
Trends, Variation, and Factors Influencing Antibiotic Prescribing: A Longitudinal Study in Primary Care Using a Multilevel Modelling Approach


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting
2.3. Antibiotic Prescribing Data
2.4. Factors Associated with Antibiotic Prescribing
2.5. Statistical Analysis
3. Results
3.1. Temporal Changes and Between-Practice Variation in Antibiotic Prescribing
3.2. Factors Influencing Antibiotic Prescribing
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ventola, C.L. The antibiotic resistance crisis: Part 1: Causes and threats. Pharm. Ther. 2015, 40, 277. [Google Scholar]
- Prestinaci, F.; Pezzotti, P.; Pantosti, A. Antimicrobial resistance: A global multifaceted phenomenon. Pathog. Glob. Health 2015, 109, 309–318. [Google Scholar] [CrossRef]
- Review on Antimicrobial Resistance. Antimicrobial Resistance: Tackling a Crisis for the Health and Wealth of Nations; HM Government and Welcome Trust: London, UK, 2014; Available online: https://wellcomecollection.org/works/rdpck35v (accessed on 7 February 2021).
- Cassini, A.; Högberg, L.D.; Plachouras, D.; Quattrocchi, A.; Hoxha, A.; Simonsen, G.S.; Colomb-Cotinat, M.; Kretzschmar, M.E.; Devleesschauwer, B.; Cecchini, M.; et al. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European Economic Area in 2015: A population-level modelling analysis. Lancet Infect Dis. 2019, 19, 56–66. [Google Scholar] [CrossRef]
- Department of Health. UK Five Year Antimicrobial Resistance Strategy 2013 to 2018; Department of Health and Social Care: London, UK, 2013. Available online: https://www.gov.uk/government/publications/uk-5-year-antimicrobial-resistance-strategy-2013-to-2018 (accessed on 7 May 2021).
- Ashiru-Oredope, D.; Hopkins, S.; English Surveillance Programme for Antimicrobial Utilization and Resistance Oversight Group. Antimicrobial stewardship: English Surveillance Programme for Antimicrobial Utilization and Resistance (ESPAUR). J. Antimicrob. Chemother. 2013, 68, 2421–2423. [Google Scholar] [CrossRef]
- Nuffield Trust. Antibiotic Prescribing. 2020. Available online: https://www.nuffieldtrust.org.uk/resource/antibiotic-prescribing (accessed on 7 May 2021).
- HM Government. Tackling Antimicrobial Resistance 2019–2024: The UK’s Five-Year National Action Plan; Department of Health and Social Care: London, UK, 2019. Available online: https://www.gov.uk/government/publications/uk-5-year-action-plan-for-antimicrobial-resistance-2019-to-2024 (accessed on 12 February 2021).
- Edwin, P. Strategy for Tackling Antimicrobial Resistance (STAR) 2012–2017; Department of Health, Social Services, and Public Safety: London, UK, 2012. Available online: https://www.health-ni.gov.uk/publications/strategy-and-guidelines-tackling-antimicrobial-resistance (accessed on 12 February 2021).
- Department of Health. Changing the Culture 2019–2024: One Health. In Tackling Antimicrobial Resistance in Northern Ireland: A Five-Year Action Plan; Department of Agriculture, Environment and Rural Afffairs: London, UK, 2019. Available online: https://www.daera-ni.gov.uk/publications/changing-culture-2019-2024-one-health (accessed on 20 February 2021).
