
Antimicrobial Effects of Minocycline, Tigecycline, Ciprofloxacin, and Levofloxacin against Elizabethkingia anophelis Using In Vitro Time-Kill Assays and In Vivo Zebrafish Animal Models


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting and Ethics
2.2. MIC Determination
2.3. Bacterial Strain
2.4. In Vitro Time-Kill Studies
2.5. Analysis of Time-Kill Curves
2.6. Preparation of Bacteria for the Animal Study
2.7. Antimicrobial Effects in Zebrafish with E. anophelis Infection
3. Results
3.1. Antimicrobial Susceptibility Determined Using MIC
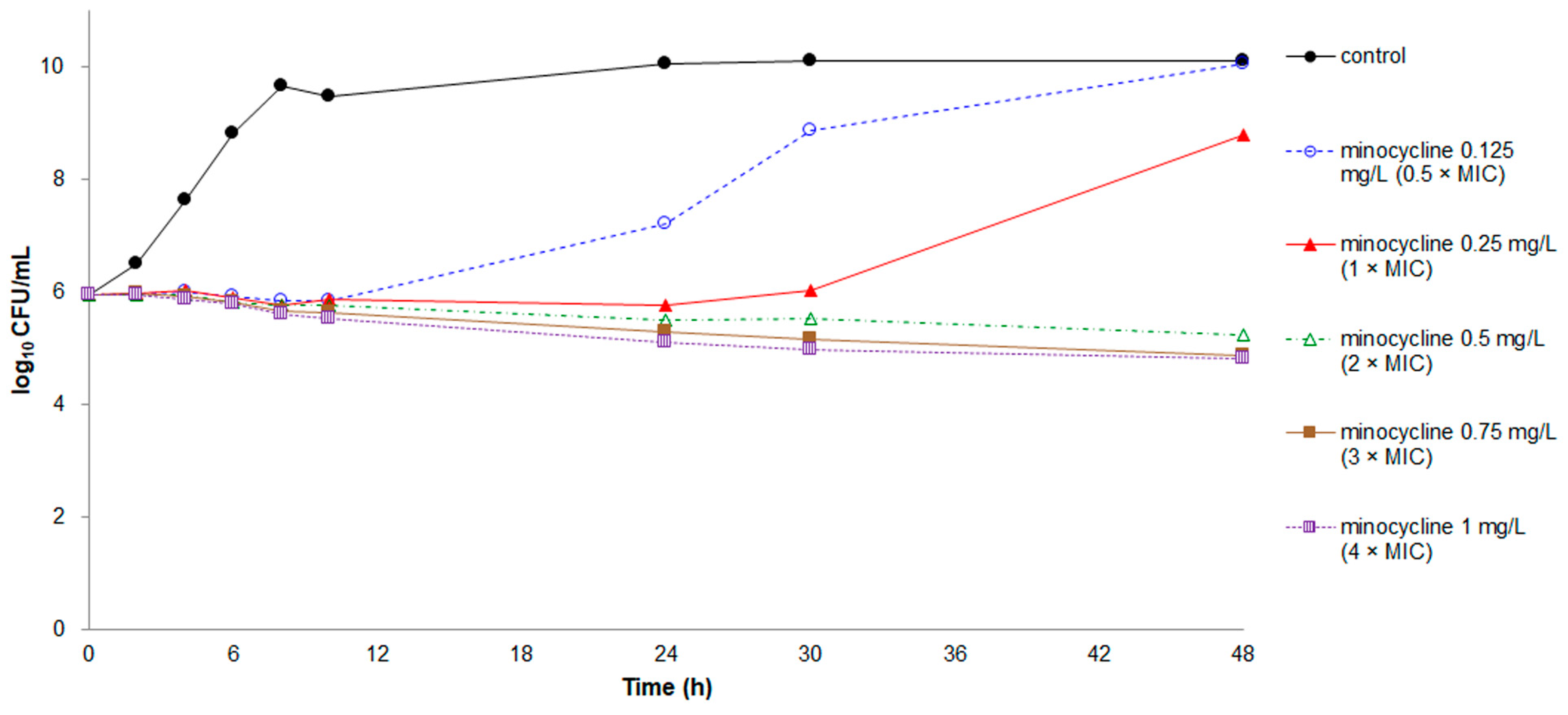
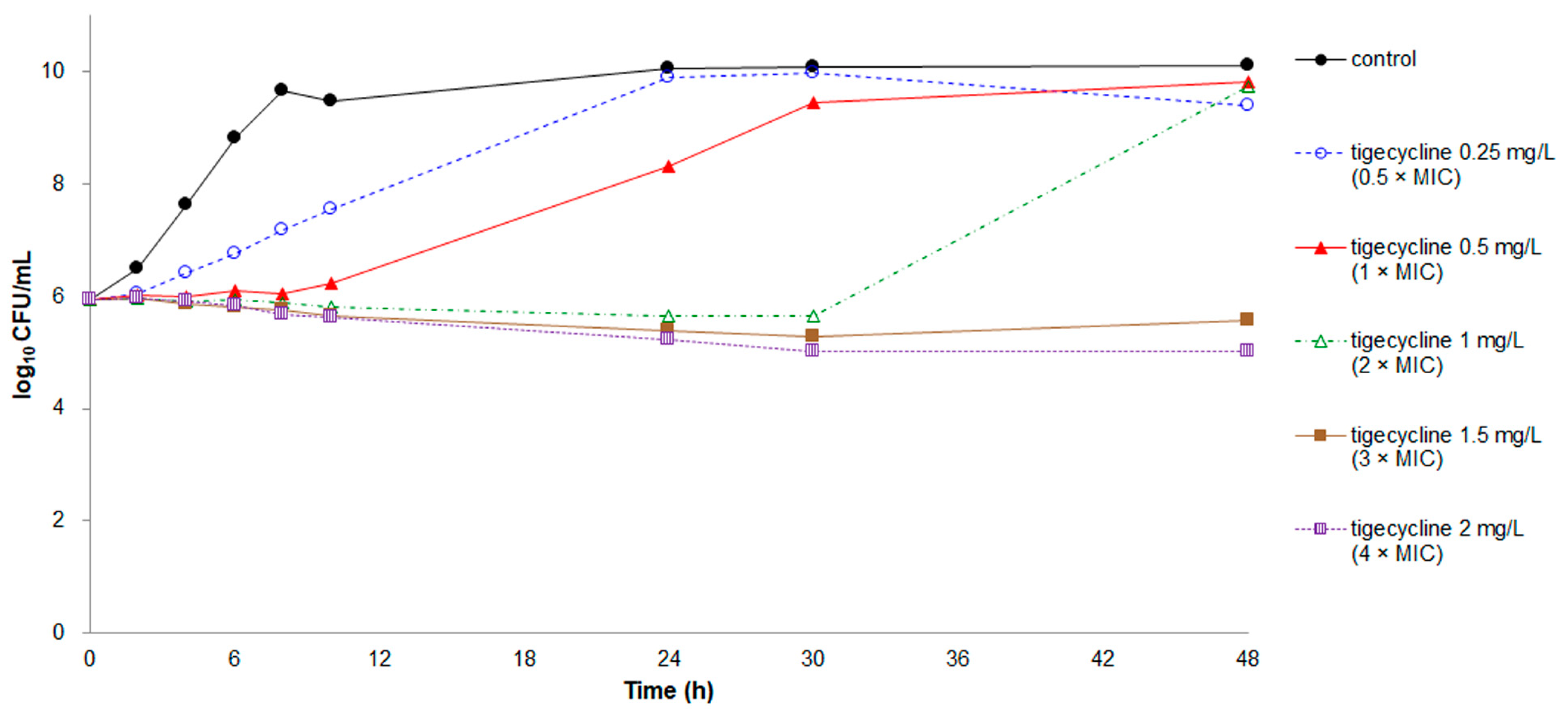
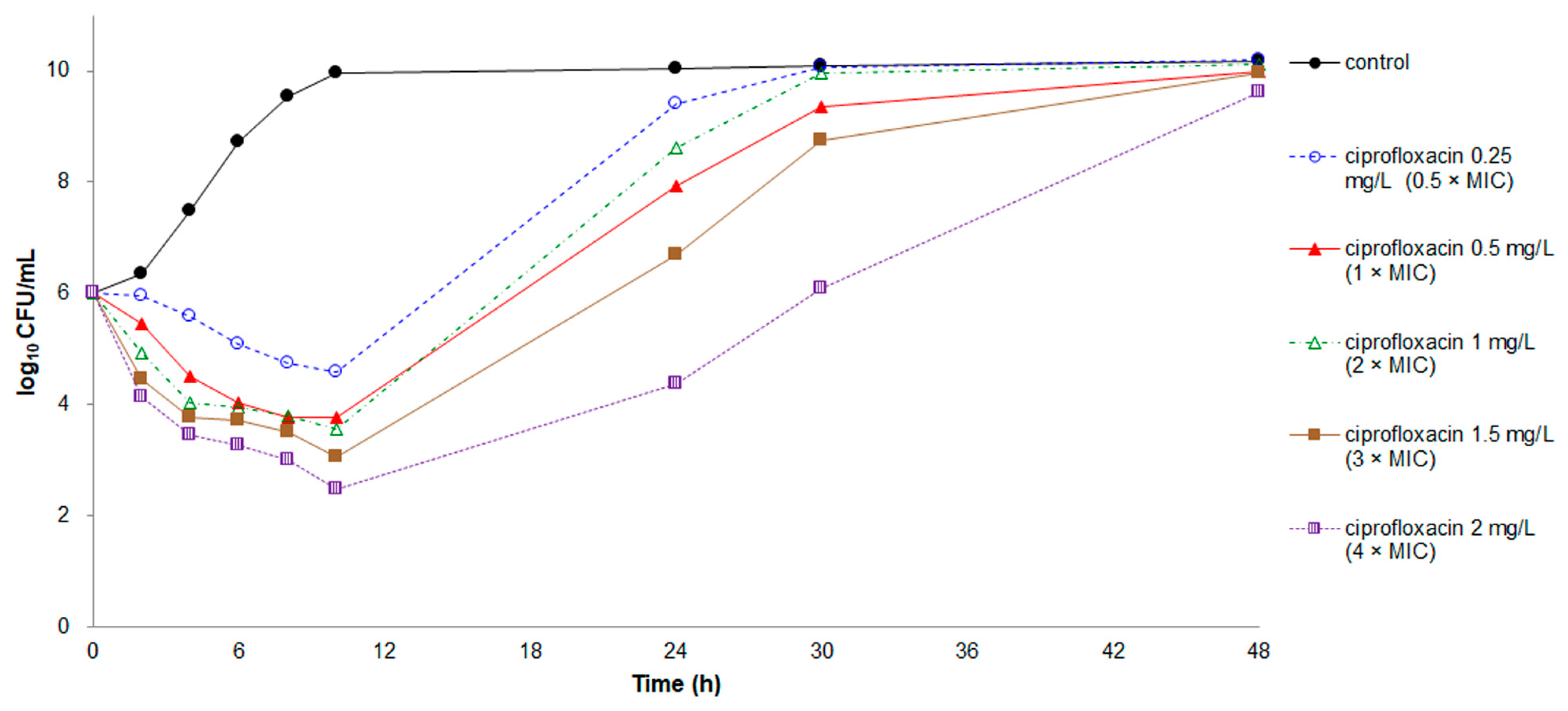
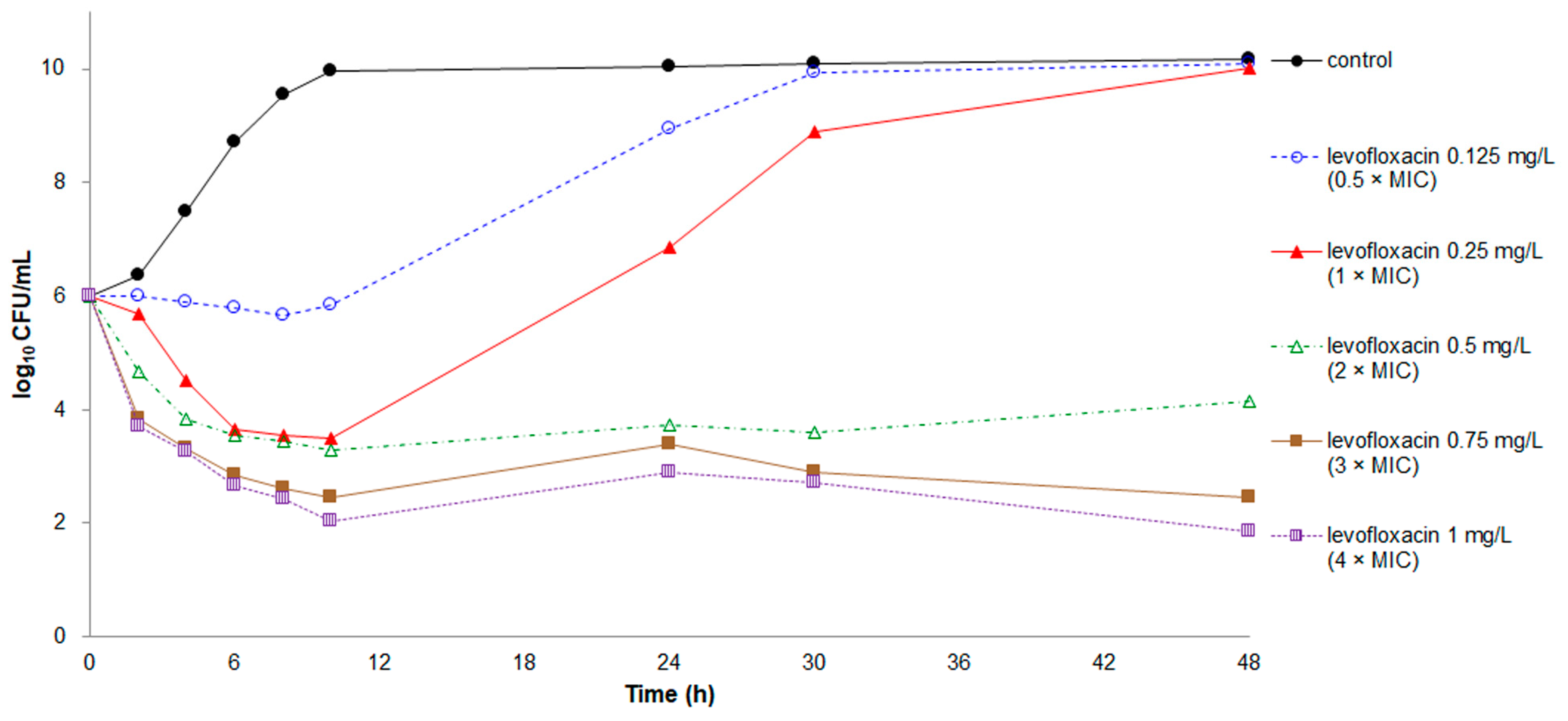
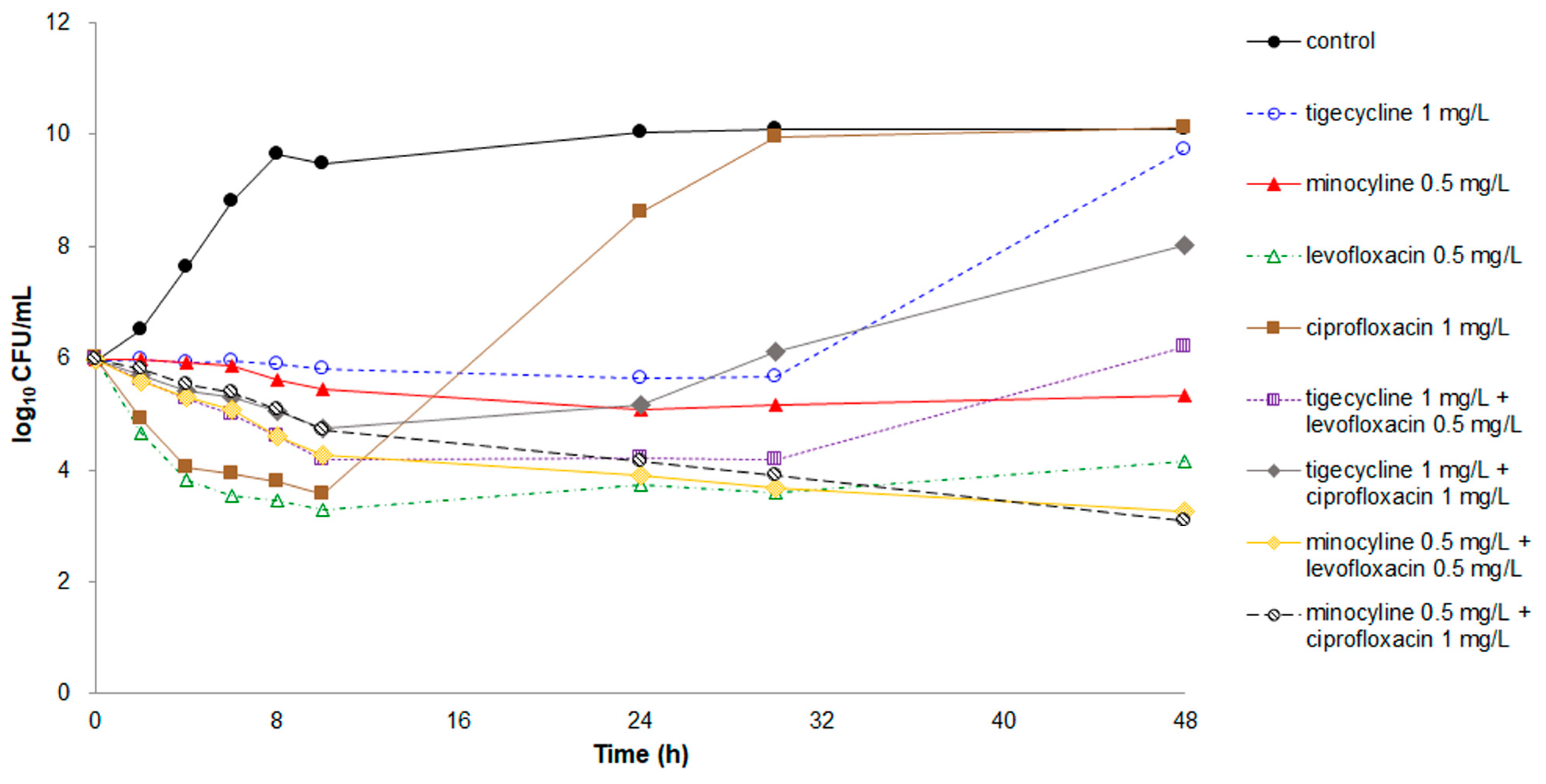
3.2. Time-Kill Studies of Single-Agent Therapy
3.3. Time-Kill Studies of Dual-Agent Combinations
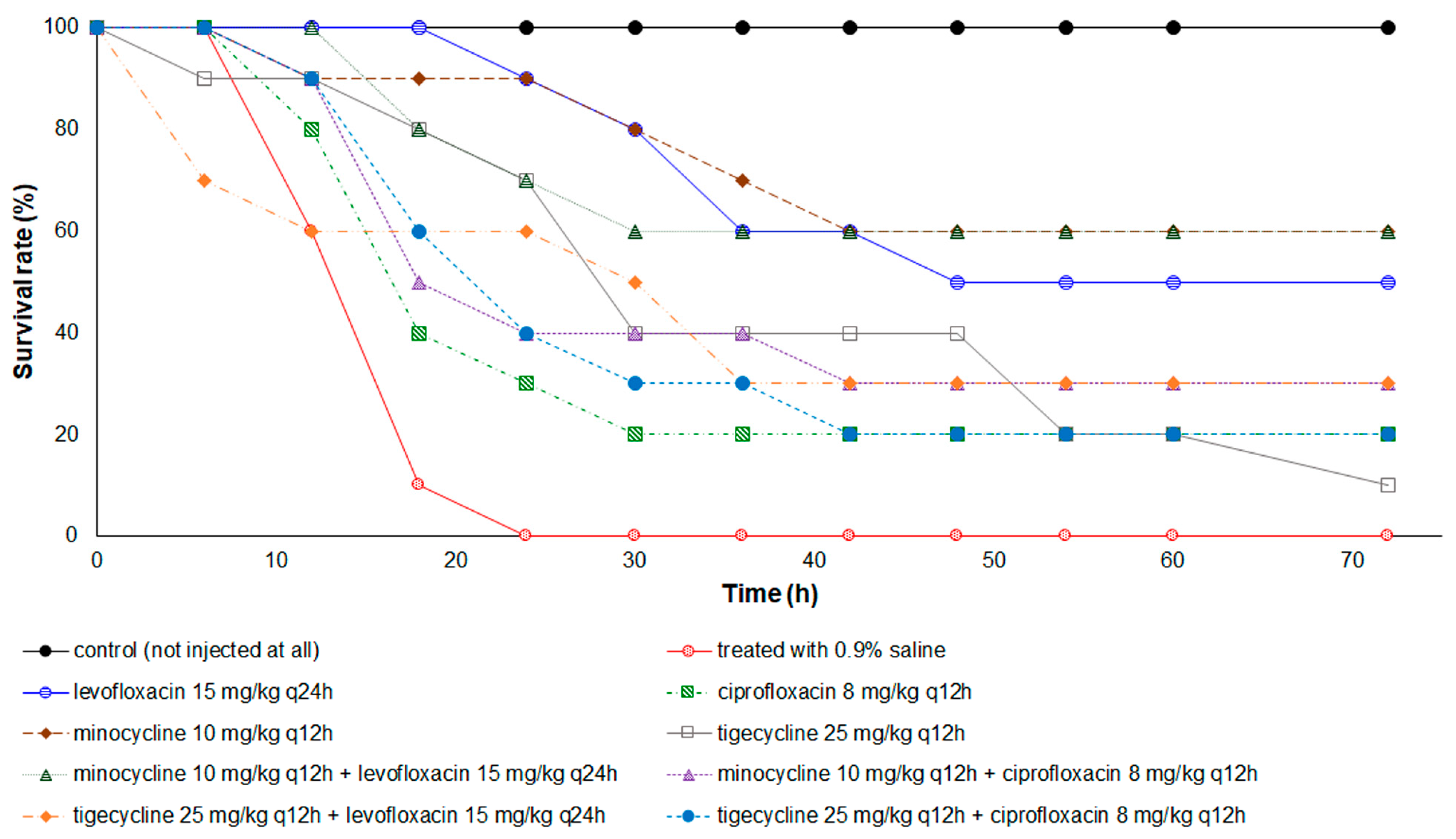
3.4. Therapeutic Effects of Antibiotics in the Zebrafish Animal Model
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Lin, J.N.; Lai, C.H.; Yang, C.H.; Huang, Y.H. Elizabethkingia infections in humans: From genomics to clinics. Microorganisms 2019, 7, 295. [Google Scholar] [CrossRef]
