
Use of a Silver-Impregnated Vascular Graft: Single-Center Experience

 ,
,
Abstract
1. Introduction
2. Methods
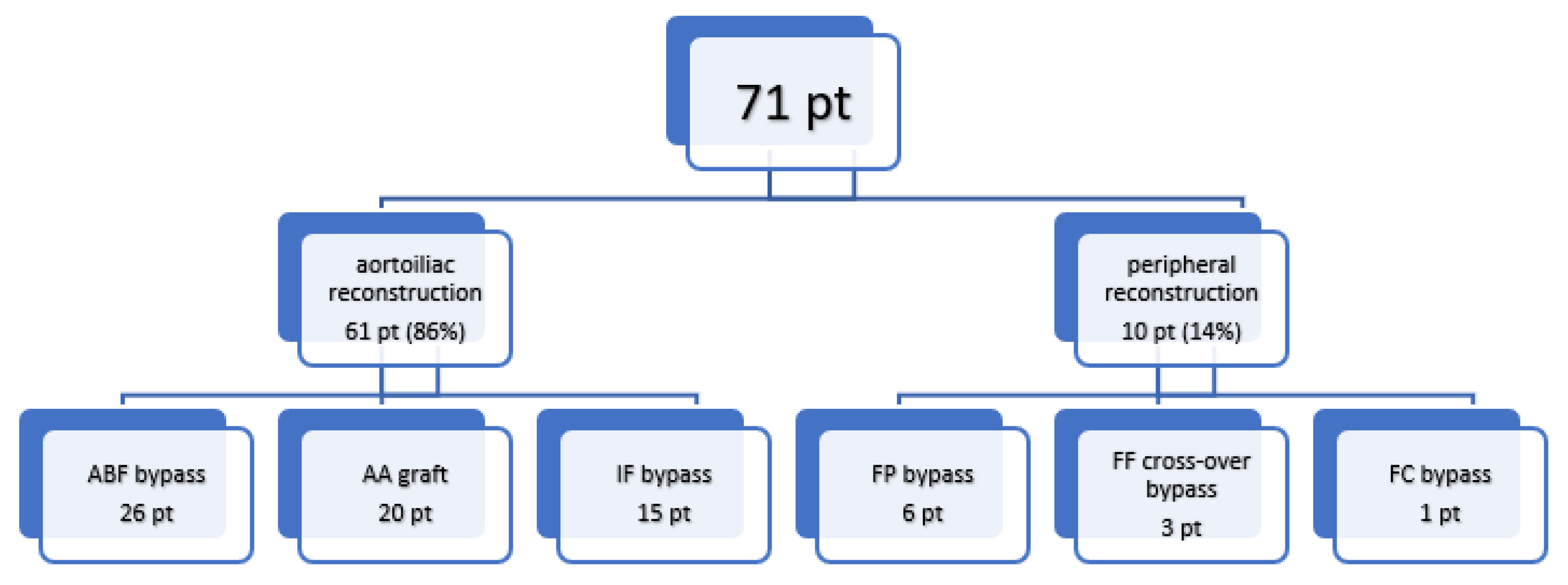
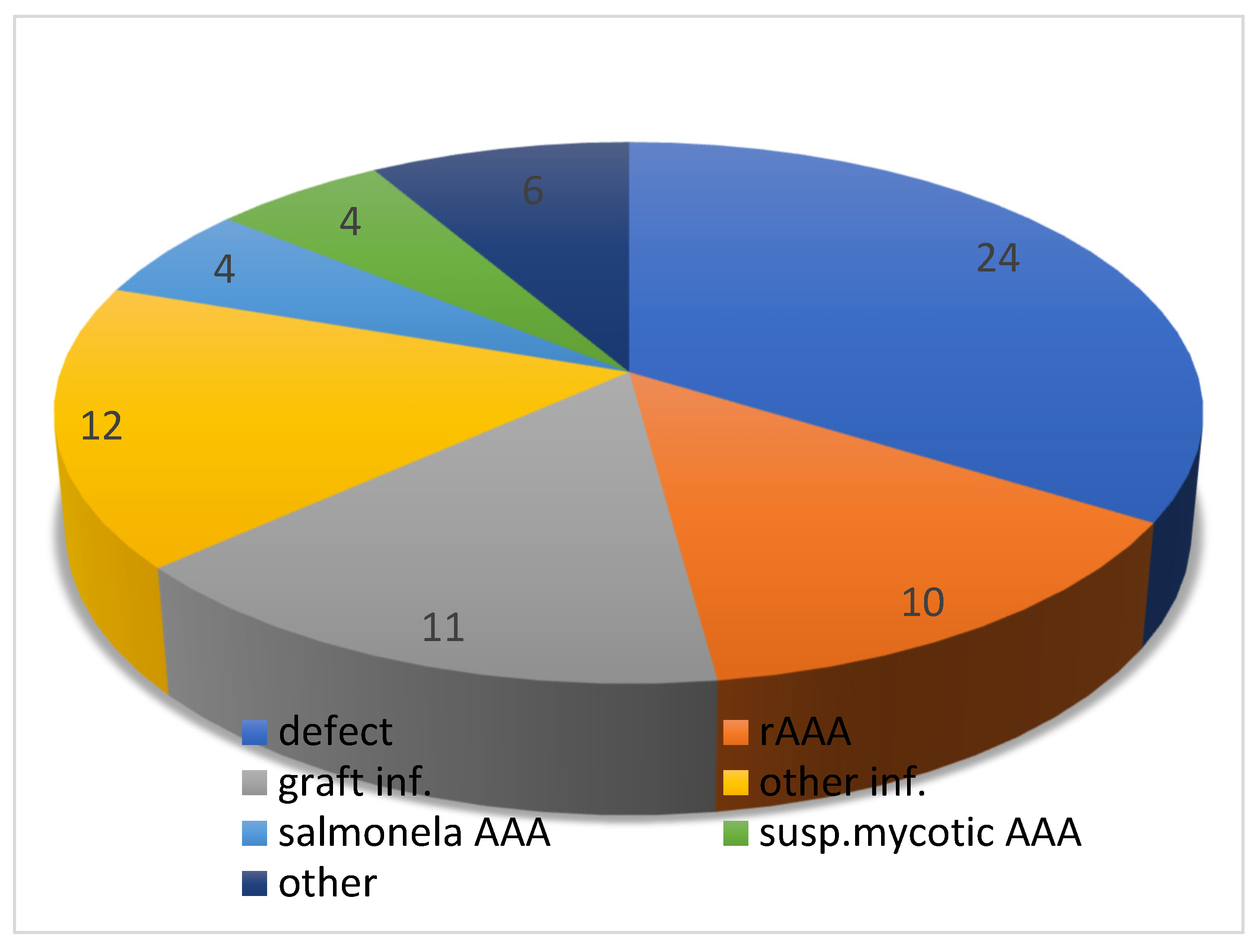
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Batt, M.; Feugier, P.; Camou, F.; Coffy, A.; Senneville, E.; Caillon, J.; Calvet, B.; Chidiac, C.; Laurent, F.; Revest, M.; et al. A Meta-Analysis of Outcomes after In Situ Reconstructions for Aortic Graft Infection. Angiology 2018, 69, 370–379. [Google Scholar] [CrossRef] [PubMed]
- Gharamti, A.; Kanafani, Z.A. Vascular Graft Infections An update. Infect. Dis. Clin. N. Am. 2018, 32, 789–809. [Google Scholar] [CrossRef] [PubMed]
- Seeger, J.M. Management of patients with prosthetic vascular graft infection. Am. Surg. 2000, 66, 166–177. [Google Scholar] [PubMed]
- Blaha, L.; Bulejčík, J.; Říha, D. Vascular graft infection in the aortoiliac territory—Our view in the light of European Society for Vascular Surgery Guidelines—The retrospective observation study. Perspect. Surg. 2021, 100, 330–338. [Google Scholar] [CrossRef]
- Sebesta, P.; Stádler, P.; Sedivý, P.; Zdráhal, P.; El Samman, K.; Jindrák, V.; Syrůcek, M. Radikální operace infekce cévní protézy v aortofemorální pozici s pomocí cerstvého tepenného allograftu: Nase strednedobé zkus-enosti [Radical operation of infected aortofemoral prosthesis using fresh arterial allograft: Our mid-term experience]. Rozhl. V Chir. 2011, 90, 4–13. (In Czech) [Google Scholar]
- Shiraev, T.P.; de Boer, M.; Joseph, S.; Loa, J.; Qasabian, R. Aortic graft explants—A single institution analysis of incidence and outcomes. Vascular 2022. [Google Scholar] [CrossRef]
- Ricco, J.-B. InterGard silver bifurcated graft: Features and results of a multicenter clinical study. J. Vasc. Surg. 2006, 44, 339–346. [Google Scholar] [CrossRef]
- El-Gamel, A. Proximal Aortic Graft Infection: Time for Treatment in an Aortic Centre? Heart Lung Circ. 2022, 31, 4–6. [Google Scholar] [CrossRef]
