Therapeutic Drug Monitoring of Meropenem and Piperacillin in Critical Illness—Experience and Recommendations from One Year in Routine Clinical Practice

 ,
,
Abstract
1. Introduction
2. Results
2.1. Demographic and Clinical Data
2.2. Assessment of Meropenem Trough Sample Concentration
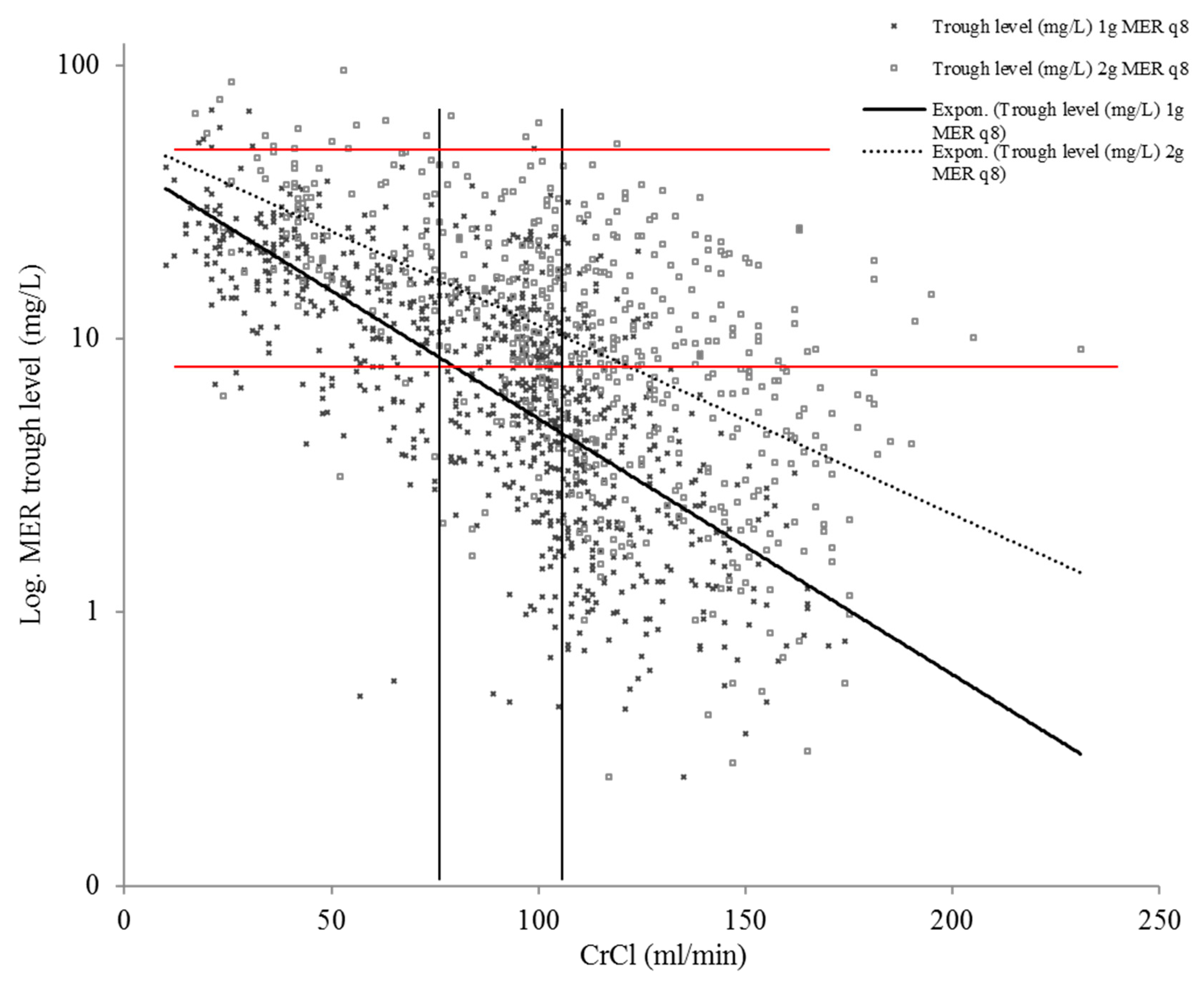
2.3. The Impact of Renal Function on Meropenem Concentration
2.4. Assessment of Piperacillin Trough Sample Concentration
2.5. The Impact of Renal Function on Piperacillin Concentrations
2.6. Changes in Target Attainment and Dosing Regimens Caused by the TDM-program
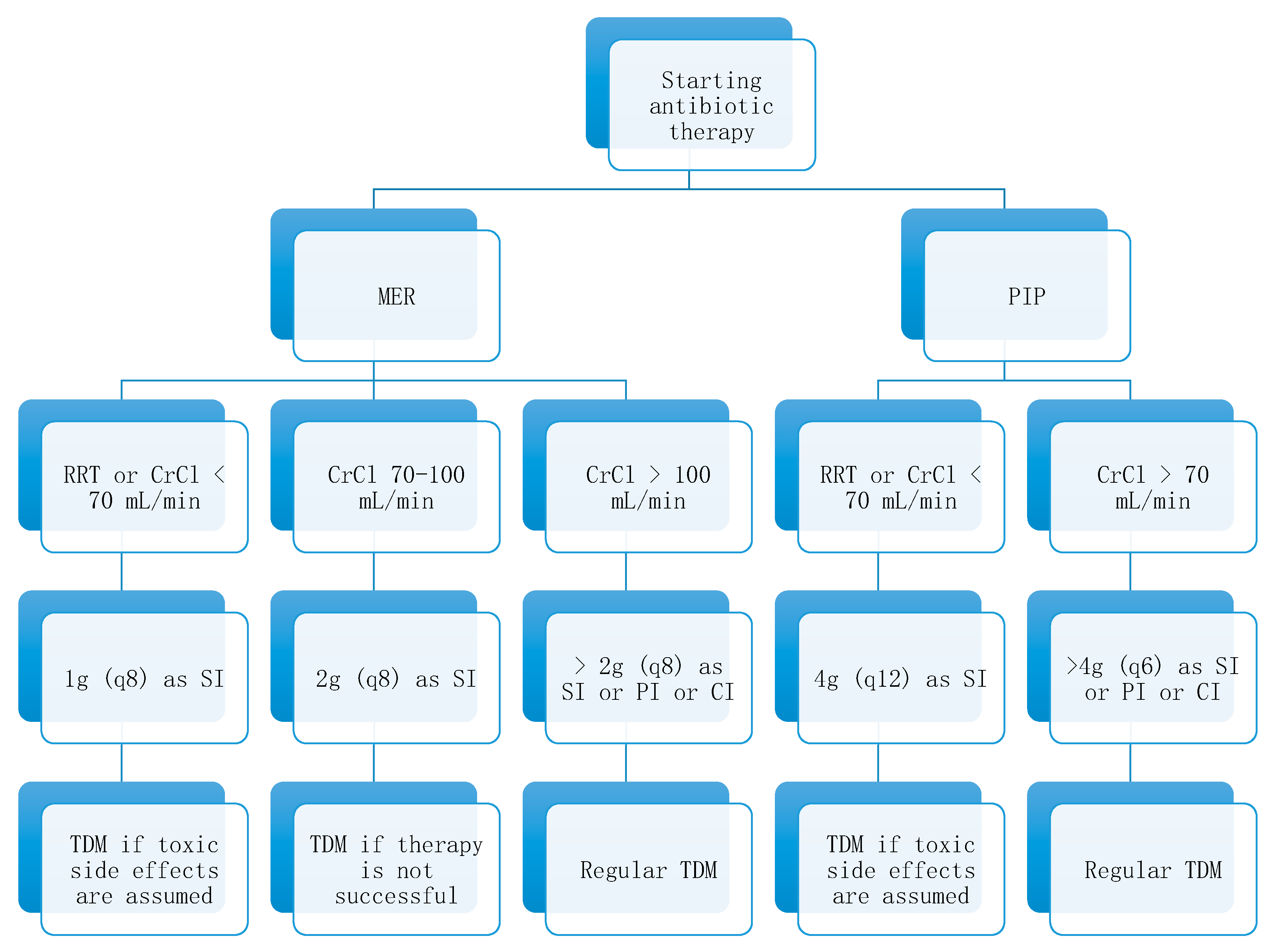
2.7. Dosing Algorithm for Meropenem and Piperacillin Based on Renal Function
3. Discussion
4. Materials and Methods
4.1. Study Setting
4.2. Study Population
4.3. Drug Administration, TDM, and Data Collection
4.4. Sample Collection and Laboratory Testing
4.5. Pharmacokinetic/pharmacodynamic Targets
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Ethics approval and consent to participate
References
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017, 43, 304–377. [Google Scholar] [CrossRef]
- Angus, D.C.; Linde-Zwirble, W.T.; Lidicker, J.; Clermont, G.; Carcillo, J.; Pinsky, M.R. Epidemiology of severe sepsis in the United States: Analysis of incidence, outcome, and associated costs of care. Crit. Care Med. 2001, 29, 1303–1310. [Google Scholar] [CrossRef]
- Felton, T.W.; Goodwin, J.; O’Connor, L.; Sharp, A.; Gregson, L.; Livermore, J.; Howard, S.J.; Neely, M.N.; Hope, W.W. Impact of Bolus dosing versus continuous infusion of Piperacillin and Tazobactam on the development of antimicrobial resistance in Pseudomonas aeruginosa. Antimicrob. Agents Chemother. 2013, 57, 5811–5819. [Google Scholar] [CrossRef]
- Kumar, A. Early antimicrobial therapy in severe sepsis and septic shock. Curr. Infect. Dis. Rep. 2010, 12, 336–344. [Google Scholar] [CrossRef]
- Kumar, A.; Ellis, P.; Arabi, Y.; Roberts, D.; Light, B.; Parrillo, J.E.; Dodek, P.; Wood, G.; Kumar, A.; Simon, D. Initiation of inappropriate antimicrobial therapy results in a fivefold reduction of survival in human septic shock. Chest 2009, 136, 1237–1248. [Google Scholar] [CrossRef] [PubMed]
- Taccone, F.S. Pierre-François, L.; Thierry, D.; Herbert, S.; Isabelle, D.; Xavier, W.; Daniel, D.B.; Brice, L.; Pierre, W.; Jean-Louis, V.; et al. Insufficient beta-lactam concentrations in the early phase of severe sepsis and septic shock. Crit. Care 2010, 14, R126. [Google Scholar] [CrossRef] [PubMed]
