
Racial Disparities in Periprosthetic Joint Infections after Primary Total Joint Arthroplasty: A Retrospective Study

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Measures
2.1.1. Primary Outcome
2.1.2. Primary Exposure
2.1.3. Potential Confounders and Mediators
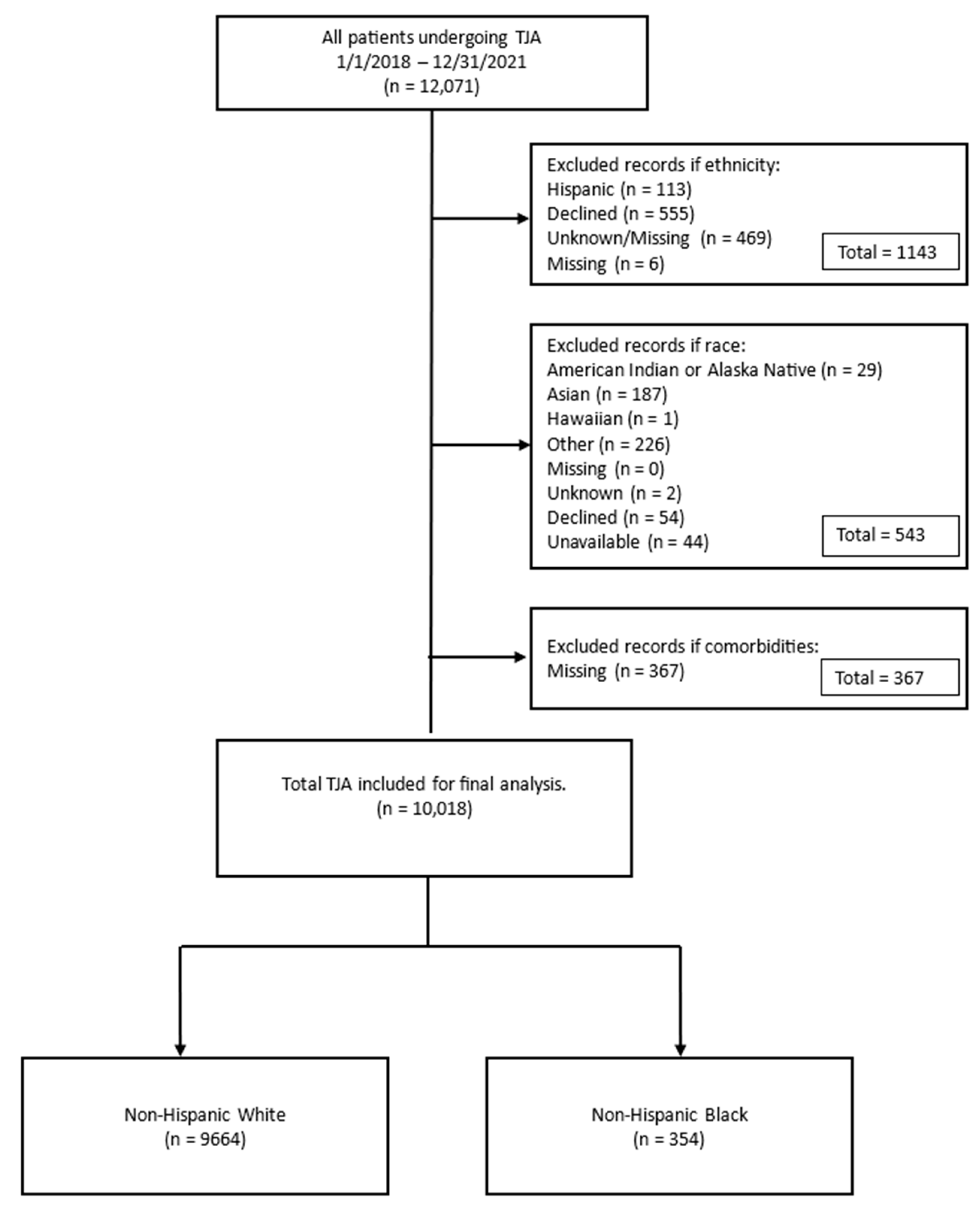
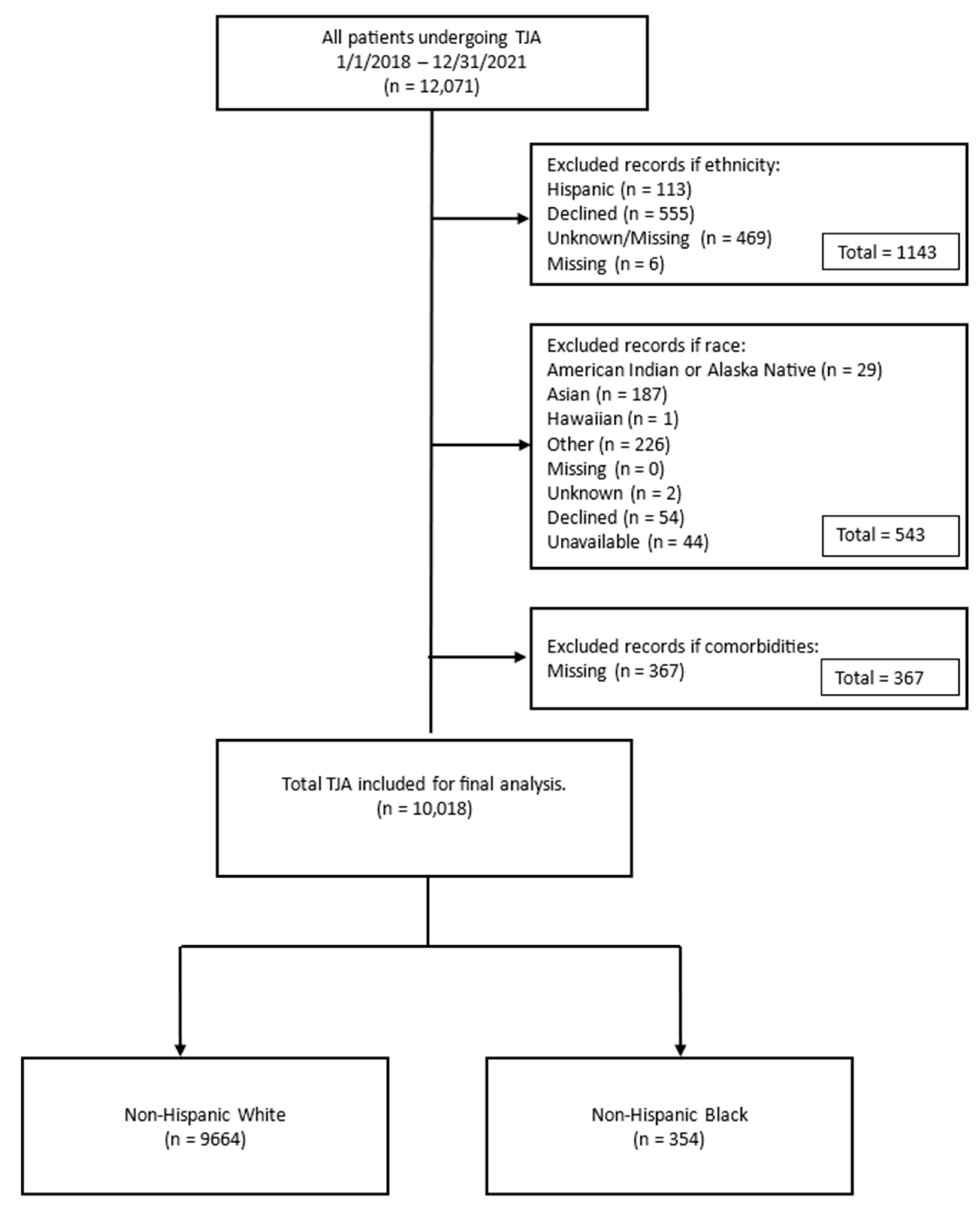
2.2. Inclusion/Exclusion Criteria
2.3. Statistical Analyses
3. Results
3.1. Descriptive Statistics
3.2. Bivariate Associations
3.3. Primary Outcome
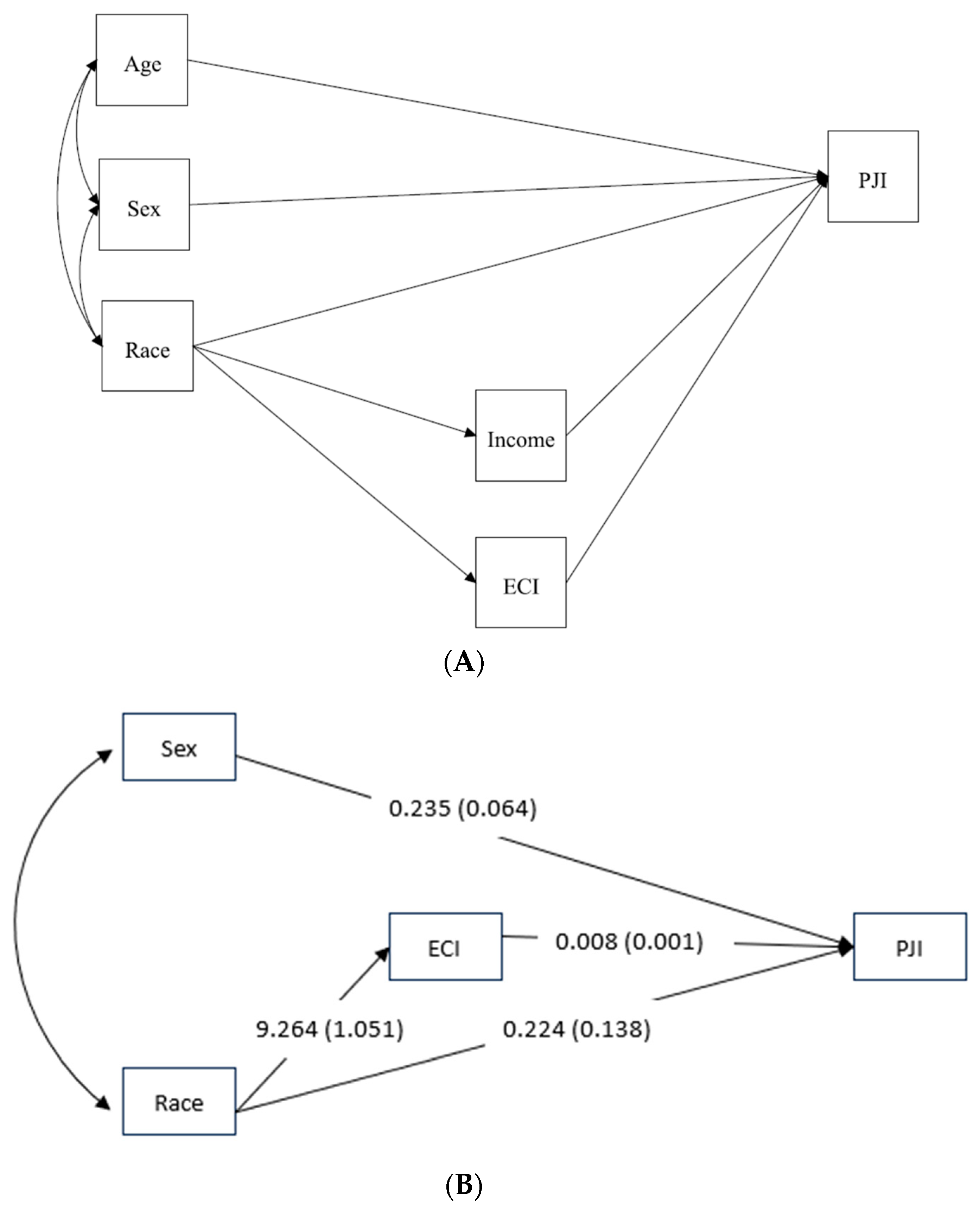
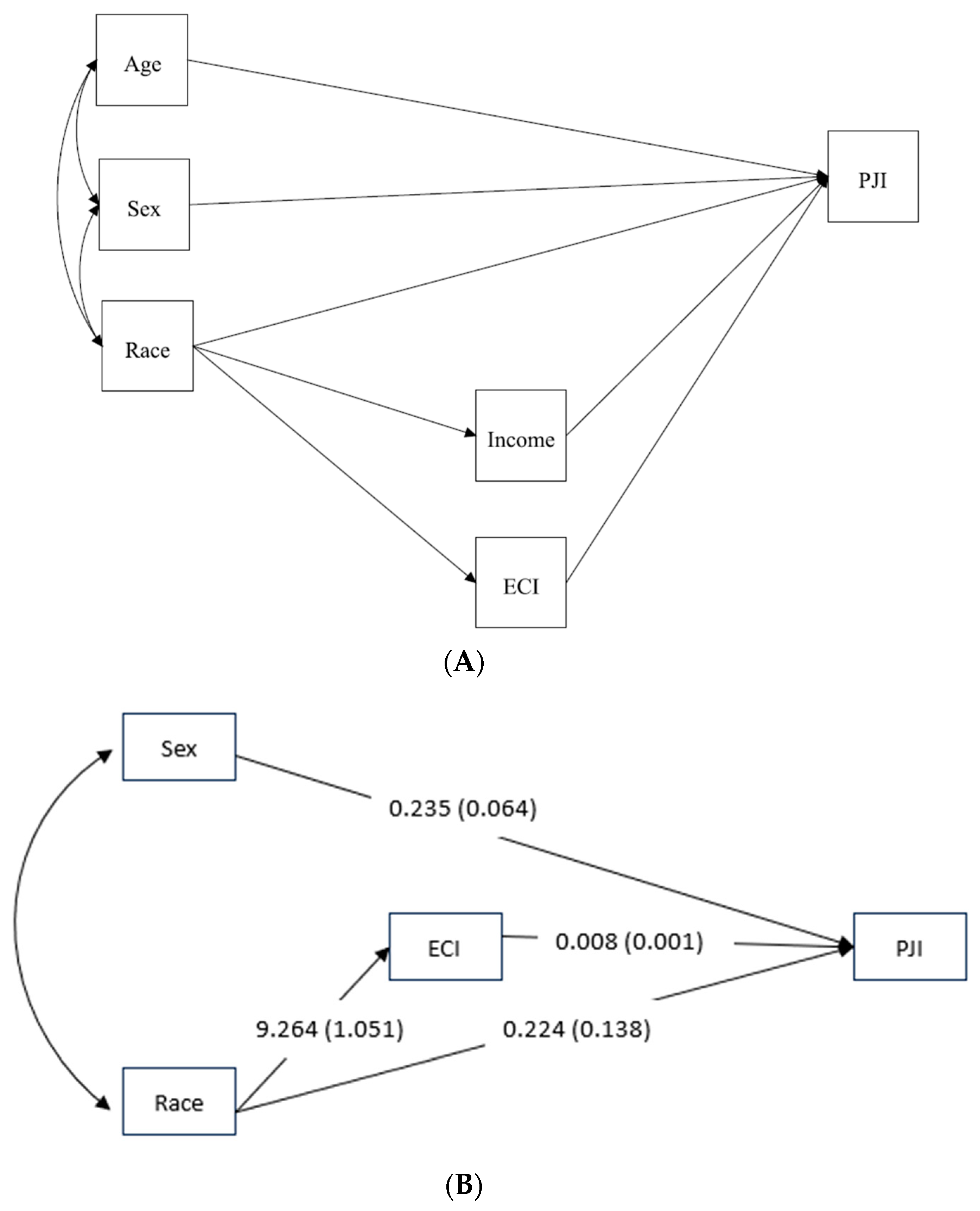
3.4. Mediation Analyses
4. Discussion
4.1. The Incidence of PJI in NH Black Individuals Was Twice That of NH White Individuals after Adjusting for Age and Sex
4.2. The Presence of Comorbidities Significantly Mediated the Relationship between Race and PJI and Explained 26% of the Total Effect of Race on the Incidence of PJI
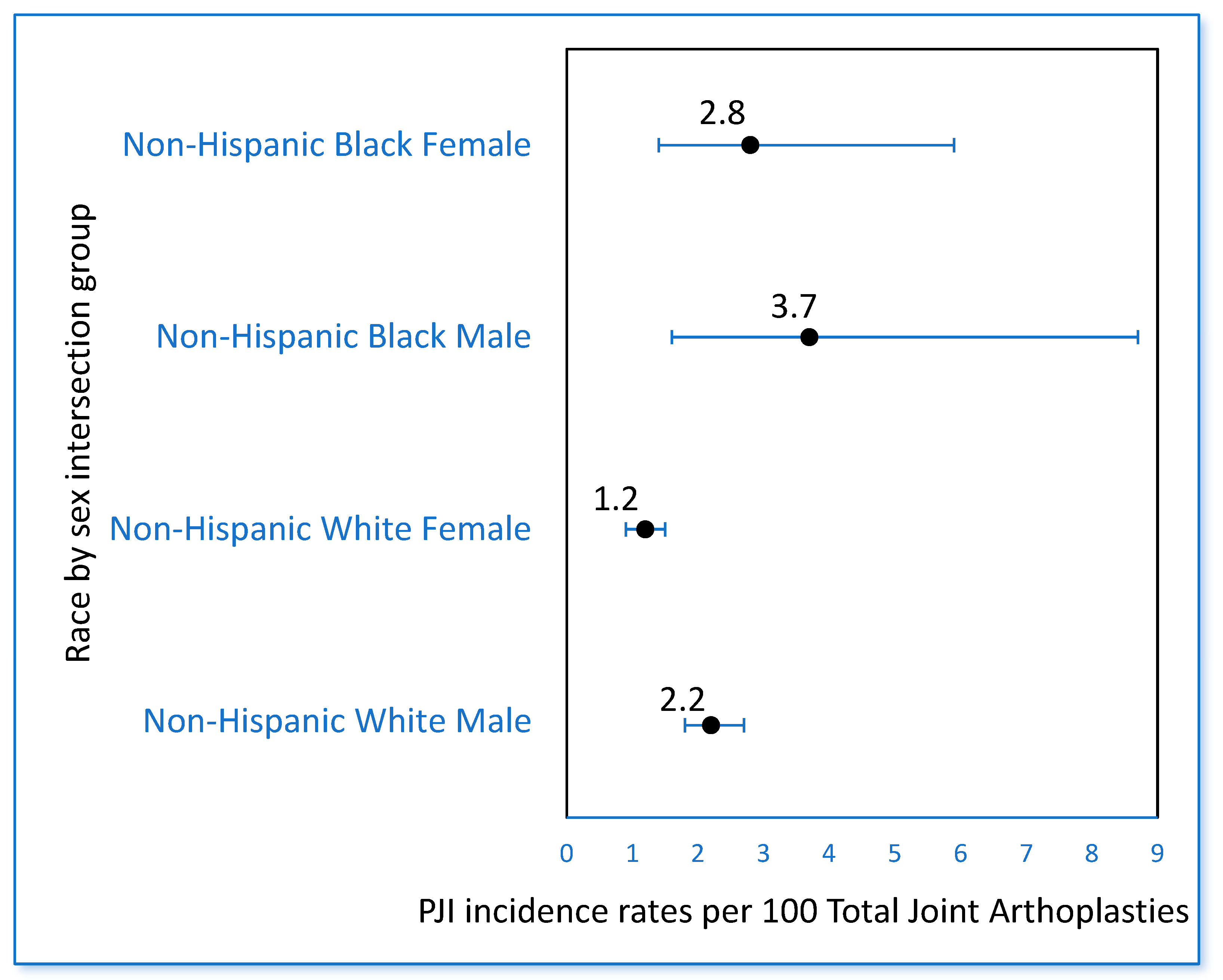
4.3. At the Intersection of Race and Sex, NH Black Males Had the Highest Incidence of PJI
4.4. Limitations
4.5. Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tande, A.J.; Patel, R. Prosthetic Joint Infection. Clin. Microbiol. Rev. 2014, 27, 302–345. [Google Scholar] [CrossRef] [PubMed]
- Namba, R.S.; Inacio, M.C.S.; Paxton, E.W. Risk Factors Associated with Deep Surgical Site Infections after Primary Total Knee Arthroplasty: An Analysis of 56,216 Knees. J. Bone Jt. Surg. Am. 2013, 95, 775–782. [Google Scholar] [CrossRef]