- Goossens, H.; Ferech, M.; Vander Stichele, R. Outpatient antibiotic use in Europe and association with resistance: A cross-national database study. Lancet 2005, 365, 579–587. [Google Scholar] [CrossRef]
- Smieszek, T.; Pouwels, K.; Dolk, C.; Smith, D.; Hopkins, S.; Sharland, M.; Hay, A.; Moore, M.; Robotham, J.V. Potential for reducing inappropriate antibiotic prescribing in English primary care. J. Antimicrob. Chemother. 2018, 73, ii36–ii43. [Google Scholar] [CrossRef]
- Wise, J. Antibiotic prescribing is higher in deprived areas of England. BMJ 2015, 351, h6117. [Google Scholar] [CrossRef] [PubMed]
- Covvey, J.R.; Johnson, B.F.; Elliott, V.; Malcolm, W.; Mullen, A.B. An association between socioeconomic deprivation and primary care antibiotic prescribing in Scotland. Antimicrob. Chemother. 2014, 69, 835–841. [Google Scholar] [CrossRef] [PubMed]
- Butler, C.C.; Dunstan, F.; Heginbothom, M.; Mason, B.; Roberts, Z.; Hillier, S.; Howe, R.; Palmer, S.; Howard, A. Containing antibiotic resistance: Decreased antibiotic-resistant coliform urinary tract infections with reduction in antibiotic prescribing by general practices. Br. J. Gen. Pract. 2007, 57, 785–792. [Google Scholar]
- Bucholc, M.; O’Kane, M.; Ashe, S.; Wong-Lin, K. Prescriptive variability of drugs by general practitioners. PLoS ONE 2018, 13, e0189599. [Google Scholar] [CrossRef]
- Curtis, H.J.; Walker, A.J.; Mahtani, K.R.; Goldacre, B. Time trends and geographical variation in prescribing of antibiotics in England 1998–2017. J. Antimicrob. Chemother. 2019, 74, 242–250. [Google Scholar] [CrossRef] [PubMed]
- Kozyrskyj, A.L.; Dahl, M.E.; Chateau, D.G.; Mazowita, G.B.; Klassen, T.P.; Law, B.J. Evidence-based prescribing of antibiotics for children: Role of socioeconomic status and physician characteristics. CMAJ 2004, 171, 139–145. [Google Scholar] [CrossRef]
- Mousquès, J.; Renaud, T.; Scemama, O. Is the “practice style” hypothesis relevant for general practitioners? An analysis of antibiotics prescription for acute rhinopharyngitis. Soc. Sci. Med. 2010, 70, 1176–1184. [Google Scholar] [CrossRef]
- Wang, K.Y.; Seed, P.; Schofield, P.; Ibrahim, S.; Ashworth, M. Which practices are high antibiotic prescribers? A cross-sectional analysis. Br. J. Gen. Pract. 2009, 59, e315–e320. [Google Scholar] [CrossRef]
- Fernández-Álvarez, I.; Zapata-Cachafeiro, M.; Vázquez-Lago, J.; López-Vázquez, P.; Piñeiro-Lamas, M.; Rodríguez, R.G.; Figueiras, A. Pharmaceutical companies information and antibiotic prescription patterns: A follow-up study in Spanish primary care. PLoS ONE 2019, 14, e0221326. [Google Scholar] [CrossRef] [PubMed]
- HSC Business Services Organisation. Prescribing by GP Practice. Available online: http://www.hscbusiness.hscni.net/services/2471.htm (accessed on 20 January 2021).
- Northern Ireland Statistics and Research Agency. Northern Ireland Multiple Deprivation Measures 2017. 2019. Available online: https://www.nisra.gov.uk/publications/nimdm17-results (accessed on 22 January 2021).
- Northern Ireland Statistics and Research Agency. 2017 Mid Year Population Estimates for Northern Ireland. 2018. Available online: https://www.nisra.gov.uk/publications/2017-mid-year-population-estimates-northern-ireland (accessed on 28 January 2021).
- Northern Ireland Statistics and Research Agency. Urban-Rural Geography Documents (2015). 2017. Available online: https://www.nisra.gov.uk/publications/urban-rural-geography-documents-2015 (accessed on 28 January 2021).
- HSC Business Services Organisation. General Medical Services Statistics. 2020. Available online: https://hscbusiness.hscni.net/services/3174.htm (accessed on 12 February 2021).
