
Which Are the Best Regimens of Broad-Spectrum Beta-Lactam Antibiotics in Burn Patients? A Systematic Review of Evidence from Pharmacology Studies


 and
and
Abstract
:1. Introduction
2. Results
2.1. Ceftazidime
Synthesis of the Findings concerning Drug Regimens for Ceftazidime
2.2. Cefepime
Synthesis of the Findings concerning Drug Regimens for Cefepime
2.3. Piperacillin-Tazobactam
Synthesis of the Findings concerning Drug Regimens for Piperacillin-Tazobactam
2.4. Meropenem
Synthesis of the Findings concerning Drug Regimens for Meropenem
2.5. Imipenem-Cilastatin
Synthesis of the Findings concerning Drug Regimens for Imipenem-Cilastatin
2.6. Aztreonam
Synthesis of the Findings concerning Drug Regimens for Aztreonam
2.7. New Beta-Lactam-Beta-Lactamase Inhibitor Combinations, Ceftaroline, Ceftobiprole and Cefiderocol
Synthesis of the Findings concerning Drug Regimens for New Beta-Lactam-Beta-Lactamase Inhibitor Combinations, Ceftaroline, Ceftobiprole and Cefiderocol
3. Discussion
4. Materials and Methods
5. Conclusions
6. Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Search Strings

{kind=link}
| Search Strings | Number of Hits | Paper after TIAB and Full-Text Analysis * |
|---|---|---|
| (“burn” [tiab] or “burns” [tiab] or “burned” [tiab]) and “piperacillin” [tiab] | 127 | 10 |
| (“burn” [tiab] or “burns” [tiab] or “burned” [tiab]) and “ceftazidime” [tiab] | 168 | 7 |
| (“burn” [tiab] or “burns” [tiab] or “burned” [tiab]) and “cefepime" [tiab] | 51 | 5 |
| (“burn” [tiab] or “burns” [tiab] or “burned” [tiab]) and “meropenem” [tiab] | 131 | 11 |
| (“burn” [tiab] or “burns” [tiab] or “burned” [tiab]) and “imipenem” [tiab] | 270 | 8 |
| (“burn” [tiab] or “burns” [tiab] or “burned” [tiab]) and “aztreonam” [tiab] | 48 | 2 |
| (“burn” [tiab] or “burns” [tiab] or “burned” [tiab]) and “avibactam” [tiab] | 5 | 1 |
| (“burn” [tiab] or “burns” [tiab] or “burned” [tiab]) and “vaborbactam” [tiab] | 2 | 0 |
| (“burn” [tiab] or “burns” [tiab] or “burned” [tiab]) and “ceftolozane” [tiab] | 2 | 0 |
| (“burn” [tiab] or “burns” [tiab] or “burned” [tiab]) and “relebactam” [tiab] | 1 | 0 |
| (“burn” [tiab] or “burns” [tiab] or “burned” [tiab]) and “ceftaroline” [tiab] | 3 | 0 |
| (“burn” [tiab] or “burns” [tiab] or “burned” [tiab]) and “ceftobiprole” [tiab] | 2 | 0 |
| (“burn” [tiab] or “burns” [tiab] or “burned” [tiab]) and “cefiderocol” [tiab] | 3 | 0 |
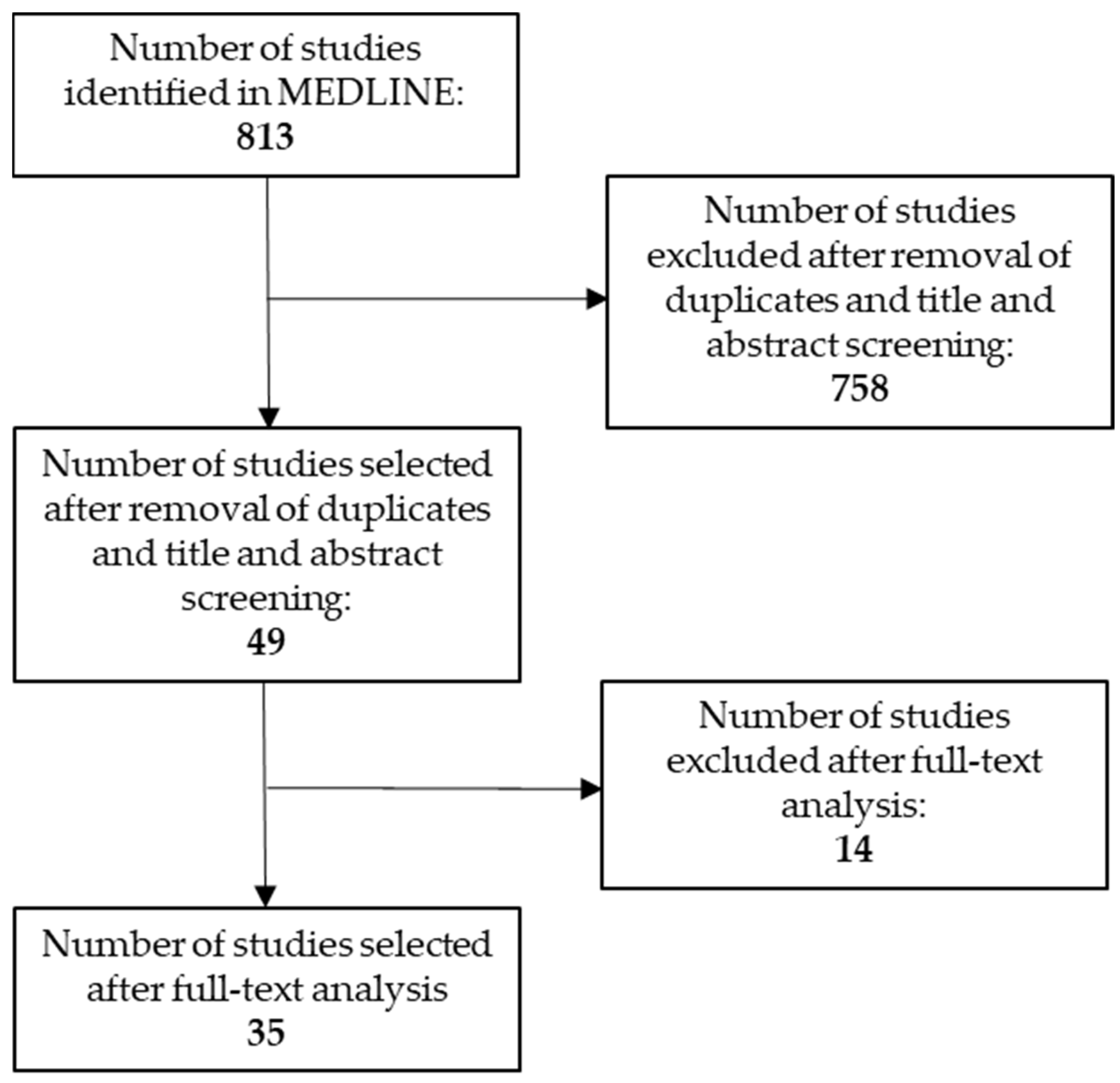
| Total * | 813 | 44 |
References
- Blanchet, B.; Jullien, V.; Vinsonneau, C.; Tod, M. Influence of Burns on Pharmacokinetics and Pharmacodynamics of Drugs Used in the Care of Burn Patients. Clin. Pharmacokinet. 2008, 47, 635–654. [Google Scholar] [CrossRef]
- Cota, J.M.; FakhriRavari, A.; Rowan, M.P.; Chung, K.K.; Murray, C.K.; Akers, K.S. Intravenous Antibiotic and Antifungal Agent Pharmacokinetic-Pharmacodynamic Dosing in Adults with Severe Burn Injury. Clin. Ther. 2016, 38, 2016–2031. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.A.; Abdul-Aziz, M.H.; Lipman, J.; Mouton, J.W.; Vinks, A.A.; Felton, T.W.; Hope, W.W.; Farkas, A.; Neely, M.N.; Schentag, J.J.; et al. Individualised Antibiotic Dosing for Patients Who Are Critically Ill: Challenges and Potential Solutions. Lancet Infect. Dis. 2014, 14, 498–509. [Google Scholar] [CrossRef] [PubMed]
- Jeschke, M.G. Postburn Hypermetabolism: Past, Present, and Future. J. Burn. Care Res. 2016, 37, 86–96. [Google Scholar] [CrossRef]
- Steele, A.N.; Grimsrud, K.N.; Sen, S.; Palmieri, T.L.; Greenhalgh, D.G.; Tran, N.K. Gap Analysis of Pharmacokinetics and Pharmacodynamics in Burn Patients: A Review. J. Burn. Care Res. 2015, 36, e194–e211. [Google Scholar] [CrossRef] [PubMed]
