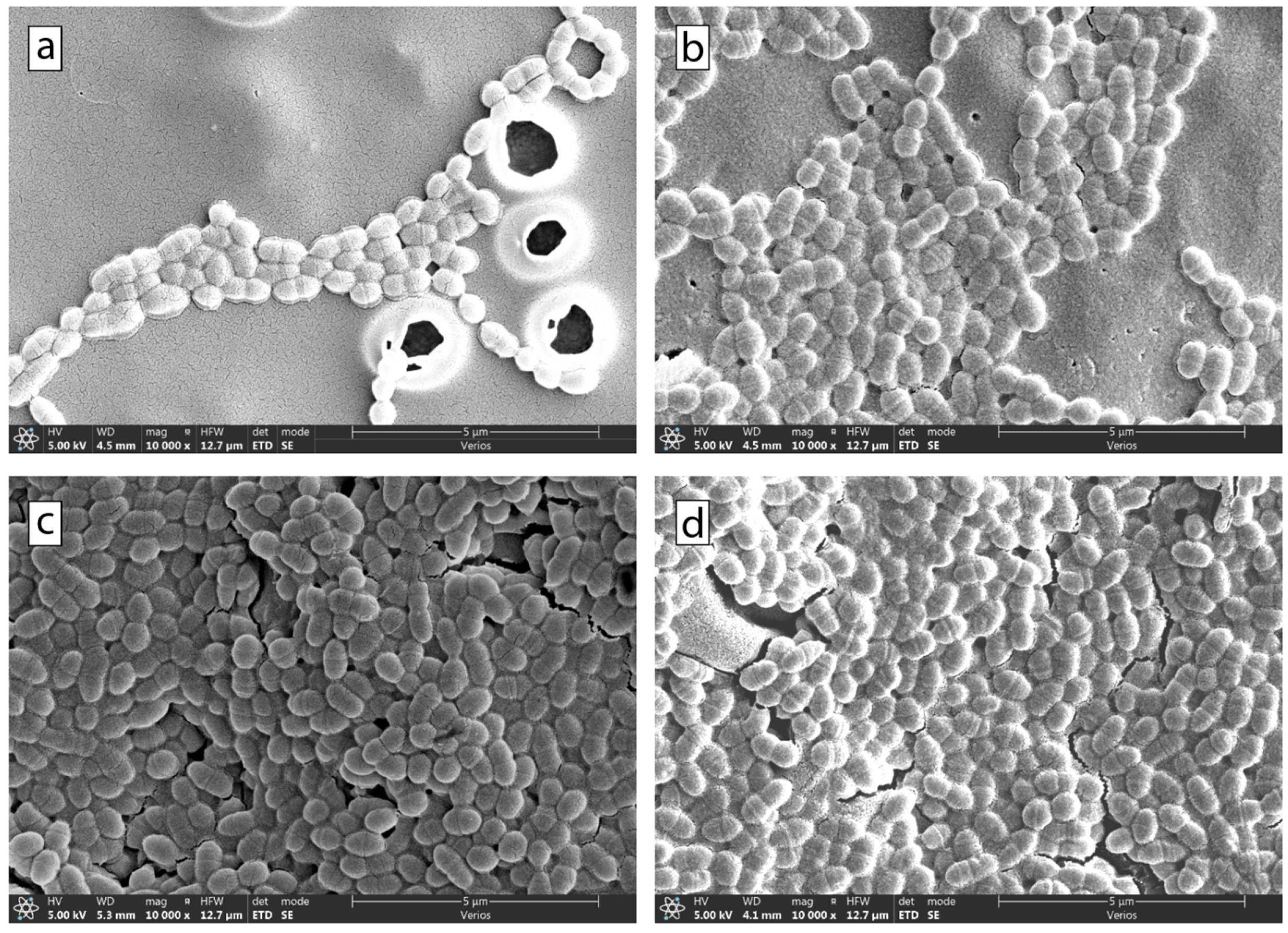
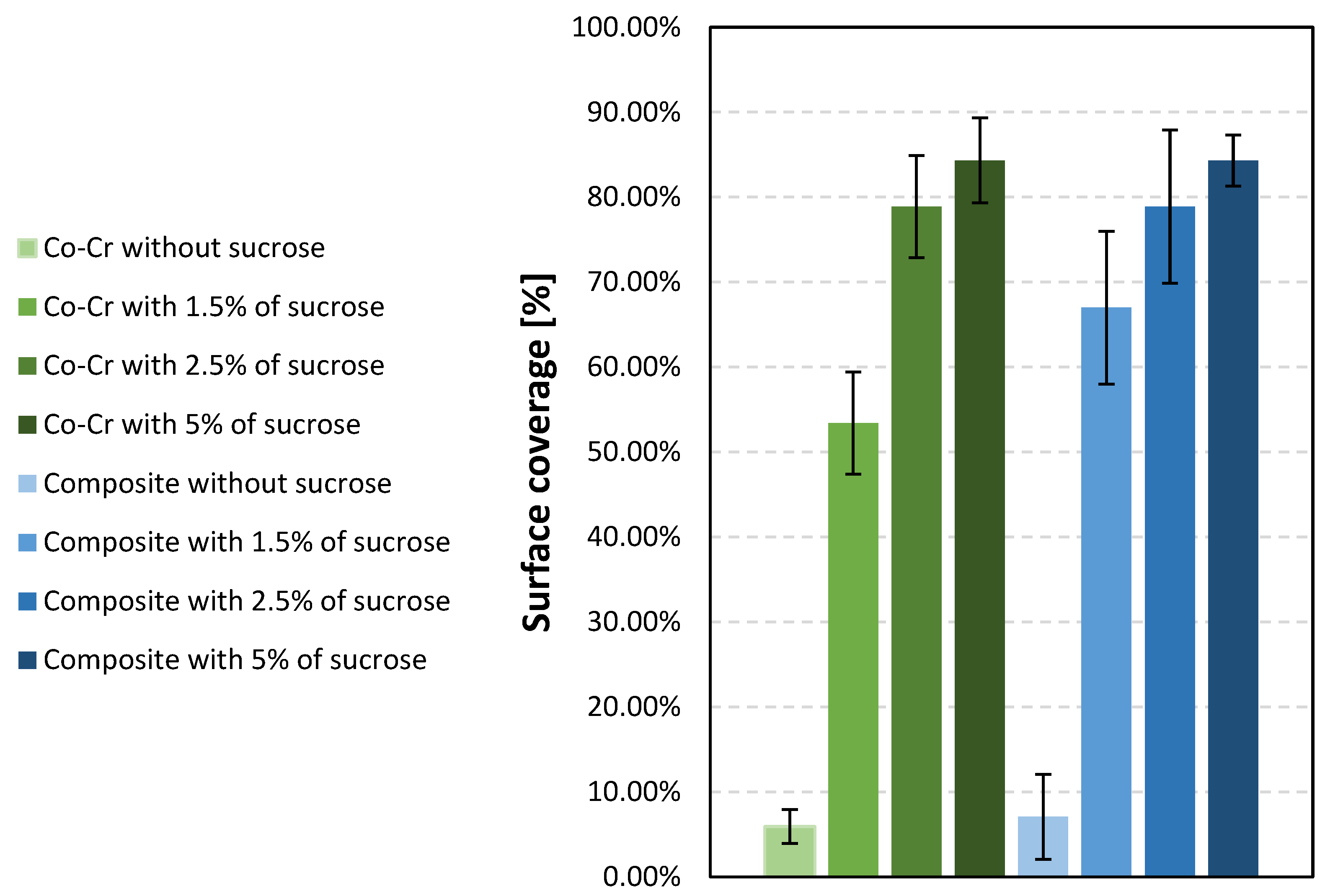
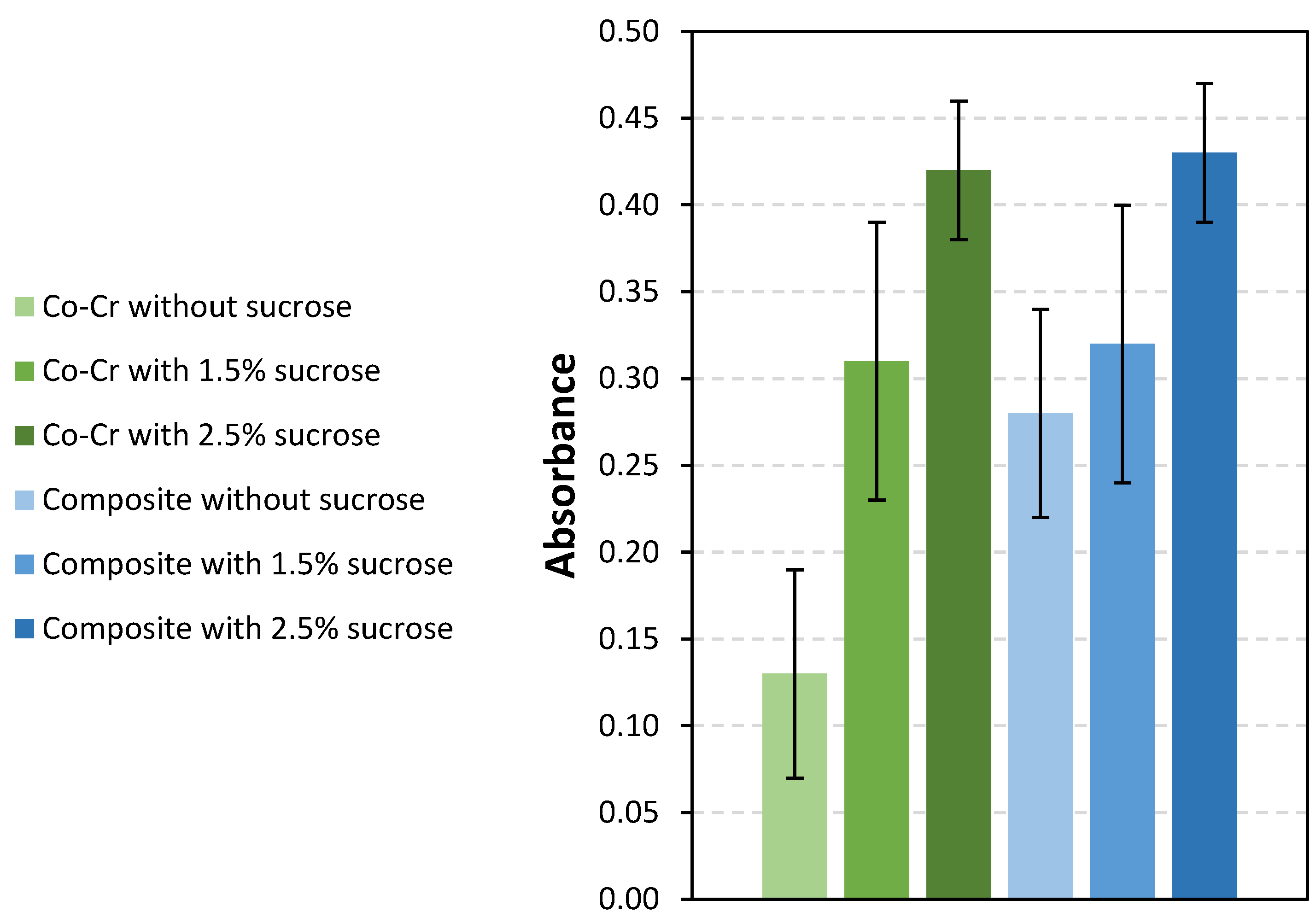
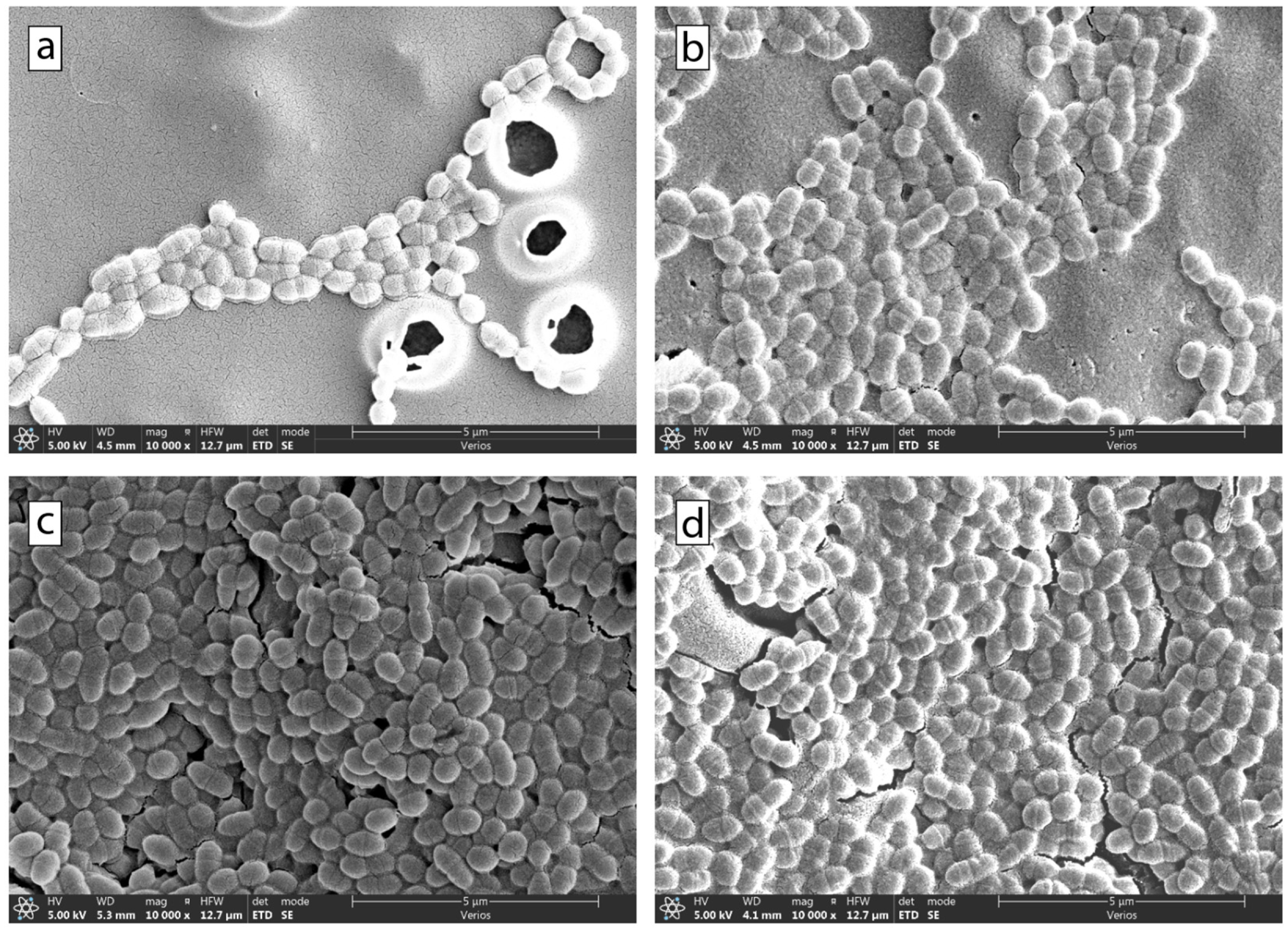
3.4. Bacterial Adhesion Extent
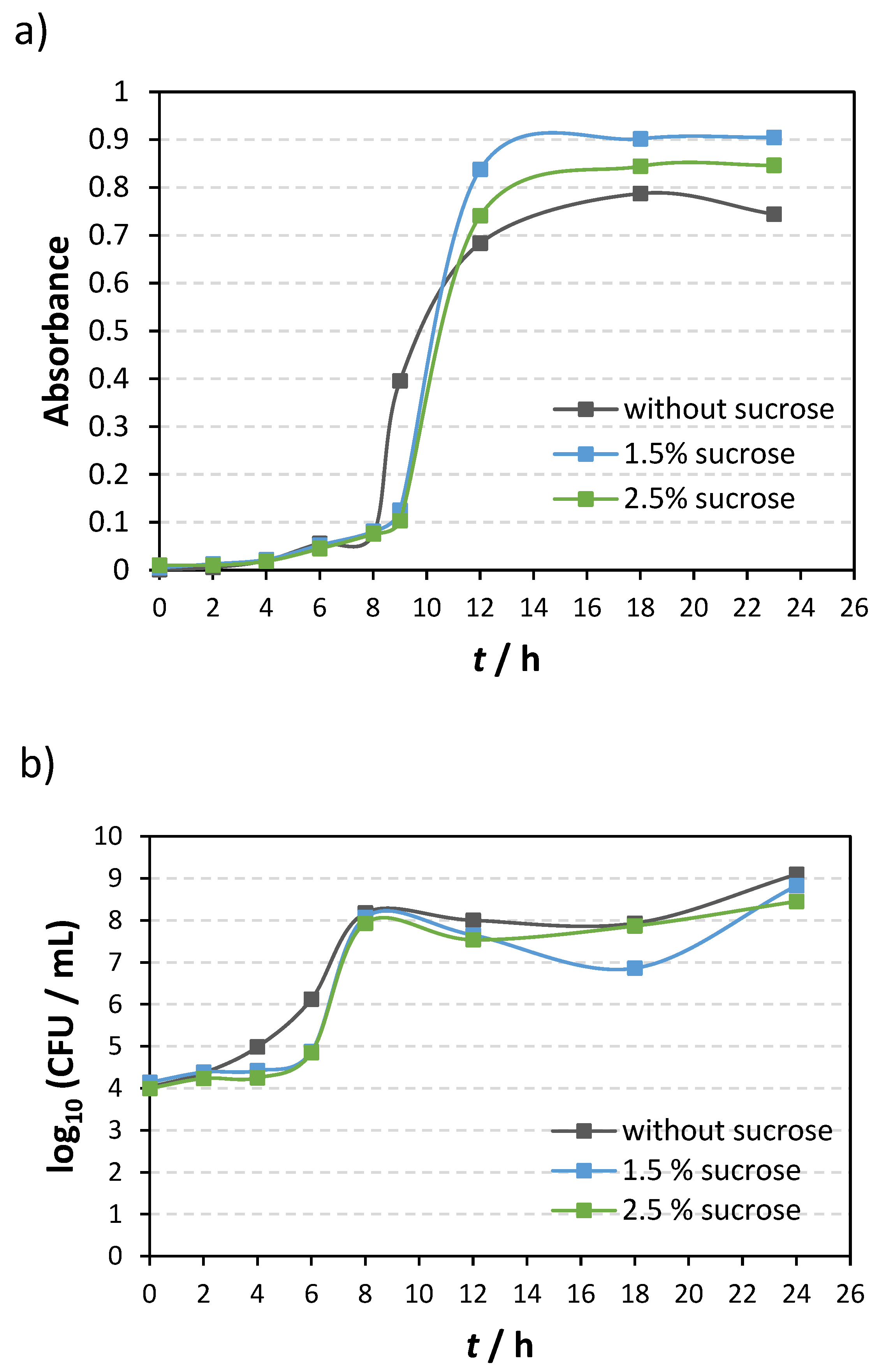
Bacterial Growth Curve of Streptococcus mutans Depends upon the Presence or Absence of Sucrose
4. Discussion
4.1. Roughness
4.2. Contact Angle
4.3. Zeta Potential
4.4. Bacterial Adhesion Extent
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Han, A.; Tsoi, J.K.H.; Rodrigues, F.P.; Leprince, J.G.; Palin, W.M. Bacterial Adhesion Mechanisms on Dental Implant Surfaces and the Influencing Factors. Int. J. Adhes. Adhes. 2016, 69, 58–71. [Google Scholar] [CrossRef]
- Mahler, D.; Sakaguchi, R.L. Restorative Materials—Metals. In Craig’s Restorative Dental Materials; Sakaguchi, R.L., Powers, J.M., Eds.; Elsevier Mosby: Philadelphia, PA, USA, 2012; pp. 199–251. [Google Scholar]
- Lovegrove, J.M. Dental Plaque Revisited: Bacteria Associated with Periodontal Disease. J. N. Z. Soc. Periodontol. 2004, 87, 7–21. [Google Scholar]
- Kamel, J.H.; Salman, F.D. Prevalence of Secondary Caries Around Posterior Restoration. Acta Sci. Med. Sci. 2022, 6, 03–10. [Google Scholar] [CrossRef]
- Brouwer, F.; Askar, H.; Paris, S.; Schwendicke, F. Detecting Secondary Caries Lesions. J. Dent. Res. 2016, 95, 143–151. [Google Scholar] [CrossRef]
- Mjör, I.A.; Toffenetti, F. Secondary Caries: A Literature Review with Case Reports. Quintessence Int. 2000, 31, 165–179. [Google Scholar] [PubMed]