- Zander, J.; Dobbeler, G.; Nagel, D.; Maier, B.; Scharf, C.; Huseyn-Zada, M.; Jung, J.; Frey, L.; Vogeser, M.; Zoller, M. Piperacillin concentration in relation to therapeutic range in critically ill patients--a prospective observational study. Crit. Care 2016, 20, 79. [Google Scholar] [CrossRef] [PubMed]
- Dulhunty, J.M.; Roberts, J.A.; Davis, J.S.; Webb, S.A.; Bellomo, R.; Gomersall, C.; Shirwadkar, C.; Eastwood, G.M. Myburgh, J. Paterson, D.L. et al. A Multicenter Randomized Trial of Continuous versus Intermittent beta-Lactam Infusion in Severe Sepsis. Am. J. Respir. Crit. Care Med. 2015, 192, 1298–1305. [Google Scholar] [CrossRef] [PubMed]
- Craig, W.A. The pharmacology of meropenem, a new carbapenem antibiotic. Clin. Infect. Dis. 1997, 24 (Suppl. 2), S266–S275. [Google Scholar] [CrossRef]
- Goncalves-Pereira, J.; Povoa, P. Antibiotics in critically ill patients: A systematic review of the pharmacokinetics of beta-lactams. Crit. Care 2011, 15, R206. [Google Scholar] [CrossRef]
- Roberts, J.A.; Abdul-Aziz, M.H.; Lipman, J.; Mouton, J.W.; Vinks, A.A.; Felton, T.W.; Hope, W.W.; Farkas, A.; Neely, M.N.; Schentag, J.J.; et al. Individualised antibiotic dosing for patients who are critically ill: Challenges and potential solutions. Lancet Infect. Dis. 2014, 14, 498–509. [Google Scholar] [CrossRef]
- De Waele, J.J.; Lipman, J.; Akova, M.; Bassetti, M.; Dimopoulos, G.; Kaukonen, M.; Koulenti, D.; Martin, C.; Montravers, P.; Rello, J. Risk factors for target non-attainment during empirical treatment with beta-lactam antibiotics in critically ill patients. Intensive Care Med. 2014, 40, 1340–1351. [Google Scholar] [CrossRef] [PubMed]
- Jamal, J.A.; Economou, C.J.; Lipman, J.; Roberts, J.A. Improving antibiotic dosing in special situations in the ICU: Burns, renal replacement therapy and extracorporeal membrane oxygenation. Curr. Opin. Crit. Care 2012, 18, 460–471. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.A.; Paul, S.K.; Akova, M.; Bassetti, M.; De Waele, J.J.; Dimopoulos, G.; Kaukonen, K.M.; Koulenti, D.; Martin, C.; Montravers, P. DALI: Defining antibiotic levels in intensive care unit patients: Are current beta-lactam antibiotic doses sufficient for critically ill patients? Clin. Infect. Dis. 2014, 58, 1072–1083. [Google Scholar] [CrossRef]
- Li, C.; Du, X.; Kuti, J.L.; Nicolau, D.P. Clinical pharmacodynamics of meropenem in patients with lower respiratory tract infections. Antimicrob. Agents Chemother. 2007, 51, 1725–1730. [Google Scholar] [CrossRef]
