
Reservoir of Antibiotic Residues and Resistant Coagulase Negative Staphylococci in a Healthy Population in the Greater Accra Region, Ghana

 ,
,  ,
, 
Abstract
:1. Introduction
2. Results
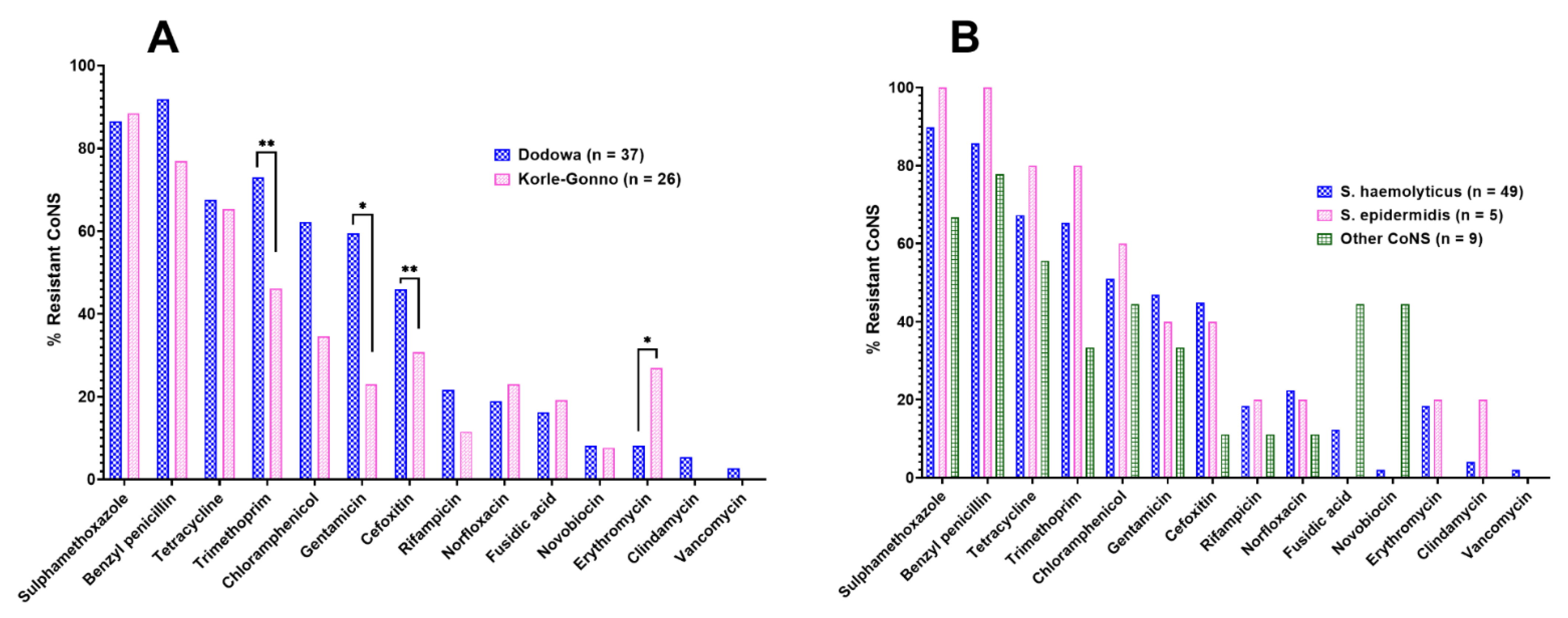
2.1. Microbiological Assay
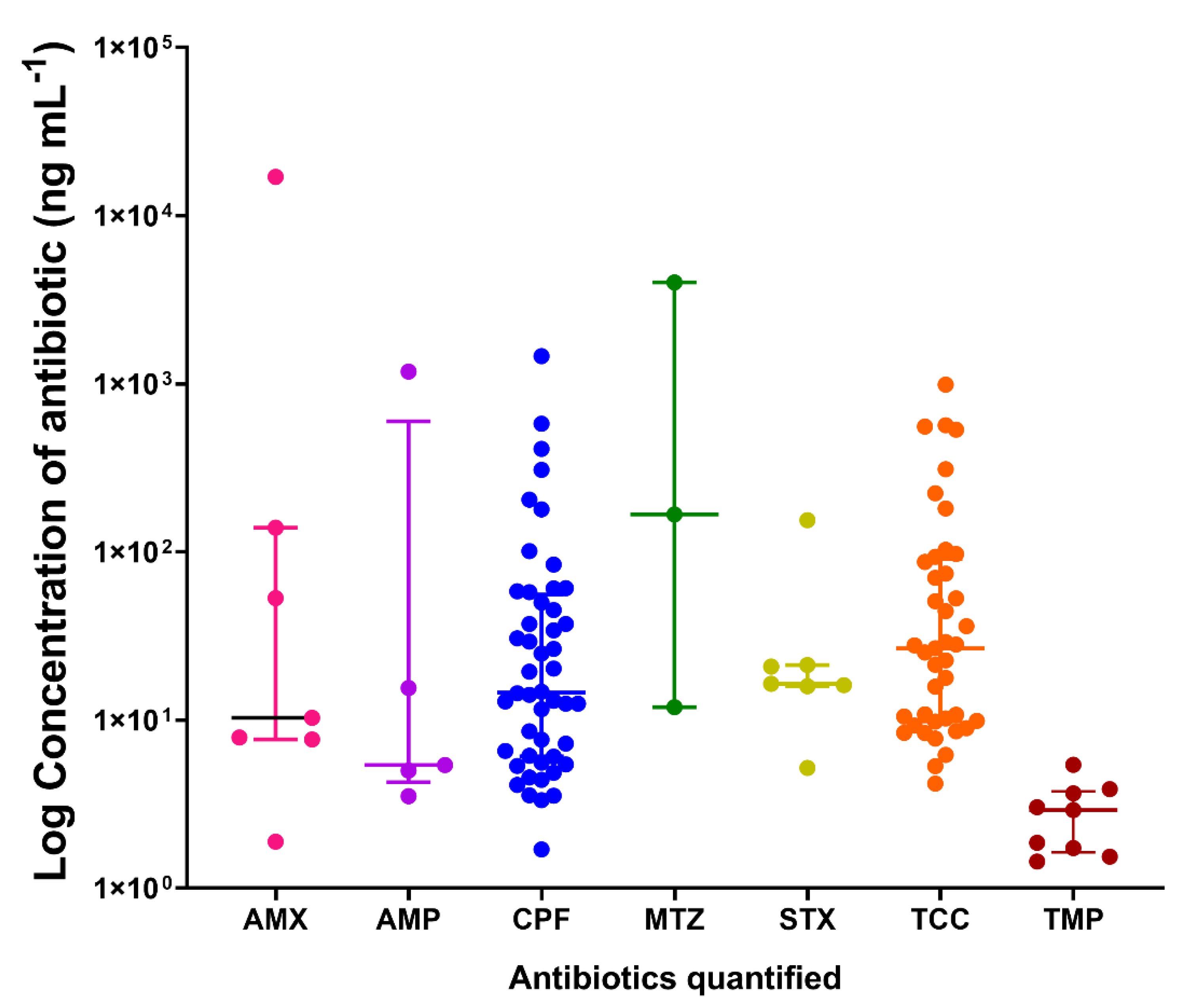
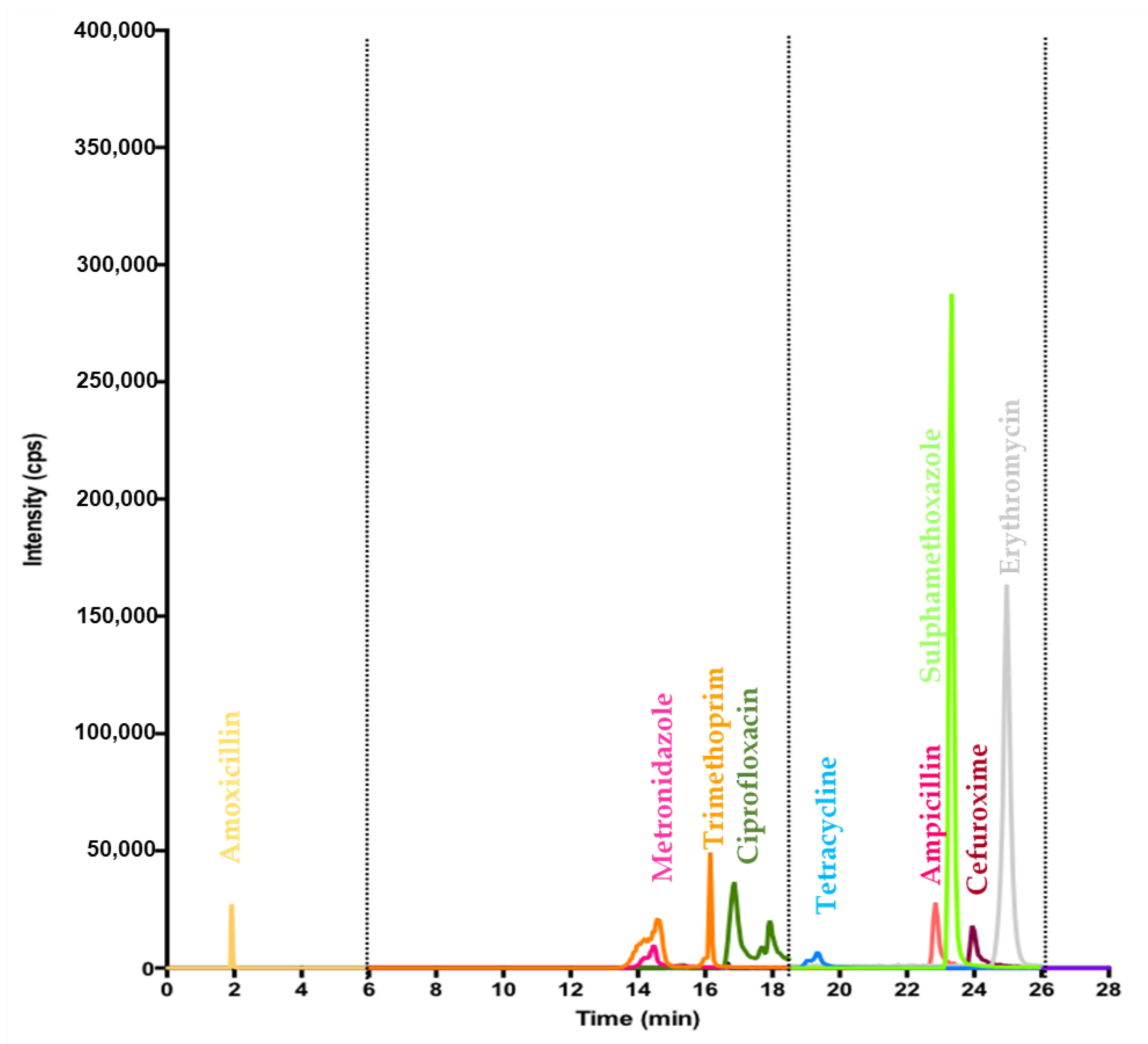
