

Pharmacokinetic, Pharmacokinetic/Pharmacodynamic, and Safety Investigations of Lefamulin in Healthy Chinese Subjects

Abstract
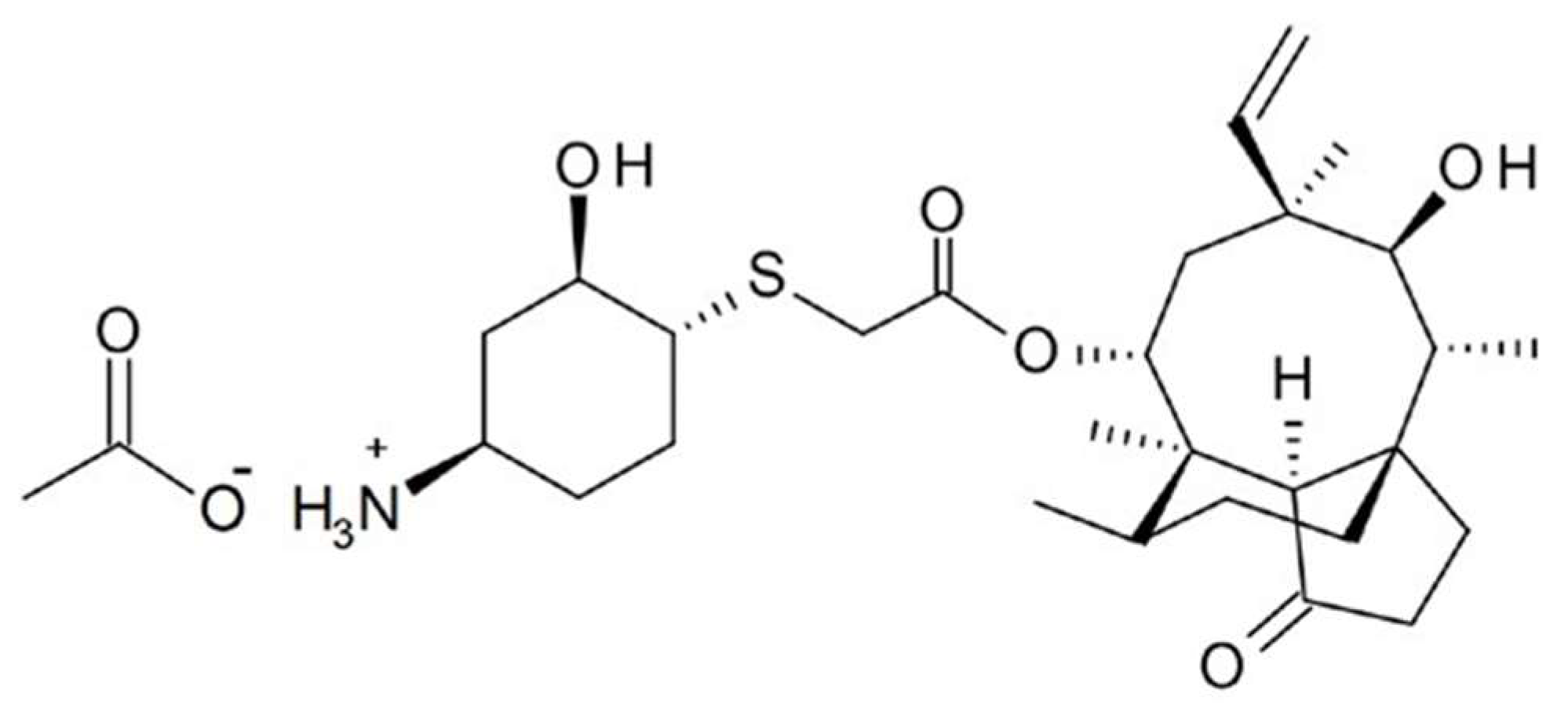
:1. Introduction
2. Results
2.1. Demographic Characteristics
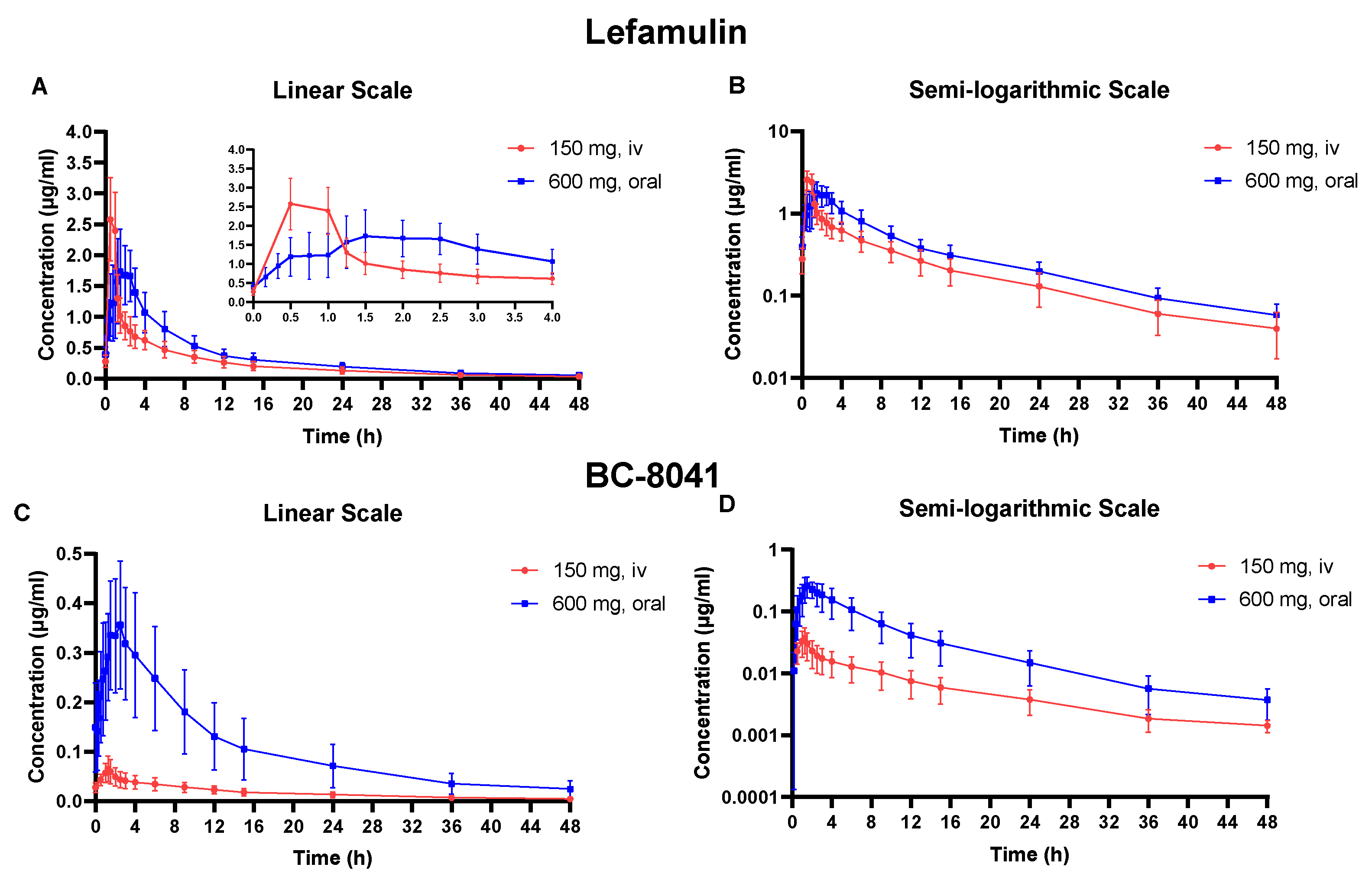
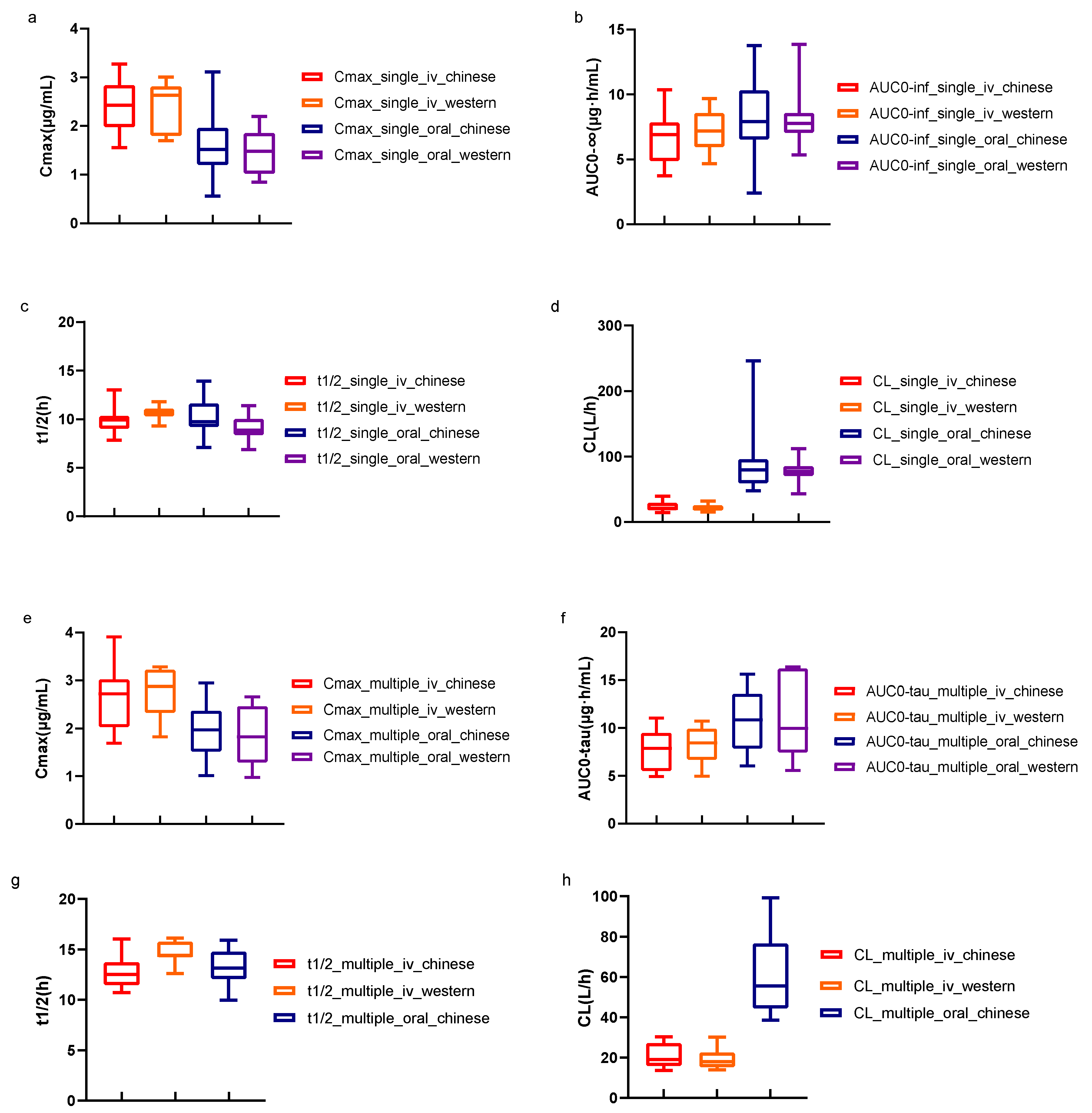
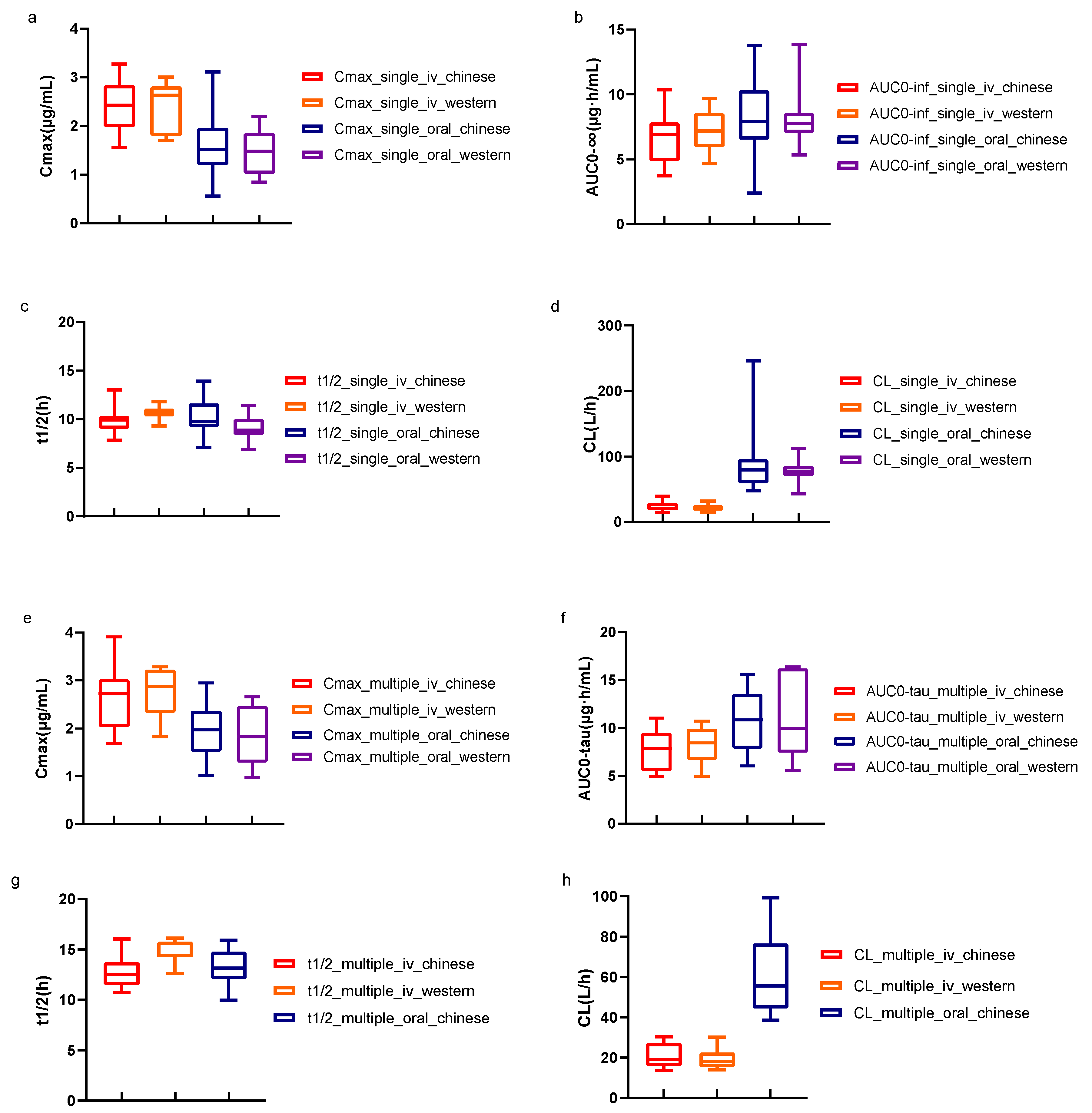
2.2. PK Characteristics
2.3. PK/PD Analysis
2.4. Safety Evaluation
3. Discussion
4. Materials and Methods
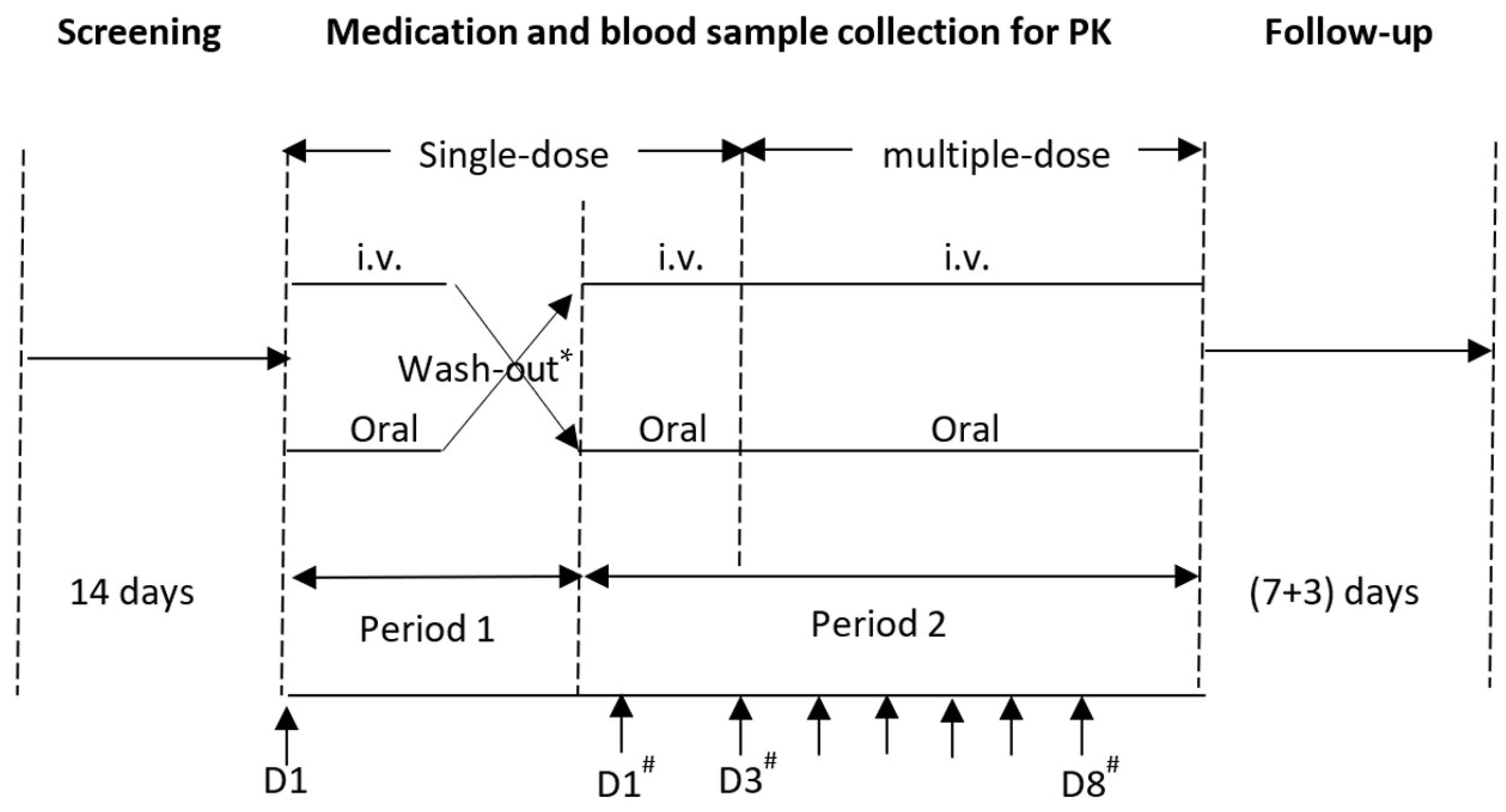
4.1. Study Designs
4.2. Subjects
4.3. Drug and Administration
4.4. Blood Sample Collection, Processing, and Determination
4.5. Determination of Blood Concentration
4.6. PK Analysis
4.7. Susceptibility Study