- Guilhaumou, R.; Benaboud, S.; Bennis, Y.; Dahyot-Fizelier, C.; Dailly, E.; Gandia, P.; Goutelle, S.; Lefeuvre, S.; Mongardon, N.; Roger, C. Optimization of the treatment with beta-lactam antibiotics in critically ill patients-guidelines from the French Society of Pharmacology and Therapeutics (Societe Francaise de Pharmacologie et Therapeutique-SFPT) and the French Society of Anaesthesia and Intensive Care Medicine (Societe Francaise d’Anesthesie et Reanimation-SFAR). Crit. Care 2019, 23, 104. [Google Scholar] [CrossRef]
- Ehmann, L.; Zoller, M.; Minichmayr, I.K.; Scharf, C.; Maier, B.; Schmitt, M.V.; Hartung, N.; Huisinga, W.; Vogeser, M.; Frey, L.; et al. Role of renal function in risk assessment of target non-attainment after standard dosing of meropenem in critically ill patients: A prospective observational study. Crit. Care 2017, 21, 263. [Google Scholar] [CrossRef]
- Weber, N.; Jackson, K.; McWhinney, B.; Ungerer, J.; Kennedy, G.; Lipman, J.; Roberts, J.A. Evaluation of pharmacokinetic/pharmacodynamic and clinical outcomes with 6-hourly empiric piperacillin-tazobactam dosing in hematological malignancy patients with febrile neutropenia. J. Infect. Chemother. 2019. [Google Scholar] [CrossRef]
- Delattre, I.K.; Taccone, F.S.; Jacobs, F.; Hites, M.; Dugernier, T.; Spapen, H.; Laterre, P.F.; Wallemacq, P.E.; Van Bambeke, F.; Tulkens, P.M. Optimizing beta-lactams treatment in critically-ill patients using pharmacokinetics/pharmacodynamics targets: Are first conventional doses effective? Expert Rev. Anti-Infect. Ther. 2017, 15, 677–688. [Google Scholar] [CrossRef]
- Carrie, C.; Legeron, R.; Petit, L.; Ollivier, J.; Cottenceau, V.; d’Houdain, N.; Boyer, P.; Lafitte., F.; Xuereb, F.; Sztark, F. Higher than standard dosing regimen are needed to achieve optimal antibiotic exposure in critically ill patients with augmented renal clearance receiving piperacillin-tazobactam administered by continuous infusion. J. Crit. Care 2018, 48, 66–71. [Google Scholar] [CrossRef]
- Jacobs, A.; Taccone, F.S.; Roberts, J.A.; Jacobs, F.; Cotton, F.; Wolff, F.; Creteur, J.; Vincent, J.-L.; Hites, M. beta-Lactam Dosage Regimens in Septic Patients with Augmented Renal Clearance. Antimicrob. Agents Chemother. 2018, 62. [Google Scholar] [CrossRef] [PubMed]
- Tamatsukuri, T.; Ohbayashi, M.; Kohyama, N.; Kobayashi, Y.; Yamamoto, T.; Fukuda, K.; Nakamura, S.; Miyake, Y.; Dohi, K.; Kogo, M. The exploration of population pharmacokinetic model for meropenem in augmented renal clearance and investigation of optimum setting of dose. J. Infect. Chemother. 2018, 24, 834–840. [Google Scholar] [CrossRef] [PubMed]