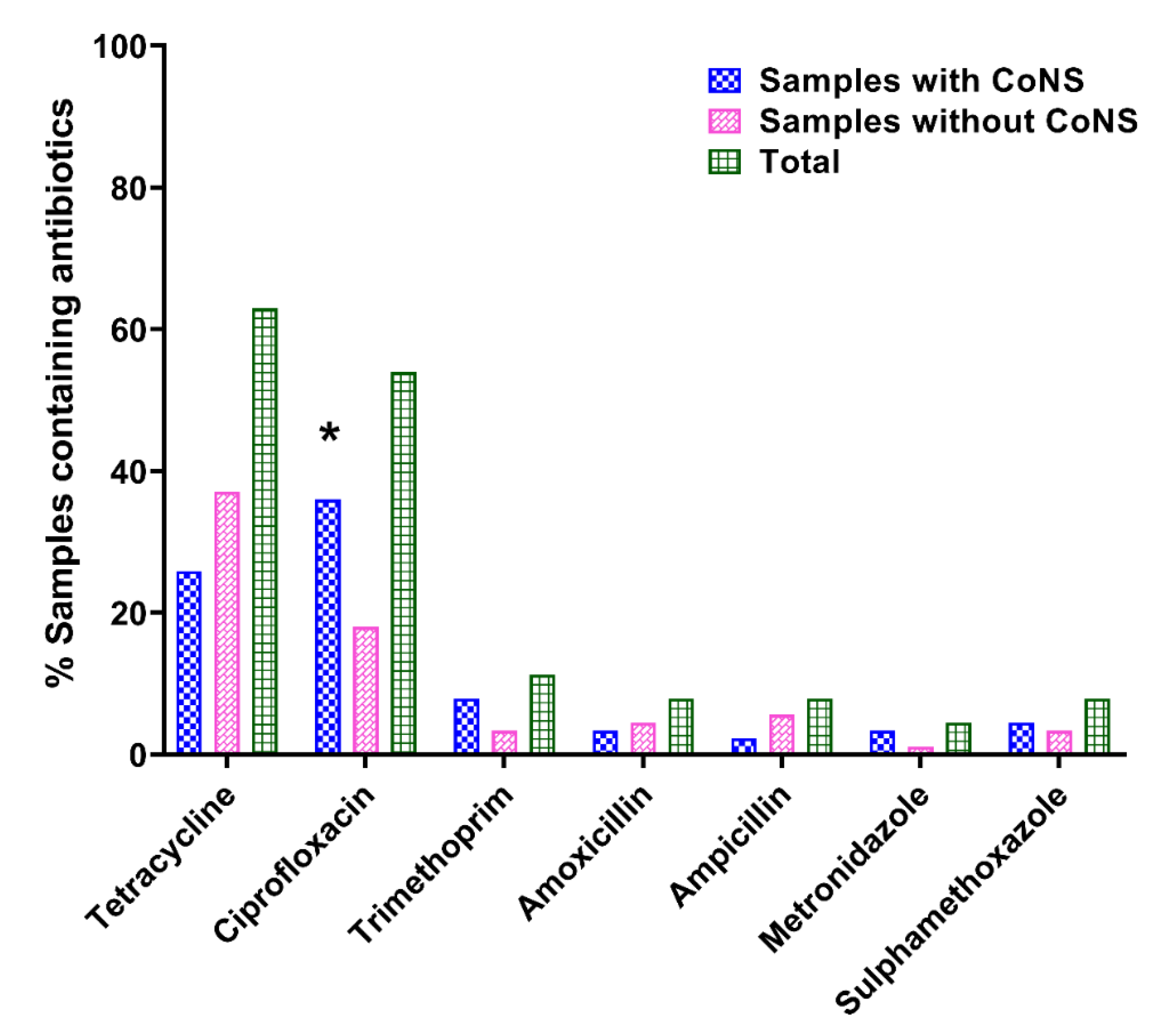
2.2. Pharmaceutical Analysis
3. Discussion
3.1. Identified CoNS Isolates and Their Resistance to Antibiotics
3.2. Antibiotics in Urine Samples
4. Materials and Methods
4.1. Sampling Sites
4.2. Participant Screening and Sample Collection
4.3. Microbiological Assay
4.3.1. Urine Sample Screening, and CoNS Isolation and Identification
4.3.2. Antimicrobial Susceptibility Testing
4.4. Analysis of Antibiotic Residues in Urine Samples
4.4.1. Reagents and Chemicals
4.4.2. Preparation of Standard Solutions and Mobile Phases
4.4.3. Sample Preparation and Clean-Up
4.4.4. Chromatographic Conditions
4.4.5. Development and Validation of the LC-MS/MS Method
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Finch, R. Innovation—Drugs and diagnostics. J. Antimicrob. Chemother. 2007, 60, i79–i82. [Google Scholar] [CrossRef]
- GBD-Collaborators Global Burden of Disease. Available online: https://www.thelancet.com/gbd (accessed on 17 July 2020).