- Nicholson, A.C.; Gulvik, C.A.; Whitney, A.M.; Humrighouse, B.W.; Graziano, J.; Emery, B.; Bell, M.; Loparev, V.; Juieng, P.; Gartin, J.; et al. Revisiting the taxonomy of the genus Elizabethkingia using whole-genome sequencing, optical mapping, and MALDI-TOF, along with proposal of three novel Elizabethkingia species: Elizabethkingia bruuniana sp. nov., Elizabethkingia ursingii sp. nov., and Elizabethkingia occulta sp. nov. Antonie Leeuwenhoek 2018, 111, 55–72. [Google Scholar] [CrossRef]
- Teo, J.; Tan, S.Y.; Tay, M.; Ding, Y.; Kjelleberg, S.; Givskov, M.; Lin, R.T.; Yang, L. First case of E anophelis outbreak in an intensive-care unit. Lancet 2013, 382, 855–856. [Google Scholar] [CrossRef]
- Lau, S.K.; Chow, W.N.; Foo, C.H.; Curreem, S.O.; Lo, G.C.; Teng, J.L.; Chen, J.H.; Ng, R.H.; Wu, A.K.; Cheung, I.Y.; et al. Elizabethkingia anophelis bacteremia is associated with clinically significant infections and high mortality. Sci. Rep. 2016, 6, 26045. [Google Scholar] [CrossRef] [PubMed]
- Han, M.S.; Kim, H.; Lee, Y.; Kim, M.; Ku, N.S.; Choi, J.Y.; Yong, D.; Jeong, S.H.; Lee, K.; Chong, Y. Relative prevalence and antimicrobial susceptibility of clinical isolates of Elizabethkingia species based on 16S rRNA gene sequencing. J. Clin. Microbiol. 2017, 55, 274–280. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.N.; Lai, C.H.; Yang, C.H.; Huang, Y.H.; Lin, H.H. Clinical manifestations, molecular characteristics, antimicrobial susceptibility patterns and contributions of target gene mutation to fluoroquinolone resistance in Elizabethkingia anophelis. J. Antimicrob. Chemother. 