- Mahmoud, S.H.; Shen, C. Augmented Renal Clearance in Critical Illness: An Important Consideration in Drug Dosing. Pharmaceutics 2017, 9, 36. [Google Scholar] [CrossRef] [PubMed]
- Leroy, A.; Fillastre, J.P.; Borsa-Lebas, F.; Etienne, I.; Humbert, G. Pharmacokinetics of meropenem (ICI 194,660) and its metabolite (ICI 213,689) in healthy subjects and in patients with renal impairment. Antimicrob. Agents Chemother. 1992, 36, 2794–2798. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Paul-Ehrlich-Gesellschaft für Chemotherapie e.V. Kalkulierte parenterale Initialtherapie bakterieller Erkrankungen bei Erwachsenen - Update 2018. 2018. Available online: https://www.awmf.org/uploads/tx_szleitlinien/082-006l_S2k_Parenterale_Antibiotika_2019-08.pdf (accessed on 20 March 2020).
- de With, K.; Allerberger, F.; Amann, S.; Apfalter, P.; Brodt, H.R.; Eckmanns, T.; Fellhauer, M.; Geiss, H.K.; Janata, O.; Krause, R. Strategies to enhance rational use of antibiotics in hospital: A guideline by the German Society for Infectious Diseases. Infection 2016, 44, 395–439. [Google Scholar] [CrossRef] [PubMed]
- Wong, G.; Briscoe, S.; McWhinney, B.; Ally, M.; Ungerer, J.; Lipman, J.; Roberts, J.A. Therapeutic drug monitoring of beta-lactam antibiotics in the critically ill: Direct measurement of unbound drug concentrations to achieve appropriate drug exposures. J. Antimicrob. Chemother. 2018, 73, 3087–3094. [Google Scholar] [CrossRef]
- Imani, S.; Buscher, H.; Day, R.; Gentili, S.; Jones, G.R.D.; Marriott, D.; Norris, R.; Sandaradura, I. An evaluation of risk factors to predict target concentration non-attainment in critically ill patients prior to empiric beta-lactam therapy. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 2171–2175. [Google Scholar] [CrossRef]
- Fournier, A.; Eggimann, P.; Pagani, J.L.; Revelly, J.P.; Decosterd, L.A.; Marchetti, O.; Pannatier, A.; Voirol, P.; Que, Y.A. Impact of the introduction of real-time therapeutic drug monitoring on empirical doses of carbapenems in critically ill burn patients. Burns 2015, 41, 956–968. [Google Scholar] [CrossRef]
- Muller, A.E.; Huttner, B.; Huttner, A. Therapeutic Drug Monitoring of Beta-Lactams and Other Antibiotics in the Intensive Care Unit: Which Agents, Which Patients and Which Infections? Drugs 2018, 78, 439–451. [Google Scholar] [CrossRef]
- Kim, Y.J.; Kim, S.I.; Lee, Y.D.; Choi, H.J.; Choi, J.Y.; Yoon, S.K.; You, Y.K.; Kim, D.G. Carbapenem-resistant Acinetobacter baumannii Bacteremia in Liver Transplant Recipients. Transplant. Proc. 2018, 50, 1132–1135. [Google Scholar] [CrossRef]
