
The Appearance of Antiphage Antibodies in Sera of Patients Treated with Phages

 , , , and
, , , and
Abstract
1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Bacteriophages
4.3. Plate Phage Neutralization Test
4.4. Categories of the Results of PT
- A—Pathogen eradication and/or recovery (eradication confirmed by the results of bacterial cultures. Recovery refers to wound healing or complete subsidence of the infection symptoms);
- B—Good clinical result (almost complete subsidence of some infection symptoms, together with significant improvement in the patient’s general condition after completion of PT);
- C—Clinical improvement (discernible reduction in the intensity of some infection symptoms after completion of PT to a degree not observed before PT, when no treatment was used).
- D—Questionable clinical improvement (reduction in the intensity of some infection symptoms to the degree that could also be observed before PT);
- E—Transient clinical improvement (reduction in the intensity of some infection symptoms observed only during the application of phage preparations and not after the termination of PT);
- F—No response to treatment (lack of reduction in the intensity of some infection symptoms observed before PT);
- G—Clinical deterioration (of symptoms of infection at the end of PT).
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Górski, A.; Międzybrodzki, R.; Węgrzyn, G.; Jończyk-Matysiak, E.; Borysowski, J.; Weber-Dąbrowska, B. Phage therapy: Current status and perspectives. Med. Res. Rev. 2020, 40, 459–463. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.; Wang, C.; Zhou, X.; Guo, X.; Yang, Y.; Liu, W.; Zhao, R.; Song, H. Bacteriophage therapy for drug-resistant Staphylococcus aureus infections. Front. Cell Infect. Microbiol. 2024, 14, 1336821. [Google Scholar] [CrossRef] [PubMed]
- Olawade, D.B.; Fapohunda, O.; Egbon, E.; Ebiesuwa, O.A.; Usman, S.O.; Faronbi, A.O.; Fidelis, S.C. Phage therapy: A targeted approach to overcoming antibiotic resistance. Microb. Pathog. 2024, 197, 107088. [Google Scholar] [CrossRef] [PubMed]
