
Direct Disk Diffusion Testing and Antimicrobial Stewardship for Gram-Negative Bacteremia in the Context of High Multidrug Resistance
 , , ,
, , ,
Abstract
1. Introduction
2. Results
2.1. Patient Characteristics
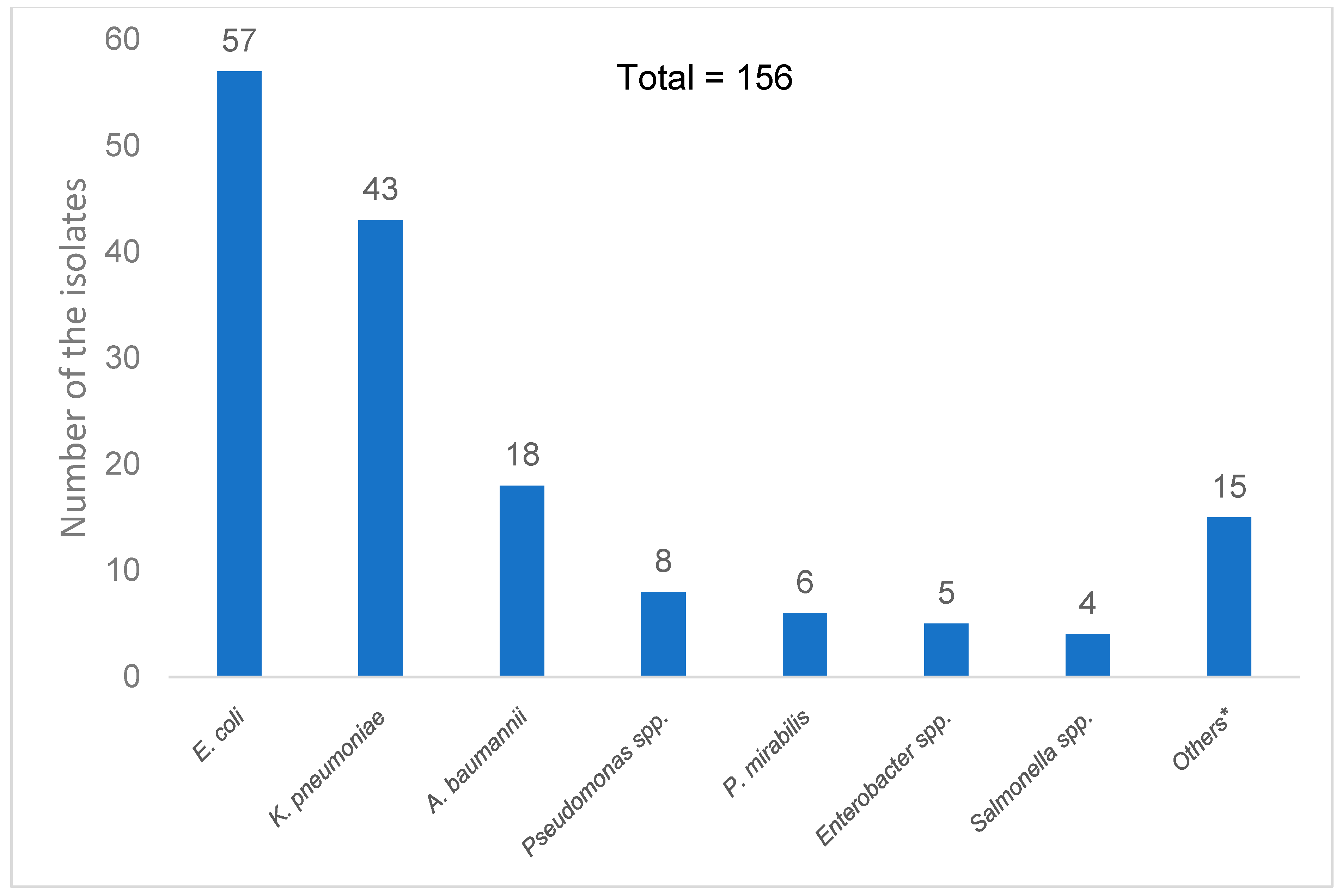
2.2. Infectious Source, Microbiological Findings, and Antimicrobial Therapy
2.3. Empirical and Definitive Antibiotic Therapy
2.4. Accuracy of Direct Disk Diffusion Test
2.5. Antibiotic Adjustments and Time to Optimal Therapy
2.6. Clinical Outcomes
2.7. Subgroup Analysis in the Patients with Multidrug-Resistant Bacteremia
2.8. Factors Associated with Death
3. Discussion
4. Materials and Methods
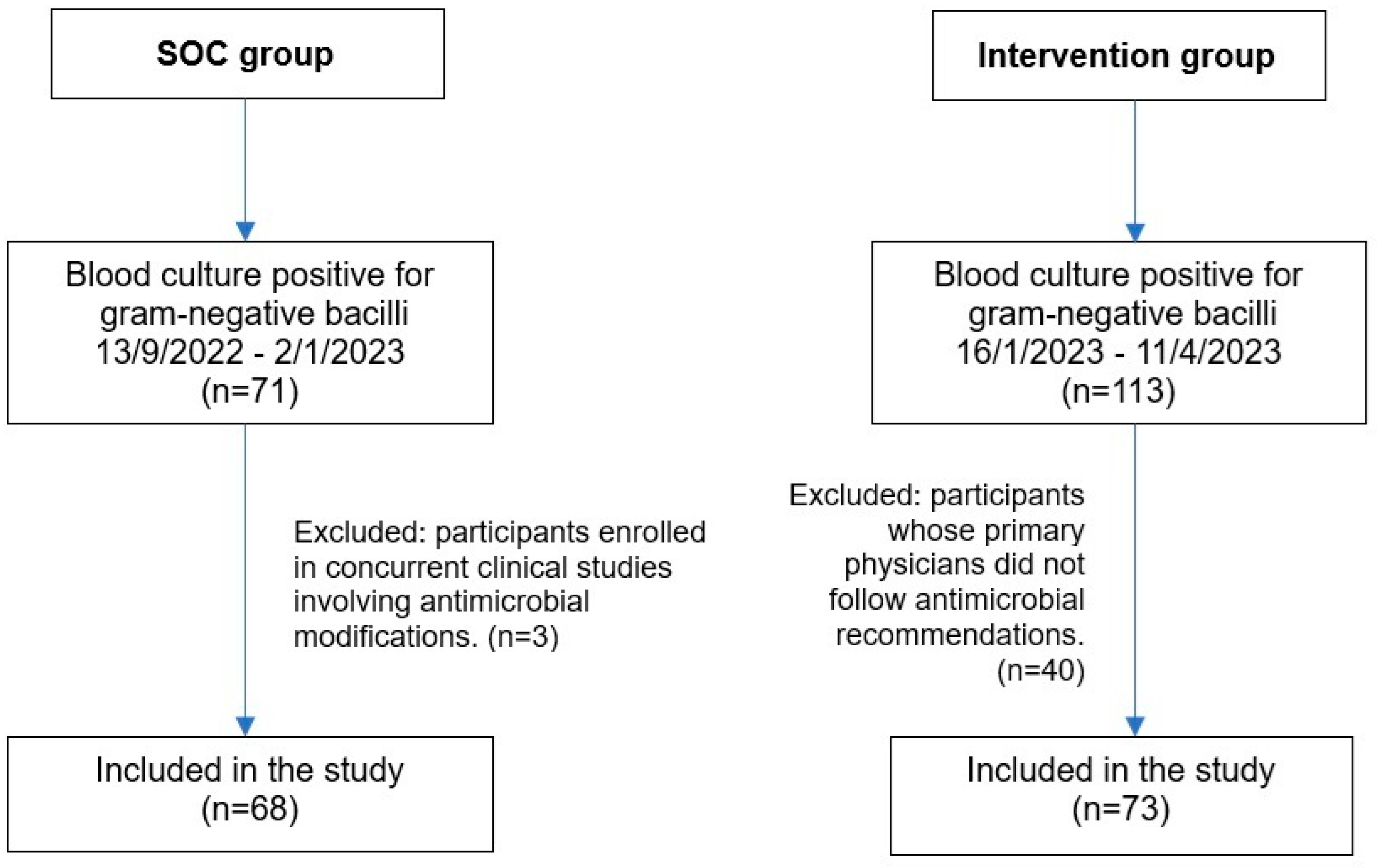
4.1. Study Design
4.2. Study Population
4.3. Disk Diffusion Susceptibility Testing
4.4. Intervention and Antimicrobial Stewardship Protocol
4.5. Definitions of Study Outcomes
4.6. Outcome Measures
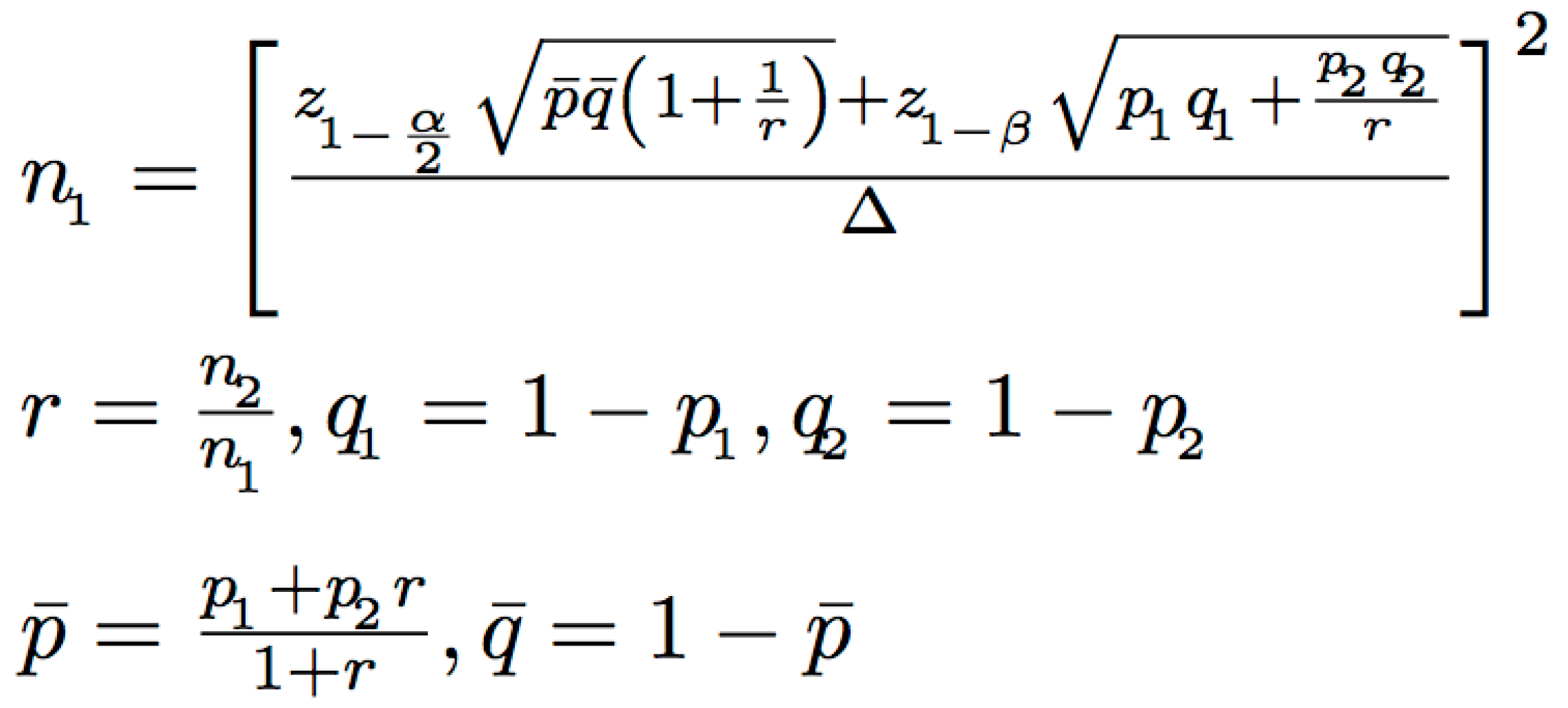
4.7. Statistical Analysis
4.8. Ethical Consideration
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| GNBSIs | Gram-negative blood stream infections |
| MDR | Multidrug-resistant |
| RAST | Rapid antimicrobial susceptibility testing |
| AMS | Antimicrobial stewardship |
| LOS | Length of stay |
| DD | Disk diffusion |
| CLSI | Clinical and Laboratory Standards Institute |
| SOFA | Sequential Organ Failure Assessment |
| WBC | White blood cell |
| SOC | Standard of care |
| CA | Categorical agreement |
| mE | Minor errors |
| ME | Major errors |
| VME | Very major errors |
| ICU | Intensive care unit |
| cOR | Crude odds ratio |
| aOR | Adjusted odds ratio |
| MHA | Mueller-Hinton agar |
| XDR | Extremely drug-resistant |
| UCS | Universal Coverage Scheme |
| SSS | Social Security Scheme |
| CSMBS | Civil Servant Medical Benefit Scheme |
| ESBL | Extended-spectrum beta-lactamase |
