Antimicrobial Stewardship in Cardiac Device Surgery: Impact of Behavioural Change Interventions on Extended Prophylaxis Practices


Abstract
1. Introduction
2. Methodology
2.1. Study Design and Setting
2.2. Data Collection
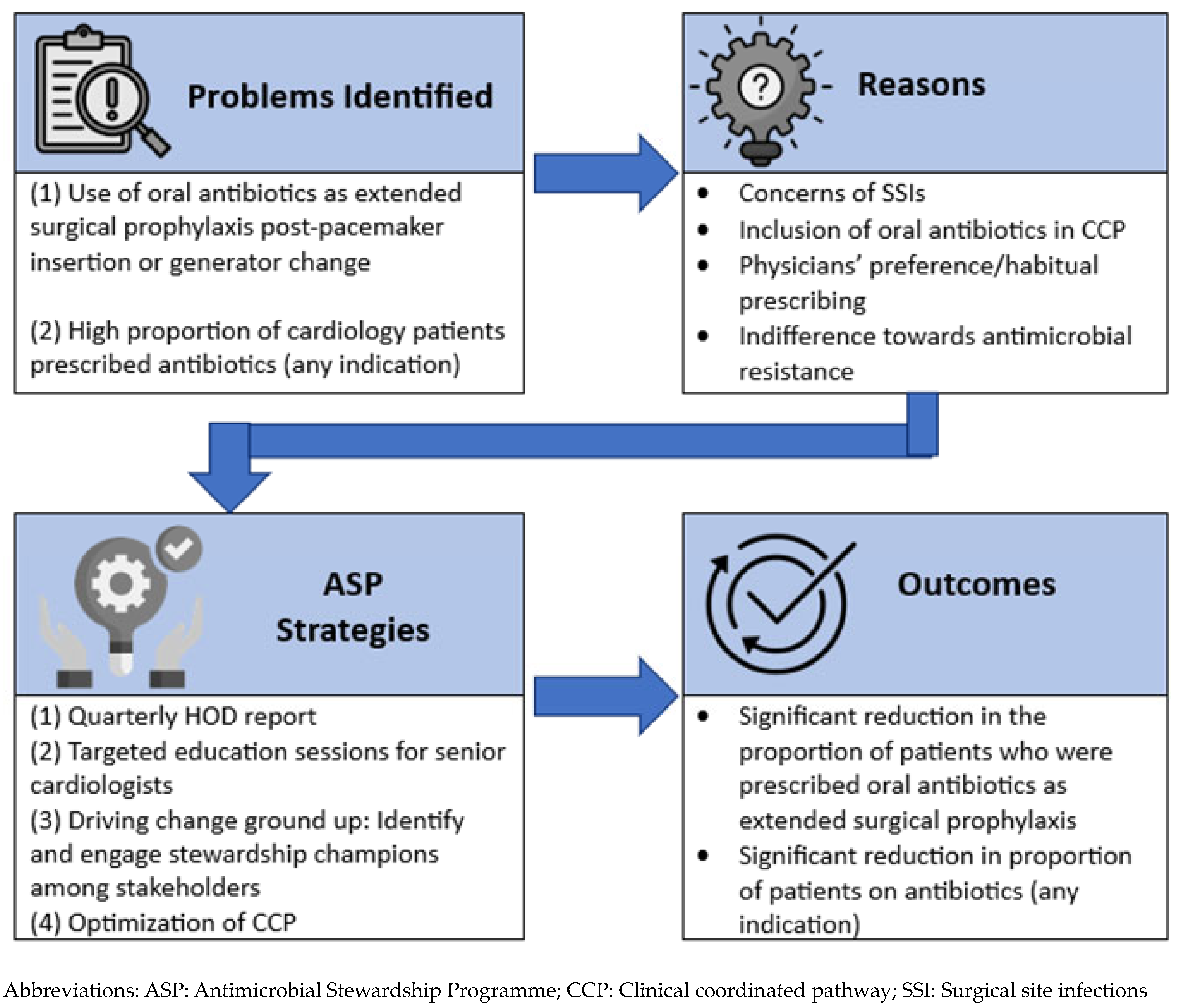
2.3. ASP Interventions
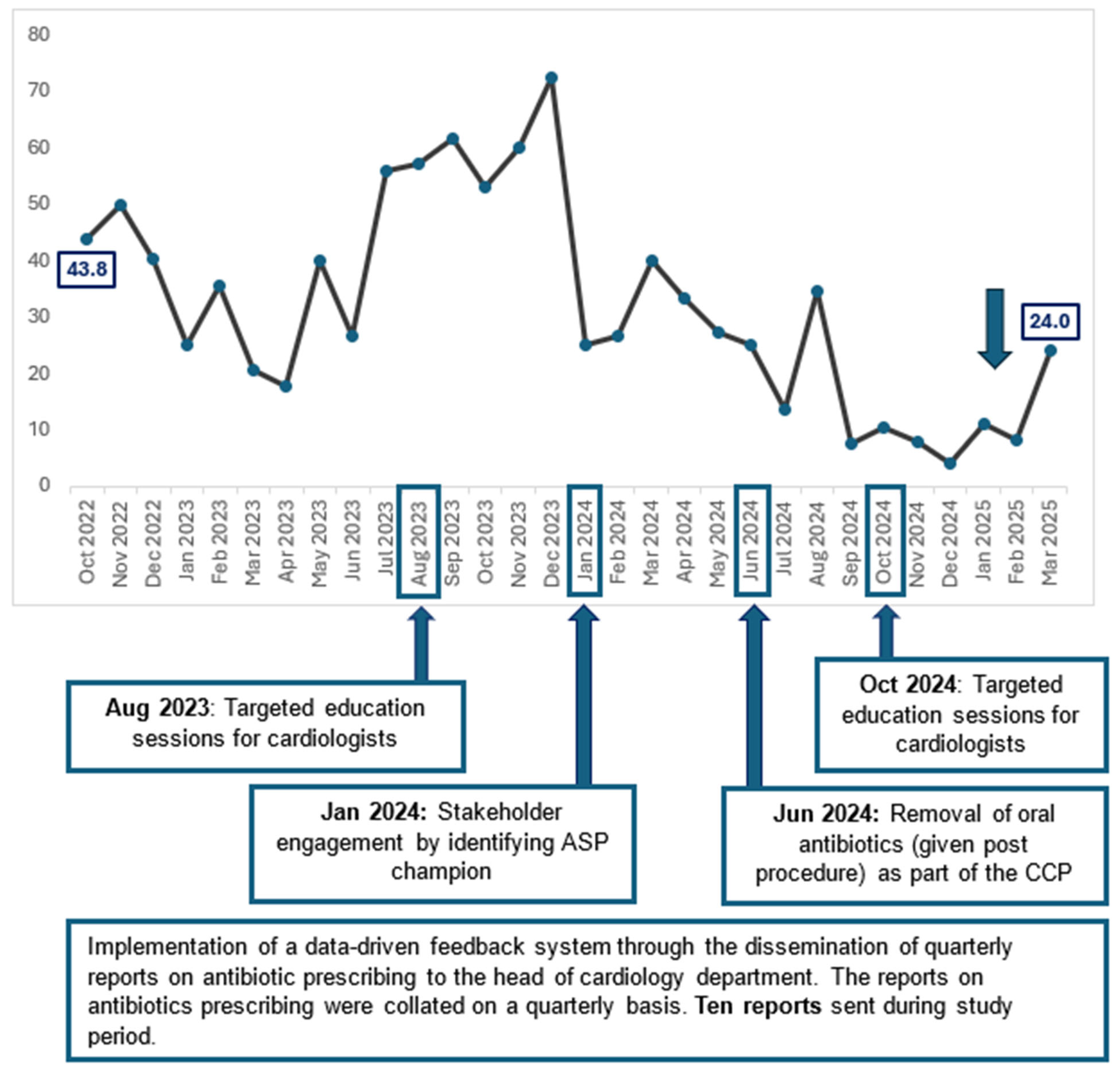
2.3.1. Implementation of a Data-Driven Feedback System Specifically on Antibiotic Use in Surgical Prophylaxis
2.3.2. Targeted Education Sessions for Cardiologists
2.3.3. Stakeholder Engagement by Identifying ASP Champions in Department of Cardiology and Partnering Them in ASP Activities
2.3.4. Clinical Pathway Optimisation Through Revisions to the Coordinated Clinical Pathway (CCP) for Pacemaker Insertion and Generator Change
2.4. Statistical Methods
3. Results
3.1. Surgical Prophylaxis
3.2. Surgical Site Infection Rates
3.3. Proportion of Inpatients on Antibiotics
4. Discussion
4.1. Impact of ASP on Extended Surgical Prophylaxis
4.2. Impact of Standard vs. Extended Prophylaxis on Surgical Site Infections, Clinical Care and Healthcare Costs
4.3. Impact of ASP Interventions on Surgical Prophylaxis with Spillover Effects on Antibiotic Consumption
4.4. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barlam, T.F.; Cosgrove, S.E.; Abbo, L.M.; MacDougall, C.; Schuetz, A.N.; Septimus, E.J.; Srinivasan, A.; Dellit, T.H.; Falck-Ytter, Y.T.; Fishman, N.O.; et al. SHEA/IDSA Clinical Practice Guidelines for Implementing an Antimicrobial Stewardship Program. Clin. Infect. Dis. 2016, 62, e51–e77. [Google Scholar] [CrossRef] [PubMed]
- Loo, L.W.; Liew, Y.X.; Lee, W.; Lee, L.W.; Chlebicki, P.; Kwa, A.L.-H. Discontinuation of antibiotic therapy within 24 hours of treatment initiation for patients with no clinical evidence of bacterial infection: A 5-year safety and outcome study from Singapore General Hospital Antimicrobial Stewardship Program. Int. J. Antimicrob. Agents 2019, 53, 606–611. [Google Scholar] [CrossRef] [PubMed]