- WHO. World Health Statistics 2009; World Health Organization: Geneve, Switzerland, 2009. [Google Scholar]
- Van Boeckel, T.P.; Gandra, S.; Ashok, A.; Caudron, Q.; Grenfell, B.T.; Levin, S.A.; Laxminarayan, R. Global antibiotic consumption 2000 to 2010: An analysis of national pharmaceutical sales data. Lancet Infect. Dis. 2014, 14, 742–750. [Google Scholar] [CrossRef]
- Okeke, I.N.; Laxminarayan, R.; Bhutta, Z.A.; Duse, A.G.; Jenkins, P.; O’Brien, T.F.; Pablos-Mendez, A.; Klugman, K.P. Antimicrobial resistance in developing countries. Part I: Recent trends and current status. Lancet Infect. Dis. 2005, 5, 481–493. [Google Scholar] [CrossRef]
- Laxminarayan, R.; Heymann, D.L. Challenges of drug resistance in the developing world. BMJ Br. Med. J. 2012, 344, e1567. [Google Scholar] [CrossRef] [Green Version]
- Zaidi, A.K.; Huskins, W.C.; Thaver, D.; Bhutta, Z.A.; Abbas, Z.; Goldmann, D.A. Hospital-acquired neonatal infections in developing countries. Lancet 2005, 365, 1175–1188. [Google Scholar] [CrossRef]
- Bekoe, S.O.; Ahiabu, M.A.; Orman, E.; Tersbøl, B.P.; Adosraku, R.K.; Hansen, M.; Frimodt-Moller, N.; Styrishave, B. Exposure of consumers to substandard antibiotics from selected authorised and unauthorised medicine sales outlets in Ghana. Trop. Med. Int. Health 2020, 25, 962–975. [Google Scholar] [CrossRef]
- Darko, G.; Borquaye, L.S.; Acheampong, A.; Oppong, K.; Bernardino, R. Veterinary antibiotics in dairy products from Kumasi, Ghana. Cogent Chem. 2017, 3, 1343636. [Google Scholar] [CrossRef]
- Bogusz, M.J.; Hassan, H.; Al-Enazi, E.; Ibrahim, Z.; Al-Tufail, M. Application of LC-ESI-MS-MS for detection of synthetic adulterants in herbal remedies. J. Pharm. Biomed. Anal. 2006, 41, 554–564. [Google Scholar] [CrossRef] [PubMed]
- Morgenstern, M.; Erichsen, C.; Hackl, S.; Mily, J.; Militz, M.; Friederichs, J.; Hungerer, S.; Bühren, V.; Moriarty, T.F.; Post, V.; et al. Antibiotic resistance of commensal Staphylococcus aureus and coagulase-negative staphylococci in an international cohort of surgeons: A prospective point-prevalence study. PLoS ONE 2016, 11, e0148437. [Google Scholar] [CrossRef] [PubMed]
- Parlet, C.P.; Brown, M.M.; Horswill, A.R. Commensal staphylococci influence Staphylococcus aureus skin colonization and Disease. Trends Microbiol. 2019, 27, 497–507. [Google Scholar] [CrossRef] [PubMed]
- Fowoyo, P.T.; Ogunbanwo, S.T. Antimicrobial resistance in coagulase-negative staphylococci from Nigerian traditional fermented foods. Ann. Clin. Microbiol. Antimicrob. 2017, 16, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Lerbech, A.M.; Opintan, J.A.; Bekoe, S.O.; Ahiabu, M.A.; Tersbøl, B.P.; Hansen, M.; Brightson, K.T.C.; Ametepeh, S.; Frimodt-Møller, N.; Styrishave, B. Antibiotic exposure in a low-income country: Screening urine samples for presence of antibiotics and antibiotic resistance in coagulase negative staphylococcal contaminants. PLoS ONE 2014, 9, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Long, S.S.; Prober, C.G.; Fischer, M. Principles and Practice of Pediatric Infectious Diseases E-Book; Elsevier Health Sciences: Philadelphia, PA, USA, 2017; ISBN 0323461328. [Google Scholar]
- Bennett, J.E.; Dolin, R.; Blaser, M.J. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases E-Book; Elsevier Health Sciences: Philadelphia, PA, USA, 2019; ISBN 0323550274. [Google Scholar]