4.8. PK/PD Target
4.9. PK/PD Analysis
4.10. Safety Evaluation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Novak, R. Are pleuromutilin antibiotics finally fit for human use? Ann. N. Y. Acad. Sci. 2011, 1241, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Zhanel, G.G.; Deng, C.; Zelenitsky, S.; Lawrence, C.K.; Adam, H.J.; Golden, A.; Berry, L.; Schweizer, F.; Zhanel, M.A.; Irfan, N.; et al. Lefamulin: A Novel Oral and Intravenous Pleuromutilin for the Treatment of Community-Acquired Bacterial Pneumonia. Drugs 2021, 81, 233–256. [Google Scholar] [CrossRef]
- Paukner, S.; Gelone, S.P.; Arends, S.J.R.; Flamm, R.K.; Sader, H.S. Antibacterial Activity of Lefamulin against Pathogens Most Commonly Causing Community-Acquired Bacterial Pneumonia: SENTRY Antimicrobial Surveillance Program (2015–2016). Antimicrob. Agents Chemother. 2019, 63, 1128. [Google Scholar] [CrossRef] [PubMed]
- Paukner, S.; Gelone, S.P.; Arends, S.R.; Sader, H.S. Lefamulin Activity Against Respiratory Tract Pathogens Collected in the 2017 Global SENTRY Antimicrobial Surveillance Program. In Proceedings of the ASM Microbe Conference, San Francisco, CA, USA, 20–24 June 2019. [Google Scholar]
- Wu, S.; Zheng, Y.; Guo, Y.; Yin, D.; Zhu, D.; Hu, F. In vitro Activity of Lefamulin Against the Common Respiratory Pathogens Isolated from Mainland China During 2017–2019. Front. Microbiol. 2020, 11, 578824. [Google Scholar] [CrossRef] [PubMed]