| AmpC-E | AmpC β-lactamase-producing Enterobacterales |
| CRE | Carbapenem-resistant Enterobacterales |
| CRAB | Carbapenem-resistant Acinetobacter baumannii |
| PK/PD | Pharmacokinetics and pharmacodynamics |
| SD | Standard deviation |
| IQR | Interquartile range |
| CI | Confidence intervals |
References
- Sligl, W.I.; Dragan, T.; Smith, S.W. Nosocomial Gram-Negative Bacteremia in Intensive Care: Epidemiology, Antimicrobial Susceptibilities, and Outcomes. Int. J. Infect. Dis. 2015, 37, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Kadri, S.S.; Lai, Y.L.; Warner, S.; Strich, J.R.; Babiker, A.; Ricotta, E.E.; Demirkale, C.Y.; Dekker, J.P.; Palmore, T.N.; Rhee, C.; et al. Inappropriate Empirical Antibiotic Therapy for Bloodstream Infections Based on Discordant In-Vitro Susceptibilities: A Retrospective Cohort Analysis of Prevalence, Predictors, and Mortality Risk in US Hospitals. Lancet Infect. Dis. 2021, 21, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Zilberberg, M.D.; Shorr, A.F.; Micek, S.T.; Vazquez-Guillamet, C.; Kollef, M.H. Multi-Drug Resistance, Inappropriate Initial Antibiotic Therapy and Mortality in Gram-Negative Severe Sepsis and Septic Shock: A Retrospective Cohort Study. Crit. Care 2014, 18, 596. [Google Scholar] [CrossRef] [PubMed]
- Rhee, C.; Kadri, S.S.; Dekker, J.P.; Danner, R.L.; Chen, H.C.; Fram, D.; Zhang, F.; Wang, R.; Klompas, M. Prevalence of Antibiotic-Resistant Pathogens in Culture-Proven Sepsis and Outcomes Associated with Inadequate and Broad-Spectrum Empiric Antibiotic Use. JAMA Netw. Open 2020, 3, e202899. [Google Scholar] [CrossRef] [PubMed]
- Marquet, K.; Liesenborgs, A.; Bergs, J.; Vleugels, A.; Claes, N. Incidence and Outcome of Inappropriate In-Hospital Empiric Antibiotics for Severe Infection: A Systematic Review and Meta-Analysis. Crit. Care 2015, 19, 63. [Google Scholar] [CrossRef] [PubMed]