- American Burn Association. 2016 National Burn Repository Report of Data from 2006–2015; American Burn Association: Chicago, IL, USA, 2016. [Google Scholar]
- Krishnan, P.; Frew, Q.; Green, A.; Martin, R.; Dziewulski, P. Cause of Death and Correlation with Autopsy Findings in Burns Patients. Burns 2013, 39, 583–588. [Google Scholar] [CrossRef] [PubMed]
- Fitzwater, J.; Purdue, G.F.; Hunt, J.L.; O’Keefe, G.E. The Risk Factors and Time Course of Sepsis and Organ Dysfunction after Burn Trauma. J. Trauma 2003, 54, 959–966. [Google Scholar] [CrossRef] [PubMed]
- Keen, E.F.; Robinson, B.J.; Hospenthal, D.R.; Aldous, W.K.; Wolf, S.E.; Chung, K.K.; Murray, C.K. Prevalence of Multidrug-Resistant Organisms Recovered at a Military Burn Center. Burns 2010, 36, 819–825. [Google Scholar] [CrossRef]
- van Duin, D.; Strassle, P.D.; DiBiase, L.M.; Lachiewicz, A.M.; Rutala, W.A.; Eitas, T.; Maile, R.; Kanamori, H.; Weber, D.J.; Cairns, B.A.; et al. Timeline of Health Care-Associated Infections and Pathogens after Burn Injuries. Am. J. Infect. Control 2016, 44, 1511–1516. [Google Scholar] [CrossRef]
- Bonapace, C.R.; White, R.L.; Friedrich, L.V.; Norcross, E.D.; Bosso, J.A. Pharmacokinetics of Cefepime in Patients with Thermal Burn Injury. Antimicrob. Agents Chemother. 1999, 43, 2848–2854. [Google Scholar] [CrossRef]
- Boucher, B.A.; Hudson, J.Q.; Hill, D.M.; Swanson, J.M.; Wood, G.C.; Laizure, S.C.; Arnold-Ross, A.; Hu, Z.-Y.; Hickerson, W.L. Pharmacokinetics of Imipenem/Cilastatin Burn Intensive Care Unit Patients Undergoing High-Dose Continuous Venovenous Hemofiltration. Pharmacotherapy 2016, 36, 1229–1237. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, L.V.; White, R.L.; Kays, M.B.; Brundage, D.M.; Yarbrough, D. Aztreonam Pharmacokinetics in Burn Patients. Antimicrob. Agents Chemother. 1991, 35, 57–61. [Google Scholar] [CrossRef]
- Fournier, A.; Eggimann, P.; Pantet, O.; Pagani, J.L.; Dupuis-Lozeron, E.; Pannatier, A.; Sadeghipour, F.; Voirol, P.; Que, Y.-A. Impact of Real-Time Therapeutic Drug Monitoring on the Prescription of Antibiotics in Burn Patients Requiring Admission to the Intensive Care Unit. Antimicrob. Agents Chemother. 2018, 62, e01818-17. [Google Scholar] [CrossRef] [PubMed]
- Machado, A.S.; Oliveira, M.S.; Sanches, C.; da Silva Junior, C.V.; Gomez, D.S.; Gemperli, R.; Santos, S.R.C.J.; Levin, A.S. Clinical Outcome and Antimicrobial Therapeutic Drug Monitoring for the Treatment of Infections in Acute Burn Patients. Clin. Ther. 2017, 39, 1649–1657.e3. [Google Scholar] [CrossRef] [PubMed]
- Corcione, S.; D’Avolio, A.; Loia, R.C.; Pensa, A.; Segala, F.V.; De Nicolò, A.; Fatiguso, G.; Romeo, M.; Di Perri, G.; Stella, M.; et al. Pharmacokinetics of Meropenem in Burn Patients with Infections Caused by Gram-Negative Bacteria: Are We Getting Close to the Right Treatment? J. Glob. Antimicrob. Resist. 2020, 20, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Xie, F. Population Pharmacokinetics and Simulations of Imipenem in Critically Ill Patients Undergoing Continuous Renal Replacement Therapy. Int. J. Antimicrob. Agents 2019, 53, 98–105. [Google Scholar] [CrossRef]
- Wong, G.; Brinkman, A.; Benefield, R.J.; Carlier, M.; De Waele, J.J.; El Helali, N.; Frey, O.; Harbarth, S.; Huttner, A.; McWhinney, B.; et al. An International, Multicentre Survey of β-Lactam Antibiotic Therapeutic Drug Monitoring Practice in Intensive Care Units. J. Antimicrob. Chemother. 2014, 69, 1416–1423. [Google Scholar] [CrossRef]