- Prince, W.T.; Ivezic-Schoenfeld, Z.; Lell, C.; Tack, K.J.; Novak, R.; Obermayr, F.; Talbot, G.H. Phase II clinical study of BC-3781, a pleuromutilin antibiotic, in treatment of patients with acute bacterial skin and skin structure infections. Antimicrob. Agents Chemother. 2013, 57, 2087–2094. [Google Scholar] [CrossRef] [PubMed]
- Alexander, E.; Goldberg, L.; Das, A.F.; Moran, G.J.; Sandrock, C.; Gasink, L.B.; Spera, P.; Sweeney, C.; Paukner, S.; Wicha, W.W.; et al. Oral Lefamulin vs Moxifloxacin for Early Clinical Response Among Adults with Community-Acquired Bacterial Pneumonia: The LEAP 2 Randomized Clinical Trial. JAMA 2019, 322, 1661–1671. [Google Scholar] [CrossRef] [PubMed]
- File, T.M.; Goldberg, L.; Das, A.; Sweeney, C.; Saviski, J.; Gelone, S.P.; Seltzer, E.; Paukner, S.; Wicha, W.W.; Talbot, G.H.; et al. Efficacy and Safety of Intravenous-to-oral Lefamulin, a Pleuromutilin Antibiotic, for the Treatment of Community-acquired Bacterial Pneumonia: The Phase III Lefamulin Evaluation Against Pneumonia (LEAP 1) Trial. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2019, 69, 1856–1867. [Google Scholar] [CrossRef] [PubMed]
- XENLETA® (lefamulin). EMA Summary of Product Characteristics. Nabriva Therapeutics Ireland DAC: Dublin, Ireland, 2021. Available online: https://www.ema.europa.eu/en/documents/product-information/xenleta-epar-product-information_en.pdf(accessed on 21 August 2023).