- Ponyon, J.; Kerdsin, A.; Preeprem, T.; Ungcharoen, R. Risk Factors of Infections Due to Multidrug-Resistant Gram-Negative Bacteria in a Community Hospital in Rural Thailand. Trop. Med. Infect. Dis. 2022, 7, 328. [Google Scholar] [CrossRef] [PubMed]
- Chaisathaphol, T.; Chayakulkeeree, M. Epidemiology of Infections Caused by Multidrug-Resistant Gram-Negative Bacteria in Adult Hospitalized Patients at Siriraj Hospital. J. Med. Assoc. Thail. 2014, 97, S35–S45. [Google Scholar] [PubMed]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; Mcintyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. Intensive Care Med. 2021, 47, 1181–1247. [Google Scholar] [CrossRef] [PubMed]
- Tamma, P.D.; Heil, E.L.; Justo, J.A.; Mathers, A.J.; Satlin, M.J.; Bonomo, R.A. Infectious Diseases Society of America 2024 Guidance on the Treatment of Antimicrobial-Resistant Gram-Negative Infections. Clin. Infect. Dis. 2024, ciae403. [Google Scholar] [CrossRef] [PubMed]
- Paul, M.; Carrara, E.; Retamar, P.; Tängdén, T.; Bitterman, R.; Bonomo, R.A.; de Waele, J.; Daikos, G.L.; Akova, M.; Harbarth, S.; et al. European Society of Clinical Microbiology and Infectious Diseases (ESCMID) Guidelines for the Treatment of Infections Caused by Multidrug-Resistant Gram-Negative Bacilli (Endorsed by European Society of Intensive Care Medicine). Clin. Microbiol. Infect. 2022, 28, 521–547. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, D.; Kerdsin, A.; Akeda, Y.; Sugawara, Y.; Sakamoto, N.; Matsumoto, Y.; Motooka, D.; Ishihara, T.; Nishi, I.; Laolerd, W.; et al. Nationwide Surveillance in Thailand Revealed Genotype-Dependent Dissemination of Carbapenem-Resistant Enterobacterales. Microb. Genom. 2022, 8, 797. [Google Scholar] [CrossRef] [PubMed]