- Ionescu, A.C.; Brambilla, E.; Travan, A.; Marsich, E.; Donati, I.; Gobbi, P.; Turco, G.; Di Lenarda, R.; Cadenaro, M.; Paoletti, S.; et al. Silver–Polysaccharide Antimicrobial Nanocomposite Coating for Methacrylic Surfaces Reduces Streptococcus Mutans Biofilm Formation in Vitro. J. Dent. 2015, 43, 1483–1490. [Google Scholar] [CrossRef]
- Veiga, N.; Aires, D.; Douglas, F.; Pereira, M.; Vaz, A.; Rama, L.; Silva, M.; Miranda, V.; Pereira, F.; Vidal, B.; et al. Dental Caries: A Review. J. Dent. Oral Health 2016, 2, 43–47. [Google Scholar]
- Islam, B.; Khan, S.N.; Khan, A.U. Dental Caries: From Infection to Prevention. Med. Sci. Monit. 2007, 13, RA196–RA203. [Google Scholar]
- Forssten, S.D.; Björklund, M.; Ouwehand, A.C. Streptococcus Mutans, Caries and Simulation Models. Nutrients 2010, 2, 290–298. [Google Scholar] [CrossRef] [PubMed]
- Quirynen, M.; Van Der Mei, H.C.; Bollen, C.M.L.; Schotte, A.; Marechal, M.; Doornbusch, G.I.; Naert, I.; Busscher, H.J.; Van Steenberghe, D. An In Vivo Study of the Influence of the Surface Roughness of Implants on the Microbiology of Supra- and Subgingival Plaque. J. Dent. Res. 1993, 72, 1304–1309. [Google Scholar] [CrossRef]
- Boks, N.P.; Norde, W.; van der Mei, H.C.; Busscher, H.J. Forces Involved in Bacterial Adhesion to Hydrophilic and Hydrophobic Surfaces. Microbiology 2008, 154, 3122–3133. [Google Scholar] [CrossRef] [PubMed]
- Filipović, U.; Dahmane, R.G.; Ghannouchi, S.; Zore, A.; Bohinc, K. Bacterial Adhesion on Orthopedic Implants. Adv. Colloid Interface Sci. 2020, 283, 102228. [Google Scholar] [CrossRef] [PubMed]