- XENLETA® (lefamulin). US Prescribing Information; Nabriva Therapeutics US, Inc.: Fort Washington, PA, USA, 2019. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/211672s000,211673s000lbl.pdf (accessed on 21 August 2023).
- Wicha, W.W.; Strickmann, D.B.; Paukner, S. Pharmacokinetics/pharmacodynamics of lefamulin in a neutropenic murine pneumonia model with Staphylococcus aureus and Streptococcus pneumoniae. J. Antimicrob. Chemother. 2019, 74 (Suppl. 3), iii11–iii18. [Google Scholar] [CrossRef] [PubMed]
- China CHINET. Available online: https://www.chinets.com/Data/AntibioticDrugFast (accessed on 5 July 2023).
- Zhang, L.; Wicha, W.W.; Bhavnani, S.M.; Rubino, C.M. Prediction of lefamulin epithelial lining fluid penetration after intravenous and oral administration using Phase 1 data and population pharmacokinetics methods. J. Antimicrob. Chemother. 2019, 74 (Suppl. 3), iii27–iii34. [Google Scholar] [CrossRef]
- Prince, W.; Wicha, W.; Strickmann, D.; Moschetti, V.; Obermayr, F.; Novak, R. Safety, tolerance and pharmacokinetics of single and repeat doses of BC-3781, a novel antimicrobial. Headache 2010, 11, 1. [Google Scholar]
- Wicha, W.W.; Prince, W.T.; Lell, C.; Heilmayer, W.; Gelone, S.P. Pharmacokinetics and tolerability of lefamulin following intravenous and oral dosing. J. Antimicrob. Chemother. 2019, 74 (Suppl. 3), iii19–iii26. [Google Scholar] [CrossRef] [PubMed]
- Chahine, E.B.; Sucher, A.J. Lefamulin: The First Systemic Pleuromutilin Antibiotic. Ann. Pharmacother. 2020, 54, 1203–1214. [Google Scholar] [CrossRef]
- Wicha, W.W.; Craig, W.A.; Andes, D. In vivo pharmacodynamics of lefamulin, the first systemic pleuromutilin for human use, in a neutropenic murine thigh infection model. J. Antimicrob. Chemother. 2019, 74 (Suppl. 3), iii5–iii10. [Google Scholar] [CrossRef] [PubMed]
- FDA. NDA/BLA Multi-Disciplinary Review and Evaluation; FDA: Silver Spring, MD, USA, 2019.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | 150 mg IV Administration (N = 20) | 600 mg Oral Administration (N = 20) * | Parameters | 150 mg IV Administration Every 12 h, D3–8 (N = 10) | 600 mg Oral Administration Every 12 h, D3–8 (N = 10) * |
|---|---|---|---|---|---|
| Cmax (μg/mL) | 2.41 ± 0.51 | 1.56 ± 0.58 | Cmax,ss (μg/mL) | 2.63 ± 0.67 | 1.94 ± 0.57 |
| tmax (h) | NA | 1.38, 0.35–3.00 | Cmin,ss (μg/mL) | 0.27 ± 0.09 | 0.37 ± 0.11 |
| t1/2 (h) | 9.9 ± 1.2 | 10.15 ± 1.7 | Cavg,ss (μg/mL) | 0.65 ±0.17 | 0.89 ± 0.27 |
| AUC0–t (μg·h/mL) | 6.75 ±1.79 | 7.51 ± 2.76 | tmax,ss (h) | NA | 1.75, 1.25–3.00 |
| AUC0–inf (μg·h/mL) | 6.90 ± 1.84 | 7.71 ± 2.82 | t1/2,ss (h) | 12.7 ± 1.6 | 13.2 ± 1.9 |
| AUC0–12 h (μg·h/mL) | 5.34 ± 1.34 | 5.87 ± 2.08 | AUC0–24 h,ss (μg·h/mL) | 10.03 ± 2.87 | 13.91 ± 4.10 |
| AUC0–24 h (μg·h/mL) | 6.24 ± 1.61 | 6.91 ± 2.51 | AUC0−tau,ss (μg·h/mL) | 7.84 ± 2.07 | 10.64 ± 3.23 |
| Vz (L) | 332.7 ± 100.0 | 1308 ± 542.6 | Vz,ss (L) | 368.6 ± 90.2 | 1177 ± 412.4 |
