
Intra-Articular Injections Prior to Total Knee Arthroplasty Do Not Increase the Risk of Periprosthetic Joint Infection: A Prospective Cohort Study

 ,
, 

Abstract
1. Introduction
2. Results
3. Discussion
4. Materials and Methods
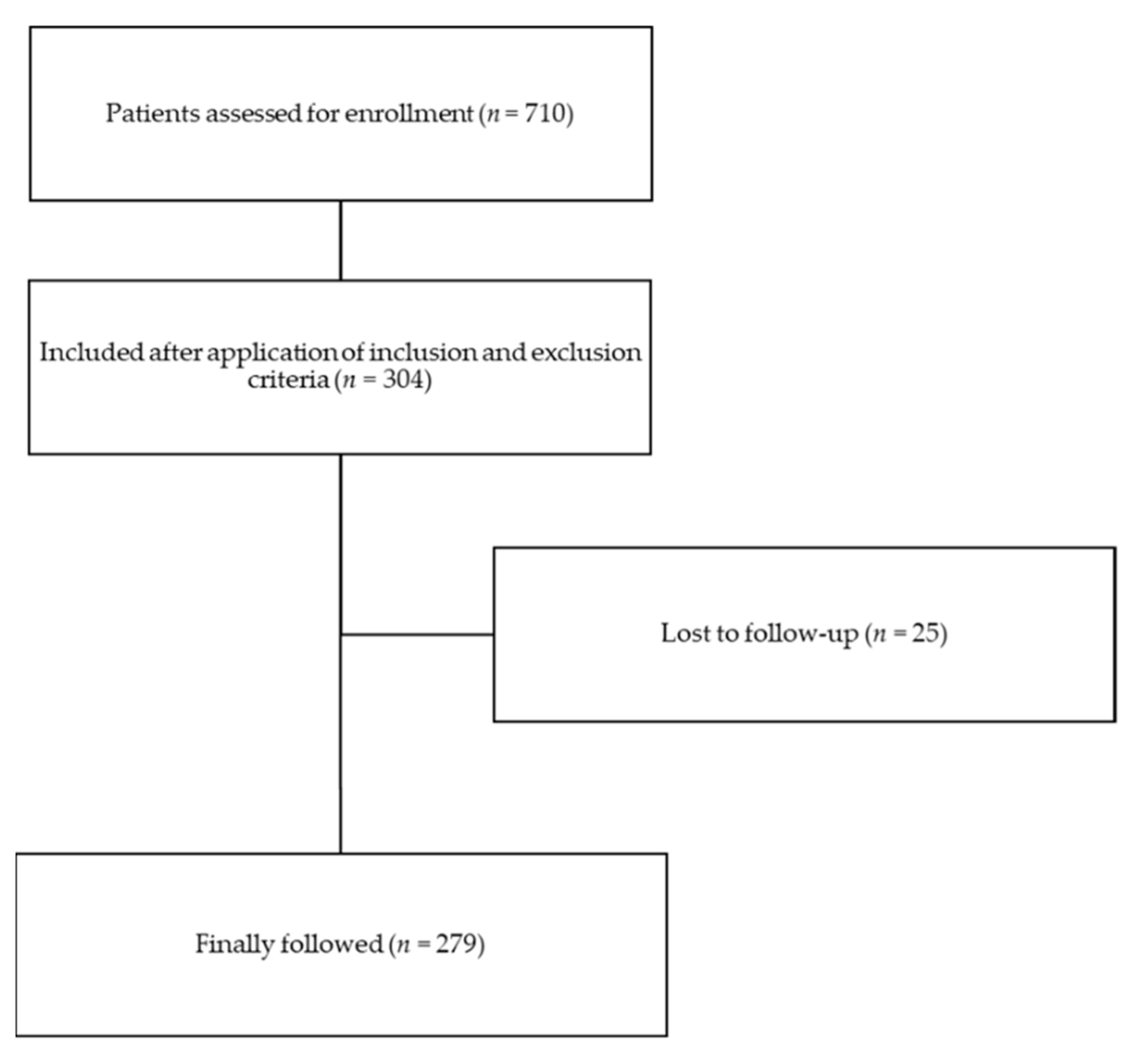
4.1. Participants
4.2. Outcome
4.3. Follow-Up
4.4. Statistical Analyses
4.5. Ethics
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Parvizi, J.; Shohat, N.; Gehrke, T. Prevention of Periprosthetic Joint Infection: New Guidelines. Bone Jt. J. 2017, 99-B, 3–10. [Google Scholar] [CrossRef]
- Kurtz, S.M.; Lau, E.C.; Son, M.-S.; Chang, E.T.; Zimmerli, W.; Parvizi, J. Are We Winning or Losing the Battle With Periprosthetic Joint Infection: Trends in Periprosthetic Joint Infection and Mortality Risk for the Medicare Population. J. Arthroplast. 2018, 33, 3238–3245. [Google Scholar] [CrossRef] [PubMed]
- Hartzler, M.A.; Li, K.; Geary, M.B.; Odum, S.M.; Springer, B.D. Complications in the Treatment of Prosthetic Joint Infection. Bone Jt. J 2020, 102-B, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Perez, S.; Dauchy, F.-A.; Salvo, F.; Quéroué, M.; Durox, H.; Delobel, P.; Chambault, R.; Ade, M.; Cazanave, C.; Desclaux, A.; et al. Severe Adverse Events during Medical and Surgical Treatment of Hip and Knee Prosthetic Joint Infections. Med. Mal. Infect. 2020. [Google Scholar] [CrossRef] [PubMed]