- HSC Business Services Organisation. Available online: https://data.nicva.org/dataset/gp-practices (accessed on 12 February 2021).
- Goldstein, H. Multilevel Statistical Models; John Wiley & Sons: Hoboken, NJ, USA, 2011. [Google Scholar]
- Wagenmakers, E.J.; Farrell, S. AIC model selection using Akaike weights. Psychon. Bull. Rev. 2004, 11, 192–196. [Google Scholar] [CrossRef]
- Department of Health. Appendix A: COVID-19 Impacts on HSC Services, Excluding Secondary Care. 2020. Available online: https://www.health-ni.gov.uk/sites/default/files/publications/health/appendix-a.pdf (accessed on 7 December 2021).
- Girvin, B.; Hsia, Y.; Turner, W. Antimicrobial stewardship in Northern Ireland during COVID-19. Prescriber 2021, 32, 15–20. [Google Scholar] [CrossRef]
- Thomson, K.; Berry, R.; Robinson, T.; Brown, H.; Bambra, C.; Todd, A. An examination of trends in antibiotic prescribing in primary care and the association with area-level deprivation in England. BMC Public Health 2020, 20, 1148. [Google Scholar] [CrossRef]
- Frazer, J.S.; Frazer, G.R. GP prescribing in Northern Ireland by deprivation index: Retrospective analysis. Fam. Med. Community Health 2020, 8, e000376. [Google Scholar] [CrossRef] [PubMed]
- Yao, Q.; Liu, C.; Ferrier, J.A.; Sun, J. Urban-rural inequality regarding drug prescriptions in primary care facilities—A pre-post comparison of the National Essential Medicines Scheme of China. Int. J. Equity Health 2015, 14, 58. [Google Scholar] [CrossRef]
- Ironmonger, D.; Edeghere, O.; Verlander, N.Q.; Gossain, S.; Hopkins, S.; Hilton, B.; Hawkey, P.M. Effect of general practice characteristics and antibiotic prescribing on Escherichia coli antibiotic non-susceptibility in the West Midlands region of England: A 4 year ecological study. J. Antimicrob. Chemother. 2018, 73, 787–794. [Google Scholar] [CrossRef] [PubMed]
- Clark, A.W.; Durkin, M.J.; Olsen, M.A.; Keller, M.; Ma, Y.; O’Neil, C.A.; Butler, A.M. Rural–urban differences in antibiotic prescribing for uncomplicated urinary tract infection. Infect. Control Hosp. Epidemiol. 2021, 2021, 1437–1444. [Google Scholar] [CrossRef] [PubMed]
- de Jong, J.; Bos, J.H.; de Vries, T.W.; de Jong-van den Berg, L.T. Use of antibiotics in rural and urban regions in The Netherlands: An observational drug utilization study. BMC Public Health 2014, 14, 677. [Google Scholar] [CrossRef] [PubMed]
- Dyar, O.J.; Yang, D.; Yin, J. Variations in antibiotic prescribing among village doctors in a rural region of Shandong province, China: A cross-sectional analysis of prescriptions. BMJ Open 2020, 10, e036703. [Google Scholar] [CrossRef]
- Bou-Antoun, S.; Costelloe, C.; Honeyford, K.; Mazidi, M.; Hayhoe, B.W.J.; Holmes, A.; Johnson, A.P.; Aylin, P. Age-related decline in antibiotic prescribing for uncomplicated respiratory tract infections in primary care in England following the introduction of a national financial incentive (the Quality Premium) for health commissioners to reduce use of antibiotics in the community: An interrupted time series analysis. J. Antimicrob. Chemother. 2018, 73, 2883–2892. [Google Scholar]
- Semenza, J.C.; Suk, J.E.; Tsolova, S. Social determinants of infectious diseases: A public health priority. Eurosurveillance 2010, 15, 19608. [Google Scholar] [CrossRef][Green Version]
- Oz, H.S. Nutrients, Infectious and Inflammatory Diseases. Nutrients 2017, 9, 1085. [Google Scholar] [CrossRef]
- Arcavi, L.; Benowitz, N.L. Cigarette smoking and infection. Arch. Intern. Med. 2004, 164, 2206–2216. [Google Scholar] [CrossRef]
- Buckley, B.; Henschke, N.; Bergman, H.; Skidmore, B.; Klemm, E.; Villanueva, G.; Garritty, C.; Paul, M. Impact of vaccination on antibiotic usage: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2019, 25, 1213–1225. [Google Scholar] [CrossRef] [PubMed]
- Health and Social Care Board and Public Health Agency. The Northern Ireland Management of Infection Guidelines for Primary and Community Care. Available online: https://viewer.microguide.global/guide/1000000198 (accessed on 10 August 2021).