| CL (L/h) | 23.5 ±7.2 | 92.5 ± 48.0 | CLss (L/h) | 20.5 ± 5.9 | 61.6 ± 20.0 |
| / | / | / | Rac(Cmax) | 1.0 ± 0.1 | 1.3 ± 0.1 |
| / | / | / | Rac(AUC) | 1.4 ± 0.1 | 1.6 ± 0.3 |
| / | / | / | DF (%) | 363.6 ± 32.8 | 178.4 ± 27.9 |
| Parameters | 150 mg IV Administration (N = 20) | 600 mg Oral Administration (N = 20) * | Parameters | 150 mg IV Administration Every 12 h, D3–8 (N = 10) | 600 mg Oral Administration Every 12 h, D3–8 (N = 10) * |
|---|---|---|---|---|---|
| Cmax (μg/mL) | 0.04 ± 0.01 | 0.3 ± 0.10 | Cmax,ss (μg/mL) | 0.07 ± 0.03 | 0.38 ±0.12 |
| tmax (h) | NA | 1.50, 0.75–3.00 | Cmin,ss (μg/mL) | 0.02 ± 0.01 | 0.13 ± 0.07 |
| t1/2 (h) | 11.59 ±2.89 | 9.72 ± 1.43 | Cavg,ss (μg/mL) | 0.04 ± 0.01 | 0.23 ± 0.10 |
| AUC0−t (μg·h/mL) | 0.28 ± 0.13 | 1.84 ± 0.82 | tmax,ss (h) | NA | 2.25, 1.25–2.50 |
| AUC0−inf (μg·h/mL) | 0.30 ± 0.14 | 1.90 ± 0.85 | t1/2,ss (h) | 14.57 ± 2.23 | 14.71 ± 2.34 |
| AUC0–12 h (μg·h/mL) | 0.18 ± 0.08 | 1.37 ±0.56 | AUC0–24 h,ss (μg·h/mL) | 0.63 ± 0.23 | 4.0 ± 1.80 |
| AUC0–24 h (μg·h/mL) | 0.24 ± 0.11 | 1.68 ±0.73 | AUC0−tau,ss (μg·h/mL) | 0.43 ± 0.15 | 2.81 ± 1.15 |
| Vz (L) | NA | NA | Vz,ss (L) | NA | NA |
| CL (L/h) | NA | NA | CLss (L/h) | NA | NA |
| / | / | / | Rac(Cmax) | 1.80 ± 0.42 | 1.14 ± 0.21 |
| / | / | / | Rac(AUC) | 2.64 ± 0.62 | 1.66 ± 0.36 |
| / | / | / | DF (%) | 120.0 ± 21.8 | 116.6 ± 29.5 |
| (a) | |||||||
| S. pneumoniae (MIC90 = 0.125 mg/L) | |||||||
| PK/PD Target | 1.37 (1-log10 cfu Reduction) | ||||||
| Protein Binding Rate | 74.1 | 80 | 85 | 90 | 95 | 97.4 | |
| MIC (mg/L) | 0.015 | 100 | 100 | 100 | 100 | 99 | 97 |
| 0.03 | 100 | 99 | 99 | 99 | 97 | 94 | |
| 0.06 | 99 | 99 | 98 | 97 | 94 | 88 | |
| 0.125 | 98 | 97 | 95 | 93 | 86 | 73 | |
| 0.25 | 95 | 94 | 90 | 86 | 73 | 55 | |
| 0.5 | 89 | 86 | 81 | 72 | 54 | 36 | |
| (b) | |||||||
| S. aureus(MIC90 = 0.06 mg/L) | |||||||
| PK/PD Target | 2.13 (1-log10 cfu Reduction) | ||||||
| Protein Binding Rate | 74.1 | 80 | 85 | 90 | 95 | 97.4 | |
| MIC (mg/L) | 0.015 | 100 | 100 | 100 | 99 | 98 | 95 |
| 0.03 | 99 | 99 | 99 | 97 | 95 | 90 | |
| 0.06 | 98 | 98 | 97 | 95 | 89 | 80 | |
| 0.125 | 96 | 94 | 93 | 89 | 78 | 63 | |
| 0.25 | 91 | 89 | 85 | 77 | 60 | 43 | |
| 0.5 | 83 | 78 | 71 | 60 | 41 | 25 | |
| Protein Binding Rate | Target | S. pneumoniae (MIC90 = 0.125 mg/L) | Target | S. aureus (MIC90 = 0.06 mg/L) |
|---|---|---|---|---|
| 74.1 | 1.37 | 98 | 2.13 | 99 |
| 80 | 97 | 98 | ||
| 85 | 97 | 98 | ||
| 90 | 94 | 96 | ||
| 95 | 91 | 92 | ||
| 97.4 | 88 | 86 |
| 150 mg IV Administration (N = 20), n (%) | 600 mg PO Administration (N = 20), n (%) | |
|---|---|---|
| Treatment-related TEAEs | 11 (55.0) | 12 (60.0) |
| Gastrointestinal disorders | 7 (35.0) | 13 (65.0) |
| Nausea | 2 (10.0) | 5 (25.0) |
| Abdominal discomfort | 1 (5.0) | 4 (20.0) |
| Abdominal pain upper | 1 (5.0) | 3 (15.0) |
| Abdominal pain | 0 | 3 (15.0) |
| Diarrhoea | 0 | 3 (15.0) |
| General disorders and administration site conditions | 10 (50.0) | 0 |