- Abranches, J.; Zeng, L.; Kajfasz, J.K.; Palmer, S.R.; Chakraborty, B.; Wen, Z.T.; Richards, V.P.; Brady, L.J.; Lemos, J.A. Biology of Oral Streptococci. Microbiol. Spectr. 2018, 6, 42–60. [Google Scholar] [CrossRef] [PubMed]
- Lemos, J.A.; Palmer, S.R.; Zeng, L.; Wen, Z.T.; Kajfasz, J.K.; Freires, I.A.; Abranches, J.; Brady, L.J. The Biology of Streptococcus Mutans. Microbiol. Spectr. 2019, 7, 56–69. [Google Scholar] [CrossRef] [PubMed]
- Negrini, T.d.C.; Ren, Z.; Miao, Y.; Kim, D.; Simon-Soro, Á.; Liu, Y.; Koo, H.; Arthur, R.A. Dietary Sugars Modulate Bacterial-Fungal Interactions in Saliva and Inter-Kingdom Biofilm Formation on Apatitic Surface. Front. Cell. Infect. Microbiol. 2022, 12, 993640. [Google Scholar] [CrossRef] [PubMed]
- Van Amerongen, J.P.; Watson, T.F.; Opdam, N.J.M.; Roeters, F.J.M. Restoring the Tooth: «The Seal Is the Deal». In Dental Caries: The Disease and Its Clinical Management; Fejerskov, O., Kidd, E.A.M., Eds.; Blackwell: Oxford, UK, 2008; pp. 387–395. [Google Scholar]
- Cai, J.-N.; Jung, J.-E.; Dang, M.-H.; Kim, M.-A.; Yi, H.-K.; Jeon, J.-G. Functional Relationship between Sucrose and a Cariogenic Biofilm Formation. PLoS ONE 2016, 11, e0157184. [Google Scholar] [CrossRef]
- Grosgogeat, B.; Vaicelyte, A.; Gauthier, R.; Janssen, C.; Le Borgne, M. Toxicological Risks of the Cobalt–Chromium Alloys in Dentistry: A Systematic Review. Materials 2022, 15, 5801. [Google Scholar] [CrossRef]