- Raviv, Y.; Shitrit, D.; Amital, A.; Fox, B.; Bakal, I.; Tauber, R.; Bishara, J.; Kramer, M.R. Multidrug-resistant Klebsiella pneumoniae acquisition in lung transplant recipients. Clin. Transplant. 2012, 26, E388–E394. [Google Scholar] [CrossRef] [PubMed]
- Kothekar, A.T.; Divatia, J.V.; Myatra, S.N.; Patil, A.; Nookala Krishnamurthy, M.; Maheshwarappa, H.M.; Siddiqui, S.S.; Gurjar, M.; Biswas, S.; Gota, V. Clinical pharmacokinetics of 3-h extended infusion of meropenem in adult patients with severe sepsis and septic shock: Implications for empirical therapy against Gram-negative bacteria. Ann. Intensive Care 2020, 10, 4. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.Y.; Gu, J.; Lyu, J.; Liu, D.; Wang, Y.T.; Liu, F.; Zhu, F.X.; An, Y.Z. Pharmacokinetic and Pharmacodynamic Efficacies of Continuous versus Intermittent Administration of Meropenem in Patients with Severe Sepsis and Septic Shock: A Prospective Randomized Pilot Study. Chin. Med. J. 2017, 130, 1139–1145. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.C.; Tai, C.H.; Liao, W.Y.; Wang, C.C.; Kuo, C.H.; Lin, S.W.; Ku, S.C. Augmented renal clearance is associated with inadequate antibiotic pharmacokinetic/pharmacodynamic target in Asian ICU population: A prospective observational study. Infect. Drug Resist. 2019, 12, 2531–2541. [Google Scholar] [CrossRef]
- De Waele, J.J.; Carrette, S.; Carlier, M.; Stove, V.; Boelens, J.; Claeys, G.; Leroux-Roels, I.; Hoste, E.; Depuydt, P.; Decruyenaere, J. Therapeutic drug monitoring-based dose optimisation of piperacillin and meropenem: A randomised controlled trial. Intensive Care Med. 2014, 40, 380–387. [Google Scholar] [CrossRef]
- Carlier, M.; Taccone, F.S.; Beumier, M.; Seyler, L.; Cotton, F.; Jacobs, F.; Roberts, J.A. Population pharmacokinetics and dosing simulations of cefepime in septic shock patients receiving continuous renal replacement therapy. Int. J. Antimicrob. Agents 2015, 46, 413–419. [Google Scholar] [CrossRef]
- Leegwater, E.; Kraaijenbrink, B.V.C.; Moes, D.; Purmer, I.M.; Wilms, E.B. Population pharmacokinetics of ceftriaxone administered as continuous or intermittent infusion in critically ill patients. J. Antimicrob. Chemother. 2020. [Google Scholar] [CrossRef]
- Fachinformation Meronem® 2019. Available online: https://www.pfizermed.de/fileadmin/produktdatenbank/pdf/016053_freigabe.pdf (accessed on 20 March 2020).
- Fachinformation Piperacillin-Tazobactam-Teva® 4 g/ 0,5 g Pulver zur Herstellung einer Infusionslösung 2017. Available online: https://s3.eu-central-1.amazonaws.com/prod-cerebro-ifap/media_all/81160.pdf (accessed on 20 March 2020).