- Puges, M.; Bérard, X.; Caradu, C.; Accoceberry, I.; Gabriel, F.; Cazanave, C. Fungal Vascular Graft and Endograft Infections are Frequently Associated with Aorto-Enteric Fistulas. Eur. J. Vasc. Endovasc. Surg. 2021, 62, 819–820. [Google Scholar] [CrossRef]
- Rufa, M.; Ursulescu, A.; Stan, A.; Göbel, N.; Albert, M.; Franke, U.F.W. Cryopreserved aortic homograft, lifeline treatment for infected vascular prosthesis with mediastinal abscess in a re-redo case. J. Surg. Case Rep. 2022, 2022, rjab644. [Google Scholar] [CrossRef]
- Kouijzer, I.J.; Van der Jagt, M.F.; Bleeker-Rovers, C.P.; Dirven, M.; de Mast, Q.; Poyck, P.P. Outcome in Patients after Autologous Femoral Vein Reconstruction for Primary Aortic Infection and Aortic Graft Infection: A Case Series. Ann. Vasc. Surg. 2021, 18. [Google Scholar] [CrossRef]
- Neufang, A.; Savvidis, S. Operative technique and morbidity of superficial femoral vein harvest. Gefässchirurgie 2016, 21, 45–54. [Google Scholar] [CrossRef][Green Version]
- Spacek, M.; Měřička, P.; Janoušek, L.; Štádler, P.; Adamec, M.; Vlachovský, R.; Guňka, I.; Navrátil, P.; Thieme, F.; Špunda, R.; et al. Current vascular allograft procurement, cryopreservation and transplantation techniques in the Czech Republic. Adv. Clin. Exp. Med. 2019, 28, 529–534. [Google Scholar] [CrossRef]
- Larena-Avellaneda, A.; Russmann, S.; Fein, M.; Debus, E.S. Prophylactic use of the silver-acetate–coated graft in arterial occlusive disease: A retrospective, comparative study. J. Vasc. Surg. 2009, 50, 790–798. [Google Scholar] [CrossRef][Green Version]
- Berard, X.; Puges, M.; Pinaquy, J.-B.; Cazanave, C.; Stecken, L.; Bordenave, L.; Pereyre, S.; M’Zali, F. In vitro Evidence of Improved Antimicrobial Efficacy of Silver and Triclosan Containing Vascular Grafts Compared with Rifampicin Soaked Grafts. Eur. J. Vasc. Endovasc. Surg. 2019, 57, 424–432. [Google Scholar] [CrossRef]