- Al Jabbari, Y.S. Physico-Mechanical Properties and Prosthodontic Applications of Co-Cr Dental Alloys: A Review of the Literature. J. Adv. Prosthodont. 2014, 6, 138–145. [Google Scholar] [CrossRef]
- Yeung, A.L.P.; Lo, E.C.M.; Chow, T.W.; Clark, R.K.F. Oral Health Status of Patients 5–6 Years after Placement of Cobalt-Chromium Removable Partial Dentures. J. Oral Rehabil. 2000, 27, 183–189. [Google Scholar] [CrossRef]
- Sulistiani, D.A.; Widjijono, W.; Dharmastiti, R. Bacterial Adhesion of Streptococcus Mutans to Cobalt Chromium Recast Alloys. Maj. Kedokt. Gigi Indones. 2022, 7, 84. [Google Scholar] [CrossRef]
- Vaicelyte, A.; Janssen, C.; Le Borgne, M.; Grosgogeat, B. Cobalt–Chromium Dental Alloys: Metal Exposures, Toxicological Risks, CMR Classification, and EU Regulatory Framework. Crystals 2020, 10, 1151. [Google Scholar] [CrossRef]
- Yildirim Üçüncü, M.; Kazım ÜÇÜNCÜ, M. Comparison of the Mechanical Properties of Various Microhybrid Dental Composites. Euroasian Dent. Res. 2023, 1, 58–64. [Google Scholar]
- Motevasselian, F.; Zibafar, E.; Yassini, E.; Mirzaei, M.; Pourmirhoseni, N. Adherence of Streptococcus Mutans to Microhybrid and Nanohybrid Resin Composites and Dental Amalgam: An In Vitro Study. J. Dent. 2017, 14, 337–343. [Google Scholar]
- Tuncer, S.; Demirci, M.; Öztaş, E.; Tekçe, N.; Uysal, Ö. Microhybrid versus Nanofill Composite in Combination with a Three Step Etch and Rinse Adhesive in Occlusal Cavities: Five Year Results. Restor. Dent. Endod. 2017, 42, 253. [Google Scholar] [CrossRef] [PubMed]