- Usman, M.; Frey, O.R.; Hempel, G. Population pharmacokinetics of meropenem in elderly patients: Dosing simulations based on renal function. Eur. J. Clin. Pharmacol. 2017, 73, 333–342. [Google Scholar] [CrossRef]
- Sukarnjanaset, W.; Jaruratanasirikul, S.; Wattanavijitkul, T. Population pharmacokinetics and pharmacodynamics of piperacillin in critically ill patients during the early phase of sepsis. J. Pharmacokinet. Pharmacodyn. 2019, 46, 251–261. [Google Scholar] [CrossRef]
- Imani, S.; Buscher, H.; Marriott, D.; Gentili, S.; Sandaradura, I. Too much of a good thing: A retrospective study of beta-lactam concentration-toxicity relationships. J. Antimicrob. Chemother. 2017, 72, 2891–2897. [Google Scholar] [CrossRef]
- Beumier, M.; Casu, G.S.; Hites, M.; Wolff, F.; Cotton, F.; Vincent, J.L.; Jacobs, F.; Taccone, F.S. Elevated beta-lactam concentrations associated with neurological deterioration in ICU septic patients. Minerva Anestesiol. 2015, 81, 497–506. [Google Scholar] [PubMed]
- Udy, A.A.; Varghese, J.M.; Altukroni, M.; Briscoe, S.; McWhinney, B.C.; Ungerer, J.P.; Lipman, J.; Roberts, J.A. Subtherapeutic initial beta-lactam concentrations in select critically ill patients: Association between augmented renal clearance and low trough drug concentrations. Chest 2012, 142, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Abdul-Aziz, M.H.; Lipman, J.; Akova, M.; Bassetti, M.; De Waele, J.J.; Dimopoulos, G.; Dulhunty, J.; Kaukonen, K.M.; Koulenti, D.; Martin, C.; et al. Is prolonged infusion of piperacillin/tazobactam and meropenem in critically ill patients associated with improved pharmacokinetic/pharmacodynamic and patient outcomes? An observation from the Defining Antibiotic Levels in Intensive care unit patients (DALI) cohort. J. Antimicrob. Chemother. 2016, 71, 196–207. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, N.; Jen, S.P.; Altshuler, D.; Papadopoulos, J.; Pham, V.P.; Dubrovskaya, Y. Evaluation of Meropenem Extended Versus Intermittent Infusion Dosing Protocol in Critically Ill Patients. J. Intensive Care Med. 2018, 885066618784264. [Google Scholar] [CrossRef] [PubMed]
- Carlier, M.; Carrette, S.; Roberts, J.A.; Stove, V.; Verstraete, A.; Hoste, E.; Depuydt, P.; Decruyenaere, J.; Lipman, J.; Wallis, S.C. Meropenem and piperacillin/tazobactam prescribing in critically ill patients: Does augmented renal clearance affect pharmacokinetic/pharmacodynamic target attainment when extended infusions are used? Crit. Care 2013, 17, R84. [Google Scholar] [CrossRef] [PubMed]
- Carrie, C.; Petit, L.; d’Houdain, N.; Sauvage, N.; Cottenceau, V.; Lafitte, M.; Foumenteze, C.; Hisz, Q.; Menu, D.; Legeron, R. Association between augmented renal clearance, antibiotic exposure and clinical outcome in critically ill septic patients receiving high doses of beta-lactams administered by continuous infusion: A prospective observational study. Int. J. Antimicrob. Agents 2018, 51, 443–449. [Google Scholar] [CrossRef]
- Rhodes, N.J.; Liu, J.; O’Donnell, J.N.; Dulhunty, J.M.; Abdul-Aziz, M.H.; Berko, P.Y.; Nadler, B.; Lipman, J.; Roberts, J.A. Prolonged Infusion Piperacillin-Tazobactam Decreases Mortality and Improves Outcomes in Severely Ill Patients: Results of a Systematic Review and Meta-Analysis. Crit. Care Med. 2018, 46, 236–243. [Google Scholar] [CrossRef]
- Richter, D.C.; Frey, O.; Röhr, A.; Roberts, J.A.; Köberer, A.; Fuchs, T.; Papadimas, N.; Heinzel-Gutenbrunner, M.; Brenner, T.; Lichtenstern, C. Therapeutic drug monitoring-guided continuous infusion of piperacillin/tazobactam significantly improves pharmacokinetic target attainment in critically ill patients: A retrospective analysis of four years of clinical experience. Infection 2019, 47, 1001–1011. [Google Scholar] [CrossRef]