- Liew, Y.X.; Lee, W.; Loh, J.C.Z.; Cai, Y.; Tang, S.S.L.; Lim, C.L.L.; Teo, J.; Ong, R.W.Q.; Kwa, A.L.-H.; Chlebicki, M.P. Impact of an antimicrobial stewardship programme on patient safety in Singapore General Hospital. Int. J. Antimicrob. Agents 2012, 40, 55–60. [Google Scholar] [CrossRef]
- Ng, T.M.; Ang, L.W.; Heng, S.T.; Kwa, A.L.-H.; Wu, J.E.; Seah, X.F.V.; Lee, S.Y.; Seah, J.; Choo, R.; Lim, P.L.; et al. Antibiotic utilisation and resistance over the first decade of nationally funded antimicrobial stewardship programmes in Singapore acute-care hospitals. Antimicrob. Resist. Infect. Control 2023, 12, 82. [Google Scholar] [CrossRef]
- Cai, Y.; Venkatachalam, I.; Tee, N.W.; Tan, T.Y.; Kurup, A.; Wong, S.Y.; Low, C.Y.; Wang, Y.; Lee, W.; Liew, Y.X.; et al. Prevalence of Healthcare-Associated Infections and Antimicrobial Use Among Adult Inpatients in Singapore Acute-Care Hospitals: Results From the First National Point Prevalence Study. Clin. Infect. Dis. 2017, 64, S61–S67. [Google Scholar] [CrossRef]
- Versporten, A.; Zarb, P.; Caniaux, I.; Gros, M.-F.; Drapier, N.; Miller, M.; Jarlier, V.; Nathwani, D.; Goossens, H.; Koraqi, A.; et al. Antimicrobial consumption and resistance in adult hospital inpatients in 53 countries: Results of an internet-based global point prevalence study. Lancet Glob. Health 2018, 6, e619–e629. [Google Scholar] [CrossRef]
- Kusumoto, F.M.; Schoenfeld, M.H.; Wilkoff, B.L.; Berul, C.I.; Birgersdotter-Green, U.M.; Carrillo, R.; Cha, Y.-M.; Clancy, J.; Deharo, J.-C.; Ellenbogen, K.A.; et al. 2017 HRS expert consensus statement on cardiovascular implantable electronic device lead management and extraction. Heart Rhythm 2017, 14, e503–e551, Erratum in Heart Rhythm 2021, 18, 1814. [Google Scholar] [CrossRef]
- Baddour, L.M.; Epstein, A.E.; Erickson, C.C.; Knight, B.P.; Levison, M.E.; Lockhart, P.B.; Masoudi, F.A.; Okum, E.J.; Wilson, W.R.; Beerman, L.B. Update on cardiovascular implantable electronic device infections and their management: A scientific statement from the American Heart Association. Circulation 2010, 121, 458–477. [Google Scholar] [CrossRef]