- Silva, R.A.B.; Nelson-Filho, P.; De-Oliveira, K.M.H.; Romualdo, P.C.; Gatón-Hernandez, P.; Aires, C.P.; Silva, L.A.B. Adhesion and Initial Colonization of Streptococcus Mutans Is Influenced by Time and Composition of Different Composites. Int. J. Odontostomatol. 2018, 12, 395–400. [Google Scholar] [CrossRef]
- Heintze, S.D.; Loguercio, A.D.; Hanzen, T.A.; Reis, A.; Rousson, V. Clinical Efficacy of Resin-Based Direct Posterior Restorations and Glass-Ionomer Restorations—An Updated Meta-Analysis of Clinical Outcome Parameters. Dent. Mater. 2022, 38, e109–e135. [Google Scholar] [CrossRef]
- Maran, B.M.; de Geus, J.L.; Gutiérrez, M.F.; Heintze, S.; Tardem, C.; Barceleiro, M.O.; Reis, A.; Loguercio, A.D. Nanofilled/Nanohybrid and Hybrid Resin-Based Composite in Patients with Direct Restorations in Posterior Teeth: A Systematic Review and Meta-Analysis. J. Dent. 2020, 99, 103407. [Google Scholar] [CrossRef]
- de Andrade, A.; Duarte, R.; Medeiros e Silva, F.D.; Batista, A.; Lima, K.; Monteiro, G.; Montes, M. Resin Composite Class I Restorations: A 54-Month Randomized Clinical Trial. Oper. Dent. 2014, 39, 588–594. [Google Scholar] [CrossRef]
- Sirin Karaarslan, E.; Aytac Bal, F.; Buldur, M.; Altan, H. Twenty-Four-Month Clinical Comparison of Two Bulk-Fill and a Microhybrid Composite Restorations in Class II Cavities. Eur. J. Prosthodont. Restor. Dent. 2021, 29, 231–240. [Google Scholar] [CrossRef] [PubMed]