- Lemaignen, A.; Bernard, L.; Marmor, S.; Ferry, T.; Grammatico-Guillon, L.; Astagneau, P. Epidemiology of Complex Bone and Joint Infections in France Using a National Registry: The CRIOAc Network. J. Infect. 2021, 82, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Cahill, J.; Shadbolt, B.; Scarvell, J.; Smith, P. Quality of Life after Infection in Total Joint Replacement. J. Orthop. Surg. 2008, 16, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Mur, I.; Jordán, M.; Rivera, A.; Pomar, V.; González, J.C.; López-Contreras, J.; Crusi, X.; Navarro, F.; Gurguí, M.; Benito, N. Do Prosthetic Joint Infections Worsen the Functional Ambulatory Outcome of Patients with Joint Replacements? A Retrospective Matched Cohort Study. Antibiotics 2020, 9, 872. [Google Scholar] [CrossRef]
- Healthcare-Associated Infections: Surgical Site Infections—Annual Epidemiological Report for 2017. Available online: https://www.ecdc.europa.eu/en/publications-data/healthcare-associated-infections-surgical-site-infections-annual-1 (accessed on 29 January 2021).
- Kurtz, S.M.; Lau, E.; Watson, H.; Schmier, J.K.; Parvizi, J. Economic Burden of Periprosthetic Joint Infection in the United States. J. Arthroplast. 2012, 27, 61–65.e1. [Google Scholar] [CrossRef]
- Richardson, S.S.; Schairer, W.W.; Sculco, T.P.; Sculco, P.K. Comparison of Infection Risk with Corticosteroid or Hyaluronic Acid Injection Prior to Total Knee Arthroplasty. J. Bone Jt. Surg. Am. 2019, 101, 112–118. [Google Scholar] [CrossRef]
- Tande, A.J.; Patel, R. Prosthetic Joint Infection. Clin. Microbiol. Rev. 2014, 27, 302. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Guidelines on the Prevention of Surgical Site Infection. Available online: http://www.who.int/gpsc/ssi-prevention-guidelines/en/ (accessed on 31 January 2021).