- Khan, N.K.; Subramaniam, V.; Hee, C. Antibiotic prophylaxis for permanent pacemaker implantation: An observational study of practice in England. Br. J. Cardiol 2010, 17, 144–147. [Google Scholar]
- de Oliveira, J.C.; Martinelli, M.; Nishioka, S.A.D.O.; Varejão, T.; Uipe, D.; Pedrosa, A.A.A.; Costa, R.; Danik, S.B. Efficacy of antibiotic prophylaxis before the implantation of pacemakers and cardioverter-defibrillators: Results of a large, prospective, randomized, double-blinded, placebo-controlled trial. Circ. Arrhythmia Electrophysiol. 2009, 2, 29–34. [Google Scholar] [CrossRef]
- Da Costa, A.; Kirkorian, G.; Cucherat, M.; Delahaye, F.; Chevalier, P.; Cerisier, A.; Isaaz, K.; Touboul, P. Antibiotic prophylaxis for permanent pacemaker insertion: A meta-analysis. Circulation 1998, 97, 1796–1801. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.; Huang, T.; Lin, L.; Lee, P.; Lin, C.; Lee, C.; Chao, T.; Li, Y.; Chen, J. Efficacy of postoperative prophylactic antibiotics in reducing permanent pacemaker infections. Clin. Cardiol. 2017, 40, 559–565. [Google Scholar] [CrossRef] [PubMed]
- Kabulski, G.M.; Northup, A.; Wiggins, B.S. Postoperative Antibiotic Prophylaxis Following Cardiac Implantable Electronic Device Placement. J. Innov. Card. Rhythm. Manag. 2019, 10, 3777–3784. [Google Scholar] [PubMed]
- Krahn, A.D.; Longtin, Y.; Philippon, F.; Birnie, D.H.; Manlucu, J.; Angaran, P.; Rinne, C.; Coutu, B.; Low, R.A.; Essebag, V. Prevention of Arrhythmia Device Infection Trial—The PADIT Trial. J. Am. Coll. Cardiol. 2018, 72, 3098–3109. [Google Scholar] [CrossRef]
- Rennert-May, E.; Leal, J.; Zhang, Z.; Rajakumar, I.; Smith, S.; Conly, J.M.; Exner, D.; Kuriachan, V.; Chew, D. Rates of post procedural prophylactic antibiotic use following cardiac implantable electronic device insertion and the impact on surgical site infections in Alberta, Canada. Antimicrob. Resist. Infect. Control 2024, 13, 147. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). National Healthcare Safety Network (NHSN) Patient Safety Component Manual; CDC: Atlanda, GA, USA, 2024; Chapter 9: Surgical Site Infection (SSI) Event. [Google Scholar]