- Huang, H. Ion Release from NiTi Orthodontic Wires in Artificial Saliva with Various Acidities. Biomaterials 2003, 24, 3585–3592. [Google Scholar] [CrossRef] [PubMed]
- Nozaki, K.; Koizumi, H.; Horiuchi, N.; Nakamura, M.; Okura, T.; Yamashita, K.; Nagai, A. Suppression Effects of Dental Glass-Ceramics with Polarization-Induced Highly Dense Surface Charges against Bacterial Adhesion. Dent. Mater. J. 2015, 34, 671–678. [Google Scholar] [CrossRef]
- Gharechahi, M.; Moosavi, H.; Forghani, M. Effect of Surface Roughness and Materials Composition. J. Biomater. Nanobiotechnol. 2012, 3, 541–546. [Google Scholar] [CrossRef]
- Kozmos, M.; Virant, P.; Rojko, F.; Abram, A.; Rudolf, R.; Raspor, P.; Zore, A.; Bohinc, K. Bacterial Adhesion of Streptococcus Mutans to Dental Material Surfaces. Molecules 2021, 26, 1152. [Google Scholar] [CrossRef] [PubMed]
- Teughels, W.; Van Assche, N.; Sliepen, I.; Quirynen, M. Effect of Material Characteristics and/or Surface Topography on Biofilm Development. Clin. Oral Implants Res. 2006, 17, 68–81. [Google Scholar] [CrossRef] [PubMed]
- Carneiro, P.; Ramos, T.; de Azevedo, C.; de Lima, E.; de Souza, S.; Turbino, M.; Cesar, P.; Matos, A. Influence of Finishing and Polishing Techniques and Abrasion on Transmittance and Roughness of Composite Resins. Oper. Dent. 2016, 41, 634–641. [Google Scholar] [CrossRef] [PubMed]
- Azam, M.; Khan, A.; Muzzafar, D.; Faryal, R.; Siddiqi, S.; Ahmad, R.; Chauhdry, A.; Rehman, I. Structural, Surface, in Vitro Bacterial Adhesion and Biofilm Formation Analysis of Three Dental Restorative Composites. Materials 2015, 8, 3221–3237. [Google Scholar] [CrossRef]