- Berríos-Torres, S.I.; Umscheid, C.A.; Bratzler, D.W.; Leas, B.; Stone, E.C.; Kelz, R.R.; Reinke, C.E.; Morgan, S.; Solomkin, J.S.; Mazuski, J.E.; et al. Centers for Disease Control and Prevention Guideline for the Prevention of Surgical Site Infection, 2017. JAMA Surg. 2017, 152, 784. [Google Scholar] [CrossRef]
- Charlesworth, J.; Fitzpatrick, J.; Perera, N.K.P.; Orchard, J. Osteoarthritis-a Systematic Review of Long-Term Safety Implications for Osteoarthritis of the Knee. BMC Musculoskelet. Disord. 2019, 20. [Google Scholar] [CrossRef]
- Caldwell, J.R. Intra-Articular Corticosteroids. Guide to Selection and Indications for Use. Drugs 1996, 52, 507–514. [Google Scholar] [CrossRef]
- Bannuru, R.R.; Osani, M.C.; Vaysbrot, E.E.; Arden, N.K.; Bennell, K.; Bierma-Zeinstra, S.M.A.; Kraus, V.B.; Lohmander, L.S.; Abbott, J.H.; Bhandari, M.; et al. OARSI Guidelines for the Non-Surgical Management of Knee, Hip, and Polyarticular Osteoarthritis. Osteoarthr. Cartil. 2019, 27, 1578–1589. [Google Scholar] [CrossRef]
- Kolasinski, S.L.; Neogi, T.; Hochberg, M.C.; Oatis, C.; Guyatt, G.; Block, J.; Callahan, L.; Copenhaver, C.; Dodge, C.; Felson, D.; et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Care Res. 2020, 72, 149–162. [Google Scholar] [CrossRef] [PubMed]
- Marsland, D.; Mumith, A.; Barlow, I.W. Systematic Review: The Safety of Intra-Articular Corticosteroid Injection Prior to Total Knee Arthroplasty. Knee 2014, 21, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Cancienne, J.M.; Werner, B.C.; Luetkemeyer, L.M.; Browne, J.A. Does Timing of Previous Intra-Articular Steroid Injection Affect the Post-Operative Rate of Infection in Total Knee Arthroplasty? J. Arthroplast. 2015, 30, 1879–1882. [Google Scholar] [CrossRef]
- Bedard, N.A.; Pugely, A.J.; Elkins, J.M.; Duchman, K.R.; Westermann, R.W.; Liu, S.S.; Gao, Y.; Callaghan, J.J. The John N. Insall Award: Do Intraarticular Injections Increase the Risk of Infection After TKA? Clin. Orthop. Relat. Res. 2017, 475, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Joshy, S.; Thomas, B.; Gogi, N.; Modi, A.; Singh, B.K. Effect of Intra-Articular Steroids on Deep Infections Following Total Knee Arthroplasty. Int. Orthop. 2006, 30, 91–93. [Google Scholar] [CrossRef] [PubMed]
- Desai, A.; Ramankutty, S.; Board, T.; Raut, V. Does Intraarticular Steroid Infiltration Increase the Rate of Infection in Subsequent Total Knee Replacements? Knee 2009, 16, 262–264. [Google Scholar] [CrossRef] [PubMed]
- Horne, G.; Devane, P.; Davidson, A.; Adams, K.; Purdie, G. The Influence of Steroid Injections on the Incidence of Infection Following Total Knee Arthroplasty. N. Z. Med. J. 2008, 121, U2896. [Google Scholar] [PubMed]
- Papavasiliou, A.V.; Isaac, D.L.; Marimuthu, R.; Skyrme, A.; Armitage, A. Infection in Knee Replacements after Previous Injection of Intra-Articular Steroid. J. Bone Jt. Surg. Br. 2006, 88, 321–323. [Google Scholar] [CrossRef]