- Surat, G.; Bernsen, D.; Schimmer, C. Antimicrobial Stewardship measures in cardiac surgery and its impact on surgical site infections. J. Cardiothorac. Surg. 2021, 16, 309. [Google Scholar] [CrossRef]
- Charani, E.; Edwards, R.; Sevdalis, N.; Alexandrou, B.; Sibley, E.; Mullett, D.; Franklin, B.D.; Holmes, A. Behavior Change Strategies to Influence Antimicrobial Prescribing in Acute Care: A Systematic Review. Clin. Infect. Dis. 2011, 53, 651–662. [Google Scholar] [CrossRef]
- Davey, P.; Peden, C.; Charani, E.; Marwick, C.; Michie, S. Time for action—Improving the design and reporting of behaviour change interventions for antimicrobial stewardship in hospitals: Early findings from a systematic review. Int. J. Antimicrob. Agents 2015, 45, 203–212. [Google Scholar] [CrossRef]
- Davey, P.; Marwick, C.A.; Scott, C.L.; Charani, E.; McNeil, K.; Brown, E.; Gould, I.M.; Ramsay, C.R.; Michie, S. Interventions to improve antibiotic prescribing practices for hospital inpatients (Review). Cochrane Database Syst. Rev. 2017, CD003543. [Google Scholar] [CrossRef]
- Zheng, K.; Xie, Y.; Dan, L.; Mao, M.; Chen, J.; Li, R.; Wang, X.; Hesketh, T. Effectiveness of Educational Interventions for Health Workers on Antibiotic Prescribing in Outpatient settings in China: A Systematic Review and Meta-Analysis. Antibiotics 2022, 11, 791. [Google Scholar] [CrossRef]
- Yong, C.W.; Choe, R.; Chua, S.K.X.; Lum, J.L.; Wang, W.C.-W. Utilising a COM-B framework to modify antibiotic prescription behaviours following third molar surgeries. Ann. Acad. Med. Singap. 2025, 54, 340–349. [Google Scholar] [CrossRef] [PubMed]
- Cialdini, R.B. The Psychology of Persuasion (Revised Edition); Harper Business: New York City, NY, USA, 2009. [Google Scholar]
- Borek, A.J.; Campbell, A.; Dent, E.; Moore, M.; Butler, C.C.; Holmes, A.; McLeod, M.; Tonkin-Crine, S.; on behalf of the STEP-UP study team; Anyanwu, P.E.; et al. Development of an intervention to support the implementation of evidence-based strategies for optimising antibiotic prescribing in general practice. Implement. Sci. Commun. 2021, 2, 104. [Google Scholar] [CrossRef] [PubMed]