- Tibbetts, R.; George, S.; Burwell, R.; Rajeev, L.; Rhodes, P.A.; Singh, P.; Samuel, L. Performance of the reveal rapid antibiotic susceptibility testing system on Gram-negative blood cultures at a large urban hospital. J. Clin. Microbiol. 2022, 60, e0009822. [Google Scholar] [CrossRef] [PubMed]
- Savage, T.J.; Rao, S.; Joerger, J.; Ozonoff, A.; McAdam, A.J.; Sandora, T.J. Predictive Value of Direct Disk Diffusion Testing from Positive Blood Cultures in a Children’s Hospital and Its Utility in Antimicrobial Stewardship. J. Clin. Microbiol. 2021, 59, e02445-20. [Google Scholar] [CrossRef] [PubMed]
- Giacobbe, D.R.; Giani, T.; Bassetti, M.; Marchese, A.; Viscoli, C.; Rossolini, G.M. Rapid Microbiological Tests for Bloodstream Infections Due to Multidrug Resistant Gram-Negative Bacteria: Therapeutic Implications. Clin. Microbiol. Infect. 2020, 26, 713–722. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, R.; Humphries, R. Rapid Antimicrobial Susceptibility Testing Methods for Blood Cultures and Their Clinical Impact. Front. Med. 2021, 8, 635831. [Google Scholar] [CrossRef] [PubMed]
- MacVane, S.H.; Dwivedi, H.P. Evaluating the Impact of Rapid Antimicrobial Susceptibility Testing for Bloodstream Infections: A Review of Actionability, Antibiotic Use and Patient Outcome Metrics. J. Antimicrob. Chemother. 2024, 79, i13–i25. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Kim, I.; Kang, C.K.; Jun, K.I.; Yoo, S.H.; Chun, J.Y.; Jung, J.; Kim, Y.J.; Kim, D.Y.; Jo, H.B.; et al. Enhanced Antimicrobial Stewardship Based on Rapid Phenotypic Antimicrobial Susceptibility Testing for Bacteraemia in Patients with Haematological Malignancies: A Randomized Controlled Trial. Clin. Microbiol. Infect. 2021, 27, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, R.; Komarow, L.; Virk, A.; Rajapakse, N.; Schuetz, A.N.; Dylla, B.; Earley, M.; Lok, J.; Kohner, P.; Ihde, S.; et al. Randomized Trial Evaluating Clinical Impact of RAPid IDentification and Susceptibility Testing for Gram-Negative Bacteremia: RAPIDS-GN. Clin. Infect. Dis. 2021, 73, e39–e46. [Google Scholar] [CrossRef] [PubMed]