2018, 73, 2497–2502. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.N.; Lai, C.H.; Yang, C.H.; Huang, Y.H. Comparison of clinical manifestations, antimicrobial susceptibility patterns, and mutations of fluoroquinolone target genes between Elizabethkingia meningoseptica and Elizabethkingia anophelis isolated in Taiwan. J. Clin. Med. 2018, 7, 538. [Google Scholar] [CrossRef] [PubMed]
- Perrin, A.; Larsonneur, E.; Nicholson, A.C.; Edwards, D.J.; Gundlach, K.M.; Whitney, A.M.; Gulvik, C.A.; Bell, M.E.; Rendueles, O.; Cury, J.; et al. Evolutionary dynamics and genomic features of the Elizabethkingia anophelis 2015 to 2016 Wisconsin outbreak strain. Nat. Commun. 2017, 8, 15483. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, C.; Kim, C.H. Zebrafish as a model for infectious disease and immune function. Fish Shellfish Immunol. 2008, 25, 341–350. [Google Scholar] [CrossRef]
- Moore, L.S.P.; Owens, D.S.; Jepson, A.; Turton, J.F.; Ashworth, S.; Donaldson, H.; Holmes, A.H. Waterborne Elizabethkingia meningoseptica in adult critical care. Emerg. Infect. Dis. 2016, 22, 9–17. [Google Scholar] [CrossRef]
- Yung, C.F.; Maiwald, M.; Loo, L.H.; Soong, H.Y.; Tan, C.B.; Lim, P.K.; Li, L.; Tan, N.W.; Chong, C.Y.; Tee, N.; et al. Elizabethkingia anophelis and association with tap water and handwashing, Singapore. Emerg. Infect. Dis. 2018, 24, 1730–1733. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, A.; Chenia, H.Y. Biofilm formation and adherence characteristics of an Elizabethkingia meningoseptica isolate from Oreochromis mossambicus. Ann. Clin. Microbiol. Antimicrob. 2011, 10, 16. [Google Scholar] [CrossRef] [PubMed]
- Hu, R.; Yuan, J.; Meng, Y.; Wang, Z.; Gu, Z. Pathogenic Elizabethkingia miricola infection in cultured black-spotted frogs, China, 2016. Emerg. Infect. Dis. 2017, 23, 2055–2059. [Google Scholar] [CrossRef]
- Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing, M100, 30th ed.; CLSI: Wayne, PA, USA, 2020. [Google Scholar]
- Kelesidis, T.; Karageorgopoulos, D.E.; Kelesidis, I.; Falagas, M.E. Tigecycline for the treatment of multidrug-resistant Enterobacteriaceae: A systematic review of the evidence from microbiological and clinical studies. J. Antimicrob. Chemother. 2008, 62, 895–904. [Google Scholar] [CrossRef]
- Ko, W.C.; Chiang, S.R.; Lee, H.C.; Tang, H.J.; Wang, Y.Y.; Chuang, Y.C. In vitro and in vivo activities of fluoroquinolones against Aeromonas hydrophila. Antimicrob. Agents Chemother. 2003, 47, 2217–2222. [Google Scholar] [CrossRef]
- Peck, K.R.; Kim, M.J.; Choi, J.Y.; Kim, H.S.; Kang, C.-I.; Cho, Y.K.; Park, D.W.; Lee, H.J.; Lee, M.S.; Ko, K.S. In vitro time-kill studies of antimicrobial agents against blood isolates of imipenem-resistant Acinetobacter baumannii, including colistin- or tigecycline-resistant isolates. J. Med. Microbiol. 2012, 61, 353–360. [Google Scholar] [CrossRef]