- Amin, N.H.; Omiyi, D.; Kuczynski, B.; Cushner, F.D.; Scuderi, G.R. The Risk of a Deep Infection Associated With Intraarticular Injections Before a Total Knee Arthroplasty. J. Arthroplast. 2016, 31, 240–244. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Jiang, X.; Tian, W. Does Previous Intra-Articular Steroid Injection Increase the Risk of Joint Infection Following Total Hip Arthroplasty or Total Knee Arthroplasty? A Meta-Analysis. Med. Sci. Monit. 2014, 20, 1878–1883. [Google Scholar] [CrossRef]
- Xing, D.; Yang, Y.; Ma, X.; Ma, J.; Ma, B.; Chen, Y. Dose Intraarticular Steroid Injection Increase the Rate of Infection in Subsequent Arthroplasty: Grading the Evidence through a Meta-Analysis. J. Orthop. Surg. Res. 2014, 9. [Google Scholar] [CrossRef]
- Pereira, L.C.; Kerr, J.; Jolles, B.M. Intra-Articular Steroid Injection for Osteoarthritis of the Hip Prior to Total Hip Arthroplasty: Is It Safe? A Systematic Review. Bone Jt. J. 2016, 98-B, 1027–1035. [Google Scholar] [CrossRef] [PubMed]
- Lenguerrand, E.; Whitehouse, M.R.; Beswick, A.D.; Kunutsor, S.K.; Foguet, P.; Porter, M.; Blom, A.W. Risk Factors Associated with Revision for Prosthetic Joint Infection Following Knee Replacement: An Observational Cohort Study from England and Wales. Lancet Infect. Dis. 2019, 19, 589–600. [Google Scholar] [CrossRef]
- Kapadia, B.H.; Berg, R.A.; Daley, J.A.; Fritz, J.; Bhave, A.; Mont, M.A. Periprosthetic Joint Infection. Lancet 2016, 387, 386–394. [Google Scholar] [CrossRef]
- Sadr Azodi, O.; Bellocco, R.; Eriksson, K.; Adami, J. The Impact of Tobacco Use and Body Mass Index on the Length of Stay in Hospital and the Risk of Post-Operative Complications among Patients Undergoing Total Hip Replacement. J. Bone Jt. Surg. Br. 2006, 88, 1316–1320. [Google Scholar] [CrossRef]
- Cizmic, Z.; Feng, J.E.; Huang, R.; Iorio, R.; Komnos, G.; Kunutsor, S.K.; Metwaly, R.G.; Saleh, U.H.; Sheth, N.; Sloan, M. Hip and Knee Section, Prevention, Host Related: Proceedings of International Consensus on Orthopedic Infections. J. Arthroplast. 2019, 34, S255–S270. [Google Scholar] [CrossRef]
- Kaspar, S.; de V de Beer, J. Infection in Hip Arthroplasty after Previous Injection of Steroid. J. Bone Jt. Surg. Br. 2005, 87, 454–457. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, S.M.; Ong, K.L.; Lau, E.; Bozic, K.J.; Berry, D.; Parvizi, J. Prosthetic Joint Infection Risk after TKA in the Medicare Population. Clin. Orthop. Relat. Res. 2010, 468, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Hox, J.J.; De Leeuw, E.D. A Comparison of Nonresponse in Mail, Telephone, and Face-to-Face Surveys. Qual. Quant. 1994, 28, 329–344. [Google Scholar] [CrossRef]
- Sinclair, M.; O’Toole, J.; Malawaraarachchi, M.; Leder, K. Comparison of Response Rates and Cost-Effectiveness for a Community-Based Survey: Postal, Internet and Telephone Modes with Generic or Personalised Recruitment Approaches. BMC Med. Res. Methodol. 2012, 12, 132. [Google Scholar] [CrossRef]
- Feveile, H.; Olsen, O.; Hogh, A. A Randomized Trial of Mailed Questionnaires versus Telephone Interviews: Response Patterns in a Survey. BMC Med. Res. Methodol. 2007, 7, 27. [Google Scholar] [CrossRef] [PubMed]
- Gwam, C.U.; Mohamed, N.S.; Dávila Castrodad, I.M.; George, N.E.; Remily, E.A.; Wilkie, W.A.; Barg, V.; Gbadamosi, W.A.; Delanois, R.E. Factors Associated with Non-Home Discharge after Total Knee Arthroplasty: Potential for Cost Savings? Knee 2020, 27, 1176–1181. [Google Scholar] [CrossRef]