- Taubert, M.; Zoller, M.; Maier, B.; Frechen, S.; Scharf, C.; Holdt, L.M.; Frey, L.; Vogeser, M.; Fuhr, U.; Zander, J. Predictors of Inadequate Linezolid Concentrations after Standard Dosing in Critically Ill Patients. Antimicrob. Agents Chemother. 2016, 60, 5254–5261. [Google Scholar] [CrossRef]
- Khachman, D.; Conil, J.M.; Georges, B.; Saivin, S.; Houin, G.; Toutain, P.L.; Laffont, C.M. Optimizing ciprofloxacin dosing in intensive care unit patients through the use of population pharmacokinetic-pharmacodynamic analysis and Monte Carlo simulations. J. Antimicrob. Chemother. 2011, 66, 1798–1809. [Google Scholar] [CrossRef]
- Paal, M.; Zoller, M.; Schuster, C.; Vogeser, M.; Schutze, G. Simultaneous quantification of cefepime, meropenem, ciprofloxacin, moxifloxacin, linezolid and piperacillin in human serum using an isotope-dilution HPLC-MS/MS method. J. Pharm. Biomed. Anal. 2018, 152, 102–110. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro 3rd, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T. A new equation to estimate glomerular filtration rate. Ann. Intern Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Schuster, C.; Sterz, S.; Teupser, D.; Brügel, M.; Vogeser, M.; Paal, M. Multiplex Therapeutic Drug Monitoring by Isotope-dilution HPLC-MS/MS of Antibiotics in Critical Illnesses. J. Vis. Exp. 2018. [Google Scholar] [CrossRef] [PubMed]
- Minichmayr, I.K.; Roberts, J.A.; Frey, O.R.; Roehr, A.C.; Kloft, C.; Brinkmann, A. Development of a dosing nomogram for continuous-infusion meropenem in critically ill patients based on a validated population pharmacokinetic model. J. Antimicrob. Chemother. 2018, 73, 1330–1339. [Google Scholar] [CrossRef]
- Quinton, M.C.; Bodeau, S.; Kontar, L.; Zerbib, Y.; Maizel, J.; Slama, M.; Masmoudi, K.; Lemaire-Hurtel, A.S.; Bennis, Y. Neurotoxic Concentration of Piperacillin during Continuous Infusion in Critically Ill Patients. Antimicrob. Agents Chemother. 2017, 61. [Google Scholar] [CrossRef]
- Wong, G.; Briscoe, S.; Adnan, S.; McWhinney, B.; Ungerer, J.; Lipman, J.; Roberts, J.A. Protein binding of beta-lactam antibiotics in critically ill patients: Can we successfully predict unbound concentrations? Antimicrob. Agents Chemother. 2013, 57, 6165–6170. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | n (%) or Median (Interquartile-Range) |
|---|---|
| Age (years) | 61 (48–73) |
| Sex (male/female) | 190/99 |
| Weight (kg) | 74 (64–87) |
| BMI (kg/m2) | 24.7 (21.3–28.5) |
| SOFA Score on the first day of sampling | 12 (8–14) |
| Serum creatinine on the first day of sampling | 1.0 (0.8–1.7) |
| CrCl on the first day of sampling, mL/min | 90 (73–113) |
| CrCl <45 mL/min on the first day of sampling | 30 (15.3) |
| CrCl 45–90 mL/min on the first day of sampling | 58 (29.6) |
| CrCl >90 mL/min on the first day of sampling | 108 (55.1) |
| RRT | 83 (28.7) |
| LETX | 27 (9.3) |
| LTX | 96 (33.2) |
| ARDS | 31 (10.7) |
| TDM | Samples (%) | Subtherapeutic (%) | Toxic (%) | Median (mg/L) (IQR) | Statistic | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| All | 100 | 39.3 | 2.1 | 10.9 (4.9–19.5) | |||||||
| 1 g (q8) | 70.2 | 40.8 | 1.3 | 10.6 (4.6–17.9) | Lower than 2 g (q8) (p < 0.01, r = 0.18) | ||||||
| 2 g (q8) | 29.8 | 35.0 | 3.8 | 11.7 (5.8–27.5) | Higher than 1 g (q8) (p < 0.01, r = 0.18) | ||||||
| Group 1 | all | 24.3 | 12.4 | 4.5 | 17.4 (11.4–21.9) | ||||||
| 1 g (q8) | 2 g (q8) | 19.4 | 4.9 | 13.8 | 6.7 | 3.1 | 10.1 | 16.4 (11.4–21.9) | 30.8 (19.2–38.6) | ||
| Group 2 | All | 17.7 | 11.1 | 7.4 | 19.6 (14.1–27.5) | ||||||
| 1 g (q8) | 2 g (q8) | 13.5 | 4.2 | 13.4 | 3.9 | 2.8 | 22.1 | 17.9 (12.7–24.5) | 28.7 (18.2–41.9) | ||
| Group 3 | All | 19.0 | 37.5 | 1.4 | 9.9 (5.6–14.8) | ||||||
| 1 g (q8) | 2 g (q8) | 13.2 | 5.8 | 46.7 | 16.8 | 0.4 | 3.7 | 8.6 (4.9–12.7) | 15.0 (9.3–23.6) | ||