- Edwards, J.R.; Peterson, K.D.; Mu, Y.; Banerjee, S.; Allen-Bridson, K.; Morrell, G.; Dudeck, M.A.; Pollock, D.A.; Horan, T.C. National Healthcare Safety Network (NHSN) Report: Data Summary for 2006 through 2008, Issued December 2009. Am. J. Infect. Control 2009, 37, 783–805. [Google Scholar] [CrossRef] [PubMed]
- Premkumar, A.; Kolin, D.A.; Farley, K.X.; Wilson, J.M.; McLawhorn, A.S.; Cross, M.B.; Sculco, P.K. Projected Economic Burden of Periprosthetic Joint Infection of the Hip and Knee in the United States. J. Arthroplast. 2021, 36, 1484–1489.e3. [Google Scholar] [CrossRef]
- Zimmerli, W.; Trampuz, A.; Ochsner, P.E. Prosthetic Joint Infections. N. Engl. J. Med. 2004, 351, 1645–1654. [Google Scholar] [CrossRef]
- Kurtz, S.; Ong, K.; Lau, E.; Mowat, F.; Halpern, M. Projections of Primary and Revision Hip and Knee Arthroplasty in the United States from 2005 to 2030. J. Bone Jt. Surg. Am. 2007, 89, 780–785. [Google Scholar] [CrossRef]
- Beam, E.; Osmon, D. Prosthetic Joint Infection Update. Infect. Dis. Clin. N. Am. 2018, 32, 843–859. [Google Scholar] [CrossRef]
- Helwig, P.; Morlock, J.; Oberst, M.; Hauschild, O.; Hübner, J.; Borde, J.; Südkamp, N.P.; Konstantinidis, L. Periprosthetic Joint Infection—Effect on Quality of Life. Int. Orthop. 2014, 38, 1077–1081. [Google Scholar] [CrossRef]
- Blom, A.W.; Beswick, A.D.; Burston, A.; Carroll, F.E.; Garfield, K.; Gooberman-Hill, R.; Harris, S.; Kunutsor, S.K.; Lane, A.; Lenguerrand, E.; et al. Surgical Treatment of Prosthetic Joint Infection: The INFORM Randomised Controlled Trial Health Economic Analysis. In Infection after Total Joint Replacement of the Hip and Knee: Research Programme Including the INFORM RCT; National Institute for Health and Care Research: Southampton, UK, 2022. [Google Scholar]