- Ventres, J.J.; Ting, M.H.; Parente, D.M.; Rogers, R.; Norris, A.M.; Benitez, G.; Shehadeh, F.; Bobenchik, A.M.; Mylonakis, E.; Chapin, K.C.; et al. Combination of a Rapid Diagnostic Assay and Antimicrobial Stewardship Intervention for Gram-Negative Bacteremia. Open Forum Infect. Dis. 2024, 11, ofae477. [Google Scholar] [CrossRef] [PubMed]
- Rajshekar, D.; Chaudhari, K.V.; Bhat, P.; Prakash, S.S.; Raghvan, R.; Vasanth, S.; Jayakar, S.; Sugumaran, R.; Kannambath, R.; Chowdury, S.; et al. Evaluation of performance of direct disk diffusion test from positively flagged blood culture broth: A large scale study from South India. J. Lab. Physicians 2019, 11, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Jonasson, E.; Matuschek, E.; Kahlmeter, G. The EUCAST Rapid Disc Diffusion Method for Antimicrobial Susceptibility Testing Directly from Positive Blood Culture Bottles. J Antimicrob. Chemotherapy 2020, 75, 968–978. [Google Scholar] [CrossRef] [PubMed]
- Chandrasekaran, S.; Abbott, A.; Campeau, S.; Zimmer, B.L.; Weinstein, M.; Thrupp, L.; Hejna, J.; Walker, L.; Ammann, T.; Kirn, T.; et al. Direct-from-Blood-Culture Disk Diffusion to Determine Antimicrobial Susceptibility of Gram-Negative Bacteria: Preliminary Report from the Clinical and Laboratory Standards Institute Methods Development and Standardization Working Group. J. Clin. Microbiol. 2018, 56, e01678-17. [Google Scholar] [CrossRef] [PubMed]
- CLSI Supplement M100; Performance Standards for Antimicrobial Susceptibility Testing. Clinical and Laboratory Standards Institute (CLSI): Wayne, PA, USA, 2025.