- Localio, A.R.; Berlin, J.A.; Ten Have, T.R.; Kimmel, S.E. Adjustments for Center in Multicenter Studies: An Overview. Ann. Intern. Med. 2001, 135, 112–123. [Google Scholar] [CrossRef] [PubMed]
- Pellegrini, A.; Legnani, C.; Meani, E. A New Perspective on Current Prosthetic Joint Infection Classifications: Introducing Topography as a Key Factor Affecting Treatment Strategy. Arch. Orthop. Trauma Surg. 2019, 139, 317–322. [Google Scholar] [CrossRef] [PubMed]
- Parvizi, J.; Gehrke, T.; Chen, A.F. Proceedings of the International Consensus on Periprosthetic Joint Infection. Bone Jt. J. 2013, 95-B, 1450–1452. [Google Scholar] [CrossRef] [PubMed]
- Shohat, N.; Bauer, T.; Buttaro, M.; Budhiparama, N.; Cashman, J.; Della Valle, C.J.; Drago, L.; Gehrke, T.; Marcelino Gomes, L.S.; Goswami, K.; et al. Hip and Knee Section, What Is the Definition of a Periprosthetic Joint Infection (PJI) of the Knee and the Hip? Can the Same Criteria Be Used for Both Joints?: Proceedings of International Consensus on Orthopedic Infections. J. Arthroplast. 2019, 34, S325–S327. [Google Scholar] [CrossRef]
- Zimmerli, W.; Trampuz, A.; Ochsner, P.E. Prosthetic-Joint Infections. N. Engl. J. Med. 2004, 351, 1645–1654. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Patients (n = 304) |
|---|---|
| Mean age, years ± SD | 71.8 ± 8.9 |
| [min–max] | [31–91] |
| Sex: | |
| -Female, n (%) | 220 (72.4) |
| -Male, n (%) | 84 (27.6) |
| Mean weight, kg ± SD | 82.0 ± 16.3 |
| [min–max] | [46–149] |
| Mean height, cm ± SD | 162.9 ± 9.3 |
| [min–max] | [136–190] |
| Mean BMI, kg/m2 ± SD | 30.9 ± 5.3 |
| [min–max] | [19.4–47.6] |
| Diabetes mellitus: | |
| -Type 1, n (%) | 7 (2.3) |
| -Type 2, n (%) | 43 (14.1) |
| -None, n (%) | 254 (83.6) |
| Smoking: | |
| -Active, n (%) | 14 (4.6) |
| -Cessation, n (%) | 49 (16.1) |
| -None, n (%) | 241 (79.3) |
| Alcoholism: | |
| -Active, n (%) | 23 (7.5) |
| -Cessation, n (%) | 5 (1.7) |
| -None, n (%) | 276 (90.8) |
| Mean ASA Score, mean ± SD | 2.3 ± 0.6 |
| [min–max] | [1–4] |
| Prior IA injection, n (%): | 207 (68.1) |
| -CS | 32 (15.5) |
| -HA | 101 (48.8) |
| -CS+HA | 51 (24.6) |
| -Unknown | 23 (11.1) |
| No prior IA injection, n (%) | 97 (31.9) |
| Patients | Age Years | Sex F/M | BMI | Diabetes | Smoking | Alcoholism | ASA | Infiltrations | Delay Surgery-PJI | Surgery | Bacteria | Antibiotic Therapy | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| DTS | Medication | n | Type | Duration | |||||||||||
| 1 | 73 | M | 32.3 | No | No | Yes | 1 | 14 m | CS | 1 | 11 d | Debridement, implant retention, replacement of exchangeable components | Methi-S Staph. aureus | Levofloxacin + Rifampicin | 12 w |
| 2 | 64 | F | 33.3 | Type 2 | No | No | 3 | - | - | 0 | 4 w | One-Stage Arthroplasty Exchange | Methi-S Staph. aureus | Levofloxacin + Rifampicin | 12 w |
| 3 | 88 | M | 20.4 | No | Former smoker | No | 2 | 1 m | HA | 9 | 5 w | One-Stage Arthroplasty Exchange | Methi-S Staph. aureus | Levofloxacin + Rifampicin | 12 w |