- Xu, Y.; Huang, T.B.; Schuetz, M.A.; Choong, P.F.M. Mortality, Patient-Reported Outcome Measures, and the Health Economic Burden of Prosthetic Joint Infection. EFORT Open Rev. 2023, 8, 690–697. [Google Scholar] [CrossRef]
- Okewunmi, J.; Mihalopoulos, M.; Huang, H.-H.; Mazumdar, M.; Galatz, L.M.; Poeran, J.; Moucha, C.S. Racial Differences in Care and Outcomes after Total Hip and Knee Arthroplasties: Did the Comprehensive Care for Joint Replacement Program Make a Difference? J. Bone Jt. Surg. 2022, 104, 949–958. [Google Scholar] [CrossRef]
- Aseltine, R.H.; Wang, W.; Benthien, R.A.; Katz, M.; Wagner, C.; Yan, J.; Lewis, C.G. Reductions in Race and Ethnic Disparities in Hospital Readmissions Following Total Joint Arthroplasty from 2005 to 2015. J. Bone Jt. Surg. Am. 2019, 101, 2044–2050. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.C.; Green, T.M.; Burney, D.W. Movement Is Life—Optimizing Patient Access to Total Joint Arthroplasty: Dental Health Disparities. J. Am. Acad. Orthop. Surg. 2022, 30, 1036–1038. [Google Scholar] [CrossRef] [PubMed]
- Sabesan, V.J.; Rankin, K.A.; Nelson, C. Movement Is Life—Optimizing Patient Access to Total Joint Arthroplasty: Obesity Disparities. J. Am. Acad. Orthop. Surg. 2022, 30, 1028–1035. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, M.I.; Burney, D.; Jones, L.C. Movement Is Life—Optimizing Patient Access to Total Joint Arthroplasty: Smoking Cessation Disparities. J. Am. Acad. Orthop. Surg. 2022, 30, 1055–1058. [Google Scholar] [CrossRef]