- Jhaveri, T.A.; Taqi, A.; Pearson, J.C.; Kanjilal, S. Impact of Direct Disk-Diffusion Testing on Time to Optimal Antibiotic Therapy. Antimicrob. Steward. Healthc. Epidemiol. 2023, 3, e59. [Google Scholar] [CrossRef]
- Pilmis, B.; Thy, M.; Diep, J.; Krob, S.; Périllaud, C.; Couzigou, C.; Vidal, B.; Mizrahi, A.; Lourtet-Hascoët, J.; Le Monnier, A.; et al. Clinical Impact of Rapid Susceptibility Testing on MHR-SIR Directly from Blood Cultures. J Antimicrob. Chemother. 2019, 74, 3063–3068. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Kim, T.S.; Song, S.H.; Choi, J.; Han, S.; Kim, D.Y.; Kwon, S.; Lee, E.; Song, K.H.; Choe, P.G.; et al. Direct Rapid Antibiotic Susceptibility Test (DRAST) for Blood Culture and Its Potential Usefulness in Clinical Practice. J. Med. Microbiol. 2018, 67, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, R.; Giri, A.; Komarow, L.; Souli, M.; Doernberg, S.B.; Patel, R. Impact of rapid antibiotic susceptibility testing for Gram-negative bacteremia varies by pathogen type and resistance: A secondary analysis of the RAPIDS GN trial. Microbiol. Spectr. 2025, 13, e0178924. [Google Scholar] [CrossRef] [PubMed]
- Deawtrakulchai, P.; Cheawchanwattana, S.; Sribenjalux, W.; Meesing, A. The Comparative Accuracy of Pooled vs Individual Blood Culture Sampling Methods for Diagnosis of Catheter-Related Bloodstream Infection. BMC Infect. Dis. 2022, 22, 622. [Google Scholar] [CrossRef] [PubMed]
- CLSI Supplement M100; Performance Standards for Antimicrobial Susceptibility Testing. Clinical and Laboratory Standards Institute (CLSI): Wayne, PA, USA, 2022.
- Tiengrim, S.; Mootsikapun, P.; Wonglakorn, L.; Changpradub, D.; Thunyaharn, S.; Tantisiriwat, W.; Santiwatanakul, S.; Malithong, A.; U-thainual, N.; Kiratisin, P.; et al. Comparative In Vitro Activity of Sitafloxacin Against Bacteria Isolated from Thai Patients with Urinary Tract Infections and Lower Respiratory Tract Infections in 2016. J. Med. Assoc. Thail. 2017, 100, 1061–1072. [Google Scholar]
- Centers for Disease Control and Prevention (CDC). Facility Guidance for Control of Carbapenem-Resistant Enterobacteriaceae (CRE): November 2015 Update—CRE Toolkit. Available online: https://www.cdc.gov/hai/pdfs/cre/cre-guidance-508.pdf (accessed on 17 May 2025).
- Tamma, P.D.; Aitken, S.L.; Bonomo, R.A.; Mathers, A.J.; van Duin, D.; Clancy, C.J. Infectious Diseases Society of America Guidance on the Treatment of Extended-Spectrum β-Lactamase Producing Enterobacterales (ESBL-E), Carbapenem-Resistant Enterobacterales (CRE), and Pseudomonas aeruginosa with Difficult-to-Treat Resistance (DTR-P. aeruginosa). Clin. Infect. Dis. 2021, 72, e169–e183. [Google Scholar] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Characteristics | SOC (N = 68) | Intervention (N = 73) | p-Value | |
|---|---|---|---|---|
| Male sex, no. (%) | 42 (61.8) | 43 (58.9) | 0.729 | |
| Age (years, mean (SD)) | 60.4 (16.1) | 62.6 (17.3) | 0.293 | |
| BMI (kg/m2, median (IQR)) | 22.6 (6.4) | 22.7 (6.1) | 0.800 | |
| Type of admission unit, no. (%) | 0.352 | |||
| Medicine | 33 (48.5) | 44 (60.3) | ||
| Surgery | 29 (42.6) | 23 (31.5) | ||
| Others * | 6 (8.8) | 6 (8.2) | ||
| Charlson comorbidity index (median, (IQR)) | 4 (5) | 4 (4) | 0.695 | |