| 4 | 78 | F | 37.5 | No | No | No | 3 | - | - | 0 | 5 w | Debridement, implant retention, replacement of exchangeable components | Methi-S Staph. aureus | Levofloxacin + Clindamycin | 12 w |
| 5 | 85 | M | 28.7 | No | No | No | 3 | 4 m | CS | 3 | 4 w | Debridement, implant retention, replacement of exchangeable components | Methi-S Staph. aureus | Levofloxacin + Rifampicin | 12 w |
| 6 | 53 | M | 26.9 | No | No | No | 2 | 12 m | HA | unknown | 12 d | Debridement, implant retention, replacement of exchangeable components | Staph. capitis | Levofloxacin + Rifampicin | 8 w |
| 7 | 77 | M | 24.4 | No | Former smoker | No | 3 | 10 m | CS + HA | 7 | 5 m | Initially irrigation and debridment, then 4 months later 1-Stage Arthroplasty Exchange | Strep. oralis | Moxifloxacin + Amoxicillin after lavage; Moxifloxacin + Clindamycin after 1-stage exchange | 12 w |
| 8 | 74 | M | 29.4 | No | Current smoker | No | 3 | 4 m | CS + HA | 7 | 14 d | Debridement, implant retention, replacement of exchangeable components | Methi-R Staph. aureus | Cotrimoxazole + fusidic acid, then Clindamycin + fusidic acid (renal insufficiency) | 12 w |
| Independent Variables | Odds-Ratio | CI 95% | p |
|---|---|---|---|
| Age | 1.03 | 0.94–1.12 | 0.48 |
| Sex | 0.05 | 0.006–0.41 | 0.005 |
| BMI | 0.93 | 0.8–1.08 | 0.35 |
| Smoking | 2.36 | 0.54–10.1 | 0.24 |
| Diabetes mellitus | 0.72 | 0.08–5.98 | 0.76 |
| Alcoholism | 1.77 | 0.2–15.1 | 0.59 |
| ASA | 2.12 | 0.6–7.43 | 0.23 |
| Injection < 6 months | 3.46 | 0.79–15 | 0.09 |
| Characteristics | Males n = 84 | Females n = 220 | p |
|---|---|---|---|
| Mean age, years ± SD | 70.5 ± 8.8 | 72.3 ± 8.9 | 0.12 a |
| Mean BMI, kg/m2 ± SD | 30.6 ± 5.2 | 30.9 ± 5.4 | 0.71 a |
| Smoking (Active or cessation), n | 35 | 28 | 0.001 b |
| Diabetes mellitus, n | 21 | 29 | 0.01 b |
| Active alcoholism, n | 19 | 4 | 0.0001 b |
| ASA ≥ 3, n | 37 | 60 | 0.01 b |
| Injection < 6 months, n | 12 | 30 | 0.88 b |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grondin, J.; Menu, P.; Métayer, B.; Crenn, V.; Dauty, M.; Fouasson-Chailloux, A. Intra-Articular Injections Prior to Total Knee Arthroplasty Do Not Increase the Risk of Periprosthetic Joint Infection: A Prospective Cohort Study. Antibiotics 2021, 10, 330. https://doi.org/10.3390/antibiotics10030330
Grondin J, Menu P, Métayer B, Crenn V, Dauty M, Fouasson-Chailloux A. Intra-Articular Injections Prior to Total Knee Arthroplasty Do Not Increase the Risk of Periprosthetic Joint Infection: A Prospective Cohort Study. Antibiotics. 2021; 10(3):330. https://doi.org/10.3390/antibiotics10030330
Chicago/Turabian StyleGrondin, Jérôme, Pierre Menu, Benoit Métayer, Vincent Crenn, Marc Dauty, and Alban Fouasson-Chailloux. 2021. "Intra-Articular Injections Prior to Total Knee Arthroplasty Do Not Increase the Risk of Periprosthetic Joint Infection: A Prospective Cohort Study" Antibiotics 10, no. 3: 330. https://doi.org/10.3390/antibiotics10030330
APA StyleGrondin, J., Menu, P., Métayer, B., Crenn, V., Dauty, M., & Fouasson-Chailloux, A. (2021). Intra-Articular Injections Prior to Total Knee Arthroplasty Do Not Increase the Risk of Periprosthetic Joint Infection: A Prospective Cohort Study. Antibiotics, 10(3), 330. https://doi.org/10.3390/antibiotics10030330