- Wiznia, D.H.; Jimenez, R.; Harrington, M. Movement Is Life—Optimizing Patient Access to Total Joint Arthroplasty: Diabetes Mellitus Disparities. J. Am. Acad. Orthop. Surg. 2022, 30, 1017–1022. [Google Scholar] [CrossRef]
- Ayanian, J.Z.; Williams, R.A. Principles for Eliminating Racial and Ethnic Disparities in Health Care under Healthcare Reform. In Healthcare Disparities at the Crossroads with Healthcare Reform; Williams, R.A., Ed.; Springer: Boston, MA, USA, 2011; pp. 421–432. ISBN 978-1-4419-7136-4. [Google Scholar]
- Delgado, R.; Stefancic, J. Critical Race Theory: The Cutting Edge; Temple University Press: Philadelphia, PA, USA, 2000; ISBN 978-1-56639-714-8. [Google Scholar]
- Lopez, I.H. White by Law: The Legal Construction of Race; NYU Press: New York, NY, USA, 1996; ISBN 978-0-8147-5137-4. [Google Scholar]
- Miller, H.N.; LaFave, S.; Marineau, L.; Stephens, J.; Thorpe, R.J. The Impact of Discrimination on Allostatic Load in Adults: An Integrative Review of Literature. J. Psychosom. Res. 2021, 146, 110434. [Google Scholar] [CrossRef]
- Fernander, A. What Does Critical Race Theory Have to Do with Academic Medicine? J. Natl. Med. Assoc. 2022, 114, 274–277. [Google Scholar] [CrossRef]
- Smedley, A.; Smedley, B.D. Race as Biology Is Fiction, Racism as a Social Problem Is Real: Anthropological and Historical Perspectives on the Social Construction of Race. Am. Psychol. 2005, 60, 16–26. [Google Scholar] [CrossRef]