- Archana, A.; Patel, P.S.; Kumar, R.; Nath, G. Neutralizing antibody response against subcutaneously injected bacteriophages in rabbit model. Virusdisease 2021, 32, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Gembara, K.; Dąbrowska, K. Interaction of bacteriophages with the immune system: Induction of bacteriophage-specific antibodies. Methods Mol. Biol. 2024, 2734, 183–196. [Google Scholar] [CrossRef] [PubMed]
- Łusiak-Szelachowska, M.; Żaczek, M.; Weber-Dąbrowska, B.; Międzybrodzki, R.; Letkiewicz, S.; Fortuna, W.; Rogóż, P.; Szufnarowski, K.; Jończyk-Matysiak, E.; Olchawa, E.; et al. Antiphage activity of sera during phage therapy in relation to its outcome. Future Microbiol. 2017, 12, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Żaczek, M.; Łusiak-Szelachowska, M.; Jończyk-Matysiak, E.; Weber-Dąbrowska, B.; Międzybrodzki, R.; Owczarek, B.; Kopciuch, A.; Fortuna, W.; Rogóż, P.; Górski, A. Antibody production in response to staphylococcal MS-1 phage cocktail in patients undergoing phage therapy. Front. Microbiol. 2016, 7, 1681. [Google Scholar] [CrossRef] [PubMed]
- Nick, J.A.; Dedrick, R.M.; Gray, A.L.; Vladar, E.K.; Smith, B.E.; Freeman, K.G.; Malcolm, K.C.; Epperson, L.E.; Hasan, N.A.; Hendrix, J.; et al. Host and pathogen response to bacteriophage engineered against Mycobacterium abscessus lung infection. Cell 2022, 185, 1860–1874.e12. [Google Scholar] [CrossRef] [PubMed]
- Le, T.; Nang, S.C.; Zhao, J.; Yu, H.H.; Li, J.; Gill, J.J.; Liu, M.; Aslam, S. Therapeutic potential of intravenous phage as standalone therapy for recurrent drug-resistant urinary tract infections. Antimicrob. Agents Chemother. 2023, 67, e0003723. [Google Scholar] [CrossRef] [PubMed]
- Dan, J.M.; Lehman, S.M.; Al-Kolla, R.; Penziner, S.; Afshar, K.; Yung, G.; Golts, E.; Law, N.; Logan, C.; Kovach, Z.; et al. Development of host immune response to bacteriophage in a lung transplant recipient on adjunctive phage therapy for a multidrug-resistant pneumonia. J. Infect. Dis. 2023, 227, 311–316. [Google Scholar] [CrossRef] [PubMed]