- Lin, J.N.; Chang, L.L.; Lai, C.H.; Lin, K.J.; Lin, M.F.; Yang, C.H.; Lin, H.H.; Chen, Y.H. Development of an animal model for alcoholic liver disease in zebrafish. Zebrafish 2015, 12, 271–280. [Google Scholar] [CrossRef]
- Saralahti, A.; Piippo, H.; Parikka, M.; Henriques-Normark, B.; Rämet, M.; Rounioja, S. Adult zebrafish model for pneumococcal pathogenesis. Dev. Comp. Immunol. 2014, 42, 345–353. [Google Scholar] [CrossRef]
- Tang, H.J.; Chang, M.C.; Ko, W.C.; Huang, K.Y.; Lee, C.L.; Chuang, Y.C. In vitro and in vivo activities of newer fluoroquinolones against Vibrio vulnificus. Antimicrob. Agents Chemother. 2002, 46, 3580–3584. [Google Scholar] [CrossRef] [PubMed]
- Ko, W.C.; Lee, H.C.; Chiang, S.R.; Yan, J.J.; Wu, J.J.; Lu, C.L.; Chuang, Y.C. In vitro and in vivo activity of meropenem and sulbactam against a multidrug-resistant Acinetobacter baumannii strain. J. Antimicrob. Chemother. 2004, 53, 393–395. [Google Scholar] [CrossRef]
- Greig, S.L.; Scott, L.J. Intravenous minocycline: A review in Acinetobacter infections. Drugs 2016, 76, 1467–1476. [Google Scholar] [CrossRef]
- Noskin, G.A. Tigecycline: A new glycylcycline for treatment of serious infections. Clin. Infect. Dis. 2005, 41, S303–S314. [Google Scholar] [CrossRef]