- Huebner, J.; Goldmann, D.A. Coagulase-negative staphylococci: Role as pathogens. Annu. Rev. Med. 1999, 50, 223–236. [Google Scholar] [CrossRef] [PubMed]
- Asante, J.; Amoako, D.G.; Abia, A.L.K.; Somboro, A.M.; Govinden, U.; Bester, L.A.; Essack, S.Y. Review of clinically and epidemiologically relevant coagulase-negative staphylococci in Africa. Microb. Drug Resist. 2020, 26, 951–970. [Google Scholar] [CrossRef] [Green Version]
- John, J.F.; Harvin, A.M. History and evolution of antibiotic resistance in coagulase-negative staphylococci: Susceptibility profiles of new anti-staphylococcal agents. Ther. Clin. Risk Manag. 2007, 3, 1143. [Google Scholar]
- Azanu, D.; Styrishave, B.; Darko, G.; Weisser, J.J.; Abaidoo, R.C. Occurrence and risk assessment of antibiotics in water and lettuce in Ghana. Sci. Total Environ. 2018, 622–623, 293–305. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Zhang, X.; Li, Y.; Gao, H.; Ling, P.; Li, X.; Chen, Q.; Ma, A.; Shao, H.; Li, M.; et al. Simultaneous screening and determination of eight tetracycline antibiotics illegally adulterated in herbal preparations using HPLC–DAD combined with LC–MS–MS. Chromatographia 2018, 81, 303–314. [Google Scholar] [CrossRef]
- Wang, Y.; Kuo, S.; Shu, M.; Yu, J.; Huang, S.; Dai, A.; Two, A.; Gallo, R.L.; Huang, C.-M. Staphylococcus epidermidis in the human skin microbiome mediates fermentation to inhibit the growth of Propionibacterium acnes: Implications of probiotics in acne vulgaris. Appl. Microbiol. Biotechnol. 2014, 98, 411–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Otto, M. Staphylococcus epidermidis—The “accidental” pathogen. Nat. Rev. Microbiol. 2009, 7, 555–567. [Google Scholar] [CrossRef] [Green Version]
- De Allori, M.C.G.; Jure, M.Á.; Romero, C.; De Castillo, M.E.C. Antimicrobial resistance and production of biofilms in clinical isolates of coagulase-negative Staphylococcus strains. Biol. Pharm. Bull. 2006, 29, 1592–1596. [Google Scholar] [CrossRef] [Green Version]
- Newman, M.J.; Frimpong, E.; Donkor, E.S.; Opintan, J.A.; Asamoah-Adu, A. Resistance to antimicrobial drugs in Ghana. Infect. Drug Resist. 2011, 4, 215. [Google Scholar] [CrossRef] [Green Version]
- Afari-Asiedu, S.; Kinsman, J.; Boamah-Kaali, E.; Abdulai, M.A.; Gyapong, M.; Sankoh, O.; Hulscher, M.; Asante, K.P.; Wertheim, H. To sell or not to sell; The differences between regulatory and community demands regarding access to antibiotics in rural Ghana. J. Pharm. Policy Pract. 2018, 11, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaplan, W.; Laing, R. Priority Medicines for Europe and the World; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Xu, M.; Huang, B.; Gao, F.; Zhai, C.; Yang, Y.; Li, L.; Wang, W.; Shi, L. Assessment of adulterated traditional Chinese medicines in China: 2003–2017. Front. Pharmacol. 2019, 10, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Li, F.F.; Guo, C.C.; Zhang, Y.L.; Wang, N.; Shi, Y.; Wang, S.Q. A screening method based on 1D CSSF-TOCSY for the identification and quantification of 11 illegal adulterants in herbal medicines. Microchem. J. 2020, 153, 104495. [Google Scholar] [CrossRef]
- FDA Products Recall and Alert. Available online: http://www.fdaghana.gov.gh/recall-products.php (accessed on 13 January 2021).