- Dedrick, R.M.; Smith, B.E.; Cristinziano, M.; Freeman, K.G.; Jacobs-Sera, D.; Belessis, Y.; Whitney Brown, A.; Cohen, K.A.; Davidson, R.M.; van Duin, D.; et al. Phage therapy of Mycobacterium infections: Compassionate use of phages in 20 patients with drug-resistant mycobacterial disease. Clin. Infect. Dis. 2023, 76, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Bernabéu-Gimeno, M.; Pardo-Freire, M.; Chan, B.K.; Turner, P.E.; Gil-Brusola, A.; Pérez-Tarazona, S.; Carrasco-Hernández, L.; Quintana-Gallego, E.; Domingo-Calap, P. Neutralizing antibodies after nebulized phage therapy in cystic fibrosis patients. Med 2024, 5, 1096–1111.e6. [Google Scholar] [CrossRef] [PubMed]
- Berkson, J.D.; Wate, C.E.; Allen, G.B.; Schubert, A.M.; Dunbar, K.E.; Coryell, M.P.; Sava, R.L.; Gao, Y.; Hastie, J.L.; Smith, E.M.; et al. Phage-specific immunity impairs efficacy of bacteriophage targeting Vancomycin Resistant Enterococcus in a murine model. Nat. Commun. 2024, 15, 2993. [Google Scholar] [CrossRef] [PubMed]
- Dedrick, R.M.; Freeman, K.G.; Nguyen, J.A.; Bahadirli-Talbott, A.; Smith, B.E.; Wu, A.E.; Ong, A.S.; Lin, C.T.; Ruppel, L.C.; Parrish, N.M.; et al. Potent antibody-mediated neutralization limits bacteriophage treatment of a pulmonary Mycobacterium abscessus infection. Nat. Med. 2021, 27, 1357–1361. [Google Scholar] [CrossRef] [PubMed]
- Dedrick, R.M.; Freeman, K.G.; Nguyen, J.A.; Bahadirli-Talbott, A.; Cardin, M.E.; Cristinziano, M.; Smith, B.E.; Jeong, S.; Ignatius, E.H.; Lin, C.T.; et al. Nebulized bacteriophage in a patient with refractory Mycobacterium abscessus lung disease. Open Forum Infect. Dis. 2022, 9, ofac194. [Google Scholar] [CrossRef] [PubMed]
- Międzybrodzki, R.; Borysowski, J.; Weber-Dąbrowska, B.; Fortuna, W.; Letkiewicz, S.; Szufnarowski, K.; Pawełczyk, Z.; Rogóż, P.; Kłak, M.; Wojtasik, E.; et al. Clinical aspects of phage therapy. Adv. Virus Res. 2012, 83, 73–121. [Google Scholar] [CrossRef]
- Łobocka, M.; Hejnowicz, M.S.; Dąbrowski, K.; Gozdek, A.; Kosakowski, J.; Witkowska, M.; Ulatowska, M.I.; Weber-Dąbrowska, B.; Kwiatek, M.; Parasion, S.; et al. Genomics of staphylococcal Twort-like phages--potential therapeutics of the post-antibiotic era. Adv. Virus Res. 2012, 83, 143–216. [Google Scholar] [CrossRef] [PubMed]
- Żaczek, M.; Weber-Dąbrowska, B.; Łusiak-Szelachowska, M.; Międzbrodzki, R.; Górski, A. Polish contribution into the advancement of phage treatment in humans. In Bacterial Viruses: Exploitation for Biocontrol and Therapeutics; Coffey, A., Buttimer, C., Eds.; Caister Academic Press: Poole, UK, 2020; pp. 187–202. [Google Scholar] [CrossRef]