- Hurst, A.L.; Child, J.; Pearce, K.; Palmer, C.; Todd, J.K.; Parker, S.K. Handshake Stewardship: A Highly Effective Rounding-based Antimicrobial Optimization Service. Pediatr. Infect. Dis. J. 2016, 35, 1104–1110. [Google Scholar] [CrossRef] [PubMed]
- Neuner, E.A.; Atkinson, A.; Ilges, D.; Krekel, T.; Ritchie, D.J.; Bewley, A.F.; Durkin, M.J.; Hsueh, K.; Sayood, S. Mixed methods evaluation of handshake antimicrobial stewardship on adult inpatient medicine floors. Antimicrob. Steward. Healthc. Epidemiol. 2023, 3, e210. [Google Scholar] [CrossRef]
- Kosharek, A.; Neuner, E.; Welch, E.; January, S.; Bewley, A.; Hsueh, K.; Sayood, S. Handshake Antimicrobial stewardship for adult surgical patients. Antimicrob. Steward. Healthc. Epidemiol. 2025, 5, 46. [Google Scholar] [CrossRef]
- Martinez-Sobalvarro, J.V.; Júnior, A.A.P.; Pereira, L.B.; Baldoni, A.O.; Ceron, C.S.; dos Reis, T.M. Antimicrobial stewardship for surgical antibiotic prophylaxis and surgical site infections: A systematic review. Int. J. Clin. Pharm. 2022, 44, 301–319. [Google Scholar] [CrossRef]
- Asundi, A.; Stanislawski, M.; Mehta, P.; Barón, A.E.; Gold, H.; Mull, H.; Ho, P.M.; Gupta, K.; Branch-Elliman, W. Prolonged antimicrobial prophylaxis following cardiac device procedures increases preventable harm: Insights from the VA CART program. Infect. Control Hosp. Epidemiol. 2018, 39, 1030–1036. [Google Scholar] [CrossRef]
- Baillargeon, J.; Holmes, H.M.; Lin, Y.-L.; Raji, M.A.; Sharma, G.; Kuo, Y.-F. Concurrent Use of Warfarin and Antibiotics and the Risk of Bleeding in Older Adults. Am. J. Med. 2012, 125, 183–189. [Google Scholar] [CrossRef]
- Spanakis, M.; Alon-Ellenbogen, D.; Ioannou, P.; Spernovasilis, N. Antibiotics and Lipid-Modifying Agents: Potential Drug-Drug Interactions and Their Clinical Implications. Pharmacy 2023, 11, 130. [Google Scholar] [CrossRef]
- Vega, A.J.; Smith, C.; Matejowsky, H.G.; Thornhill, K.J.; Borne, G.E.; Mosieri, C.N.; Shekoohi, S.; Cornett, E.M.; Kaye, A.D. Warfarin and Antibiotics: Drug Interactions and Clinical Considerations. Life 2023, 13, 1661. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