- Tabah, A.; De Waele, J.; Lipman, J.; Zahar, J.R.; Cotta, M.O.; Barton, G.; Timsit, J.-F.; Roberts, J.A.; Working Group for Antimicrobial Use in the ICU within the Infection Section of the European Society of Intensive Care Medicine (ESICM). The ADMIN-ICU Survey: A Survey on Antimicrobial Dosing and Monitoring in ICUs. J. Antimicrob. Chemother. 2015, 70, 2671–2677. [Google Scholar] [CrossRef] [PubMed]
- Hong, L.T.; Downes, K.J.; FakhriRavari, A.; Abdul-Mutakabbir, J.C.; Kuti, J.L.; Jorgensen, S.; Young, D.C.; Alshaer, M.H.; Bassetti, M.; Bonomo, R.A.; et al. International Consensus Recommendations for the Use of Prolonged-Infusion Beta-Lactam Antibiotics: Endorsed by the American College of Clinical Pharmacy, British Society for Antimicrobial Chemotherapy, Cystic Fibrosis Foundation, European Society of Clinical Microbiology and Infectious Diseases, Infectious Diseases Society of America, Society of Critical Care Medicine, and Society of Infectious Diseases Pharmacists. Pharmacotherapy 2023, 43, 740–777. [Google Scholar] [CrossRef]
- Abdul-Aziz, M.H.; Alffenaar, J.-W.C.; Bassetti, M.; Bracht, H.; Dimopoulos, G.; Marriott, D.; Neely, M.N.; Paiva, J.-A.; Pea, F.; Sjovall, F.; et al. Antimicrobial Therapeutic Drug Monitoring in Critically Ill Adult Patients: A Position Paper. Intensive Care Med. 2020, 46, 1127–1153. [Google Scholar] [CrossRef] [PubMed]
- Alshaer, M.; Mazirka, P.; Burch, G.; Peloquin, C.; Drabick, Z.; Carson, J. Experience with Implementing a Beta-Lactam Therapeutic Drug Monitoring Service in a Burn Intensive Care Unit: A Retrospective Chart Review. J. Burn. Care Res. 2022, 44, 121–128. [Google Scholar] [CrossRef]
- Aoki, Y.; Urakami, T.; Magarifuchi, H.; Nagasawa, Z.; Nagata, M.; Fukuoka, M. The Importance of Pharmacokinetic Consultation of Cefepime Treatment for Pseudomonas Aeruginosa Bacteremia: A Case Report of Severe Thermal Burn Injury. J. Infect. Chemother. 2011, 17, 407–411. [Google Scholar] [CrossRef]
- Boucher, B.A.; Hickerson, W.L.; Kuhl, D.A.; Bombassaro, A.M.; Jaresko, G.S. Imipenem Pharmacokinetics in Patients with Burns. Clin. Pharmacol. Ther. 1990, 48, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Bourget, P.; Lesne-Hulin, A.; Le Reveillé, R.; Le Bever, H.; Carsin, H. Clinical Pharmacokinetics of Piperacillin-Tazobactam Combination in Patients with Major Burns and Signs of Infection. Antimicrob. Agents Chemother. 1996, 40, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Conil, J.M.; Georges, B.; Lavit, M.; Seguin, T.; Tack, I.; Samii, K.; Chabanon, G.; Houin, G.; Saivin, S. Pharmacokinetics of Ceftazidime and Cefepime in Burn Patients: The Importance of Age and Creatinine Clearance. Int. J. Clin. Pharmacol. Ther. 2007, 45, 529–538. [Google Scholar] [CrossRef] [PubMed]
- Conil, J.M.; Georges, B.; Lavit, M.; Laguerre, J.; Samii, K.; Houin, G.; Saivin, S. A Population Pharmacokinetic Approach to Ceftazidime Use in Burn Patients: Influence of Glomerular Filtration, Gender and Mechanical Ventilation. Br. J. Clin. Pharmacol. 2007, 64, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Conil, J.M.; Georges, B.; Fourcade, O.; Seguin, T.; Houin, G.; Saivin, S. Intermittent Administration of Ceftazidime to Burns Patients: Influence of Glomerular Filtration. Int. J. Clin. Pharmacol. Ther. 2007, 45, 133–142. [Google Scholar] [CrossRef]
- Conil, J.-M.; Georges, B.; Ravat, F.; Ruiz, S.; Seguin, T.; Metsu, D.; Fourcade, O.; Saivin, S. Ceftazidime Dosage Recommendations in Burn Patients: From a Population Pharmacokinetic Approach to Clinical Practice via Monte Carlo Simulations. Clin. Ther. 2013, 35, 1603–1612. [Google Scholar] [CrossRef]