- van Loosdrecht, M.C.; Lyklema, J.; Norde, W.; Schraa, G.; Zehnder, A.J. The Role of Bacterial Cell Wall Hydrophobicity in Adhesion. Appl. Environ. Microbiol. 1987, 53, 1893–1897. [Google Scholar] [CrossRef] [PubMed]
- Song, F.; Koo, H.; Ren, D. Effects of Material Properties on Bacterial Adhesion and Biofilm Formation. J. Dent. Res. 2015, 94, 1027–1034. [Google Scholar] [CrossRef]
- Cai, J.-N.; Choi, H.-M.; Jeon, J.-G. Relationship between Sucrose Concentration and Bacteria Proportion in a Multispecies Biofilm. J. Oral Microbiol. 2021, 13, 1910443. [Google Scholar] [CrossRef] [PubMed]
- Meldrum, R.J.; Brocklehurst, T.F.; Wilson, D.R.; Wilson, P.D.G. The Effects of Cell Immobilization, PH and Sucrose on the Growth of Listeria Monocytogenes Scott A at 10 °C. Food Microbiol. 2003, 20, 97–103. [Google Scholar] [CrossRef]
- Høiby, N.; Bjarnsholt, T.; Givskov, M.; Molin, S.; Ciofu, O. Antibiotic Resistance of Bacterial Biofilms. Int. J. Antimicrob Agents 2010, 35, 322–332. [Google Scholar] [CrossRef] [PubMed]
- Stewart, P.S.; William Costerton, J. Antibiotic Resistance of Bacteria in Biofilms. Lancet 2001, 358, 135–138. [Google Scholar] [CrossRef]
- Contardo, M.S.; Díaz, N.; Lobos, O.; Padilla, C.; Giacaman, R.A. Oral Colonization by Streptococcus Mutans and Its Association with the Severity of Periodontal Disease in Adults. Rev. Clin. Periodoncia Implantol. Rehabil. Oral 2011, 4, 9–12. [Google Scholar] [CrossRef]