- Nalichowski, R.; Keogh, D.; Chueh, H.C.; Murphy, S.N. Calculating the Benefits of a Research Patient Data Repository. AMIA Annu. Symp. Proc. 2006, 2006, 1044. [Google Scholar]
- Elixhauser, A.; Steiner, C.; Harris, D.R.; Coffey, R.M. Comorbidity Measures for Use with Administrative Data. Med. Care 1998, 36, 8–27. [Google Scholar] [CrossRef]
- Agency for Healthcare Quality and Research Healthcare Cost and Utilization Project User Guide: Elixhauser Comorbidity Software Refined for ICD-10-CM Diagnoses, V2023.1. Available online: https://hcup-us.ahrq.gov/toolssoftware/comorbidityicd10/CMR-User-Guide-v2023-1.pdf. (accessed on 14 September 2023).
- Moore, B.J.; White, S.; Washington, R.; Coenen, N.; Elixhauser, A. Identifying Increased Risk of Readmission and In-Hospital Mortality Using Hospital Administrative Data: The AHRQ Elixhauser Comorbidity Index. Med. Care 2017, 55, 698–705. [Google Scholar] [CrossRef] [PubMed]
- US Income Statistics—Current Census Data for Zip Codes. Available online: https://www.incomebyzipcode.com/ (accessed on 26 June 2023).
- Löwik, C.A.M.; Zijlstra, W.P.; Knobben, B.A.S.; Ploegmakers, J.J.W.; Dijkstra, B.; de Vries, A.J.; Kampinga, G.A.; Mithoe, G.; Al Moujahid, A.; Jutte, P.C.; et al. Obese Patients Have Higher Rates of Polymicrobial and Gram-Negative Early Periprosthetic Joint Infections of the Hip than Non-Obese Patients. PLoS ONE 2019, 14, e0215035. [Google Scholar] [CrossRef] [PubMed]
- Humphrey, T.J.; Tatara, A.M.; Bedair, H.S.; Alpaugh, K.; Melnic, C.M.; Nelson, S.B. Rates and Outcomes of Periprosthetic Joint Infection in Persons Who Inject Drugs. J. Arthroplast. 2023, 38, 152–157. [Google Scholar] [CrossRef]