- Cotta, M.O.; Gowen, B.; Truloff, N.; Bursle, E.; McWhinney, B.; Ungerer, J.P.J.; Roberts, J.A.; Lipman, J. Even High-Dose Extended Infusions May Not Yield Desired Concentrations of β-Lactams: The Value of Therapeutic Drug Monitoring. Infect. Dis. 2015, 47, 739–742. [Google Scholar] [CrossRef]
- Dailly, E.; Kergueris, M.F.; Pannier, M.; Jolliet, P.; Bourin, M. Population Pharmacokinetics of Imipenem in Burn Patients. Fundam. Clin. Pharmacol. 2003, 17, 645–650. [Google Scholar] [CrossRef]
- Dailly, E.; Pannier, M.; Jolliet, P.; Bourin, M. Population Pharmacokinetics of Ceftazidime in Burn Patients. Br. J. Clin. Pharmacol. 2003, 56, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Doh, K.; Woo, H.; Hur, J.; Yim, H.; Kim, J.; Chae, H.; Han, S.; Yim, D.-S. Population Pharmacokinetics of Meropenem in Burn Patients. J. Antimicrob. Chemother. 2010, 65, 2428–2435. [Google Scholar] [CrossRef] [PubMed]
- Falcone, M.; Menichetti, F.; Cattaneo, D.; Tiseo, G.; Baldelli, S.; Galfo, V.; Leonildi, A.; Tagliaferri, E.; Di Paolo, A.; Pai, M.P. Pragmatic Options for Dose Optimization of Ceftazidime/Avibactam with Aztreonam in Complex Patients. J. Antimicrob. Chemother. 2021, 76, 1025–1031. [Google Scholar] [CrossRef] [PubMed]
- Gomez, D.S.; Sanches-Giraud, C.; Silva, C.V.; Oliveira, A.M.R.R.; da Silva, J.M.; Gemperli, R.; Santos, S.R.C.J. Imipenem in Burn Patients: Pharmacokinetic Profile and PK/PD Target Attainment. J. Antibiot. 2015, 68, 143–147. [Google Scholar] [CrossRef] [PubMed]
- Hallam, M.-J.; Allen, J.M.; James, S.E.; Donaldson, P.M.W.; Davies, J.G.; Hanlon, G.W.; Dheansa, B.S. Potential Subtherapeutic Linezolid and Meropenem Antibiotic Concentrations in a Patient with Severe Burns and Sepsis. J. Burn. Care Res. 2010, 31, 207–209. [Google Scholar] [CrossRef]
- Jeon, S.; Han, S.; Lee, J.; Hong, T.; Paek, J.; Woo, H.; Yim, D.-S. Population Pharmacokinetic Analysis of Piperacillin in Burn Patients. Antimicrob. Agents Chemother. 2014, 58, 3744–3751. [Google Scholar] [CrossRef]
- Le Floch, R.; Arnould, J.-F.; Pilorget, A.; Dally, E.; Naux, E. Concentrations sanguines d’antibiotiques chez les patients brûlés. Étude rétrospective sur cinq ans [Antimicrobial blood concentrations in burns. A five years’ retrospective survey]. Pathol. Biol. 2010, 58, 137–143. [Google Scholar] [CrossRef]
- Messiano, C.G.; Morales Junior, R.; Pereira, G.O.; da Silva Junior, E.M.; de Souza Gomez, D.; Santos, S.R.C.J. Therapeutic Target Attainment of 3-Hour Extended Infusion of Meropenem in Patients with Septic Burns. Clin. Ther. 2022, 44, 624–629. [Google Scholar] [CrossRef]
- Olbrisch, K.; Kisch, T.; Thern, J.; Kramme, E.; Rupp, J.; Graf, T.; Wicha, S.G.; Mailänder, P.; Raasch, W. After Standard Dosage of Piperacillin Plasma Concentrations of Drug Are Subtherapeutic in Burn Patients. Naunyn Schmiedebergs Arch. Pharmacol. 2019, 392, 229–241. [Google Scholar] [CrossRef]
- Patel, B.M.; Paratz, J.; See, N.C.; Muller, M.J.; Rudd, M.; Paterson, D.; Briscoe, S.E.; Ungerer, J.; McWhinney, B.C.; Lipman, J.; et al. Therapeutic Drug Monitoring of Beta-Lactam Antibiotics in Burns Patients—A One-Year Prospective Study. Ther. Drug Monit. 2012, 34, 160–164. [Google Scholar] [CrossRef]
- Por, E.D.; Akers, K.S.; Chung, K.K.; Livezey, J.R.; Selig, D.J. Population Pharmacokinetic Modeling and Simulations of Imipenem in Burn Patients with and without Continuous Venovenous Hemofiltration in the Military Health System. J. Clin. Pharmacol. 2021, 61, 1182–1194. [Google Scholar] [CrossRef] [PubMed]