- Dani, S.; Prabhu, A.; Chaitra, K.; Desai, N.; Patil, S.; Rajeev, R. Assessment of Streptococcus Mutans in Healthy versus Gingivitis and Chronic Periodontitis: A Clinico-Microbiological Study. Contemp. Clin. Dent. 2016, 7, 529. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zore, A.; Rojko, F.; Mlinarić, N.M.; Veber, J.; Učakar, A.; Štukelj, R.; Pondelak, A.; Sever Škapin, A.; Bohinc, K. Effect of Sucrose Concentration on Streptococcus mutans Adhesion to Dental Material Surfaces. Coatings 2024, 14, 165. https://doi.org/10.3390/coatings14020165
Zore A, Rojko F, Mlinarić NM, Veber J, Učakar A, Štukelj R, Pondelak A, Sever Škapin A, Bohinc K. Effect of Sucrose Concentration on Streptococcus mutans Adhesion to Dental Material Surfaces. Coatings. 2024; 14(2):165. https://doi.org/10.3390/coatings14020165
Chicago/Turabian StyleZore, Anamarija, Franc Rojko, Nives Matijaković Mlinarić, Jona Veber, Aleksander Učakar, Roman Štukelj, Andreja Pondelak, Andrijana Sever Škapin, and Klemen Bohinc. 2024. "Effect of Sucrose Concentration on Streptococcus mutans Adhesion to Dental Material Surfaces" Coatings 14, no. 2: 165. https://doi.org/10.3390/coatings14020165
APA StyleZore, A., Rojko, F., Mlinarić, N. M., Veber, J., Učakar, A., Štukelj, R., Pondelak, A., Sever Škapin, A., & Bohinc, K. (2024). Effect of Sucrose Concentration on Streptococcus mutans Adhesion to Dental Material Surfaces. Coatings, 14(2), 165. https://doi.org/10.3390/coatings14020165