- Ndugga, N.; Artiga, S. Disparities in Health and Health Care. Available online: https://www.kff.org/racial-equity-and-health-policy/issue-brief/disparities-in-health-and-health-care-5-key-question-and-answers/ (accessed on 14 September 2023).
- Muthén, B.M.; Muthén, L. Mplus. In Handbook of Item Response Theory, 1st ed.; van der Linden, W.J., Ed.; Chapman and Hall/CRC: Boca Raton, FL, USA, 2017; ISBN 978-1-315-11743-0. [Google Scholar]
- Bollen, K.A.; Long, J.S. Testing Structural Equation Models; Sage Focus Editions; Sage Publications: Newbury Park, CA, USA, 1993; ISBN 978-0-8039-4506-7. [Google Scholar]
- Office of Disease Prevention and Health Promotion Health Equity in Healthy People 2030. Available online: https://health.gov/healthypeople/priority-areas/health-equity-healthy-people-2030 (accessed on 15 September 2023).
- Centers for Medicare & Medicaid Services States Advancing All-Payer Health Equity Approaches and Development (AHEAD) Model. Available online: https://www.cms.gov/priorities/innovation/innovation-models/ahead (accessed on 15 September 2023).
- Baddour, L.; Chen, A. Prosthetic Joint Infection: Epidemiology, Microbiology, Clinical Manifestations, and Diagnosis. Available online: https://www.uptodate.com/contents/prosthetic-joint-infection-epidemiology-microbiology-clinical-manifestations-and-diagnosis?search=periprosthetic%20joint%20infections&source=search_result&selectedTitle=2~150&usage_type=default&display_rank=2 (accessed on 16 September 2023).