- Ramon-Lopez, A.; Allen, J.M.; Thomson, A.H.; Dheansa, B.S.; James, S.E.; Hanlon, G.W.; Stewart, B.; Davies, J.G. Dosing Regimen of Meropenem for Adults with Severe Burns: A Population Pharmacokinetic Study with Monte Carlo Simulations. J. Antimicrob. Chemother. 2015, 70, 882–890. [Google Scholar] [CrossRef] [PubMed]
- Sampol, E.; Jacquet, A.; Viggiano, M.; Bernini, V.; Manelli, J.C.; Lacarelle, B.; Durand, A. Plasma, Urine and Skin Pharmacokinetics of Cefepime in Burns Patients. J. Antimicrob. Chemother. 2000, 46, 315–317. [Google Scholar] [CrossRef] [PubMed]
- Selig, D.J.; Akers, K.S.; Chung, K.K.; Kress, A.T.; Livezey, J.R.; Por, E.D.; Pruskowski, K.A.; DeLuca, J.P. Comparison of Piperacillin and Tazobactam Pharmacokinetics in Critically Ill Patients with Trauma or with Burn. Antibiotics 2022, 11, 618. [Google Scholar] [CrossRef] [PubMed]
- Selig, D.J.; Akers, K.S.; Chung, K.K.; Pruskowski, K.A.; Livezey, J.R.; Por, E.D. Meropenem Pharmacokinetics in Critically Ill Patients with or without Burn Treated with or without Continuous Veno-Venous Haemofiltration. Br. J. Clin. Pharmacol. 2022, 88, 2156–2168. [Google Scholar] [CrossRef]
- Shikuma, L.R.; Ackerman, B.H.; Weaver, R.H.; Solem, L.D.; Strate, R.G.; Cerra, F.B.; Zaske, D.E. Thermal Injury Effects on Drug Disposition: A Prospective Study with Piperacillin. J. Clin. Pharmacol. 1990, 30, 632–637. [Google Scholar] [CrossRef]
- Torian, S.C.; Wiktor, A.J.; Roper, S.E.; Laramie, K.E.; Miller, M.A.; Mueller, S.W. Burn Injury and Augmented Renal Clearance: A Case for Optimized Piperacillin-Tazobactam Dosing. J. Burn. Care Res. 2023, 44, 203–206. [Google Scholar] [CrossRef]
- Walstad, R.A.; Aanderud, L.; Thurmann-Nielsen, E. Pharmacokinetics and Tissue Concentrations of Ceftazidime in Burn Patients. Eur. J. Clin. Pharmacol. 1988, 35, 543–549. [Google Scholar] [CrossRef]
- Longuet, P.; Lecapitaine, A.L.; Cassard, B.; Bastita, R.; Gauzit, R.; Lesprit, P.; Haddad, R.; Vanjak, D.; Diamantis, S. Preparing and Administering Injectable Antibiotics: How to Avoid Playing God. Méd. Mal. Infect. 2016, 46, 242–268. [Google Scholar] [CrossRef]
- Boucher, B.A.; Kuhl, D.A.; Hickerson, W.L. Pharmacokinetics of Systemically Administered Antibiotics in Patients with Thermal Injury. Clin. Infect. Dis. 1992, 14, 458–463. [Google Scholar] [CrossRef]
- Veiga, R.P.; Paiva, J.-A. Pharmacokinetics-Pharmacodynamics Issues Relevant for the Clinical Use of Beta-Lactam Antibiotics in Critically Ill Patients. Crit. Care 2018, 22, 233. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves-Pereira, J.; Póvoa, P. Antibiotics in Critically Ill Patients: A Systematic Review of the Pharmacokinetics of β-Lactams. Crit. Care 2011, 15, R206. [Google Scholar] [CrossRef] [PubMed]
- Barajas-Nava, L.A.; López-Alcalde, J.; Roqué i Figuls, M.; Solà, I.; Bonfill Cosp, X. Antibiotic Prophylaxis for Preventing Burn Wound Infection. Cochrane Database Syst. Rev. 2013, 6, CD008738. [Google Scholar] [CrossRef] [PubMed]
- Gatti, M.; Cojutti, P.G.; Pascale, R.; Tonetti, T.; Laici, C.; Dell’Olio, A.; Siniscalchi, A.; Giannella, M.; Viale, P.; Pea, F. Assessment of a PK/PD Target of Continuous Infusion Beta-Lactams Useful for Preventing Microbiological Failure and/or Resistance Development in Critically Ill Patients Affected by Documented Gram-Negative Infections. Antibiotics 2021, 10, 1311. [Google Scholar] [CrossRef]
- EUCAST: MIC and Zone Distributions and ECOFFs. Available online: https://www.eucast.org/mic_and_zone_distributions_and_ecoffs (accessed on 25 September 2023).