- Żaczek, M.; Górski, A.; Weber-Dąbrowska, B.; Letkiewicz, S.; Fortuna, W.; Rogóż, P.; Pasternak, E.; Międzybrodzki, R. A through synthesis of Phage Therapy Unit activity in Poland—Its history, milestones and international recognition. Viruses 2022, 14, 1170. [Google Scholar] [CrossRef] [PubMed]
- Pescovitz, M.D.; Torgerson, T.R.; Ochs, H.D.; Ocheltree, E.; McGee, P.; Krause-Steinrauf, H.; Lachin, J.M.; Canniff, J.; Greenbaum, C.; Herold, K.C.; et al. Effect of rituximab on human in vivo antibody immune responses. J. Allergy Clin. Immunol. 2011, 128, 1295–1302. [Google Scholar] [CrossRef] [PubMed]
- Adams, M.H. Methods of study of bacterial viruses. In Bacteriophages; Adams, M.H., Ed.; Interscience: New York, NY, USA, 1959; pp. 443–522. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| Patient No. | Type of Infection | Phages Used in PT | K Before PT | K During PT | K After PT | Days of PT | Clinical Outcome of PT a |
|---|---|---|---|---|---|---|---|
| 1 | soft tissue infection | Staph_1N | 0.27 | 0.36 | n.s. | 14 | D |
| 2 | bone infection | Staph_1N | 0.15 | 0.29 | n.s. | 18 | F |
| 3 | upper respiratory tract infection | Staph_1N | 0.19 | 0.67 | n.s. | 18 | F |
| 4 | bone infection | Staph_A5L | 0.04 | 0.38 | n.s. | 21 | F |
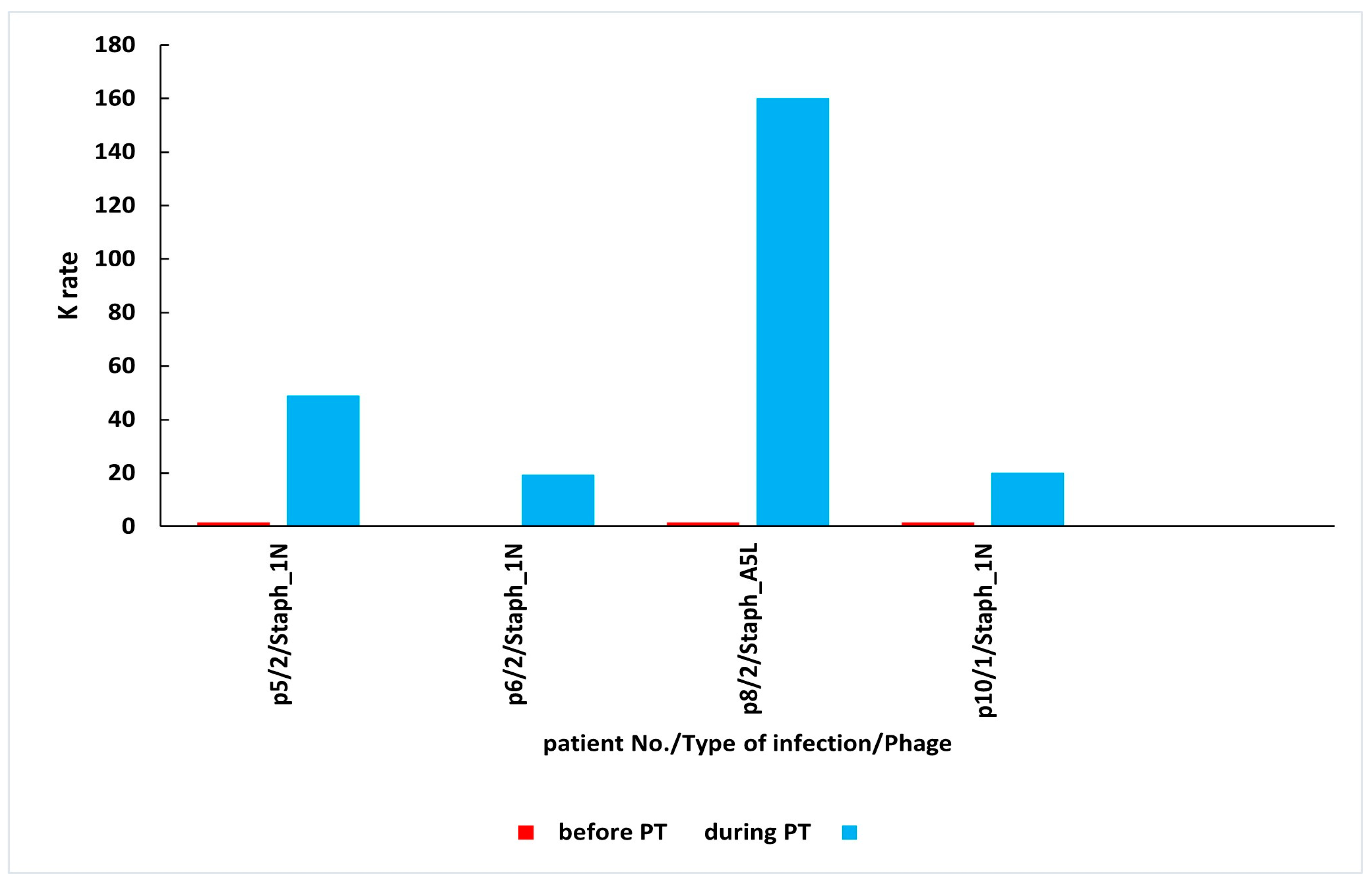
| 5 | bone infection | Staph_1N | 0.05 | 48.86 | n.s. | 21 | E |
| 6 | bone infection | Staph_1N | 0.00 | 19.51 | n.s. | 28 | D |
| 7 | bone infection | Staph_1N | 0.02 | 0.02 | 0.02 | 28 | C |
| 8 | bone infection | Staph_A5L | 0.25 | 160.08 | 303.99 | 35 | D |
| 9 | soft tissue infection | Staph_A5L | 0.05 | 0.25 | n.s. | 56 | D |
| 10 | soft tissue infection | Staph_1N | 0.36 | 20.15 | n.s. | 56 | C |
| 11 | bone infection | Staph_1N | 0.02 | 143.12 (2.5 months after PT) | 22.18 (1 year and 8 months after PT) | 24 | C |
| Mean K ± SD | 0.12 ± 0.11 | 35.79 ± 56.56 |
| Patient No. | Type of Infection | Phages Used in PT | K Before PT | K During PT | K After PT | Days of PT | Clinical Outcome of PT a |
|---|---|---|---|---|---|---|---|
| 1 | soft tissue infection | Staph_1N | 0.06 | 0.32 | n.s | 12 | E |
| 2 | soft tissue infection | Staph_A5L | 0.14 | 0.15 | 0.05 | 14 | E |