- Nelson, S.B.; Pinkney, J.A.; Chen, A.F.; Tande, A.J. Periprosthetic Joint Infection: Current Clinical Challenges. Clin. Infect. Dis. 2023, 77, e34–e45. [Google Scholar] [CrossRef] [PubMed]
- Office of Disease Prevention and Health Promotion Reduce Drug Overdose Deaths—Data—Healthy People 2030. Available online: https://health.gov/healthypeople/objectives-and-data/browse-objectives/drug-and-alcohol-use/reduce-drug-overdose-deaths-su-03/data?group=Race/Ethnicity&from=2018&to=2021&state=United%20States&populations=#edit-submit (accessed on 15 September 2023).
- Washington, T.B.; Johnson, V.R.; Kendrick, K.; Ibrahim, A.A.; Tu, L.; Sun, K.; Stanford, F.C. Disparities in Access and Quality of Obesity Care. Gastroenterol. Clin. N. Am. 2023, 52, 429–441. [Google Scholar] [CrossRef]
- Nardone, A.; Rudolph, K.E.; Morello-Frosch, R.; Casey, J.A. Redlines and Greenspace: The Relationship between Historical Redlining and 2010 Greenspace across the United States. Environ. Health Perspect. 2021, 129, 17006. [Google Scholar] [CrossRef]
- Swope, C.B.; Hernández, D.; Cushing, L.J. The Relationship of Historical Redlining with Present-Day Neighborhood Environmental and Health Outcomes: A Scoping Review and Conceptual Model. J. Urban Health 2022, 99, 959–983. [Google Scholar] [CrossRef]
- Washington, H.A. A Terrible Thing to Waste: Environmental Racism and Its Assault on the American Mind, 1st ed.; Little, Brown Spark: New York, NY, USA, 2019; ISBN 978-0-316-50943-5. [Google Scholar]
- Hanna-Attisha, M. What the Eyes Don’t See: A Story of Crisis, Resistance, and Hope in an American City; One World: New York, NY, USA, 2018; ISBN 978-0-399-59083-2. [Google Scholar]
- Brown, E.J.; Polsky, D.; Barbu, C.M.; Seymour, J.W.; Grande, D. Racial Disparities in Geographic Access to Primary Care in Philadelphia. Health Aff. 2016, 35, 1374–1381. [Google Scholar] [CrossRef]
- Kaiser Family Foundation Adults Who Report Not Having a Personal Doctor/Health Care Provider by Sex. Available online: https://www.kff.org/other/state-indicator/percent-of-adults-reporting-not-having-a-personal-doctor-by-sex/?currentTimeframe=0&selectedRows=%7B%22states%22:%7B%22south-carolina%22:%7B%7D%7D%7D&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D (accessed on 18 June 2023).
- Essien, U.R.; Dusetzina, S.B.; Gellad, W.F. A Policy Prescription for Reducing Health Disparities—Achieving Pharmacoequity. JAMA 2021, 326, 1793–1794. [Google Scholar] [CrossRef]
- Mancher, M.; Leshner, A.I. The Effectiveness of Medication-Based Treatment for Opioid Use Disorder. In Medications for Opioid Use Disorder Save Lives; National Academies Press (US): Washington, DC, USA, 2019. [Google Scholar]
- Nguemeni Tiako, M.J. Addressing Racial & Socioeconomic Disparities in Access to Medications for Opioid Use Disorder amid COVID-19. J. Subst. Abuse Treat. 2021, 122, 108214. [Google Scholar] [CrossRef]
- Antonelli, B.; Chen, A.F. Reducing the Risk of Infection after Total Joint Arthroplasty: Preoperative Optimization. Arthroplasty 2019, 1, 4. [Google Scholar] [CrossRef] [PubMed]
- Ojikutu, B.O.; Stephenson, K.E.; Mayer, K.H.; Emmons, K.M. Building Trust in COVID-19 Vaccines and beyond through Authentic Community Investment. Am. J. Public Health 2021, 111, 366–368. [Google Scholar] [CrossRef]
- Basques, B.A.; Bell, J.A.; Fillingham, Y.A.; Khan, J.M.; Della Valle, C.J. Gender Differences for Hip and Knee Arthroplasty: Complications and Healthcare Utilization. J. Arthroplast. 2019, 34, 1593–1597.e1. [Google Scholar] [CrossRef]
- Crenshaw, K. Demarginalizing the Intersection of Race and Sex: A Black Feminist Critique of Antidiscrimination Doctrine, Feminist Theory and Antiracist Politics. Univ. Chic. Leg. Forum 1989, 1989, 139. [Google Scholar]
- Hankivsky, O. Women’s Health, Men’s Health, and Gender and Health: Implications of Intersectionality. Soc. Sci. Med. 2012, 74, 1712–1720. [Google Scholar] [CrossRef] [PubMed]
- Centers for Medicare and Medicaid Services Comprehensive Care for Joint Replacement Model. Available online: https://www.cms.gov/priorities/innovation/innovation-models/cjr (accessed on 15 September 2023).