|
Standard Prophylaxis N = 380 |
Extended Prophylaxis N = 399 | p-Value | |
|---|---|---|---|
| Male (%) | 241 (63.4) | 244 (61.2) | 0.514 |
| Patients with diabetes mellitus (%) | 131 (34.5) | 147 (36.8) | 0.446 |
| Mean weight (kg) ± S.D. | 62.7 ± 15.9 | 62.4 ± 14.2 | 0.295 |
| Mean age ± S.D. | 72.5 ± 12.3 | 73.0 ± 13.9 | 0.728 |
| No. of MRSA colonisation (%) | 6 (1.6) | 9 (2.3) | 0.492 |
| Antibiotics used in prophylaxis | |||
| IV Cefazolin (%) | 304 (80.0) | N.A. | |
| IV Vancomycin (%) | 76 (20.0) | N.A. | |
| PO Cefalexin (%) | N.A. | 8 (2.0) | |
| PO Cefuroxime (%) | N.A. | 368 (92.2) | |
| PO Clindamycin (%) | N.A. | 23 (5.8) | |
| Mean duration of oral antibiotics used in extended prophylaxis ± S.D. (days) | N.A. | 3.3 ± 0.8 | |
| No. of surgical site infections (%) | 3 (0.8) | 3 (0.8) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Loo, L.W.; Zhou, Y.P.; Wang, Y.B.; Lee, L.W.; Chung, J.S. Antimicrobial Stewardship in Cardiac Device Surgery: Impact of Behavioural Change Interventions on Extended Prophylaxis Practices. Antibiotics 2025, 14, 754. https://doi.org/10.3390/antibiotics14080754
Loo LW, Zhou YP, Wang YB, Lee LW, Chung JS. Antimicrobial Stewardship in Cardiac Device Surgery: Impact of Behavioural Change Interventions on Extended Prophylaxis Practices. Antibiotics. 2025; 14(8):754. https://doi.org/10.3390/antibiotics14080754
Chicago/Turabian StyleLoo, Li Wen, Yvonne Peijun Zhou, Yi Bo Wang, Lai Wei Lee, and Jasmine Shimin Chung. 2025. "Antimicrobial Stewardship in Cardiac Device Surgery: Impact of Behavioural Change Interventions on Extended Prophylaxis Practices" Antibiotics 14, no. 8: 754. https://doi.org/10.3390/antibiotics14080754
APA StyleLoo, L. W., Zhou, Y. P., Wang, Y. B., Lee, L. W., & Chung, J. S. (2025). Antimicrobial Stewardship in Cardiac Device Surgery: Impact of Behavioural Change Interventions on Extended Prophylaxis Practices. Antibiotics, 14(8), 754. https://doi.org/10.3390/antibiotics14080754