| Underlying disease, no. (%) | ||||
| Solid organ malignancy | 23 (33.8) | 21 (28.8) | 0.517 | |
| DM | 19 (27.9) | 24 (32.9) | 0.525 | |
| Renal disease | 12 (17.6) | 14 (19.2) | 0.815 | |
| Liver disease | 8 (11.8) | 11 (15.1) | 0.566 | |
| Hematologic malignancy | 8 (11.8) | 9 (12.3) | 0.918 | |
| Coronary artery disease | 7 (10.3) | 4 (5.5) | 0.287 | |
| Cerebrovascular disease or TIA | 3 (4.4) | 4 (5.5) | 1.000 | |
| Solid organ transplantation | 4 (5.9) | 3 (4.1) | 0.771 | |
| Currently receiving immunosuppressive agent(s) | 20 (29.4) | 19 (26.0) | 0.653 | |
| SOC (N = 68) | Intervention (N = 73) | p-Value | |
|---|---|---|---|
| Clinical parameters | |||
| BT (Celsius degree, median (IQR)) | 38.7 (1.3) | 38.6 (1.8) | 0.856 |
| SBP (mmHg, mean (SD)) | 130.3 (20.7) | 131.0 (21.8) | 0.859 |
| MAP (mmHg, mean (SD)) | 92.0 (12.7) | 92.0 (14.2) | 0.890 |
| Glasgow Coma Score (median (range)) | 15 (9–15) | 15 (3–15) | 0.707 |
| Acute hypotensive episode (%) | 34 (50.0) | 31 (42.5) | 0.370 |
| Required vasopressor (%) | 24 (35.3) | 19 (26.0) | 0.232 |
| Required mechanical ventilation (%) | 14 (20.6) | 14 (19.2) | 0.843 |
| Neutropenia (%) | 6 (8.8) | 8 (11.0) | 0.672 |
| Admitted in ICU (%) | 22 (32.4) | 19 (26.0) | 0.409 |
| Pitt bacteremia score (median (range)) | 2 (0–7) | 2 (0–8) | 0.295 |
| SOFA score (median (range)) | 5 (0–18) | 4 (0–14) | 0.100 |
| Laboratory parameters | |||
| Hb (g/dL, median (IQR)) | 9.5 (3.1) | 10.0 (3.6) | 0.737 |
| WBC (cell/mm3, mean (SD)) | 15,442 (9893) | 11,809 (7800) | 0.016 |
| PMN (%, median (IQR)) | 84.2 (18) | 84.1 (23) | 0.506 |
| Platelets (×103 cell/mm3, median (IQR)) | 202.5 (167) | 176.5 (183) | 0.342 |
| Serum creatinine (mg/dL, median (IQR)) | 2.2 (1.4) | 1.5 (0.7) | 0.498 |
| ALT (U/L, median (IQR)) | 50 (78) | 50 (89) | 0.753 |
| TB (mg/dL, median (IQR)) | 1.3 (4.7) | 1.1 (1.9) | 0.641 |
| Albumin (g/dL, median (IQR)) | 3.2 (0.9) | 3.4 (1.0) | 0.049 |
| Lactate (mg/dL, median (IQR)) | 21.4 (19.9) | 23.1 (28.1) | 0.555 |
| PaO2:FiO2 ratio (median (IQR)) | 273 (213) | 350 (150) | 0.076 |
| Infectious Information | SOC (N = 68) | Intervention (N = 73) | p-Value | |
|---|---|---|---|---|
| Time from admission to blood culture collection (hours, median [IQR]) | 40.0 (293.5) | 21.3 (236.1) | 0.998 | |
| Healthcare-associated infection (%) | 35 (51.5) | 44 (60.3) | 0.293 | |
| Source of infection (%) | 0.396 | |||
| Intra-abdominal * | 23 (33.8) | 19 (26.0) | ||
| Urinary tract | 14 (20.6) | 23 (31.5) | ||
| Pneumonia | 9 (13.2) | 15 (20.5) | ||
| Primary bacteremia | 13 (19.1) | 9 (12.3) | ||
| Catheter-related blood stream infection | 5 (7.4) | 3 (4.1) | ||
| Skin and soft tissue | 4 (5.9) | 4 (5.5) | ||
| Polymicrobial Gram-negative bacteremia (%) | 10 (14.7) | 4 (5.5) | 0.067 | |
| Bacteremia from MDR pathogen | 34 (50.0) | 35 (47.9) | 0.807 | |
| Bacteremia from carbapenem-resistant pathogen | 24 (35.3) | 18 (24.7) | 0.168 | |
| Outcomes | Standard of Care (N = 68) | Intervention (N = 73) | p-Value |
|---|---|---|---|
| Antibiotic adjustments guided by RAST (%) Escalation De-escalation No adjustment | 0 (0.0) 0 (0.0) 0 (0.0) | 28 (38.4) 20 (27.4) 25 (34.2) | NA |
| Time to optimal targeted antibiotic (hour, median (IQR)) | 59.1 (68.1) | 40.0 (35.0) | 0.037 |