| Infusion site pain | 9 (45.0) | 0 |
| Infusion site pruritus | 8 (40.0) | 0 |
| Infusion site erythema | 5 (25.0) | 0 |
| Infusion site swelling | 5 (25.0) | 0 |
| Infusion site induration | 4 (20.0) | 0 |
| Infusion site haemorrhage | 1 (5.0) | 0 |
| Investigations | 7 (35.0) | 4 (20.0) |
| Blood creatinine increased | 2 (10.0) | 0 |
| Eosinophil percentage increased | 1 (5.0) | 1 (5.0) |
| Blood creatine phosphokinase increased | 0 | 1 (5.0) |
| Eosinophil count increased | 1 (5.0) | 0 |
| Nervous system disorders | 3 | 4 (20.0) |
| Headache | 1 | 3 (15.0) |
| Dizziness | 0 | 1 (5.0) |
| Ear and labyrinth disorders | 0 | 1 (5.0) |
| Ear pain | 0 | 1 (5.0) |
| Respiratory, thoracic and mediastinal disorders | 0 | 1 (5.0) |
| Oropharyngeal pain | 0 | 1 (5.0) |
| Cohort | Period 1 Single-Dose, D1 | Wash-Out Period (Days) | Period 2 | |
|---|---|---|---|---|
| Single-Dose, D1 | Multiple-Dose, D3−8 (Administration Only in the Morning on D8) | |||
| 1 | 150 mg IV administration | 7 | 600 mg oral administration | 600 mg oral administration, every 12 h |
| 2 | 600 mg oral administration | 7 | 150 mg IV administration | 150 mg IV administration, every 12 h |
| Bacteria (No. of Isolates) | Frequency Distribution (%) of MIC (mg/L) | MIC50/MIC90 | ||||
|---|---|---|---|---|---|---|
| 0.015 | 0.03 | 0.06 | 0.125 | 0.25 | ||
| Streptococcus pneumoniae (172) | 2.91 | 6.98 | 21.51 | 59.3 | 9.3 | 0.125/0.125 |
| Cumulative frequency distribution of Streptococcus pneumoniae | 2.91 | 9.88 | 31.40 | 90.70 | 100.00 | \ |
| Staphylococcus aureus (121) | 38.84 | 2.48 | 50.41 | 7.44 | 0.83 | 0.06/0.06 |
| Cumulative frequency distribution of Staphylococcus aureus | 38.84 | 41.32 | 91.74 | 99.17 | 100.00 | \ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, Y.; Wei, Q.; Bian, X.; Yang, X.; Yu, J.; Wang, J.; Yang, H.; Cao, G.; Wu, X.; Zhang, J. Pharmacokinetic, Pharmacokinetic/Pharmacodynamic, and Safety Investigations of Lefamulin in Healthy Chinese Subjects. Antibiotics 2023, 12, 1391. https://doi.org/10.3390/antibiotics12091391
Hu Y, Wei Q, Bian X, Yang X, Yu J, Wang J, Yang H, Cao G, Wu X, Zhang J. Pharmacokinetic, Pharmacokinetic/Pharmacodynamic, and Safety Investigations of Lefamulin in Healthy Chinese Subjects. Antibiotics. 2023; 12(9):1391. https://doi.org/10.3390/antibiotics12091391
Chicago/Turabian StyleHu, Yingying, Qiong Wei, Xingchen Bian, Xinyi Yang, Jicheng Yu, Jingjing Wang, Haijing Yang, Guoying Cao, Xiaojie Wu, and Jing Zhang. 2023. "Pharmacokinetic, Pharmacokinetic/Pharmacodynamic, and Safety Investigations of Lefamulin in Healthy Chinese Subjects" Antibiotics 12, no. 9: 1391. https://doi.org/10.3390/antibiotics12091391
APA StyleHu, Y., Wei, Q., Bian, X., Yang, X., Yu, J., Wang, J., Yang, H., Cao, G., Wu, X., & Zhang, J. (2023). Pharmacokinetic, Pharmacokinetic/Pharmacodynamic, and Safety Investigations of Lefamulin in Healthy Chinese Subjects. Antibiotics, 12(9), 1391. https://doi.org/10.3390/antibiotics12091391