- Obama, B. United States Health Care Reform: Progress to Date and next Steps. JAMA 2016, 316, 525–532. [Google Scholar] [CrossRef]
- Turcotte, J.J.; Brennan, J.C.; Holbert, S.E.; Dolle, S.S.; King, P.J. Enhanced Preoperative Education Pathways: A Step toward Reducing Disparities in Total Joint Arthroplasty Outcomes. J. Arthroplast. 2022, 37, 1233–1240.e1. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Characteristic | NH White (n = 9664) (no. %) | NH Black (n = 354) (no. %) |
|---|---|---|
| Age—years, mean (±SD) | 69 (±10) | 65 (±12) |
| Sex | ||
| Female | 5102 (52.8) | 226 (63.8) |
| Male | 4562 (47.2) | 128 (36.2) |
| Median Household Income †—mean (±SD) | 107,809 (±39,380) | 82,736 (±31,718) |
| Type of TJA * | ||
| TKA * | 5215 (54.0) | 193 (54.5) |
| THA * | 4449 (46.0) | 161 (45.5) |
| Comorbidities | ||
| Obesity | 2814 (29.1) | 168 (47.5) |
| Hypertension, uncomplicated | 6.066 (62.8) | 279 (78.8) |
| Hypertension, complicated | 1153 (11.9) | 85 (24.0) |
| Chronic pulmonary disease | 2255 (23.3) | 120 (33.9) |
| Diabetes, uncomplicated | 1331 (13.8) | 114 (32.2) |
| Diabetes, complicated | 854 (8.8) | 73 (20.6) |
| Renal failure | 1.040 (10.8) | 79 (22.3) |
| Liver disease | 1015 (10.5) | 59 (16.7) |
| HIV/AIDS | 21 (0.2) | 3 (0.8) |
| Metastatic cancer | 540 (5.6) | 13 (3.9) |
| Rheumatological disorders | 1261 (13.0) | 70 (19.8) |
| Blood loss anemia | 272 (2.8) | 26 (7.3) |
| Deficiency anemia | 831 (8.6) | 61 (17.2) |
| Alcohol abuse | 506 (5.2) | 24 (6.8) |
| Substance abuse | 585 (6.1) | 44 (12.4) |
| Psychoses | 81 (0.8) | 8 (2.3) |
| Depression | 2582 (26.7) | 118 (33.3) |
| Elixhauser Comorbidity Index—mean (±SD) | 18.2 (±22.6) | 27.5 (±26.9) |
| Estimate | S.E. | Est./S.E. | p-Value (Two-Tailed) | |
|---|---|---|---|---|
| PJI regressed on | ||||
| Sex | 0.235 | 0.064 | 3.691 | <0.0001 |
| Race | 0.224 | 0.138 | 1.626 | 0.104 |
| ECI | 0.008 | 0.001 | 7.140 | <0.0001 |
| ECI regressed on | ||||
| Race | 9.264 | 1.051 | 8.815 | <0.0001 |
| Effects from race to ECI to PJI | ||||
| Total | 0.301 | 0.138 | 2.173 | 0.030 |
| Indirect | 0.077 | 0.014 | 5.559 | <0.0001 |
| Direct | 0.224 | 0.138 | 1.626 | 0.104 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pinkney, J.A.; Davis, J.B.; Collins, J.E.; Shebl, F.M.; Jamison, M.P.; Acosta Julbe, J.I.; Bogart, L.M.; Ojikutu, B.O.; Chen, A.F.; Nelson, S.B. Racial Disparities in Periprosthetic Joint Infections after Primary Total Joint Arthroplasty: A Retrospective Study. Antibiotics 2023, 12, 1629. https://doi.org/10.3390/antibiotics12111629
Pinkney JA, Davis JB, Collins JE, Shebl FM, Jamison MP, Acosta Julbe JI, Bogart LM, Ojikutu BO, Chen AF, Nelson SB. Racial Disparities in Periprosthetic Joint Infections after Primary Total Joint Arthroplasty: A Retrospective Study. Antibiotics. 2023; 12(11):1629. https://doi.org/10.3390/antibiotics12111629
Chicago/Turabian StylePinkney, Jodian A., Joshua B. Davis, Jamie E. Collins, Fatma M. Shebl, Matthew P. Jamison, Jose I. Acosta Julbe, Laura M. Bogart, Bisola O. Ojikutu, Antonia F. Chen, and Sandra B. Nelson. 2023. "Racial Disparities in Periprosthetic Joint Infections after Primary Total Joint Arthroplasty: A Retrospective Study" Antibiotics 12, no. 11: 1629. https://doi.org/10.3390/antibiotics12111629
APA StylePinkney, J. A., Davis, J. B., Collins, J. E., Shebl, F. M., Jamison, M. P., Acosta Julbe, J. I., Bogart, L. M., Ojikutu, B. O., Chen, A. F., & Nelson, S. B. (2023). Racial Disparities in Periprosthetic Joint Infections after Primary Total Joint Arthroplasty: A Retrospective Study. Antibiotics, 12(11), 1629. https://doi.org/10.3390/antibiotics12111629