- Department of Health Northern Ireland. The Pharmaceutical Clinical Effectiveness Programme. Available online: https://www.health-ni.gov.uk/articles/pharmaceutical-clinical-effectiveness-programme (accessed on 10 August 2021).



{kind=link}
{kind=link}
| Year | Prescriptions | % Change in Prescriptions | Registered Patients | % Change in Registered Patients |
|---|---|---|---|---|
| 2014 | 1,564,707 | - | 1,855,949 | - |
| 2015 | 1,536,909 | −1.8 | 1,873,675 | 1.0 |
| 2016 | 1,562,211 | 1.6 | 1,902,438 | 1.5 |
| 2017 | 1,485,830 | 4.9 | 1,926,107 | 1.2 |
| 2018 | 1,438,796 | −3.2 | 1,953,334 | 1.4 |
| 2019 | 1,421,520 | −1.2 | 1,982,733 | 1.5 |
| 2020 | 1,155,323 | −18.7 | 1,999,095 | 0.8 |
| Total | 10,165,296 |
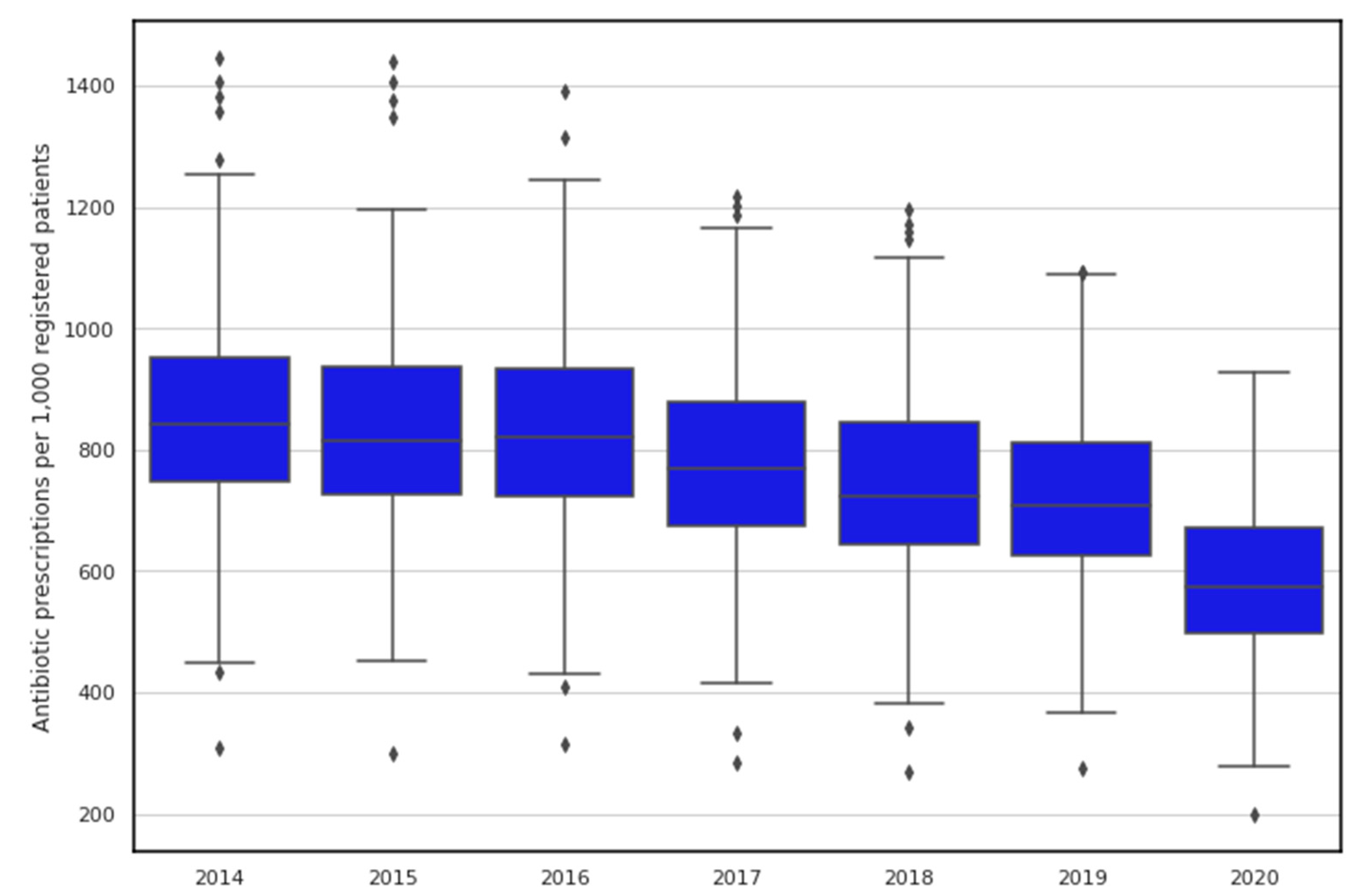
| 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | |
|---|---|---|---|---|---|---|---|
| median (IQR) | 843.1 (746.3–952.2) | 816.0 (727.1–936.2) | 819.8 (724.4–933.7) | 768.7 (674.5–877.3) | 723.5 (643.8–844.3) | 709.1 (624.6–811.1) | 573.0 (498.4–670.3) |
| min | 308.6 | 297.9 | 313.4 | 282.8 | 269.6 | 275.4 | 199.2 |