- Berger, P.; Van Herwaarden, J.A.; Harkisoen, S.; De Vries, J.P.; Ekkelenkamp, M.; Moll, F.L. Surgical treatment of infected aortic grafts. J. Cardiovasc. Surg. 2012, 53, 719–734. [Google Scholar]
- McGuinness, B.; Ali, K.P.; Phillips, S.; Stacey, M. A Scoping Review on the Use of Antibiotic-Impregnated Beads and Applications to Vascular Surgery. Vasc. Endovasc. Surg. 2019, 54, 147–161. [Google Scholar] [CrossRef]
- Clemens, M.S.; Stull, M.C.; Hata, K.W.; Heafner, T.A.; Watson, J.D.B.; Arthurs, Z.M.; Propper, B.W. Antimicrobial-bonded graft patency in the setting of a polymicrobial infection in swine (Sus scrofa). J. Vasc. Surg. 2017, 66, 1210–1216. [Google Scholar] [CrossRef]
- Bisdas, T.; Beckmann, E.; Marsch, G.; Burgwitz, K.; Wilhelmi, M.; Kuehn, C.; Haverich, A.; Teebken, O. Prevention of Vascular Graft Infections with Antibiotic Graft Impregnation Prior to Implantation: In Vitro Comparison between Daptomycin, Rifampin and Nebacetin. Eur. J. Vasc. Endovasc. Surg. 2012, 43, 448–456. [Google Scholar] [CrossRef]
- Mufty, H.; Eynde, J.V.D.; Meuris, B.; Metsemakers, W.-J.; Van Wijngaerden, E.; Vandendriessche, T.; Steenackers, H.P.; Fourneau, I. Pre-clinical in vivo Models of Vascular Graft Coating in the Prevention of Vascular Graft Infection: A Systematic Review. Eur. J. Vasc. Endovasc. Surg. 2021, 62, 99–118. [Google Scholar] [CrossRef]
- Honig, S.; Seeger, P.; Rohde, H.; Kölbel, T.; Debus, E.S.; Diener, H. Efficacy of antiseptic impregnation of aortic endografts with rifampicin compared to silver against in vitro contamination with four bacteria that frequently cause vascular graft infections. JVS Vasc. Sci. 2020, 1, 181–189. [Google Scholar] [CrossRef]
- Szeberin, Z.; Münch, Z.; Fehérvári, M.; Bíró, G.; Entz, L.; Acsády, G. Ezüst-acetáttal bevont Dacron grafttal végzett rekonstrukciós érműtétek középtávú eredményei [Mid-term results of silver-coated Dacron graft implanta-tion in aortic and lower extremity revascularization]. Magy. Sebészet 2010, 63, 369–373. [Google Scholar] [CrossRef]