- Roberts, J.A.; Paul, S.K.; Akova, M.; Bassetti, M.; Waele, J.J.D.; Dimopoulos, G.; Kaukonen, K.-M.; Koulenti, D.; Martin, C.; Montravers, P.; et al. DALI: Defining Antibiotic Levels in Intensive Care Unit Patients: Are Current β-Lactam Antibiotic Doses Sufficient for Critically Ill Patients? Clin. Infect. Dis. 2014, 58, 1072–1083. [Google Scholar] [CrossRef] [PubMed]
- Gatti, M.; Pea, F. Jumping into the Future: Overcoming Pharmacokinetic/Pharmacodynamic Hurdles to Optimize the Treatment of Severe Difficult to Treat-Gram-Negative Infections with Novel Beta-Lactams. Expert. Rev. Anti Infect. Ther. 2023, 21, 149–166. [Google Scholar] [CrossRef]
- Hoff, B.M.; Maker, J.H.; Dager, W.E.; Heintz, B.H. Antibiotic Dosing for Critically Ill Adult Patients Receiving Intermittent Hemodialysis, Prolonged Intermittent Renal Replacement Therapy, and Continuous Renal Replacement Therapy: An Update. Ann. Pharmacother. 2020, 54, 43–55. [Google Scholar] [CrossRef]
- Gatti, M.; Pea, F. Pharmacokinetic/Pharmacodynamic Target Attainment in Critically Ill Renal Patients on Antimicrobial Usage: Focus on Novel Beta-Lactams and Beta Lactams/Beta-Lactamase Inhibitors. Expert. Rev. Clin. Pharmacol. 2021, 14, 583–599. [Google Scholar] [CrossRef]
- Gatti, M.; Pea, F. Antimicrobial Dose Reduction in Continuous Renal Replacement Therapy: Myth or Real Need? A Practical Approach for Guiding Dose Optimization of Novel Antibiotics. Clin. Pharmacokinet. 2021, 60, 1271–1289. [Google Scholar] [CrossRef]
- Selig, D.J.; DeLuca, J.P.; Chung, K.K.; Pruskowski, K.A.; Livezey, J.R.; Nadeau, R.J.; Por, E.D.; Akers, K.S. Pharmacokinetics of Piperacillin and Tazobactam in Critically Ill Patients Treated with Continuous Kidney Replacement Therapy: A Mini-Review and Population Pharmacokinetic Analysis. J. Clin. Pharm. Ther. 2022, 47, 1091–1102. [Google Scholar] [CrossRef]
- Meng, L.; Mui, E.; Holubar, M.K.; Deresinski, S.C. Comprehensive Guidance for Antibiotic Dosing in Obese Adults. Pharmacotherapy 2017, 37, 1415–1431. [Google Scholar] [CrossRef] [PubMed]
- The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. Available online: http://www.prisma-statement.org/ (accessed on 25 September 2023).
- EUCAST Breakpoint Tables. Version 13.1. Available online: https://www.eucast.org/clinical_breakpoints (accessed on 25 September 2023).

| First Author | Target Antibiotic(s) | Country of the First Author | Year of Publication | Study Design | Number of Patients | Control Group | Mean % of Burned TBSA | Mean CLCR (mL/m) | Mean Body Weight (Kg) | Suggested PK/PD Target(s) |
|---|---|---|---|---|---|---|---|---|---|---|
| Alshaer [22] | FEP, TZP, MEM | USA | 2022 | Before/after study | 23 (post-intervention) | 19 (pre-intervention) | 25 | 119 | Na | Cmin > MIC; Cmin > 4 × MIC |
| Aoki [23] | FEP | Japan | 2010 | Case report | 1 | Nap | 46 | 163 | Na | 60–70% fT > MIC |
| Bonapace [11] | FEP | USA | 1999 | Clinical PK study + population PK model | 12 | Nap | 36 | 135 | 84 | 60% T > MIC |
| Boucher [24] | IPM | USA | 1990 | Clinical PK study | 11 | Nap | 43 | 105 | 71 | None |
| Boucher [12] | IPM | USA | 2016 | Clinical PK study | 10 | Nap | 23 | In CRRT | Na | None |
| Bourget [25] | TZP | France | 1995 | Clinical PK study | 10 | Nap | 41 | 120 | 78 | 100% T > MIC |
| Conil [26] | CAZ, FEP | France | 2007 | Clinical PK study | 30 | Nap | Na | Na | Na | Cmin > 4 × MIC |
| Conil [27] | CAZ | France | 2007 | Clinical PK study + population PK model | 50 | Nap | 23 | 105 | 71 | None |
| Conil [28] 05 | CAZ | France | 2007 | Randomized controlled trial with clinical PK study | 15 | 15 | Na | Na | Na | Cmin > 4 × MIC |
| Conil [29] | CAZ | France | 2013 | Clinical PK study + population PK model | 70 | Nap | 32 | 118 | 74 | Steady state concentration of 40–100 mg/L |
| Corcione [16] | MEM | Italy | 2020 | Clinical PK study + population PK model | 17 | 34 | 134 | Na | BMI: 25 kg/m2 | 75% fT > MIC |