| Group 4 | All | 39.0 | 69.4 | 0.1 | 4.5 (2.1–9.2) | ||||||
| 1 g (q8) | 2 g (q8) | 20.6 | 18.4 | 82.3 | 55.0 | 0 | 0.3 | 3.3 (1.7–6.1) | 7.2 (3.5–13.3) | ||
| Period 1 | All | 45.3 | 40.9 | 2.8 | 10.5 (4.2–19.1) | No sig. difference to period 2 (p = 0.08, r = 0.04) | |||||
| 1 g (q8) | 2 g (q8) | 36.7 | 8.6 | 41.8 | 37.3 | 1.6 | 7.6 | 10.3 (4.1–18.7) | 10.9 (4.6–23.9) | ||
| Period 2 | All | 54.7 | 38.0 | 3.1 | 11.3 (5.3–19.6) | No sig. difference to period 1 (p = 0.08, r = 0.04) | |||||
| 1 g (q8) | 2 g (q8) | 31.8 | 22.9 | 41.8 | 32.7 | 1.9 | 4.8 | 9.9 (4.7–16.7) | 13.3 (6.3–26.7) | ||
| TDM | Samples (%) | Subtherapeutic (%) | Toxic (%) | Median (mg/L) (IQR) | Statistic | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| All | 100 | 33.6 | 11.0 | 44.3 (15.7–94.4) | ||||||||||||
| q6 | 12.6 | 45.0 | 10.2 | 23.5 (12.1–51.2) | Lower than q12 (p < 0.01, r = 0.34) | |||||||||||
| q8 | 77.8 | 33.8 | 12.3 | 47.1 (15.7–96.5) | Lower than q12 (p = 0.04, r = 0.1), | |||||||||||
| q12 | 9.3 | 18.6 | 3.7 | 65.9 (40.7–120.5) | Higher than q8 (p = 0.04, r = 0.1) and q6 (p < 0.01, r = 0.34) | |||||||||||
| Group 1 | all | 24.8 | 3.3 | 15.3 | 90.6 (66.6–127.5) | |||||||||||
| q6 | q8 | q 12 | 0 | 22.9 | 1.9 | / | 3.6 | 0 | / | 16.7 | 0 | / | 91.4 (67.2–128.7) | 77.3 (50.8–121.5) | ||
| Group 2 | all | 25.2 | 5.6 | 26.2 | 94.1 (52.0–154.0) | |||||||||||
| q6 | q8 | q 12 | 2.2 | 19.5 | 3.5 | 0 | 5.8 | 4.5 | 21.4 | 28.2 | 18.2 | 63.0 (47.8–142.2) | 94.1 (50.8–162,2) | 79.0 (64.8–127.7) | ||
| Group 3 | all | 20.1 | 43.0 | 2.3 | 25.4 (15.3–47.3) | |||||||||||
| q6 | q8 | q 12 | 1.6 | 17.1 | 1.4 | 60.0 | 39.4 | 66.7 | 0 | 1.8 | 11.1 | 20.1 (13.2–31.5) | 25.9 (17.8–51.3) | 12.2 (10.3–32.7) | ||
| Group 4 | all | 29.9 | 74.2 | 0 | 12.1 (5.1–23.1) | |||||||||||
| q6 | q8 | q 12 | 9.1 | 20.8 | 0 | 53.4 | 83.3 | / | 0 | 0 | / | 6.6 (9.1–37.5) | 8.2 (3.8–17.2) | / | ||
| Period 1 | all | 46.4 | 42.4 | 6.4 | 28.3 (12.7–80.6) | Lower than period 2 (p < 0.01, r = 0.2) | ||||||||||
| q6 | q8 | q 12 | 4.7 | 41.7 | 0 | 50.0 | 41.5 | / | 0 | 7.2 | / | 22.0 (10.1–30.8) | 30.7 (14.0–81.5) | / | ||
| Period 2 | all | 53.6 | 26.1 | 15.0 | 61.5 (20.9–114.0) | Higher than period 1 (p < 0.01, r = 0.2) | ||||||||||
| q6 | q8 | q 12 | 7.9 | 36.5 | 9.2 | 44.0 | 24.5 | 16.9 | 6.0 | 18.1 | 10.2 | 29.2 (13.5–64.7) | 67.4 (23.3–124.5) | 64.6 (40.7–117.5) | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scharf, C.; Paal, M.; Schroeder, I.; Vogeser, M.; Draenert, R.; Irlbeck, M.; Zoller, M.; Liebchen, U. Therapeutic Drug Monitoring of Meropenem and Piperacillin in Critical Illness—Experience and Recommendations from One Year in Routine Clinical Practice. Antibiotics 2020, 9, 131. https://doi.org/10.3390/antibiotics9030131
Scharf C, Paal M, Schroeder I, Vogeser M, Draenert R, Irlbeck M, Zoller M, Liebchen U. Therapeutic Drug Monitoring of Meropenem and Piperacillin in Critical Illness—Experience and Recommendations from One Year in Routine Clinical Practice. Antibiotics. 2020; 9(3):131. https://doi.org/10.3390/antibiotics9030131
Chicago/Turabian StyleScharf, Christina, Michael Paal, Ines Schroeder, Michael Vogeser, Rika Draenert, Michael Irlbeck, Michael Zoller, and Uwe Liebchen. 2020. "Therapeutic Drug Monitoring of Meropenem and Piperacillin in Critical Illness—Experience and Recommendations from One Year in Routine Clinical Practice" Antibiotics 9, no. 3: 131. https://doi.org/10.3390/antibiotics9030131
APA StyleScharf, C., Paal, M., Schroeder, I., Vogeser, M., Draenert, R., Irlbeck, M., Zoller, M., & Liebchen, U. (2020). Therapeutic Drug Monitoring of Meropenem and Piperacillin in Critical Illness—Experience and Recommendations from One Year in Routine Clinical Practice. Antibiotics, 9(3), 131. https://doi.org/10.3390/antibiotics9030131