- Mufty, H.; Eynde, J.V.D.; Steenackers, H.P.; Metsemakers, W.-J.; Meuris, B.; Fourneau, I. A systematic review of preclinical data regarding commercial silver-coated vascular grafts. J. Vasc. Surg. 2021, 74, 1386–1393.e1. [Google Scholar] [CrossRef]
- Hassen-Khodja, R.; Sadaghianloo, N.; Jean-Baptiste, É. Matériaux de reconstruction aortique résistants à la contamination bactérienne [Aortic reconstruction with graft materials resistant to bacterial infections]. Bull. L’academie Natl. Med. 2013, 197, 979–991. discussion 991; (In French) [Google Scholar]
- Kessler, V.; Klopf, J.; Eilenberg, W.; Neumayer, C.; Brostjan, C. AAA Revisited: A Comprehensive Review of Risk Factors, Management, and Hallmarks of Pathogenesis. Biomedicines 2022, 10, 94. [Google Scholar] [CrossRef]
- Golemovic, M.; Skific, M.; Haluzan, D.; Pavic, P.; Cepulic, B.G. Ten-year experience with cryopreserved vascular allografts in the Croatian Cardiovascular Tissue Bank. Cell Tissue Bank. 2022, 1–18. [Google Scholar] [CrossRef]
- Wilson, W.R.; Bower, T.C.; Creager, M.A.; Amin-Hanjani, S.; O’Gara, P.T.; Lockhart, P.B.; Darouiche, R.O.; Ramlawi, B.; Derdeyn, C.; Bolger, A.F.; et al. Vascular Graft Infections, Mycotic Aneurysms, and Endovascular Infections: A Scientific Statement from the American Heart Association. Circulation 2016, 134, e412–e460. [Google Scholar] [CrossRef]
- Bisdas, T.; Wilhelmi, M.; Haverich, A.; Teebken, O.E. Cryopreserved arterial homografts vs silver-coated Dacron grafts for abdominal aortic infections with intraoperative evidence of microorganisms. J. Vasc. Surg. 2011, 53, 1274–1281.e4. [Google Scholar] [CrossRef]
- Hardman, S.; Cope, A.; Swann, A.; Bell, P.; Naylor, A.; Hayes, P. An In Vitro Model to Compare the Antimicrobial Activity of Silver-Coated Versus Rifampicin-Soaked Vascular Grafts. Ann. Vasc. Surg. 2004, 18, 308–313. [Google Scholar] [CrossRef]