| Optimal targeted antibiotic in 48 h (%) | 25 (36.8) | 50 (68.5) | <0.001 |
| Optimal targeted antibiotic in 72 h (%) | 43 (62.3) | 63 (86.2) | 0.002 |
| Ineffective antibiotic in 48 h (%) | 19 (27.9) | 9 (12.3) | 0.002 |
| Ineffective antibiotic in 72 h (%) | 12 (17.6) | 2 (2.7) | 0.003 |
| Death within 72 h after official AST reporting (%) | 0 (0.0) | 0 (0.0) | NA |
| In the ICU 72 h after standard AST reporting (%) | 15 (22.1) | 15 (20.5) | 0.872 |
| Hospital-onset CDI (%) | 5 (7.4) | 4 (5.5) | 0.738 |
| Duration of vasopressor (hour, median (IQR)) | 51.0 (68.3) | 80.5 (115.8) | 0.208 |
| SOFA score at day 3 (median (IQR)) | 4 (5) | 4 (6) | 0.740 |
| Hospital LOS (day, median (IQR)) | 13 (11.8) | 11 (11.0) | 0.195 |
| Discharge alive (%) | 56 (82.4) | 58 (79.5) | 0.662 |
| 30-day mortality (%) | 12 (16.7) | 13 (17.2) | 0.980 |
| Cost in admission (Baht, median (IQR)) | 145,230 (226,433) | 98,606 (249,940) | 0.152 |
| Factors | cOR (95%CI) | p-Value | aOR (95%CI) | p-Value |
|---|---|---|---|---|
| Optimal targeted antibiotic in 72 h | 0.39 (0.16–0.95) | 0.037 | 0.42 (0.15–1.21) | 0.108 |
| Application of direct DD testing | 1.21 (0.52–2.80) | 0.662 | … | … |
| Bacteremia from MDR pathogen | 3.04 (1.23–7.50) | 0.016 | 3.01 (1.02–8.87) | 0.046 |
| Required mechanical ventilator support | 3.14 (1.24–7.95) | 0.016 | … | … |
| Admitted in ICU | 6.30 (2.59–12.7) | <0.001 | 6.13 (2.03–18.5) | 0.001 |
| Pneumonia | 4.20 (1.61–11.0) | 0.003 | 1.86 (0.60–5.77) | 0.286 |
| Charlson comorbidity index ≥5 | 1.85 (0.79–4.30) | 0.155 | … | … |
| Pitt bacteremia score ≥4 | 2.77 (1.10–6.93) | 0.030 | 1.28 (0.40–4.10) | 0.683 |
| SOFA score ≥6 | 2.30 (0.91–5.79) | 0.078 | … | … |
| Age ≥65 year | 1.54 (0.66–3.60) | 0.313 | … | … |
| BMI <21 kg/m2 | 2.43 (1.04–5.71) | 0.041 | 4.58 (1.54–13.7) | 0.006 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sribenjalux, W.; Kulwongroj, P.; Kuwatjanakul, W.; Wonglakorn, L.; Srisak, K.; Manomaiwong, N.; Meesing, A. Direct Disk Diffusion Testing and Antimicrobial Stewardship for Gram-Negative Bacteremia in the Context of High Multidrug Resistance. Antibiotics 2025, 14, 726. https://doi.org/10.3390/antibiotics14070726
Sribenjalux W, Kulwongroj P, Kuwatjanakul W, Wonglakorn L, Srisak K, Manomaiwong N, Meesing A. Direct Disk Diffusion Testing and Antimicrobial Stewardship for Gram-Negative Bacteremia in the Context of High Multidrug Resistance. Antibiotics. 2025; 14(7):726. https://doi.org/10.3390/antibiotics14070726
Chicago/Turabian StyleSribenjalux, Wantin, Pawarit Kulwongroj, Waewta Kuwatjanakul, Lumyai Wonglakorn, Kanuengnit Srisak, Natapong Manomaiwong, and Atibordee Meesing. 2025. "Direct Disk Diffusion Testing and Antimicrobial Stewardship for Gram-Negative Bacteremia in the Context of High Multidrug Resistance" Antibiotics 14, no. 7: 726. https://doi.org/10.3390/antibiotics14070726
APA StyleSribenjalux, W., Kulwongroj, P., Kuwatjanakul, W., Wonglakorn, L., Srisak, K., Manomaiwong, N., & Meesing, A. (2025). Direct Disk Diffusion Testing and Antimicrobial Stewardship for Gram-Negative Bacteremia in the Context of High Multidrug Resistance. Antibiotics, 14(7), 726. https://doi.org/10.3390/antibiotics14070726