- Tessier, P.R.; Nicolau, D.P. Tigecycline displays in vivo bactericidal activity against extended-spectrum-β-lactamase-producing Enterobacteriaceae after 72-hour exposure period. Antimicrob. Agents Chemother. 2013, 57, 640–642. [Google Scholar] [CrossRef]
- Ozbek, B.; Mataraci, E. In vitro effectiveness of colistin, tigecycline and levofloxacin alone and combined with clarithromycin and/or heparin as lock solutions against embedded Acinetobacter baumannii strains. J. Antimicrob. Chemother. 2013, 68, 827–830. [Google Scholar] [CrossRef]
- Tang, H.J.; Chen, C.C.; Lai, C.C.; Zhang, C.C.; Weng, T.C.; Chiu, Y.H.; Toh, H.S.; Chiang, S.R.; Yu, W.L.; Ko, W.C.; et al. In vitro and in vivo antibacterial activity of tigecycline against Vibrio vulnificus. J. Microbiol. Immunol. Infect. 2018, 51, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Burrell, A.R.; McLaws, M.L.; Fullick, M.; Sullivan, R.B.; Sindhusake, D. SEPSIS KILLS: Early intervention saves lives. Med. J. Aust. 2016, 204, 73. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.E.; Kim, H.K.; Choi, S.M.; Yu, Y.; Kim, U.J.; Darboe, K.S.; Kang, S.J.; Park, K.H.; Kang, G.; Kim, Y.R.; et al. In vitro synergy and in vivo activity of tigecycline-ciprofloxacin combination therapy against Vibrio vulnificus sepsis. Antimicrob. Agents Chemother. 2019, 63. [Google Scholar] [CrossRef] [PubMed]