| Cotta [30] | MEM | Australia | 2015 | Case report | 1 | Nap | 50 | 129 | 100 | 54% fT > MIC; 10% fT > 4–6 MIC |
| Dailly [31] | IPM | France | 2003 | Clinical PK study + population PK model | 47 | Nap | 28 | Na | 75 | None |
| Dailly [32] | CAZ | France | 2003 | Clinical PK study + population PK model | 41 | Nap | 34 | Na (mean serum creatinine: 75 mmol/l) | 74 | None |
| Doh [33] | MEM | South Korea | 2010 | Clinical PK study + population PK model | 59 | 0 | 49 | 138 | 66 | 40% fT > MIC |
| Falcone [34] | ATM; CZA | Italy | 2021 | Clinical PK study + population PK model | 8 burn patients, 41 total patients | Nap | Na | Na | BMI: 24 kg/m2 | 100% fT > MIC |
| Fournier [14] | TZP; MEM | Switzerland | 2018 | Monocentric, unblinded, randomized, controlled trial | 19 | 19 | 20 | Na | Na | 100% fT > MIC |
| Friedrich [13] | ATM | USA | 1991 | Clinical PK study | 8 | Nap | 49 | Na | 83 | None |
| Gomez [35] | IPM | Brazil | 2015 | Clinical PK study + population PK model | 51 | 36 | Not specified, 36 patients with normal renal function and 15 with renal failure | 68 | Na | 40% fT > MIC |
| Hallam [36] | MEM | UK | 2010 | Case report | 1 | Nap | 52 | Na | Na | 100% fT > MIC |
| Jeon [37] | TZP | South Korea | 2014 | Clinical PK study + population PK model | 5 | Nap | 35 | 132 | 67 | 50% fT > MIC |
| Le Floch [38] | CAZ, IPM | France | 2009 | Clinical PK study | Number of patients not specified; 120 samples | Nap | 32 | 153 | 76 | 100% fT > 4xMIC |
| Li [17] | IPM | Belgium | 2018 | Clinical PK study + population PK model | 20 | Nap | Na | Na | Na | 40% fT > MIC |
| Machado [15] | TZP, IPM, MEM | Brazil | 2017 | Before/after study | 77 | 63 | 31 | Na | 81 | 100% fT > MIC for TZP; 60% fT > MIC for IPM and MEM |
| Messiano [39] | MEM | Brazil | 2022 | Clinical PK study | 15 | Nap | 33 | 100 | BMI: 24 kg/m2 | 100% fT > MIC |
| Olbrisch [40] | TZP | Germany | 2018 | Prospective cohort study with PK study + population PK model | 20 | 16 | 31 | Na | 80 | 100% fT > 4xMIC |
| Patel [41] | TZP; MEM | Australia | 2012 | Clinical PK study | 50 (6 on TZP, 1 on MEM) | Nap | 17 | 86 | Na | 100% fT > MIC; 100% fT > 4 × MIC |
| Por [42] | IPM | USA | 2021 | Clinical PK study + population PK model | 12 in CRRT | 11 not in CRRT | 43 | 132 | 98 | 40% fT > MIC |
| Ramon-Lopez [43] | MEM | UK | 2015 | Clinical PK study + population PK model | 12 | Nap | 41 | 137 | 83 | 40% T > MIC; 60% T > MIC; 80% T > MIC |
| Sampol [44] | FEP | France | 2000 | Clinical PK study | 6 | Nap | 32 | 123 | Na | None |
| Selig [45] | TZP | USA | 2022 | Case-control study + population PK model | 5 | 14 | 38 | 210 | 103 | 50% fT > MIC; 100% fT > MIC; 100% ft > 4 × MIC |
| Selig [46] | MEM | USA | 2022 | Case-control study + population PK model | 11 | 12 | 33 | 150 | 88 | 40% fT > MIC; 99% fT > MIC |
| Shikuma [47] | TZP | USA | 1990 | Clinical PK study | 9 | Nap | Na | 90–120 | Na | Not specified |
| Torian [48] | TZP | USA | 2023 | Case report | 1 | Nap | 3.2 | >120 | Na | 100% T > MIC |
| Walstad [49] | CAZ | Norway | 1998 | Clinical PK study with measurement of tissue concentration | 8 | Nap | 20–80 | Na | Na | None |
| Antibiotic | Advisable Drug Regimens in Burn Patients without Renal Impairment | Suggested Modalities of Preparation and Administration [50] |
|---|---|---|
| Ceftazidime | At least 1 g every 4 h or CI of 6 g/24 h (with loading dose) | Using syringe pump: 2 g in 50 mL of normal saline (0.9%) or glucose solution (5%), over 8 h, 3 times a day |
| Cefepime | 2 g every 8 h; consider CI of 6 g/24 h (with loading dose), particularly for severe infections or high MICs | Using syringe pump: 2 g in 50 mL of normal saline (0.9%) or glucose solution (5%), over 8 h, 3 times a day |
| Piperacillin-tazobactam | 18 g/24 h CI (with loading dose). Higher doses may be needed for patients with ARC or high MICs | Using syringe pump: 4.5 g in 50 mL of normal saline (0.9%) or glucose solution (5%), over 6 h, 4 times a day |