| max | 1444.8 | 1439.6 | 1391.9 | 1217.5 | 1194.3 | 1092.1 | 926.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Devine, P.; O’Kane, M.; Bucholc, M. Trends, Variation, and Factors Influencing Antibiotic Prescribing: A Longitudinal Study in Primary Care Using a Multilevel Modelling Approach. Antibiotics 2022, 11, 17. https://doi.org/10.3390/antibiotics11010017
Devine P, O’Kane M, Bucholc M. Trends, Variation, and Factors Influencing Antibiotic Prescribing: A Longitudinal Study in Primary Care Using a Multilevel Modelling Approach. Antibiotics. 2022; 11(1):17. https://doi.org/10.3390/antibiotics11010017
Chicago/Turabian StyleDevine, Peter, Maurice O’Kane, and Magda Bucholc. 2022. "Trends, Variation, and Factors Influencing Antibiotic Prescribing: A Longitudinal Study in Primary Care Using a Multilevel Modelling Approach" Antibiotics 11, no. 1: 17. https://doi.org/10.3390/antibiotics11010017
APA StyleDevine, P., O’Kane, M., & Bucholc, M. (2022). Trends, Variation, and Factors Influencing Antibiotic Prescribing: A Longitudinal Study in Primary Care Using a Multilevel Modelling Approach. Antibiotics, 11(1), 17. https://doi.org/10.3390/antibiotics11010017