- Yim, H.; Woo, H.; Song, W.; Park, M.J.; Kim, H.S.; Lee, K.M.; Hur, J.; Park, M.-S. Time-kill synergy tests of tigecycline combined with imipenem, amikacin, and ciprofloxacin against clinical isolates of multidrug-resistant Klebsiella pneumoniae and Escherichia coli. Ann. Clin. Lab. Sci. 2011, 41, 39–43. [Google Scholar]
- Aliskan, H.; Can, F.; Demirbilek, M.; Colakoglu, S.; Kilic, S.; Arslan, H. Determining in vitro synergistic activities of tigecycline with several other antibiotics against Brucella melitensis using checkerboard and time-kill assays. J. Chemother. Florence Italy 2009, 21, 24–30. [Google Scholar] [CrossRef]
- Petersen, P.J.; Labthavikul, P.; Jones, C.H.; Bradford, P.A. In vitro antibacterial activities of tigecycline in combination with other antimicrobial agents determined by chequerboard and time-kill kinetic analysis. J. Antimicrob. Chemother. 2006, 57, 573–576. [Google Scholar] [CrossRef]
- Principe, L.; D’Arezzo, S.; Capone, A.; Petrosillo, N.; Visca, P. In vitro activity of tigecycline in combination with various antimicrobials against multidrug resistant Acinetobacter baumannii. Ann. Clin. Microbiol. Antimicrob. 2009, 8, 18. [Google Scholar] [CrossRef] [PubMed]
- Ozbek, B.; Sentürk, A. Postantibiotic effects of tigecycline, colistin sulfate, and levofloxacin alone or tigecycline-colistin sulfate and tigecycline-levofloxacin combinations against Acinetobacter baumannii. Chemotherapy 2010, 56, 466–471. [Google Scholar] [CrossRef] [PubMed]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, J.