| 3 | soft tissue infection | Staph_A5L | 0.47 | 2.59 | n.s. | 14 | B |
| 4 | soft tissue infection | Staph_1N | 0.08 | 0.10 | n.s. | 14 | B |
| 5 | upper respiratory tract infection | Staph_A5L | 0.03 | 0.72 | n.s. | 14 | C |
| 6 | soft tissue infection | Staph_1N | 0.18 | 0.12 | n.s. | 17 | B |
| 7 | upper respiratory tract infection | Staph_1N | 0.02 | 1.42 | n.s. | 17 | E |
| 8 | soft tissue infection | Staph_1N | 0.02 | 0.27 | 0.01 | 18 | A |
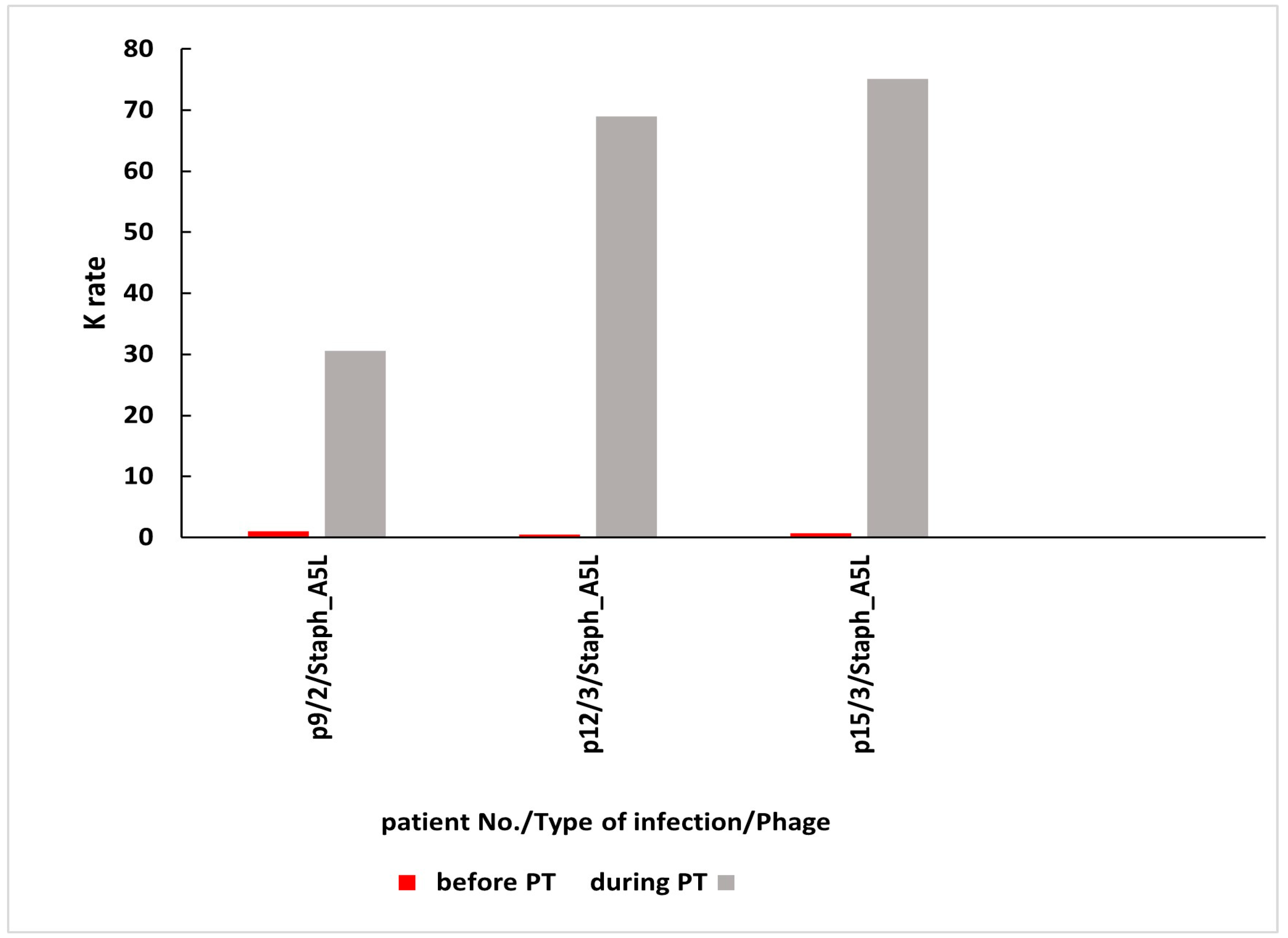
| 9 | bone infection | Staph_A5L | 0.52 | 30.56 | n.s. | 21 | C |
| 10 | bone infection | Staph_A5L | 0.03 | 0.34 | n.s. | 24 | D |
| 11 | soft tissue infection | Staph_A5L | 0.26 | 2.62 | n.s. | 28 | C |
| 12 | upper respiratory tract infection | Staph_A5L | 0.02 | 68.94 | 28.04 | 30 | E |
| 13 | upper respiratory tract infection | Staph_1N | 0.34 | 0.53 | n.s. | 47 | F |
| 14 | soft tissue infection | Staph_1N | 0.46 | 0.58 | n.s. | 55 | F |
| 15 | upper respiratory tract infection | Staph_A5L | 0.11 | 75.12 | n.s. | 56 | E |
| 16 | bone infection | Staph_1N | 0.14 | 2.86 | 71.79 (1 month after PT) | 35 | D |
| Mean K ± SD | 0.18 ± 0.17 | 11.70 ± 23.93 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Łusiak-Szelachowska, M.; Weber-Dąbrowska, B.; Żaczek, M.; Międzybrodzki, R.; Górski, A. The Appearance of Antiphage Antibodies in Sera of Patients Treated with Phages. Antibiotics 2025, 14, 87. https://doi.org/10.3390/antibiotics14010087
Łusiak-Szelachowska M, Weber-Dąbrowska B, Żaczek M, Międzybrodzki R, Górski A. The Appearance of Antiphage Antibodies in Sera of Patients Treated with Phages. Antibiotics. 2025; 14(1):87. https://doi.org/10.3390/antibiotics14010087
Chicago/Turabian StyleŁusiak-Szelachowska, Marzanna, Beata Weber-Dąbrowska, Maciej Żaczek, Ryszard Międzybrodzki, and Andrzej Górski. 2025. "The Appearance of Antiphage Antibodies in Sera of Patients Treated with Phages" Antibiotics 14, no. 1: 87. https://doi.org/10.3390/antibiotics14010087
APA StyleŁusiak-Szelachowska, M., Weber-Dąbrowska, B., Żaczek, M., Międzybrodzki, R., & Górski, A. (2025). The Appearance of Antiphage Antibodies in Sera of Patients Treated with Phages. Antibiotics, 14(1), 87. https://doi.org/10.3390/antibiotics14010087