- Van Boeckel, T.P.; Brower, C.; Gilbert, M.; Grenfell, B.T.; Levin, S.A.; Robinson, T.P.; Teillant, A.; Laxminarayan, R. Global trends in antimicrobial use in food animals. Proc. Natl. Acad. Sci. USA 2015, 112, 5649–5654. [Google Scholar] [CrossRef] [Green Version]
- Caudell, M.A.; Dorado-Garcia, A.; Eckford, S.; Creese, C.; Byarugaba, D.K.; Afakye, K.; Chansa-Kabali, T.; Fasina, F.O.; Kabali, E.; Kiambi, S.; et al. Towards a bottom-up understanding of antimicrobial use and resistance on the farm: A knowledge, attitudes, and practices survey across livestock systems in five African countries. PLoS ONE 2020, 15, e0220274. [Google Scholar] [CrossRef] [Green Version]
- Donkor, E.S.; Newman, M.J.; Yeboah-Manu, D. Epidemiological aspects of non-human antibiotic usage and resistance: Implications for the control of antibiotic resistance in Ghana. Trop. Med. Int. Health 2012, 17, 462–468. [Google Scholar] [CrossRef] [PubMed]
- Cañada-Cañada, F.; Muñoz De La Peña, A.; Espinosa-Mansilla, A. Analysis of antibiotics in fish samples. Anal. Bioanal. Chem. 2009, 395, 987–1008. [Google Scholar] [CrossRef]
- Agoba, E.E.; Adu, F.; Agyare, C.; Boamah, V.E. Antibiotic use and practices in selected fish farms in the Ashanti region of Ghana. J. Infect. Dis. Treat. 2017, 3, 1093–2472. [Google Scholar] [CrossRef] [Green Version]
- Donkor, E.S.; Anim-Baidoo, I.; Fei, E.; Amponsah, C.; Olu-Taiwo, M.; Nana-Adjei, D.; Owusu, E.; Forson, A.O. Occurrence of antibiotic residues and antibiotic-resistant bacteria in Nile tilapia sold in Accra, Ghana: Public health implications. J. Food Res. 2018, 7, 129–137. [Google Scholar] [CrossRef]
- Donkor, E.S.; Newman, M.J.; Tay, S.C.K.; Dayie, N.T.K.D.; Bannerman, E.; Olu-Taiwo, M. Investigation into the risk of exposure to antibiotic residues contaminating meat and egg in Ghana. Food Control. 2011, 22, 869–873. [Google Scholar] [CrossRef]
- EUCAST Breakpoint Tables for Interpretation of MICs and Zone Diameters Version 10.0. Available online: https://eucast.org/clinical_breakpoints/. (accessed on 17 July 2020).
- Gullberg, E.; Cao, S.; Berg, O.G.; Ilbäck, C.; Sandegren, L.; Hughes, D.; Andersson, D.I. Selection of Resistant Bacteria at Very Low Antibiotic Concentrations. PloS Pathog. 2011, 7, e1002158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blom, M.; Sørensen, T.L.; Espersen, F.; Frimodt-Møller, N. Validation of FLEXICULTTM SSI-urinary kit for use in the primary health care setting. Scand. J. Infect. Dis. 2002, 34, 430–435. [Google Scholar] [CrossRef]
- Kouri, T.; Fogazzi, G.; Gant, V.; Hallander, H.; Hofmann, W.; Guder, W.G. European Urinalysis Guidelines. Scand. J. Clin. Lab. Invest. 2000, 60, 1–96. [Google Scholar] [CrossRef]
- EUCAST Clinical Breakpoints—Breakpoints and Guidance. Available online: https://www.eucast.org/clinical_breakpoints/ (accessed on 17 July 2020).