| Meropenem | 6 g/24 h CI (with loading dose). Higher doses may be needed for patients with ARC | Using syringe pump: 2 g in 50 mL of normal saline (0.9%), over 8 h, 3 times a day |
| Imipenem-cilastatin | 500 mg every 6 h; 1 g every 6 h if ARC or MIC > 2 mg/dL | 500 mg in 100 mL of normal saline (0.9%), in 30 min, 4 times a day; 1 g in 250 mL of normal saline (0.9%), over 1 h, 4 times a day. Continuous infusion not recommended due to stability issues |
| Aztreonam | 2 g every 8 h or 6–8 g in CI (particularly for high CLCR or high MICs) | 2 g in 100 mL of normal saline (0.9%), in 30 min, 3 times a day; Using syringe pump: 3 g in 50 mL of normal saline (0.9%), over 12 h, 2 times a day |
| Ceftaroline, ceftobiprole, ceftolozane-tazobactam, meropenem-vaborbactam, imipenem-cilastatin-relebactam, cefiderocol | No specific data on burn patients. Standard regimens:
|
|
| Ceftazidime-avibactam | Insufficient data. Standard regimen: 2.5 g every 8 h | 2.5 g in 50 mL of normal saline (0.9%), over 2 h, 3 times a day. Continuous infusion may be proposed. |
| Antibiotic | Dosages Used by EUCAST to Define Breakpoints [65] | EUCAST Clinical Breakpoint Tables v. 13.1 (mg/L) | Suggested PK/PD Target [21] | |||
|---|---|---|---|---|---|---|
| Standard Dosage | High Dosage | S≤ | R> | Pre-Clinical PK/PD Target for Efficacy | Clinical PK/PD Target for Efficacy | |
| Ceftazidime | 1 g × 3 | 2 g × 3 or 1 g × 6 | Ent: 1 Pa: 0.001 | Ent: 4 Pa: 8 | 60–70% fT > MIC | 40–100% fT > MIC |
| Cefepime | 1 g × 3 or 2 g × 2 | 2 g × 3. For severe P. aeruginosa infections: 2 g in 4 h × 3 | Ent: 1 Pa: 0.001 | Ent: 4 Pa: 8 | 60–70% fT > MIC | 40–100% fT > MIC |
| Piperacillin-tazobactam | 4.5 g × 4 or 4.5 g in 4 h × 3 | 4.5 g in 3 h × 4 | Ent: 8 Pa: 0.001 | Ent: 8 Pa: 16 | 50% fT > MIC | 50–100% fT > MIC |
| Meropenem | 1 g × 3 | 2 g in 3 h × 3 | Ent: 2 Pa: 2 | Ent: 8 Pa: 8 | 40% fT > MIC | 50–100% fT > MIC |
| Imipenem-clinastatin | 0.5 g × 4 | 1 g × 4 | Ent: 2 Pa: 0.001 | Ent: 4 Pa: 4 | 40% fT > MIC | 50–100% fT > MIC |
| Aztreonam | 1 g × 3 | 2 g × 4 | Ent: 1 Pa: 0.002 | Ent: 4 Pa: 16 | / | 50–100% fT > MIC [34] |
| Ceftolozane-tazobactam | 1.5 g × 3 | 3 g × 3 | Ent: 2 Pa: 4 | Ent: 2 Pa: 4 | / | / |
| Ceftazidime-avibactam | 2.5 g in 2 h × 3 | Ent: 8 Pa: 8 | Ent: 8 Pa: 8 | / | / | |
| Meropenem-vaborbactam | 4 g in 3 h × 3 | Ent: 8 Pa: 8 | Ent: 8 Pa: 8 | / | / | |
| Imipenem-cilastatin-relebactam | 0.75 g × 4 | none | Ent: 2 Pa: 2 | Ent: 2 Pa: 2 | / | / |
| Ceftaroline | 0.6 g × 2 | 0.6 g × 3 | Ent: 0.5 | Ent: 0.5 | / | / |
| Ceftobiprole | 0.5 in 2 h × 3 | none | Ent: 0.25 | Ent: 0.25 | / | / |
| Cefiderocol | 2 g in 3 h × 3 | none | Ent: 2 Pa: 2 | Ent: 2 Pa: 2 | / | / |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tebano, G.; la Martire, G.; Raumer, L.; Cricca, M.; Melandri, D.; Pea, F.; Cristini, F. Which Are the Best Regimens of Broad-Spectrum Beta-Lactam Antibiotics in Burn Patients? A Systematic Review of Evidence from Pharmacology Studies. Antibiotics 2023, 12, 1737. https://doi.org/10.3390/antibiotics12121737
Tebano G, la Martire G, Raumer L, Cricca M, Melandri D, Pea F, Cristini F. Which Are the Best Regimens of Broad-Spectrum Beta-Lactam Antibiotics in Burn Patients? A Systematic Review of Evidence from Pharmacology Studies. Antibiotics. 2023; 12(12):1737. https://doi.org/10.3390/antibiotics12121737
Chicago/Turabian StyleTebano, Gianpiero, Giulia la Martire, Luigi Raumer, Monica Cricca, Davide Melandri, Federico Pea, and Francesco Cristini. 2023. "Which Are the Best Regimens of Broad-Spectrum Beta-Lactam Antibiotics in Burn Patients? A Systematic Review of Evidence from Pharmacology Studies" Antibiotics 12, no. 12: 1737. https://doi.org/10.3390/antibiotics12121737
APA StyleTebano, G., la Martire, G., Raumer, L., Cricca, M., Melandri, D., Pea, F., & Cristini, F. (2023). Which Are the Best Regimens of Broad-Spectrum Beta-Lactam Antibiotics in Burn Patients? A Systematic Review of Evidence from Pharmacology Studies. Antibiotics, 12(12), 1737. https://doi.org/10.3390/antibiotics12121737