- Tîlmaciu, C.-M.; Mathieu, M.; Lavigne, J.-P.; Toupet, K.; Guerrero, G.; Ponche, A.; Amalric, J.; Noël, D.; Mutin, P.H. In vitro and in vivo characterization of antibacterial activity and biocompatibility: A study on silver-containing phosphonate monolayers on titanium. Acta Biomater. 2015, 15, 266–277. [Google Scholar] [CrossRef]
- Mohseni, M.; Shamloo, A.; Aghababaei, Z.; Vossoughi, M.; Moravvej, H. Antimicrobial Wound Dressing Containing Silver Sulfadiazine with High Biocompatibility: In Vitro Study. Artif. Organs 2016, 40, 765–773. [Google Scholar] [CrossRef] [PubMed]
- Rozhin, A.; Batasheva, S.; Kruychkova, M.; Cherednichenko, Y.; Rozhina, E.; Fakhrullin, R. Biogenic Silver Nanoparticles: Synthesis and Application as Antibacterial and Antifungal Agents. Micromachines 2021, 12, 1480. [Google Scholar] [CrossRef] [PubMed]
- Al-Zoubi, N.A.; Al-Shawwa, Z. Complications of endo-vascular aortic repair for abdominal aortic aneurysm: A retrospective single-centre experience. Ann. Med. Surg. 2021, 64, 102219. [Google Scholar] [CrossRef] [PubMed]
- Berard, X.; Stecken, L.; Pinaquy, J.-B.; Cazanave, C.; Puges, M.; Pereyre, S.; Bordenave, L.; M’Zali, F. Comparison of the Antimicrobial Properties of Silver Impregnated Vascular Grafts with and without Triclosan. Eur. J. Vasc. Endovasc. Surg. 2016, 51, 285–292. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (y) | Male | Female | Total |
|---|---|---|---|
| Age 40–60 | 11 | 6 | 17 |
| Age 60–70 | 25 | 10 | 35 |
| Age 70–80 | 14 | 2 | 16 |
| Age above 80 | 3 | 0 | 3 |
| Comorbidity | |||
| DM | 16 | 3 | 19 |
| CHHF | 18 | 5 | 23 |
| CHRF | 13 | 1 | 14 |
| AH | 39 | 11 | 50 |
| ISS | 5 | 0 | 5 |
| ATB | |||
| Cephazolin (prophylaxis) | 25 | 10 | 35 |
| Cefuroxime | 5 | 2 | 7 |
| Vancomycin | 10 | 3 | 13 |
| Ciprofloxacin | 2 | 1 | 3 |
| Combination | 11 | 2 | 13 |
| Type of Reconstruction | |||
| Aortoiliac region | 49 | 12 | 61 |
| Peripheral region | 4 | 6 | 10 |
| Male | Female | Total (%) | |
|---|---|---|---|
| 30-Day Mortality | 11 | 3 | 14 (19.7%) |