- Bekoe, S.O.; Orman, E.; Asare-Nkansah, S.; Sørensen, A.M.L.; Björklund, E.; Adosraku, R.K.; Hansen, M.; Styrishave, B. Detection and quantification of antibiotic residues in urine samples of healthy individuals from rural and urban communities in Ghana using a validated SPE-LC-MS/MS method. SN Appl. Sci. 2020, 2, 1–11. [Google Scholar] [CrossRef]
- Bekoe, S.O.; Bak, S.A.; Björklund, E.; Krogh, K.A.; Okine, N.N.A.; Adosraku, R.K.; Styrishave, B.; Hansen, M. Determination of thirteen antibiotics in drug products-A new LC-MS/MS tool for screening drug product quality. Anal. Methods 2014, 6, 5847–5855. [Google Scholar] [CrossRef]
- ICH Bioanalytical Method Validation—M10. 2019. Available online: https://www.wrib.org/PDFs/ICH_M10_BMV_Draft_Guideline-190227.pdf (accessed on 5 March 2020).



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Species | Community | Resistance to ≥4 Antibiotics (MDR CoNS) | Resistance to <4 Antibiotics (Non-MDR CoNS) | Total (%) |
|---|---|---|---|---|
| S. haemolyticus | Dodowa | 24 (68.6) | 4 (28.6) | 28 (57.1) |
| Korle-Gonno | 11 (31.4) | 10 (71.4) | 21 (42.9) | |
| Sub-Total | 35 (71.4) | 14 (28.6) | 49 (77.8) | |
| S. epidermidis | Dodowa | 3 (75.0) | 1 (100.0) | 4 (80.0) |
| Korle-Gonno | 1 (25.0) | 0 (0.0) | 1 (20.0) | |
| Sub-Total | 4 (80.0) | 1 (20.0) | 5 (7.9) | |
| Other CoNS * | Dodowa | 3 (60.0) | 2 (50.0) | 5 (55.6) |
| Korle-Gonno | 2 (40.0) | 2 (50.0) | 4 (44.4) | |
| Sub-Total | 5 (55.6) | 4 (44.4) | 9 (14.3) | |
| Total | 44 (69.8) | 19 (30.2) | 63 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bekoe, S.O.; Hane-Weijman, S.; Trads, S.L.; Orman, E.; Opintan, J.; Hansen, M.; Frimodt-Møller, N.; Styrishave, B. Reservoir of Antibiotic Residues and Resistant Coagulase Negative Staphylococci in a Healthy Population in the Greater Accra Region, Ghana. Antibiotics 2022, 11, 119. https://doi.org/10.3390/antibiotics11010119
Bekoe SO, Hane-Weijman S, Trads SL, Orman E, Opintan J, Hansen M, Frimodt-Møller N, Styrishave B. Reservoir of Antibiotic Residues and Resistant Coagulase Negative Staphylococci in a Healthy Population in the Greater Accra Region, Ghana. Antibiotics. 2022; 11(1):119. https://doi.org/10.3390/antibiotics11010119
Chicago/Turabian StyleBekoe, Samuel Oppong, Sophie Hane-Weijman, Sofie Louise Trads, Emmanuel Orman, Japheth Opintan, Martin Hansen, Niels Frimodt-Møller, and Bjarne Styrishave. 2022. "Reservoir of Antibiotic Residues and Resistant Coagulase Negative Staphylococci in a Healthy Population in the Greater Accra Region, Ghana" Antibiotics 11, no. 1: 119. https://doi.org/10.3390/antibiotics11010119
APA StyleBekoe, S. O., Hane-Weijman, S., Trads, S. L., Orman, E., Opintan, J., Hansen, M., Frimodt-Møller, N., & Styrishave, B. (2022). Reservoir of Antibiotic Residues and Resistant Coagulase Negative Staphylococci in a Healthy Population in the Greater Accra Region, Ghana. Antibiotics, 11(1), 119. https://doi.org/10.3390/antibiotics11010119