-N.; Lai, C.-H.; Huang, Y.-H.; Yang, C.-H. Antimicrobial Effects of Minocycline, Tigecycline, Ciprofloxacin, and Levofloxacin against Elizabethkingia anophelis Using In Vitro Time-Kill Assays and In Vivo Zebrafish Animal Models. Antibiotics 2021, 10, 285. https://doi.org/10.3390/antibiotics10030285
Lin J-N, Lai C-H, Huang Y-H, Yang C-H. Antimicrobial Effects of Minocycline, Tigecycline, Ciprofloxacin, and Levofloxacin against Elizabethkingia anophelis Using In Vitro Time-Kill Assays and In Vivo Zebrafish Animal Models. Antibiotics. 2021; 10(3):285. https://doi.org/10.3390/antibiotics10030285
Chicago/Turabian StyleLin, Jiun-Nong, Chung-Hsu Lai, Yi-Han Huang, and Chih-Hui Yang. 2021. "Antimicrobial Effects of Minocycline, Tigecycline, Ciprofloxacin, and Levofloxacin against Elizabethkingia anophelis Using In Vitro Time-Kill Assays and In Vivo Zebrafish Animal Models" Antibiotics 10, no. 3: 285. https://doi.org/10.3390/antibiotics10030285
APA StyleLin, J.-N., Lai, C.-H., Huang, Y.-H., & Yang, C.-H. (2021). Antimicrobial Effects of Minocycline, Tigecycline, Ciprofloxacin, and Levofloxacin against Elizabethkingia anophelis Using In Vitro Time-Kill Assays and In Vivo Zebrafish Animal Models. Antibiotics, 10(3), 285. https://doi.org/10.3390/antibiotics10030285