| Hemorrhagic shock | 3 | 0 | 3 |
| Multiorgan failure | 6 | 2 | 8 |
| Sepsis | 1 | 1 | 2 |
| Morbidity | 23 | 7 | 30 (42.2%) |
| Respiratory failure | 11 | 6 | 17 |
| Multiorgan failure | 10 | 3 | 13 |
| Wound infection | 15 | 3 | 18 |
| Sepsis | 6 | 0 | 10 |
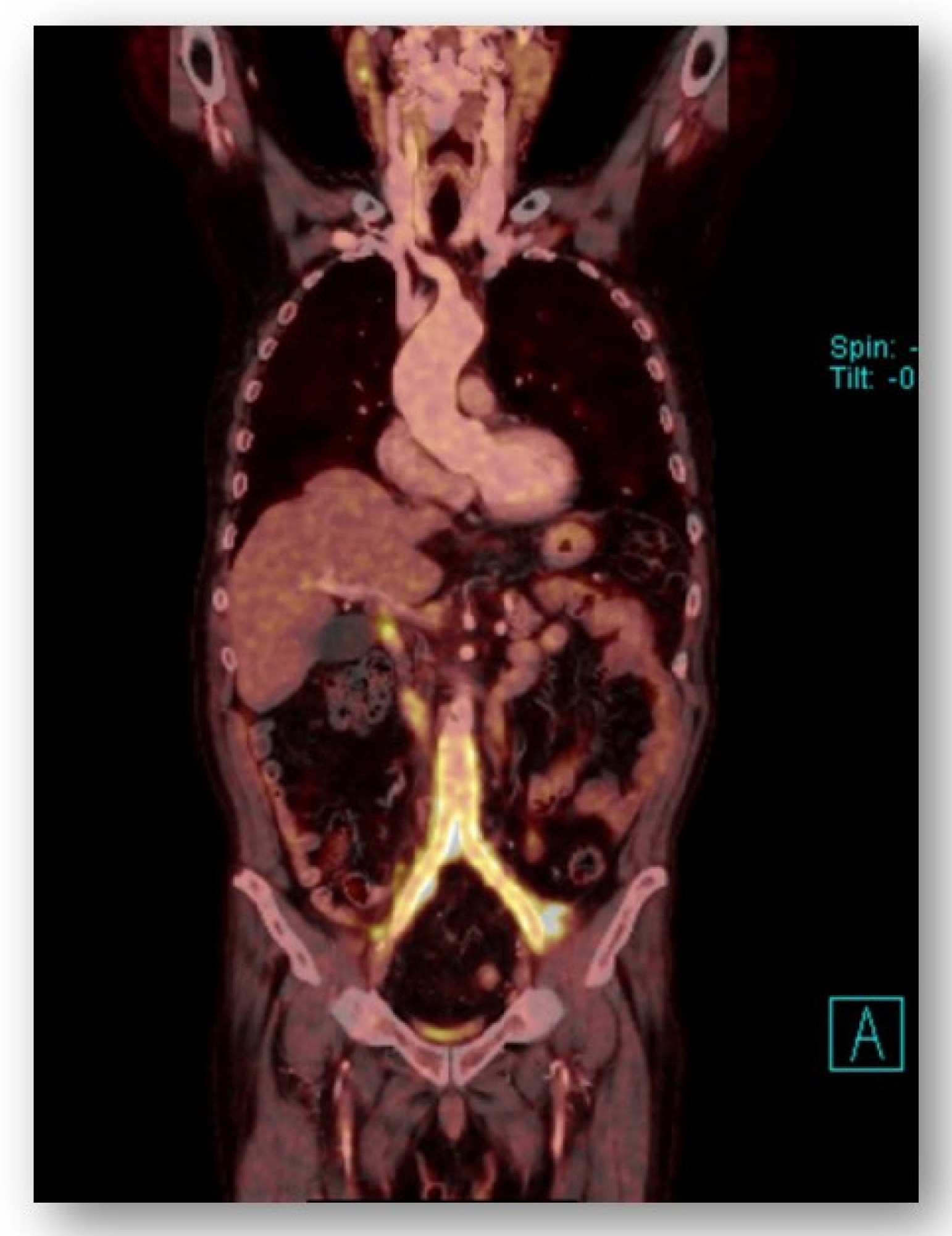
| Sex/Age | Time to Reinfection | Diagnosis | Type of Reconstruction | Indication to SG | Infectious Agents | Solution | Result |
|---|---|---|---|---|---|---|---|
| Male/72 | 12 months | PET/CT positive cultures | Aortobifemoral graft | Rupture of mycotic AAA | Salmonella enteritidis | Re-operation, graft replacement with aortic allograft | OK |
| Female/68 | 6 months | PET/CT positive cultures | Femoropopliteal bypass | Lower limb gangrene | Staphylococcus aureus | Conservative treatment (ATB—vancomycin) | OK |
| Male/63 | 2 years | PET/CT positive cultures | Femoropopliteal bypass | Previous regular vascular graft infection | Staphylococcus aureus | Conservative treatment (ATB—vancomycin) | OK |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Molacek, J.; Treska, V.; Houdek, K.; Opatrný, V.; Certik, B.; Baxa, J. Use of a Silver-Impregnated Vascular Graft: Single-Center Experience. Antibiotics 2022, 11, 386. https://doi.org/10.3390/antibiotics11030386
Molacek J, Treska V, Houdek K, Opatrný V, Certik B, Baxa J. Use of a Silver-Impregnated Vascular Graft: Single-Center Experience. Antibiotics. 2022; 11(3):386. https://doi.org/10.3390/antibiotics11030386
Chicago/Turabian StyleMolacek, Jiri, Vladislav Treska, Karel Houdek, Václav Opatrný, Bohuslav Certik, and Jan Baxa. 2022. "Use of a Silver-Impregnated Vascular Graft: Single-Center Experience" Antibiotics 11, no. 3: 386. https://doi.org/10.3390/antibiotics11030386
APA StyleMolacek, J., Treska, V., Houdek, K., Opatrný, V., Certik, B., & Baxa, J. (2022). Use of a Silver-Impregnated Vascular Graft: Single-Center Experience. Antibiotics, 11(3), 386. https://doi.org/10.3390/antibiotics11030386